
A FRAMEWORK TO SUPPORT KNOWLEDGE TRANSFER IN
THE SERVICE SECTOR
Simrn Kaur Gill, Paul Folan and Kathryn Cormican
College of Engineering and Informatics, National University of Ireland Galway, Galway, Ireland
Keywords: Knowledge Transfer, Knowledge Process, Service Sector.
Abstract: This paper introduces a framework for analysing and supporting knowledge transfer in healthcare services.
It argues that the individual is at the centre of the transfer process and, as such, needs to be catered-to within
both teams and organisations. Within the healthcare sector, safety is critical, and the effective and efficient
transfer of knowledge between healthcare professionals and patients can help to reduce the risks in the
system. Furthermore, the authors hope that a clear understanding and accurate identification of the factors
that impact the knowledge transfer process for individuals can have an impact on the knowledge transfer
process in teams and organisations. The development of a suitable approach to support knowledge transfer
for improved transfer of knowledge among these groups in the healthcare services is achieved using
technology where appropriate, through the knowledge transfer framework which is presented.
1 INTRODUCTION
The service sector has grown faster over the past few
years than any other sector in the global economy. It
now contributes a sizable percentage to the gross
domestic product of most countries (CREST R&D in
services Working Group, 2009, Eurostat, 2010). The
service sector of the economy is focused on people
interacting with people. The products of the service
sector are intangible, experience-based, and the
product is provided through personal interaction
(Straub and Karahanna, 1998, Davis, 2002).
Healthcare is part of the service sector, it is entirely
based on the interactions between individuals and
groups of professionals, be they clinicians, nurses,
patients or administrative staff.
The healthcare services are one of the most
knowledge-intensive sectors of the economy. It is
based on the generation, representation, accessibility
and transfer of knowledge between individuals,
teams and organisations. Effective and efficient
transfer of knowledge can assist healthcare services
in the control of cost, time and improving the quality
of the services provided. Knowledge transfer is seen
as crucial to the management of knowledge in an
organisation (Argote and Ingram, 2000, Lahti and
Beyerlein, 2000). During the past number of years
researchers have carried out numerous studies on the
effects of knowledge transfer, both internally and
externally to the organisation (Gilbert and Cordey-
Hayes, 1996, Moreland and Mayaskovsky, 2000). In
these studies, efficient and effective knowledge
transfer has been recognised as being one of the
critical success factors to successful knowledge
management (Lahti and Beyerlein, 2000).
The main objective of this research is to improve
the effectiveness of the knowledge transfer process
in the healthcare sector. Firstly by providing a
holistic understanding of the knowledge transfer
processes in relation to the factors that have an
impact on the process. Secondly by facilitating the
effective and efficient transfer of knowledge
between both the sender and receiver in the process
to identify and analyse the needs and requirements,
and adaptations necessary to meet them. In
particular the research will provide guidance and
support to individuals in the transfer process with
regard to the needs and requirements of the sender
and recipient. From our study the following needs
have been identified (a) an individual-centred
approach to knowledge transfer; (b) informed
decision-making; (c) effective use of information
and knowledge; (d) effective mechanism for
knowledge transfer and (e) effective use of
technology to support knowledge transfer. Through
358
Kaur Gill S., Folan P. and Cormican K..
A FRAMEWORK TO SUPPORT KNOWLEDGE TRANSFER IN THE SERVICE SECTOR.
DOI: 10.5220/0003097703580362
In Proceedings of the International Conference on Knowledge Management and Information Sharing (KMIS-2010), pages 358-362
ISBN: 978-989-8425-30-0
Copyright
c
2010 SCITEPRESS (Science and Technology Publications, Lda.)

the knowledge transfer framework support is
provided to both the sender and recipient in the
knowledge transfer process.
2 KNOWLEDGE TRANSFER
Knowledge transfer is of particular importance due
to the knowledge growth potential that occurs during
the transfer of knowledge from one individual to
another, and also from one organisation to another
(Argote and Ingram, 2000, Sveiby, 2001). Gilbert
and Cordey-Hayes (1996) propose a four stage
process towards achieving knowledge growth
potential during knowledge transfer; acquisition (the
gathering of knowledge from various sources),
communication (the distributing of this knowledge),
application (the applying of knowledge so that it is
retained) and assimilation (the result of applying the
knowledge). Knowledge transfer is not an easy
process to achieve; it is hindered at each stage in the
process as problems that occur during the stages are
not identified until the next stage begins (Argote and
Ingram, 2000, Levine and Moreland, 2000). To date
research in the area has focused on developing
individual tools to support specific area of
knowledge transfer in healthcare services. This
research seeks to develop a unified approach to
knowledge transfer in healthcare services.
3 RESEARCH METHOD
A research approach developed by Cormican and
O’Sullivan (2003) was followed.
Phase 1: Foundation. A review of literature relating
to knowledge transfer was carried out. The scope of
the review was literature in relation to knowledge
transfer definitions, concepts, scenarios and
applications. The objective of the knowledge
transfer framework is to assist the sender and
receiver in the knowledge transfer process. This is
accomplished through the framework supporting
analysis, design, development and implementation in
the process.
Phase 2: Induction. After an evaluation of the
various definitions, concepts, scenarios and
applications on knowledge transfer, a refinement of
the initial ideas from the foundation phase were
made. The refinement focused on knowledge
transfer features, characteristics and technologies.
Initial solutions were formulated in relation to the
case studies.
Phase 3: Iteration. Foundation and induction
phases were repeated a number of times to refine
and develop the initial framework. The ideas
generated were analysed and refined until the
components of the framework that are illustrated in
section 4 were developed.
Phase 4: Presentation. A summary of the
knowledge transfer framework is presented,
explained and discussed in section 4. These initial
tools will be presented to the case studies and will be
used to provide a systematic approach to analysing
the knowledge transfer process.
Phase 5: Verification. As is highlighted previously
the framework will be evaluated and verified within
a healthcare services case study. This will be
completed through empirical testing of the
framework tools during the acquisition,
communication, application and assimilation stages
of the knowledge transfer in the case study.
4 KNOWLEDGE TRANSFER
FRAMEWORK
Following the review of various knowledge transfer
methods and techniques along with classification
systems, a framework for supporting the transfer
process is presented. The framework is designed to
be used by healthcare professionals in transferring
knowledge more effectively and efficiently to other
healthcare professionals and patients. This
framework is called the Knowledge Transfer (KT)
Framework. The KT framework applies a systems
approach to analysing, designing, developing and
implementing knowledge transfer in processes. The
framework is made up of both theoretical structures
and practical techniques to enable more effective
and efficient knowledge transfer (see Figure 1).
These tools are:
• Best practice
The best practice element of the tool set incorporates
findings from numerous areas of research. These
include cognitive psychology, organisational
strategy, and organisational behaviour and
technology innovation in the area of user-centred
development. The knowledge transfer process is
cyclical and is constantly occurring. The findings
from the literature are incorporated to create a best
practice document that provides guidelines for
effective and efficient knowledge transfer. The best
practice document is examined with regard to the
following areas: acquisition, communication,
application and assimilation.
A FRAMEWORK TO SUPPORT KNOWLEDGE TRANSFER IN THE SERVICE SECTOR
359
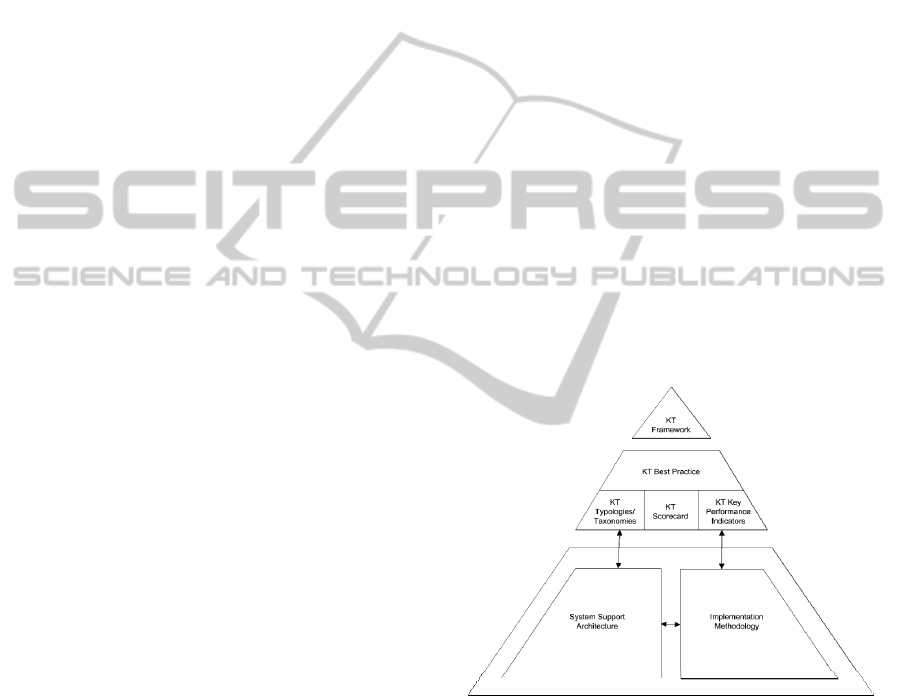
• Typologies and taxonomies
Typologies are groupings of models, which describe
different aspects of the same characteristics. The
models create a visual representation of the key
areas that need to be considered in the process and
also represent the level of interaction and overlap
between them. The typologies and taxonomies
examine three areas: individual knowledge
management; technology innovation for supporting
knowledge transfer; and knowledge transfer for
individuals, teams and organisation.
• Scorecard
There are numerous factors that can affect the
success of the knowledge transfer process.
Understanding the sender and recipient in the
process assists in evaluating the quality and
effectiveness of the knowledge that has been
transferred. An understanding of the acquisition,
communication, application and assimilation during
the knowledge transfer process must also be
realised. The human, process, and technical
environment, need to be considered with regard to a
successful knowledge transfer process. A set of four
indicators are suggested by the author to assist in a
successful knowledge transfer process. They can
also be used to assess the absorptive capacity of the
individual, and to identify the areas where the
knowledge transfer process was deficient. The four
key stages include acquisition, communication,
application and assimilation. Each of these stages is
further evaluated under need, habit, emotion, context
awareness, individual centred, sensitive and
responsive, and intuitive and adaptive.
• Key performance indicators
The key performance indicators can be used to
quantify knowledge transfer performance in
assessing the effectiveness and efficiency of the
process. In developing the performance indicators, a
combined structural and procedural framework is
applied. This combined approach incorporates the
various elements of the best practice, typologies and
taxonomies, as well as the scorecard. In developing
the performance indicators Thorndike and Hagen
(1977) three steps for test measurement have been
followed, (a) identify and define the quality or
attribute to be measured; (b) determine a set of
operations by which the attribute may be made
manifest and perceivable and (c) establish a set of
procedures or definitions for translating observations
into quantitative statements of degree or amount.
In adhering to these three principles it is hoped that
this will protect the validity of the measurement
process, particularly when attempting to measure
some aspect of human behaviour in areas where
“there is no single universally accepted test”
(Thorndike and Hagen, 1977).
• System support architecture
System support architecture is needed to provide a
systematic approach to knowledge transfer for
individuals, teams and organisations. The
architecture needs to be designed to incorporate best
practice, typology and taxonomy, check sheet and
scorecard, and the key performance indicators. The
ARIS house is used to incorporate these tools. The
ARIS house (Scheer, 1998) incorporates five
elements, organisation, data, control, function and
output.
• Implementation methodology
The methodology incorporates the tools outlined
above in a unified approach that can be applied in
the services sector of the economy in a structured
approach.
The tools that make up the framework are not
definitive and will change through further
development and application in the case study. The
aim of this research is to add to the knowledge base
in the areas outlined, provide guidance with regard
to knowledge transfer in the service sector and to
encourage further research in the area.
Figure 1: Knowledge transfer framework.
5 CASE STUDY
Healthcare is a particularly important area of the
public sector that has to adapt to meet the changing
needs of society. Therefore knowledge transfer
within healthcare services is safety critical during
transitions of care. Transitions of care in healthcare
refer to the “specific interactions, communications
and planning required for patient to safely move
from one service or setting to another” (Society of
KMIS 2010 - International Conference on Knowledge Management and Information Sharing
360

Hospital Medicine, 2006). The transitions occur
during the transfer of patients from inpatients to
outpatients. It can also be seen in acute care
transfers. These can take place between acute care
and/or sub-acute and/or non-acute care facilities.
The aim of the healthcare professionals is to
“provide leadership to promote efficient, safe
transitions of care to ensure patient safety, reduce
loss of information, and maintain the continuum of
care” (Society of Hospital Medicine, 2006). If there
is a breakdown during the transition of care, this can
result in patient dissatisfaction and poor healthcare
outcomes due to fragmented care. The aim is to
provide continuity of care (Harrison, 2004). If
transitions of care are not made efficiently and
effectively between care providers, it can have a
detrimental effect on the patient (Beach et al., 2003).
Transitions of care cannot be achieved without
collaboration between the various healthcare
providers (Thornhill et al., 2008) during knowledge
transfer. The research hopes to reduce the risks that
occur during transitions of care due to problems
arising in the transfer of knowledge between
stakeholders.
6 IMPLICATIONS AND NEXT
STEP
Knowledge is viewed by organisations as a
significant resource that can be utilised to achieve a
competitive advantage in the market place. To
achieve this requires the effective and efficient
management of knowledge. This can be achieved
through: (a) improved economic management; (b)
improved visibility of customer requirements; (c)
improved visibility of future trends; (d) improved
traceability and learning through previous
experience; (e) improved communication across
geographically distributed offices and the supply
chain; (f) improved absorption of tacit knowledge
and (g) improved informal culture of knowledge
transfer. The benefits of knowledge management are
achieved through the efficient and effective
management of the knowledge process. These
potential benefits can be facilitated through
improved support prior to, during, and after
knowledge transfer. The framework that has been
described in this paper needs to be applied and
validated in a case study. Then the potential benefits
need to be evaluated against achieved gains.
7 CONCLUSIONS
Knowledge transfer is the process of transferring
knowledge from one individual to another. The
process is not always analysed, designed, developed
or implemented. Knowledge transfer has two main
issues that need to be considered. First the processes
involved in knowledge transfer and the factors that
impact on it. Secondly the factors and issues that
impact on the transfer of knowledge being effective
and efficient for both the sender and the receiver.
The development of a suitable approach to support
improved transfer of knowledge among these groups
in healthcare services is achieved through the
knowledge transfer framework. The framework
includes a suite of tools that assist in supporting the
knowledge transfer process at an individual level.
This allows for an evaluation of the process at
various stages, which provides for more effective
adaption to changes as they occur.
ACKNOWLEDGEMENTS
This work has been partly funded by the National
University of Ireland, Galway, College of
Engineering Postgraduate Fellowship.
REFERENCES
Argote, L. & Ingram, P., 2000. Knowledge Transfer: A
Basis for Competitive Advantage in Firms
Organizational Behaviour and Human Decision
Processes, 82, 150-169.
Beach, C., Croskerry, P. & Shapiro, M., 2003. Profiles in
Patient Safety: Emergency Care Transitions. Academic
Emergency Medicine, 10, 364-367.
Cormican, K. & O'sullivan, D., 2003. A scorecard for
supporting enterprise knowledge management.
Journal of Information and Knowledge Management,
2, 191-201.
Crest R&D in Services Working Group, 2009. Promoting
the Role of R&D in Services: A report of the CREST
OMC 3% Working Group “R&D in Services”.
Luxembourg.
Davis, G.B., 2002. Anytime/Anyplace Computing and the
Future of Knowledge Work. Communications of the
ACM, 45, 67-73.
Eurostat, 2010. Quarterly Panorama of European business
statistics (1-2010). Luxembourg: E. Commission.
Gilbert, M. & Cordey-Hayes, M., 1996. Understanding the
process of knowledge transfer to achieve successful
technological innovation. Technovation, 16, 301-312.
A FRAMEWORK TO SUPPORT KNOWLEDGE TRANSFER IN THE SERVICE SECTOR
361

Harrison, M.B., 2004. Guest Editorial: Transitions,
Continuity, and Nursing Practice. Canadian Journal of
Nursing Reserch, 36.
Lahti, R.K. & Beyerlein, M.M., 2000. Knowledge
Transfer and Management Consulting: A look at "The
Firm". Business Horizons, 43, 65-74.
Levine, J.M. & Moreland, R.L., 2000. Knowledge
Transfer in Organisations: Learning from the
Experience of Others. Organizational Behaviour and
Human Decision Processes, 82, 1-8.
Moreland, R.L. & Mayaskovsky, L., 2000. Exploring the
Performance Benefits of Group Training: Transactive
Memory or Improved Communication? .
Organizational Behaviour and Human Decision
Processes, 82, 117-133.
Scheer, A.W., 1998. ARIS - Business Process Framework,
Second ed. Berlin: Springer-Verlag.
Society of Hospital Medicine, 2006. The core
competencies in hospital medicine: A framework for
cirriculum development (Supplement). Journal of
Hospital Medicine, 1, 2-95.
Straub, D. & Karahanna, E., 1998. Knowledge Worker
Communications and Recipient Availability: Toward a
Task Closure Explanation of Media Choice.
Organization Science, 9, 160-175.
Sveiby, K.-E., 2001. A knowledge-based theory of the
firm to guide in strategy formulation. Journal of
Intellectual Capital, 2, 344-358.
Thorndike, R.L. & Hagen, E.P., 1977. Measurement and
evaluation in psychology and education, 4th ed. New
York: Wiley.
Thornhill, J., Dault, M. & Clements, D., 2008. Ready, Set
...Collaborate? The Evidence Says "Go", So What's
Slowing Adoption of Inter-professional Collaboration
in Primary Healthcare Healthcare Quarterly, 11, 14-
16.
KMIS 2010 - International Conference on Knowledge Management and Information Sharing
362
