
RECORDING SPEECH SOUND AND ARTICULATION IN MRI
Daniel Aalto, Jarmo Malinen, Pertti Palo
Dept. of Mathematics and Systems Analysis, Aalto University, P.O. BOX 11100, FI-00076 Aalto, Finland
Olli Aaltonen, Martti Vainio
Institute of Behavioural Sciences, University for Helsinki, P.O. BOX 9, FI-00014 Helsingin yliopisto, Finland
Risto-Pekka Happonen, Riitta Parkkola, Jani Saunavaara
Dept. of Oral Diseases, Dept. of Radiology, Medical Imaging Center of Southwest Finland
University of Turku, FI-20014 Turun yliopisto, Finland
Keywords:
MRI, Sound recording, Speech, Vowel, Formant.
Abstract:
This article describes an arrangement for simultaneous recording of speech and the geometry of vocal tract.
Experimental design is considered from the phonetics point of view. The speech signal is recorded with an
acoustic-electrical arrangement and the vocal tract with MRI. Finally, data from pilot measurements on vowels
is presented, and its quality is discussed.
1 INTRODUCTION
Helmholtz (1863) put forward the acoustic theory of
vowels by showing that the perceived vowel quality
depends on the resonance characteristics of the vo-
cal tract. Since then, it has been the main approach
to the acoustic theory of speech production (see, e.g.,
(Fant, 1960)). Based on these ideas, Mrayati, Carr,
and Guerin (1988) presented the Distinctive Regions
Model (DRM) of speech production suggesting that
speech production derives from regions that closely
correspond to established vowel and consonant places
of articulation.
Based on these earlier ideas, models, and theories,
it is hypothesized that the vocal tract configuration
can be estimated strictly on the basis of the formant
structure. Here we present a data acquisition frame-
work for a mathematical model that not only solves
the direct problem of simulating speech sound from
a given 3D vocal track configuration, but also allows
the prediction of vocal tract shapes on the basis of res-
onances corresponding to vowel formants — the main
information bearing parameters in speech.
Such simulators (comprising only of the wave
equation in the vocal tract) have been used for
studying normal speech production acoustics (Han-
nukainen, Lukkari, Malinen, & Palo, 2007; Lu,
Nakai, & Suzuki, 1993;
ˇ
Svancara, Hor´aˇcek, & Peˇsek,
2004). When soft tissue and muscle models are in-
corporated, we expect that such a simulator is use-
ful for studying speech production from a wider pho-
netics point of view, and planning and evaluating
oral and maxillofacial surgery (Dedouch, Hor´aˇcek,
Vampola, &
ˇ
Cern´y, 2002; Nishimoto, Akagi, Kita-
mura, & Suzuki, 2004;
ˇ
Svancara & Hor´aˇcek, 2006).
See also Vahatalo, Laaksonen, Tamminen, Aaltonen,
and Happonen (2005) and Niemi, Laaksonen, Pel-
tomaki, Kurimo, Aaltonen, and Happonen (2006) for
background.
A computational model of speech production
(such as discussed in Hannukainen et al. (2007), Aalto
(2009), and Aalto, Alku, and Malinen (2009)) must
be validated by comparing simulated sound to mea-
sured sound in some metric (such as the resonance
structure, i.e., the formants). Since the simulation is
based on anatomic data, the validation of the compu-
tational model depends on recording a coupled data
set: the speech sound and the precise anatomy which
produces it. This requires imaging the vocal and nasal
tracts from the lips and nostrils to the beginning of the
trachea. We chose to use magnetic resonance imaging
(MRI) technique because of its safety in contrast to X
168
Aalto D., Malinen J., Palo P., Aaltonen O., Vainio M., Happonen R., Parkkola R. and Saunavaara J..
RECORDING SPEECH SOUND AND ARTICULATION IN MRI.
DOI: 10.5220/0003137301680173
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2011), pages 168-173
ISBN: 978-989-8425-37-9
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

ray based CT-imaging.
Using MRI poses many restrictions. When a full
3D scan of the vocal tract is desired, the acquisition
time will necessarily be long. During this time, the
test subject needs to remain stationary; in particular,
all the parts of the speech apparatus have to remain
as stable as possible as well as the fundamental fre-
quency (f
0
). We discuss these matters in Sections 3
and 4. On the other hand, the test subject’s voice
is recorded simultaneously when his
1
vocal tract is
scanned using MRI. This sound recording is carried
out using an arrangement that has already been re-
ported by Lukkari, Malinen, and Palo (2007), and Ma-
linen and Palo (2009). For previous work on simi-
lar projects, see, for example,
ˇ
Svancara et al. (2004),
Ericsdotter (2005), and Bresch, Nielsen, Nayak, and
Narayanan (2006).
The purpose of this paper is to outline experimen-
tal protocols for acquiring the above mentioned data
sets in high quality, discuss these protocols from a
wide range of perspectives, and finally present some
observations based on pilot data.
2 SPEECH RECORDING
2.1 Phonetic Materials
From an articulatory point of view, the main prob-
lem in acquiring simultaneous MRI and audio data
is the subject’s ability to alter their articulatory set-
tings very effectively in a manner that retains the main
acoustic characteristics of the speech sounds. It is
well known that human subjects adapt their motor be-
havior regarding both vision and audition (Houde &
Jordan, 1998; Kelso, Tuller, Vatikiotis-Bateson, &
Fowler, 1984). With regard to speech articulation, the
adaptation of motor behavior is particularly important
since the production goals (i.e., speech sounds) occur
in numerous different articulatory contexts. There-
fore, it can be expected that speakers are forced to
adapt their articulation even during sustained vowel
production as their articulatory setup changes due to,
e.g., the contraction of the thorax. This causes addi-
tional problems when both MRI and audio data are
acquired simultaneously and calls for careful design
of the speech materials.
There are two main sources for adaptation in sus-
tained vowel production: (1) the changing position of
the larynx due to changes in fundamental frequency,
1
We shall use a male subject in the pilot stage as analyz-
ing a male voice is generally easier than analyzing a female
voice.
cue signal MRI sequence
speech beginning speech end
Time (s)
0
14.298
Frequency
Figure 1: A spectrogram showing a full sound recording.
From left to right: cue signal for the subject (≈ 3.5 s from
the signal onset, overlapping speech for the last ≈ 500 ms);
the clean speech sample (≈ 500 ms); the speech and the
imaging noise (≈ 8 s); and the clean speech sample (≈
500 ms).
and (2) the changing shape of the vocal organs due
to the contracting thorax during a long exhalation.
The first problem can be circumvented by having the
subject produce the sustained vowels with a station-
ary fundamental frequency (f
0
). The second problem
cannot be completelety avoided and it calls for other
means to control the matching of MRI and audio data.
A partial solution is to measure the articulatory move-
ments during the vowel production.
With the above problems in mind, we designed
a plan according to which the subject was asked to
produce the sustained vowels with two different sta-
tionary f
0
levels (110 and 137.5 Hz; corresponding to
notes A2 and C#3, respectively). Furthermore, two
separate MRI imaging techniques were used: (1) a
stationary 3D image of the vocal tract was produced;
and (2) a dynamic 2D image showing the sagittal sec-
tion of the vocal tract during the vowel production.
The two f
0
levels were used to study the effect of lar-
ynx position on the vocal tract shape whereas the dy-
namic 2D image sequence was used to study the effect
of the changing vocal tract shape due to the contract-
ing thorax.
2.2 Experimental Setting
Before the imaging sequence starts, the subject lies
inside the machine in supine position in the same way
as during a standard MRI procedure of the head and
neck area. In addition, the sound collector is placed
upon the MRI coil, and it is positioned in front of test
subject’s mouth. The subject is able to speak to the
control room through the sound collector all the time.
Moreover, he can hear instructions from the control
room as well as his own (de-noised) voice (with a de-
lay of ≈ 20 ms due to acoustic wave guides) through
earphones of the MRI machine.
Before the experiment, the subject is given a de-
RECORDING SPEECH SOUND AND ARTICULATION IN MRI
169

scription of what he is asked to do next. When the
subject indicates that he is ready the experiment is
started. First, the subject hears a sinusoidal cue signal
that gives him a count-down for starting the utterance
at the right time as well as the desired pitch, i.e., the
level of f
0
.
A typical sound sample, including the cue signal,
is represented in Figure 1. The MRI machine is op-
erated so that a 500 ms “pure sample” of stabilized
utterance is obtained immediately before and right af-
ter the MRI noise interval.
After each experiment, the image data is inspected
visually and the subject gives his comments. During
the whole imaging sequence the sound sample is lis-
tened by a trained phonetician in the control room,
and unsuccessful utterances are usually detected im-
mediately. Particular attention is paid to the phonation
type and nasality. When doubt arises, the formants of
the sample are extracted from the two “pure samples”
using Praat 4.6.15; see Figure 3 below.
2.3 Imaging Sequence
Experiments were performed on a Siemens Magne-
tom Avanto 1.5T scanner (Siemens Medical Solu-
tions, Erlangen, Germany). Maximum gradient field
strength of the system is 33 mT/m (x,y,z directions)
and the maximum slew rate is 125 T/m/s.
12-element Head Matrix Coil was combined with
the 4-element Neck Matrix Coil in order to com-
pletely cover the anatomy of interest. Coil configura-
tion allowed the use of Generalized Auto-calibrating
Partially Parallel Acquisition (GRAPPA) technique to
accelerate acquisition. Technique was applied in all
the scans using acceleration factor 2.
3D VIBE (Volumetric Interpolated Breath-hold
Examination) was found out to be the most suitable
MRI sequence for the rapid 3D acquisition required in
this study. Basically, 3D VIBE is an ultra-fast gradi-
ent echo sequence with an isotropic resolution. In ad-
dition, the k-space scan is typically performed asym-
metrically in this sequence, which reduces the num-
ber of phase encoding steps in the slice-selection di-
rection leading to faster scan times. As the naming
of the sequence suggests, it was originally developed
for fast 3D imaging of the abdominal region where
breath-hold during the scan is essential. Sequence
parameters were optimized in order to minimize the
acquisition time. The following parameters allow
imaging with 1.8 mm isotropic voxels in just 7.6 s:
Time of repetition (TR) was 3.63 ms, echo time (TE)
1.19 ms, flip angle (FA) 6
◦
, receiver bandwidth (BW)
600 Hz/pixel, FOV 230 mm, matrix 128x128, number
of slices 44 and the slab thickness of 79.2 mm.
When higher resolution is required, imaging with
1.2 mm isotropic resolution is possible in 17 s when
following changes to parameters are applied: TR
3.95 ms, TE 1.34 ms, matrix 192x192, and 64 slices.
Dynamic MRI scans were performed using seg-
mented ultrafast spoiled gradient echo sequence (Tur-
boFLASH) where TR and TE were minimized. This
sequence is typically used in cardiac studies but this
time magnetization preparation pulse was not applied.
Single sagittal plane was imaged with a pace of 5.5
images per second using parameters TR 178 ms, TE
1.4 ms, FA 6
◦
, BW 651 Hz/pixel, FOV 230 mm, ma-
trix 120x160, and slice thickness 10 mm.
2.4 Sound Recording
The MRI room presents a challenging environment
for sound recording. Use of metal components and
electronics is restricted inside the MRI room, and it is
completely excluded near the MRI machine for safety
and image quality reasons.
We use the sound recording arrangement detailed
in Lukkari et al. (2007), and Malinen and Palo (2009):
A two-channel sound collector samples the speech
and noise signals in a dipole configuration. The sound
collector is an acoustically passive, non-microphonic
device which does not cause artifacts in the MR im-
ages, and it is also transparent in X-Ray CT. The
sound signals are coupled to a RF-shielded micro-
phone array by acoustic waveguides of length 3 m.
Again, the waveguides are acoustically passive and
linear, but their frequency response is far from flat
because of the longitudinal resonances that, how-
ever, have been satisfactorily controlled by special
impedance terminations at both ends of the wave
guides. The microphone array inside its Faraday cage
lies at a safe distance from the main coil of the MRI
machine. The signals are coupled from the micro-
phone array to custom RF-proof amplifier that is situ-
ated outside the MRI room. These analogue electron-
ics are used to optimally substract the noise channel
from the speech channel in real time.
The audio signal is digitized using a Digidesign
M-Box model 1, 24bit ADC, controlled by a Mac-
BookPro2,2 computer running MacOSX 10.4.9 and
Pro Tools LE 7.3.1.
2.5 Acoustic Noise in the MRI Room
Loud acoustic noise is familiar to anyone who has
undergone an MRI study. The noise originates from
the vibrations of the gradient coil support structure.
These vibrations are caused by the interactions be-
tween the pulsed magnetic fields created in gradient
BIODEVICES 2011 - International Conference on Biomedical Electronics and Devices
170
coils and the main magnetic field.
The dipole sound collector and the analog noise
cancellation (as described in Section 2.4) takes care
of a good part of the noise at low frequencies, say
< 500 Hz. In particular, we are able to obtain sound
recordings of vowel utterances in real time, most of
which have positive S/N ratios during the MRI noise.
However, we are not always able to produce a signal
that would be directly (without further de-noising) us-
able for formant extraction by, e.g., the linear predic-
tion algorithm.
For DSP-based post-processing, we record a noise
sample from each MRI sequence and configuration
used. During these recordings, the test subject lies
silently inside the MRI machine so that the acoustic
conditions are the same as in actual speech record-
ings. For comparison, some noise samples are also
collected by a directional microphone ≈ 3 m away
from the MRI machine. The frequency response of
the acoustic wave guides is measured in an anechoic
chamber. For further details, and for post-processing
and analysis of the data we refer to Aalto, Aaltonen,
Happonen, Malinen, Palo, Parkkola, Saunavaara, and
Vainio (2011).
The acoustic MRI noise is significantly different
for different imaging sequences. Ultrafast sequences
— such as 3D VIBE used in this work — require max-
imal performance of gradient system both in terms of
slew rate and amplitude. This results in exceptionally
loud acoustic noise. We remark that even smallest
changes in parameters of a given MRI sequence may
change acoustic noise significantly. It is thereby es-
sential to maintain sequence parameters and patient
positioning constant.
3 RESULTS
For successful data acquisition, it is necessary to iden-
tify relevant parameters concerning the whole exper-
imental setting that must be kept track of at all times.
It is not always a priori clear what should be regarded
as a relevant parameter, or what practical steps must
be taken to keep them under control.
Here, the relevant parameters can be divided into
two groups: (1) physiological parameters involving
the human subject; and (2) physical parameters of
the measurement equipment. As documented in Sec-
tions 2.2 – 2.5 above, we have spent much effort to
optimize and standardize physical parameters which,
indeed, we can control for, measure and compensate
to a considerable extent. Some physiological param-
eters have been considered in Section 2.1, and they
have a much more problematic nature. We proceed to
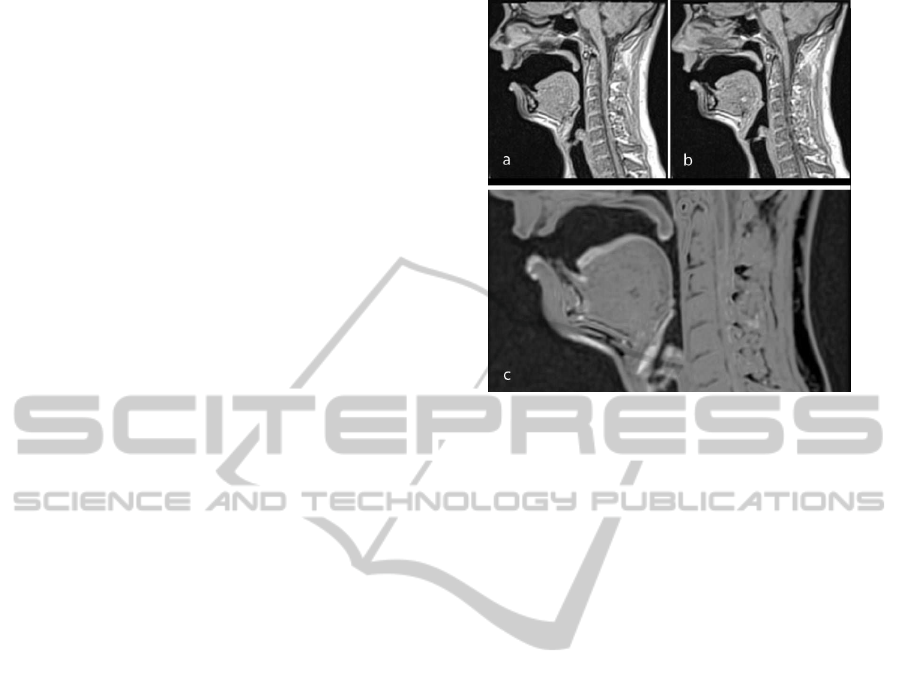
Figure 2: Mid-sagittal sections of an 8 s production of the
vowel [A] with a) f
0
= 110 Hz; and b) f
0
= 137.5 Hz. An
overlaid image is shown in c) to indicate their difference that
is visible as lighter gray. Notice in particular the difference
in position of lower lip, tongue blade and larynx.
discuss them in terms of our pilot experiments.
Let us start with the level of f
0
. The subject was
instructed to keep f
0
in a given reference value, and
he was able to do that with an error of ± 3 Hz in all
experiments. Figure 2 indicates that different levels
of f
0
result in visible differences of vocal tract con-
figuration while uttering the vowel [A].
We remark that changes in sound pressure may re-
sult in a similar change as in Figure 2. To exclude
this, the subject tried to keep the sound pressure same
in both imaging sessions, but he did not receive any
feedback in that respect. However, the (subjective)
exhalation time was of the same length in both mea-
surements. After recording and compensating the fre-
quency response of the whole setup, the sound pres-
sure levelcan be extracted from recorded signals quite
precisely. It can be observed that the sound pressure
given by the subject always increases towards the end
of the sample.
The measured formants of [A] (corresponding to
the experiment giving Figure 2) are given in (F
1
, F
2
)
-plane in Figure 3. As explained in Section 2.2, we
obtain two “pure samples” of speech, and we there-
fore have two points (connected by a line) for each
experiment in Figure 3. We have used both 7.6 s and
17 s imaging sequences, two f
0
levels, and several
phonation types.
Let us next discuss the changing of shape of vo-
cal organs. Figure 3 gives us a first indication that
the vocal tract geometry somewhat “creeps” for some
reasons during the 7.6 s MRI scan. We measured this
RECORDING SPEECH SOUND AND ARTICULATION IN MRI
171

600 650 700 750 800
1000
1050
1100
1150
1200
F1 / Hz
F2 / Hz
/a/ 137.5 Hz, 8s
/a/ 110 Hz, 8s
/a/ 110 Hz, 18s
/a/ 110 Hz, breathy, 8s
Figure 3: Formants of the vowel [A] produced with f
0
=
110 Hz and f
0
= 137.5 Hz based on 500 ms samples from
the beginning (marked with *) and the end (marked with o)
of the sustained phonation. During these samples the MRI
sequence was not active.
phenomenon for vowel [æ] directly using a dynamic
MRI sequence in the sagittal plane; see Figure 4.
Figure 4 indicates quite large changes in both the
mouth and pharyngeal cavities caused by the different
position of the larynx during a long exhalation; in Fig-
ure 2(c) there is in addition a (phantom) doubling in
the size of the vocal folds. That the larynx has moved,
is also supported by the movement of vocal folds that
can be observed from Figure 4. As explained in Sec-
tion 2.1, some movement is to be expected because of
the contracting thorax. A part of the observed changes
may, however,be due to changing aerodynamicforces
in the vocal tract that arise from variable air flow dur-
ing the MRI scan.
We note that the formants are considered as purely
acoustic parameters of the vocal tract geometry, and
— as such — they do not depend directly on dynamic
variables such as the sound pressure and the air flow
but, instead, through detectable changes in vocal tract
geometry including the time-dependent acoustic ter-
mination due to the vocal folds. It is not clear whether
one should (for physically motivated reasons) aim at
constant sound pressure or at constant air flow in a
measurement leading to Figure 3. We remark, how-
ever, that observing the flow inside the MRI machine
is probably very challenging.
4 CONCLUSIONS
We have described experimental protocols, MRI se-
quences, and a sound recording system that can be
used for simultaneous sound and anatomical data ac-
Figure 4: Overlaid image showing the difference between
the first and last frame of the 8 s dynamic image sequence
of [æ] with f
0
= 137.5 Hz. Differences are visible as lighter
gray.
quisition of human speech. The results and experi-
ences of a pilot experiment on vowel formants and
the corresponding vocal tract geometries have been
reported. Such data sets are intended for parameter
estimation, fine tuning, and validation of a mathemat-
ical model for speech production as discussed in Sec-
tion 1. However, these methods have a wide range of
applications in phonetics and medicine.
Phonetic Remarks and Observations
The MR imaging poses severe problems with regard
to both speech production by the test subject and
sound recording. The MRI requires long sustained
vowel production and — at the same time — it pro-
duces high levels of acoustic noise which masks the
speech sound.
The phonetic and articulatory problems stem from
the inability of a subject to maintain a stable vocal
tract shape long enough: there is a trade-off between
image quality in terms of resolution and speech pro-
duction “quality” in terms of articulatory stability.
The duration of an MRI scan (such as considered in
Section 2.3 above) is 7.6–17 s, and the sound record-
ing time is ≈ 2 s longer than that; see Figure 1. The
subject should be able to maintain constant position,
configuration of the vocal organs, all sound charac-
teristics, and the type of phonation during the whole
period. According to our experience, this is a difficult
requirement even for a healthy subject.
We designed a set of recording materials to ad-
dress these problems phonetically as well as possi-
ble. Our work indicates that the problems cannot be
circumvented altogether. There are, however, simple
BIODEVICES 2011 - International Conference on Biomedical Electronics and Devices
172

means to further improve articulatory stability during
recordings. We propose, at least, the following:
1. The test subject should be familiar with the MRI
noise as well as the cue signal so as to perform
optimally in the experimental situation.
2. The intensity of the cue signal should match the
MRI noise so that the initial voice production can
be maintained, i.e., possible sound intensity fluc-
tuation should be avoided.
3. The MRI noise itself is periodic and interferes
with the voice f
0
when they are close. Hence, the
cue should be matched with the MRI noise fre-
quency profile.
4. The voice sample f
0
should be standardized but in
a way that depends on the test subject.
5. The cue signal should be longer to allow the sub-
ject more time to inhale.
6. Externally triggered MRI sequences can be used
to introduce noiseless pauses.
All in all, the results from the current experiment are
encouraging. They clearly point to directions where
the setup refinements and better understanding will
iteratively approach a useful solution to the whole
problem.
REFERENCES
Aalto, A. (2009). A low-order glottis model with
nonturbulent flow and mechanically coupled acoustic
load. Master’s thesis, TKK, Helsinki. Available at
http://math.tkk.fi/research/sysnum/.
Aalto, A., Alku, P., & Malinen, J. (2009). A LF-pulse from
a simple glottal flow model. MAVEBA 2009 (pp. 199–
202). Florence, Italy.
Aalto, D., Aaltonen, O., Happonen, R., Malinen, J., Palo,
P., Saunavaara J., & Vainio, M. (2011). Recording
speech sound and articulation in MRI. Analysis and post-
processing of audio-spatial data. In preparation.
Branderud, P. (2008). Personal communication.
Bresch, E., Nielsen, J., Nayak, K., & Narayanan, S. (2006).
Synchronized and noise-robust audio recordings during
realtime magnetic resonance imaging scans (L). Jour-
nal of the Acoustical Society of America, 120(4), 1791 –
1794.
Dedouch, K., Hor´aˇcek, J., Vampola, T., &
ˇ
Cern´y, L. (2002).
Finite element modelling of a male vocal tract with con-
sideration of cleft palate. Forum Acusticum. Sevilla,
Spain.
Ericsdotter, C. (2005). Articulatory-Acoustic Relationships
in Swedish Vowel Sounds. PhD thesis, Stockholm Uni-
versity, Stockholm, Sweden.
Fant, G. (1960). Acoustic Theory of Speech Production.
Mouton, The Hague.
Hannukainen, A., Lukkari, T., Malinen, J., & Palo, P.
(2007). Vowel formants from the wave equation. Jour-
nal of the Acoustical Society of America Express Letters,
122(1), EL1–EL7.
Helmholtz, H. L. F. (1863). Die Lehre von den Tonempfind-
ungen als physiologische Grundlage fr dieTheorie der
Musik. Braunschweig: F. Vieweg.
Houde, J., & Jordan, M. (1998). Sensorimotor adaptation
in speech production. Science, 279(5354), 1213.
Kelso, J., Tuller, B., Vatikiotis-Bateson, E., & Fowler, C.
(1984). Functionally specific articulatory adaptation to
jaw perturbations during speech: Evidence for coordi-
native structures. Journal of Experimental Psychology,
10(6), 812–832.
Lu, C., Nakai, T., & Suzuki, H. (1993). Finite element sim-
ulation of sound transmission in vocal tract. J. Acoust.
Soc. Jpn. (E), 92, 2577 – 2585.
Lukkari, T., Malinen, J., & Palo, P. (2007). Recording
Speech During Magnetic Resonance Imaging. MAVEBA
2007 (pp. 163 – 166). Florence, Italy.
Malinen, J., & Palo, P. (2009). Recording speech during
MRI: Part II. MAVEBA 2009 (pp. 211–214). Florence,
Italy.
Mrayati, M., Carr, R., & Guerin, B. (1988). Distinctive
regions and modes: a new theory of speech production.
Speech Communication, (7), 257–286.
Niemi, M., Laaksonen, J., Peltomaki, T., Kurimo, J., Aalto-
nen, O., & Happonen, R. (2006). Acoustic comparison
of vowel sounds produced before and after orthognathic
surgery for mandibular advancement. Journal of Oral &
Maxillofacial Surgery, 64(6), 910–916.
Nishimoto, H., Akagi, M., Kitamura, T., & Suzuki, N.
(2004). Estimation of transfer function of vocal tract ex-
tracted from MRI data by FEM. The 18th International
Congress on Acoustics, Vol. II (pp. 1473 –1476). Kyoto,
Japan.
Vahatalo, K., Laaksonen, J., Tamminen, H., Aaltonen, O.,
& Happonen, R. (2005). Effects of genioglossal mus-
cle advancement on speech: an acoustic study of vowel
sounds. Otolaryngology - Head & Neck Surgery, 132(4),
636–640.
ˇ
Svancara, P., & Hor´aˇcek, J. (2006). Numerical Modelling of
Effect of Tonsillectomy on Production of Czech Vowels.
Acta Acustica united with Acustica, 92, 681 – 688.
ˇ
Svancara, P., Hor´aˇcek, J., & Peˇsek, L. (2004). Numerical
modelling of production of Czech Wovel /a/ based on FE
model of the vocal tract. Proceedings of International
Conference on Voice Physiology and Biomechanics.
RECORDING SPEECH SOUND AND ARTICULATION IN MRI
173
