
HYBRID METHODS OF KNOWLEDGE ELICITATION WITHIN
A UNIFIED REPRESENTATIONAL KNOWLEDGE SCHEME
Sergei Nirenburg, Marjorie McShane, Stephen Beale
University of Maryland Baltimore County, Maryland, U.S.A.
Roberta Catizone
Onyx Consulting, Sheffield, U.K.
Keywords: Knowledge engineering, Knowledge elicitation, Ontology, Intelligent agents, Automatic reasoning,
Influence diagrams.
Abstract: This paper presents a case study showing how hybrid methods of knowledge elicitation can be used to build
models in support of the functioning of intelligent agents. What facilitates both the elicitation of knowledge
and its conversion into actionable models is the use of a unified representational knowledge scheme – spe-
cifically, an unambiguous, ontologically grounded metalanguage that serves as the language of all recorded
knowledge as well as the language in which agents remember and reason.
1 INTRODUCTION
The process of acquiring knowledge from experts to
support sophisticated intelligent agents is known to
be an expensive and difficult enterprise, leading to a
long history of research in knowledge acquisition
methodologies. As Cooke (no date) reports, reviews
and categorization schemes for knowledge elicita-
tion and modeling “abound”. But, as Ford and Ster-
man (1998) write, “While many methods to elicit
information from experts have been developed, most
assist in the early phases of modeling: problem arti-
culation, boundary selection, identification of va-
riables, and qualitative causal mapping… The litera-
ture is comparatively silent, however, regarding me-
thods to elicit the information required to estimate
the parameters, initial conditions, and behavior rela-
tionships that must be specified precisely in formal
modeling.”
We have been experimenting with hybrid know-
ledge elicitation and modeling in the OntoAgent
environment, whose recent applications include
Maryland Virtual Patient (MVP) and CLinician’s
ADvisor (CLAD). MVP is a cognitive simulation
and training system whose goal is to provide medi-
cal practitioners with the opportunity to develop
clinical decision-making skills by managing many
highly differentiated artificial intelligent agents play-
ing the role of virtual patients (VPs) (McShane et al.,
2007a; Jarrell et al., 2008). These VPs can suffer
from various diseases and combinations of diseases
(McShane et al., 2007b) and are capable of realistic
physiological and cognitive responses even to unex-
pected actions on the part of the user (Nirenburg et
al., 2008a,b). CLAD seeks to decrease the cognitive
load on clinicians by providing various kinds of con-
textualized decision support (McShane et al., Sub-
mitted).
Both of these applications require many kinds of
intelligent agent behavior. In this paper we will fo-
cus on two of them: physiological simulation and
decision making in the realm of best clinical prac-
tices. Very briefly, here is how each of these func-
tionalities is used. Physiological Simulation: In
MVP, physiological simulation permits the virtual
patient to “live” over time and respond realistically
to non-scripted interventions by the user. In CLAD,
physiological simulation is used by the advisor to
project patient outcomes (over time and in response
to different treatment strategies) as input to decision
making. Decision making about clinical practices:
In MVP, knowledge about best clinical practices is
used by the tutor to provide feedback and advice to
trainees. In CLAD, knowledge about best clinical
practices is used by the advisor to carry out the main
177
Nirenburg S., McShane M., Beale S. and Catizone R..
HYBRID METHODS OF KNOWLEDGE ELICITATION WITHIN A UNIFIED REPRESENTATIONAL KNOWLEDGE SCHEME.
DOI: 10.5220/0003069601770182
In Proceedings of the International Conference on Knowledge Engineering and Ontology Development (KEOD-2010), pages 177-182
ISBN: 978-989-8425-29-4
Copyright
c
2010 SCITEPRESS (Science and Technology Publications, Lda.)

function of the system – time- and context-sensitive
advice giving.
As part of our work on knowledge-based appli-
cations, we have been developing knowledge elicita-
tion methodologies that permit domain experts to
independently carry out as much work as possible
before collaborating with knowledge engineers. We
have found truth in Hoffman and Lintern’s (2006)
statement that “methodology benefits from oppor-
tunism”: i.e., the need of a concrete knowledge elici-
tation project can offer the opportunity of discover-
ing new methodologies and new combinations of
methodologies. In turn, those methodologies can
foster more streamlined thinking for future model-
ing.
Before proceeding to the body of the paper,
which addresses specific knowledge elicitation strat-
egies used in the OntoAgent environment, some
background about our knowledge representation
scheme and our approach to knowledge elicitation is
in order.
The Knowledge Representation Scheme. All
knowledge in our system is recorded using an onto-
logically grounded metalanguage that derives from
the theory of Ontological Semantics (Nirenburg and
Raskin 2004), which is implemented in the OntoA-
gent (an extension of the earlier “OntoSem”) envi-
ronment (Beale et al. 2004; McShane, Nirenburg and
Beale, 2005). The OntoAgent meaning representation
language expresses meaning using unambiguous
ontological concepts and their instances, which are
linked to each other using ontologically recorded
properties. This metalanguage is not only the lan-
guage of recorded static knowledge, it is the language
of thought of all intelligent agents. The OntoAgent
ontology that forms the core of the environment cur-
rently contains about 9,500 concepts, most of which
belong to the general domain. It includes not only
slot-filler style knowledge but also domain and
workflow scripts (i.e., complex events) of the type
introduced by Schank and Abelson (1977). In the
medical domain, these scripts cover everything from
normal physiology to pathology to best clinical prac-
tices to decision-making on the part of the physician
and the patient.
Since our human-like intelligent agents must be
able to communicate with people in natural language,
the environment includes a large suite of natural lan-
guage processing resources and tools, including a
large lexicon whose semantic descriptions employ
ontological concepts. When intelligent agents perce-
ive language input, they automatically translate it
into the unambiguous metalanguage that they use for
remembering and reasoning; on the other end, when
they have something to communicate to a person,
they formulate the content in the metalanguage then
translate it into English.
Our approach to Knowledge Elicitation (KE).
Note: To ground our knowledge elicitation strategy
in the tradition of past work, we will point to how it
conforms to all seven of Breuker’s KADS “Know-
ledge Acquisition and Domain Structuring” prin-
ciples for the elicitation of knowledge and construc-
tion of a system (Breuker, 1987, as summarized in
Shadbolt and Burton, 1995).
KE, for the first six diseases modeled in our en-
vironment, was carried out through collaboration
between domain experts and knowledge engineers,
primarily using unstructured and semi-structured
interviews. (Cf. the KADS principle that the know-
ledge should be analyzed before design and imple-
mentation begin.) However, based on that expe-
rience, we have been able to create an automatic KE
system that guides the expert through the process of
providing much of the knowledge required for dis-
ease modeling. Our approach derives largely from
past work in a different domain – computational field
linguistics. Our Boas system (McShane and Niren-
burg 2003) was a mixed-initiative KE system aimed
at quickly gathering formally organized, machine
tractable knowledge about lesser-studied languages
from speakers of the language without the assistance
of a linguist. The mixed-initiative, expectation-driven
methodology used there has translated directly into
our OntoElicit system for KE in the medical domain.
Developing OntoElicit involved (a) organizing
the domains of normal physiology, pathology and
clinical knowledge into classes of parameters and
value sets (cf. the KADS principle that the analysis
should be model-driven as early as possible); (b)
applying past experience in modeling 6 esophageal
diseases; (c) taking into consideration the nature of
the target, generalized processors that were devel-
oped to support simulation and reasoning across
agents, applications and diseases; (d) anticipating the
needs of non-developer domain experts, who will
work with the system largely independently of know-
ledge engineers; and (e) having realistic expectations
about what can be elicited automatically and what
requires collaboration with a knowledge engineer.
OntoElicit is a web-based KE system organized
as a series of tasks. Methods of progressive disclo-
sure (“as needed” explanation) support domain ex-
perts having different levels of experience working
with the system. The descriptions below highlight the
aspects of medical modeling that are incorporated
into OntoElicit. Aspects of modeling requiring live
KEOD 2010 - International Conference on Knowledge Engineering and Ontology Development
178
collaboration with knowledge engineers are de-
scribed in McShane et al. (2007a, b).
2 PHYSIOLOGICAL MODELING
Our physiological models cover normal physiology,
pathology, and the physiological effects of interven-
tions. To make modeling realistic, we model only
events and their properties that have known utility in
our applications: that is, they must either be part of
an important chain of events, measurable by a test,
or be able to be changed by a drug, intervention, the
effects of another disease, etc. (Cf. the KADS prin-
ciple that the analysis should include the functionali-
ty of the system being developed, which we interpret
as the tenet that knowledge should not be elicited or
recorded just because we can but because we need
to.)
Modeling Normal Physiology. Physiological
scripts are recorded as complex events in the On-
toAgent ontology using the formal but still human-
readable (after minimal training) formalism shown
below.
(SWALLOW
(AGENT HUMAN) (THEME BOLUS)
(DURATION 10 (DEFAULT-MEASURE SECOND))
(PRECONDITION
(LOCATION (DOMAIN BOLUS) (RANGE MOUTH)))
(EFFECT
(LOCATION (DOMAIN BOLUS) (RANGE STOMACH)))
(HAS-EVENT-AS-PART
OROPHARYNGEAL-PHASE-OF-SWALLOWING
ESOPHAGEAL-PHASE-OF-SWALLOWING))
(
OROPHARYNGEAL-PHASE-OF-SWALLOWING
…
This is a small excerpt from the script for swal-
lowing, showing perhaps 1/20 of the entire script.
SWALLOW is the ontological concept that heads the
swallowing script. The
AGENT property of SWALLOW
is constrained to HUMAN and the THEME to a BOLUS,
which is a small mass of liquid or chewed solid food
that is swallowed. The
PRECONDITION for SWALLOW
is that the BOLUS be located in the MOUTH and the
EFFECT is that it is located in the STOMACH. The DU-
RATION
of swallowing is 10 seconds. The rest of the
script is a hierarchical encoding of fillers of the
HAS-
EVENT-AS-PART property. The subevents of SWAL-
LOW
are OROPHARYNGEAL-PHASE-OF-SWALLOWING
and ESOPHAGEAL-PHASE-OF-SWALLOWING, which
have their own subevents, which have their own
properties, and so on. (Cf. the KADS principle that
knowledge should be encoded in an incremental
way, meaning breadth-first.)
This example shows only a fraction of the ex-
pressive means used in scripts – there are also vari-
able bindings, loops, conditions, etc. However, it
suffices to make the main point: the ontological
metalanguage provides a conceptual framework for
eliciting knowledge about complex events.
In OntoElicit, domain experts are led through the
process of creating scripts by first listing the main
events of a physiological process, then adding
subevents, then adding selected properties of each
subevent:
THEME, PRECONDITION, EFFECT and select
others. They are instructed to begin at a relatively
coarse grain-size, since more details can be added as
found necessary. (Cf. the KADS principle that new
data should be elicited only when collected data has
been analyzed.) The domain expert can record the
knowledge in prose or his/her own invented semi-
formalism. (Cf. the KADS principle that an inter-
mediate level representation should be encoded
first.) The use of a fixed inventory of properties of
interest, and a structured process for eliciting them,
is similar in function to Shadbolt and Burton’s
(1995) inventory of “linguistic probes” used in a
structured interview: “The idea here is that the elici-
tor engages in a type of slot/filler dialogue”.
Modeling Diseases. Diseases are complex
events and could, in principle, be modelled using the
same type of strategy as just described for normal
physiology. However, we have found a different
operational metaphor to be useful: tables that track
relevant property values over conceptual stages of
the disease.
In OntoElicit, domain experts are asked to divide
the disease into any number of conceptual stages
correlating with important events, findings, symp-
toms or the divergence of disease paths among pa-
tients. They are also asked to indicate the typical
duration of each stage as a range (x-y in Table 1)
with a default value (d). Next, they are led through
the process of describing the physiology, symptoms,
test results and results of interventions, should the
latter be administered at each stage of the disease.
The high-level conceptual model is shown in Table
1. Note that experts are not asked to fill in a table
like this all at once: they are led through a well-
explained, step-by-step process of providing the
component knowledge.
Table 1: KE for the clinical model of a disease.
Props. Start Stage 1 Stage 2
Duration
x-y (d) x-y (d)
Physiology
P1 x-y (d) x-y (d) x-y (d)
P2 x-y (d) x-y (d) x-y (d)
Symptoms
S1 x-y (d) x-y (d) x-y (d)
S2 x-y (d) x-y (d) x-y (d)
Test Results
T1 x-y (d) x-y (d) x-y (d)
T2 x-y (d) x-y (d) x-y (d)
Interventions
I1 x-y (d) x-y (d) x-y (d)
I2 x-y (d) x-y (d) x-y (d)
HYBRID METHODS OF KNOWLEDGE ELICITATION WITHIN A UNIFIED REPRESENTATIONAL KNOWLEDGE
SCHEME
179
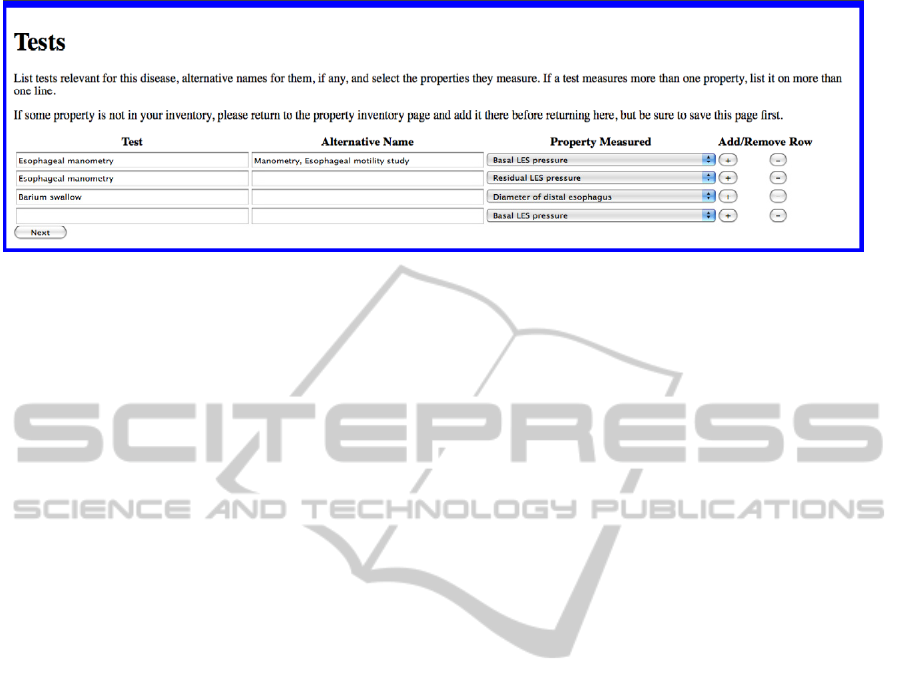
Figure
1: The first KE screen for tests, partially filled out for a particular disease.
For physiology and symptoms, the expert pro-
vides the inventory of properties (Props.) that
change over time, their start value before the disease
begins and their expected values at end of each con-
ceptual stage. Most values will be recorded as a
range of values (x-y) covering different individual
patients in the population along with a default (d)
representing the most typical value. When value sets
are numerical, the values at any point in a stage can
be interpolated by the simulation engine.
In the test results section, the expert indicates (a)
which physiological properties are measured by each
test, (b) any test results that are not among those
covered by the physiological model, e.g., visual
findings by the administrator of the test and (c) a
“specialist’s interpretation” of what the test results
returned at that stage would indicate: e.g., “Sugges-
tive of disease X.” (Raw test results for recorded
physiological properties can, of course, be provided
by the simulation engine.) The first part of this
thread of elicitation is shown in Figure 1. The prop-
erties measured were recorded earlier and are se-
lected from a pull-down menu.
For interventions, including medications, the ex-
pert indicates (a) what properties and/or symptoms
are affected by the intervention, (b) the possible out-
comes of the intervention, (c) possible side effects,
and (d) if known, the percentage of the population
expected to have each outcome and side effect.
After the properties and value sets provided by
the expert have been translated into the ontological
metalangauge, the disease models developed using
this strategy are sufficient to support the simulation
of diseases as they progress outside of “interven-
tions”, which may be generated internally (as by
another disease) or externally (as by the use of me-
dication or surgery). To accommodate the effects of
interventions, OntoElicit elicits knowledge in a simi-
lar way as for modeling normal physiology – i.e.,
using scripts – with a focus on the properties
PRE-
CONDITION
and (immediate) EFFECT. The progres-
sion or regression of the disease during or after an
intervention is again recorded using the table-based
strategy, often with only slight modifications to the
values recorded in the original model. For example,
a medication might slow the rate of progression of a
disease – affecting the filler of the parameter “stage
duration” – but leave everything else the same, or it
might relieve symptoms but leave disease progres-
sion unchanged, or it might reverse some physiolog-
ical changes but leave others unaffected.
3 MODELING CLINICAL
PRACTICES
One of the principles we follow is to record knowl-
edge in the simplest way possible to support an ap-
plication. As regards clinical advice giving, our ap-
plications use three kinds of recorded knowledge for
three functional contexts: checking the validity of a
clinical move; advising what to do next in simple,
“textbook” contexts; and advising what to do next in
complex contexts.
Checking the Validity of a Clinical Move. Our
first priority in developing MVP was to build a
simulation environment for trial-and-error learning,
with the gradual addition of tutoring support. As
such, our initial tutoring functionalities were narrow
in scope: checking whether each move by the trainee
conformed to what we call “preconditions of good
practice” and, if not, providing various extents of
information (based on user preferences) about why
not.
The knowledge needed to support this function-
ality is readily encoded using the basic slot-filler
structures of the OntoAgent ontology. For example,
for each disease we record values for the properties
SUFFICIENT-GROUNDS-TO-SUSPECT, SUFFICIENT-
GROUNDS-TO-DIAGNOSE, SUFFICIENT-GROUNDS-TO-
TREAT (e.g., clinical diagnosis or definitive diagno-
KEOD 2010 - International Conference on Knowledge Engineering and Ontology Development
180

sis), etc.. Similar inventories of properties are used
for tests, treatments, making definitive diagnoses,
and so on. The content of this knowledge is both
broader and deeper than that available in published
“best practices” guides. OntoElicit uses tables for
eliciting this information, with the experts providing
prose descriptions of property fillers. These descrip-
tions are then converted – like all other aspects of
acquired knowledge – into formal, ontologically
grounded structures by knowledge engineers and
programmers. Table 2 shows a combination of elic-
ited knowledge (with a clear background) and for-
mally encoded knowledge (with a gray background)
for one factoid about one disease.
Table 2: Sample precondition of good practice.
DISEASE ACHALASIA
PROPERTY SUFFICIENT-GROUNDS-TO-SUSPECT
Prose
filler
solid and liquid dysphagia or regurgitation
Formal
encoding
(or
(and ((SOLIDS-STICK HUMAN YES)
(LIQUIDS-STICK HUMAN YES))
(REGURGITATION-FREQUENCY
HUMAN (> 0)))))
One of the advantages of recording all knowl-
edge using the same ontological metalangauge is
that knowledge can be reused in both immediately
obvious and to-be-discovered ways. For example,
imagine that a trainee using MVP wants to posit a
diagnosis, but is told by the tutor that before doing
so the value of Property P must be known to be > =
x. Imagine further that the trainee does not know
which tests determine that property value. Using
knowledge already recorded in the ontology, the
system can look up which property values are meas-
ured by each test and return those tests that measure
the needed property value.
Since each agent in our environment has a differ-
ent ontology (knowledge base of object and event
types and their relationships) and fact repository
(knowledge base of ontological instances and their
relationships), MVP can contain multiple tutors with
different opinions about best practices all residing in
the system and used as selected by a teacher or
trainee.
Advising What to do Next in Simple and
Complex Contexts. Another type of clinical advice
that is central to CLAD and will soon be incorpo-
rated into MVP is What to do next? In the simplest
case, a single answer can be arrived at using condi-
tions recorded in the precondition and effect slots of
ontological scripts. This kind of knowledge can of-
ten be found in textbooks, sometimes even in a deci-
sion tree representation. In OntoElicit, recording this
kind of knowledge is supported using the script writ-
ing methodology described above, with an emphasis
on conditional statements.
However, many clinical moves must be decided
upon (a) in the face of competing conditions, (b)
with different preferences of different “stakeholders”
(e.g., the patient, the physician, the insurance com-
pany) and (c) using incomplete knowledge of rele-
vant property values. For those cases, we have been
experimenting with the use of Bayesian networks
that are constructed with the help of influence dia-
grams (For more on influence diagrams, see Howard
and Matheson (2005); for an example of their use in
another medical domain, see Lucas (1996); and for
more details about our work using them, see
McShane et al. (Submitted).) The knowledge en-
coded in influence diagrams represents an expert’s
opinion about the utility scores of different combina-
tions of property values associated with each possi-
ble decision. One of the main reasons why we chose
to work with influence diagrams is that the kind of
information required of experts is of a nature that
they can readily conceptualize. In essence, they are
asked: Given X combination of property values, how
good is solution Y? Given X combination of property
values, how good is solution Z? and so on. The
properties and values are familiar to our experts be-
cause they are the same ones used to build the other
models in the system. We are using the Netica
(http://www.norsys.com/) environment to create
influence diagrams. Knowledge engineers help ex-
perts to organize the problem space into subprob-
lems, as applicable, and to develop a case-specific
methodology of filling out the utility tables in the
most efficient way.
Although the nature of information required of
experts in an influence-diagram-driven methodology
is straightforward, one problem is that the number of
features involved in making a complex decision can
be large, easily driving the number of feature value
permutations into the tens or hundreds of thousands.
As in all aspects of our modeling, we approach this
problem using realistic strategies including the fol-
lowing: (1) Organizing the knowledge optimally –
e.g., covering as many variables as possible using
local decisions whose output contributes to a more
general decision; (2) Simplifying the problem space
and judging if the results are sufficient to yield real-
istic, accurate functioning – e.g., not including every
parameter we can think of but, instead, focusing on
those considered to have the most impact by clini-
cians; (3) Working toward automating the process of
knowledge acquisition – e.g., using functions to pro-
vide values for many of the feature-value combina-
HYBRID METHODS OF KNOWLEDGE ELICITATION WITHIN A UNIFIED REPRESENTATIONAL KNOWLEDGE
SCHEME
181

tions once a pattern of utility scores has been recog-
nized. (For other issues related to reducing the com-
plexity of knowledge acquisition of influence dia-
grams see Bielza, Gomez and Shenoy (2010).) Fol-
lowing these tenets, we successfully configured our
first demonstration system of CLAD.
As regards incorporating aspects of influence
diagram creation into OntoElicit, our current think-
ing is that experts could, in fact, be led through the
process of decomposing the problem into the main
variables in the decision vs. the variables in local
decisions (cf. point (1) above), but we have yet to
experiment with this methodology.
4 CONCLUSIONS
In this paper, we have provided a sweeping introduc-
tion to some of the different kinds of modeling
strategies used within the OntoAgent environment.
We have shown how our problem space design has
facilitated the creation of a mixed-initiative KE sys-
tem for encoding clinical knowledge in the metalan-
guage of the OntoAgent environment. One of the
advantages of our modeling strategies is that the
knowledge is formulated such that it can understood
not only by the expert him- or herself but also by the
wider community, as illustrated in Jarrell et al.
(2008). (Cf. the KADS principle that collected data
and analysis should be documented.) Although we
are well aware that such general strategies will not
be sufficient to overcome all modeling challenges,
we believe that they are beneficial in helping experts
to conceptualize domains quickly, independently
and in the most practical way. In this sense we be-
lieve that this work makes a contribution to over-
coming the knowledge bottleneck in constructing
practical knowledge-based systems.
REFERENCES
Beale, S., Lavoie, B., McShane, M., Nirenburg, S.,
Korelsky, T., 2004. Question answering using Onto-
logical Semantics. In Proceedings of ACL-2004 Work-
shop on Text Meaning and Interpretation.
Bielza, C., Gomez, M., Shenoy, P. P., 2010. Modeling
challenges with influence diagrams: Constructing
probability and utility models. In Decision Support
Systems (in press).
Breuker, J. (Ed.), 1987. Model-driven knowledge acquisi-
tion interpretation models. Deliverable task AI, Esprit
Project 1098 (University of Amsterdam).
Cooke, N.J. (no date), Knowledge elicitation. Available at
http://www.cerici.org/documents/Publications/Durso%
20chapter%20on%20KE.pdf
Ford, D. N., Sterman, J. D., 1998. Expert knowledge elici-
tation to improve formal and mental models. In Syst.
Dyn. Rev. 14: 309-340.
Hoffman, R. A., Lintern, G., 2006. Eliciting and
representing the knowledge of experts. In Ericsson, K.
A., Charness, N., Feltovich, P., Hoffman, R. (Eds.),
Cambridge Handbook of Expertise and Expert Per-
formance, pp. 203-222. New York, Cambridge Uni-
versity Press.
Howard, R. A., Matheson, J. E., 2005. Influence diagrams.
In Decision Anal. 2(3): 127–143.
Jarrell, B., Nirenburg, S., McShane, M., Fantry, G.,
Beale, S., 2008. Revealing the conceptual substrate of
biomedical cognitive models to the wider community.
In Medicine Meets Virtual Reality 16.
Lucas, P., 1996. Knowledge acquisition for decision-
theoretic expert systems. In AISB Quaterly, 94: 23-33.
McShane, M., Nirenburg, S., 2003. Parameterizing and
eliciting text elements across languages. In Machine
Translation 18(2): 129-165.
McShane, M., Nirenburg, S., Beale, S., 2005. Semantics-
based resolution of fragments and underspecified
structures. In Traitement Automatique des Langues
46(1): 163-184.
McShane, M., Fantry, G., Beale, S., Nirenburg, S, Jarrell,
B., 2007a. Disease interactions in cognitive simula-
tions for medical training. In Proceedings of MODSIM
World Conference, Medical Track.
McShane, M., Nirenburg, S., Beale, S., Jarrell, B., Fantry,
G., 2007b. Knowledge-based modeling and simulation
of diseases with highly differentiated clinical manife-
stations. In Proceedings of the 11th Conference on Ar-
tificial Intelligence in Medicine.
McShane, M., Nirenburg, S., Beale, S., Catizone, R.,
Submitted. A cognitive architecture for simulating bo-
dies and minds. Submitted to ICAART-2011.
Nirenburg, S., McShane, M., Beale, S., 2008a. A simu-
lated physiological/cognitive “double agent”. In Pro-
ceedings of the Workshop on Naturally Inspired Cog-
nitive Architectures at AAAI 2008 Fall Symposium.
Nirenburg, S., McShane, M., Beale, S., Jarrell, B., 2008b.
Adaptivity in a multi-agent clinical simulation system.
In Proceedings of AKRR'08 - International and Inter-
disciplinary Conference on Adaptive Knowledge Re-
presentation and Reasoning.
Nirenburg, S., Raskin, V., 2004. Ontological semantics.
Cambridge, Mass., The MIT Press.
Schank, R., Abelson, R., 1977. Scripts, plans, goals and
understanding. Hillsdale, NJ, Erlbaum.
Shadbolt, N., Burton, M., 1995. Knowledge elicitation. In
Corlett, E.N., Wilson, J.R., (Eds.), Evaluation of hu-
man work. CRC Press.
KEOD 2010 - International Conference on Knowledge Engineering and Ontology Development
182
