
EVALUATION OF A MOBILE ELECTRODE FOR ELECTRICAL
STIMULATION OF THE PERINEAL MUSCLE
Preventive or Therapeutic Treatment
Fabiana S. B. Perez
School of Medicine, University of Brasilia, Brasilia, DF, Brazil
Adson F. da Rocha, Joao Luiz A. Carvalho, Patricia M. C. Paula
Department of Electrical Engineering, University of Brasilia, Brasilia, DF, Brazil
Cleyciany B. Cruz
Faculty Padrão, Goiania, GO, Brazil
Keywords: Perineal dysfunction, Electrical stimulation, Mobile electrode, Electrotherapy and physiotherapy.
Abstract: This work evaluates the effectiveness of a new type of electrode for functional electrical stimulation of the
perineal muscle in women and in men. The new electrode is shaped like a pen, with an active stimulation
electrode located on its tip. The goals of the study are to (i) demonstrate that stimulation using the new
device results in increased muscle strength; and (ii) compare the performance of the new device with that of
a traditional (fixed) electrode. Eight patients were evaluated, following a blind study protocol. The
preliminary results suggest that stimulation with the new electrode achieves better results than stimulation
with traditional electrodes, as higher increases in strength were observed in the group that used the mobile
electrode for preventive treatment and as an option of therapeutic treatment for female and for male perineal
dysfunction, in particular on erectile dysfunction in men with spinal cord injury.
1 INTRODUCTION
The perineum is a diamond-shaped muscle group
located between the pubic symphysis, the ischial
tuberosities, and the coccyx. It is separated from the
pelvic cavity by a set of structures forming a pelvic
diaphragm, which is composed by the
pubococcygeus, iliococcygeus, and coccygeus
muscles (Galhardo et al., 2007; Godec et al., 1975
).
These muscles occlude the pelvis, and provide
support for the pelvic viscera when there is an
increase in the intra-abdominal pressure due to
physiological events such as coughing, bowel
movements, laughing, carrying weight, pregnancy,
birth delivery and sexual intercourse. This happens
through the effective contraction and relaxation of
the muscles of the pelvic floor. Perineal
dysfunctions and psychosocial problems may occur
if this coordinated action does not occur properly.
One solution to these dysfunctions is to
strengthen the perineal muscles. This can be
achieved through physical therapy techniques known
as Arnold Kegel exercises (Moreno, 2004;
Berghmans, 2006). However, some patients are
unable to perform such exercises. In such cases,
electrical stimulation may be used. Electrical
stimulation of the perineal muscles has shown
satisfactory therapeutic results in many etiology
studies (Castro et al., 1998). Electrical stimulation
has been widely used in the past years (Castro, 1998;
Nielsen et al., 1992; Okada et al., 1992; Modotte et
al., 1999) and has presented good results, especially
using intracavitary electrodes. The performance of
this technique depends on the choice of electrode,
type of wave, amplitude, cycle, pulse, and frequency
(Marques, 2008).
The treatment of perineal pathologies typically
uses intracavitary electrodes. However, studies show
256
B. Perez F., da Rocha A., A. Carvalho J., C. Paula P. and Cruz C..
EVALUATION OF A MOBILE ELECTRODE FOR ELECTRICAL STIMULATION OF THE PERINEAL MUSCLE - Preventive or Therapeutic Treatment.
DOI: 10.5220/0003173402560259
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2011), pages 256-259
ISBN: 978-989-8425-37-9
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

adverse effects due to intra-cavity electrical
stimulation with this type of electrode, such as: pain,
unpleasant sensations, fecal incontinence, vaginal
irritation and infection (Sand et al., 1995; Yamanish,
2000). Moreover, patients with spinal cord fall into a
group of contraindication for electrical stimulation
of the perineal intracavitary electrodes, Figure 1A,
due to a sensory - motor change.
Due to these drawbacks, this work investigates
an innovative non-intracavitary type of electrode:
the mobile electrode, which uses a different mode of
application.
This study compares a treatment that uses a fixed
electrode to stimulate the muscles of the perineum
with a treatment that uses a mobile pen-shaped
electrode. The choice of electrodes is based on the
study of Modotti et al. (1999). The mobile electrode
has the size of a pen-tip, and can more adequately
stimulate the motor point and the fibers of the small
muscles in comparison with the fixed electrode,
which stimulates only one or two muscles, and
whose size makes its adaptation to the perineal
region more difficult.
We evaluate the effectiveness of the fixed
electrode and the pen-electrode in the recruitment of
muscle fibers of the perineum and the time required
to achieve a given level of strength. Preliminary
results are presented. Improved muscle stimulation
may help in curing and preventing diseases, by
strengthening the muscle.
2 METHODS
The study was conducted at Cerei Clinical Center
(Goiânia, GO, Brazil). The protocol was approved
by the ethics and research committee of the Faculty
of Medicine of the University of Brasília. Eight
volunteers of 37.5 ± 7.65 (mean ± s.d.) years of age
were chosen according to the evaluation of a
questionnaire for inclusion or exclusion. The
patients selected should be linked to the institution,
between 25 and 50 years old, with no surgical
correction of perineal pelvic floor disorders,
sedentary, non-users of medical drugs other than
contraception, sexually active, non-obese and have
agreed to participate voluntarily in the research. The
volunteers were blindly/randomly allocated into two
groups, according to their arrival. After signing the
consent, the volunteers were subjected to
gynecological and strength evaluation using a
Neurodyn Evolution perineal biofeedback device
(Ibramed Ltda., Amparo, SP, Brazil) with a vaginal
pressure probe (Ibramed Ltda., Amparo, SP,
Brazil). The probe was coated with a condom, and
lubricated externally with carbogel. The device
measures the maximum and minimum cavity
pressure achieved by voluntary contraction of the
perineum. After evaluation, the patient was
subjected to the protocol of group A or B according
to the assigned group.
The experimental protocol consists of two
procedures, each applied to one of the two groups of
subjects. In group A, the patients were subjected to
electrical stimulation of the pelvic floor muscles by
pen-electrode stimulation of five points around the
vaginal opening in an arc that starts on one side of
the groin and ends on the other side, passing through
the centre of the pubic arch. This stimulates five
motor points in different muscles, by moving the
mobile pen-electrode during the thirty minutes of
therapy. The five points of the perineal region are:
the pubic region, central tendon, bilateral inguinal
region, near the labium majus, and in the direction of
the vaginal opening. The stimulator generates
seventy impulses at each session toward a total of 14
pulses per point muscle during each session. The
pen-electrode was fixed during six minutes at each
point in each session.
In the use of mobile electrode for
electrotherapeutic application in male patients with
erectile dysfunction and partial Raqui-Medullar
Trauma (RMT) is obtained satisfactory results, but
with electrode application in the body of the penis,
scrotum and central tendon.
Figure 1A shows the use of intracavitary
electrode which in man should be anal with the
patient positioned in lateral recumbence. Figure 1B
shows the fixed external electrode positioned
bilaterally in the groin which does not allow the
visualization of local skin response. Figure 1C
shows the mobile electrode in the penis body
showing the swelling of the penis.
Figure 1: A) Intracavitary electrode; B) Fixed electrode;
C) Mobile electrode.
The electrode intensity instead of going on the
threshold of the patient pain, it goes to the moment
when the therapist visualizes the scrotal contraction
or the swelling of the penis, Figure 1C.
EVALUATION OF A MOBILE ELECTRODE FOR ELECTRICAL STIMULATION OF THE PERINEAL MUSCLE -
Preventive or Therapeutic Treatment
257
Group B participants were subjected to electrical
stimulation using fixed electrodes. A group of four
electrodes, arranged in a cross shape, were placed
around the vaginal opening, thus stimulating only
two muscles. The two electrodes from cable 1 were
arranged on the central tendon and the pubis, thus
stimulating this region. The two electrodes from
cable 2 bilaterally stimulate the groin, closing the
vaginal opening. Seventy impulses were used to
simultaneously stimulate these four points during
thirty minutes of therapy.
A Neurodyn Ruby stimulator (Ibramed Ltda.,
Amparo, SP, Brazil) was configured as follows for
both groups: low frequency synchronous FES with
the following envelope: frequency = 20 kHz; period
= 50 µs; rise = 7 s; on = 10 s; decay = 10 s; off = 5 s;
time = 30 minutes. The current intensity was
adjusted according to each patient’s sensibility,
provided that the electrical stimulation reaches the
motor threshold of the muscle without triggering a
painful stimulus. A vaginal probe was introduced in
the vagina of the patient during electrotherapy, using
a Neurodyn Evolution perineal biofeedback device
(Ibramed Ltda., Amparo, SP, Brazil) to check the
pressure before and after vaginal electrotherapy in
order to observe whether there is increase in strength
or muscle fatigue caused by the electrical
stimulation. The FES frequency was chosen due to
its extensive use in the literature (Godec et al., 1975;
Nielsen et al., 1992; Okada et al., 1999, Yamanish et
al. 2000). The protocol was repeated in 12 sessions,
performed twice a week, at a total time of 30
minutes per session.
A comparative analysis of muscle fatigue of the
subjects of group A compared to group B was
performed. For each subject, the intra-session
increase in muscle strength was calculated as the
difference between end pressure (after electrical
stimulation) and initial pressure (before electrical
stimulation). The inter-session increase in muscle
strength was evaluated by linear regression of the
measured pressures from each subject.
3 RESULTS AND DISCUSSIONS
This work presents current results from an ongoing
study. Therefore, only data from the first 7
experimental sessions (out of 12) are presented.
However, the study is still in progress and complete
results will be published at the end of the
experiments.
Local muscle fatigue is a decrease in muscle
response to a repeated stimulus, i.e. a normal
physiological response of muscle is characterized by
a decrease in amplitude of motor unit potential
(Kisner, 2009). Table I presents and the angular
coefficient of the linear regression on the 7
measurements (sessions) from each subject. Positive
angular coefficients indicate a tendency of
increasing pressure with each additional session, i.e.,
an increase in muscle strength due to periodic
electrotherapy. Three out of four subjects in group A
presented positive angular coefficients, while only
one out four subjects in group B presented positive
slopes.
Table 1: Initial pressure in each session (in mmHg) and
corresponding linear regression angular coefficients.
Group Session S1 S2 S3 S4 S5 S6 S7
Angular
coefficient
A
Subject 1
13
5 113 47 57 132 69 93 −4.6071
Subject 2 64 39 92 77 73 72 84 3.8214
Subject 3 41 49 41 42 45 42 64 3.8214
Subject 4 51 50 62 39 48 51 56 0.1071
B
Subject 1 38 46 40 40 30 35 31 −1.8929
Subject 2 1 40 52 2 14 72 87 10.1429
Subject 3 79 76 131 106 101 105 2 −7.2500
Subject 4 56 62 63 49 46 62 55 −0.7143
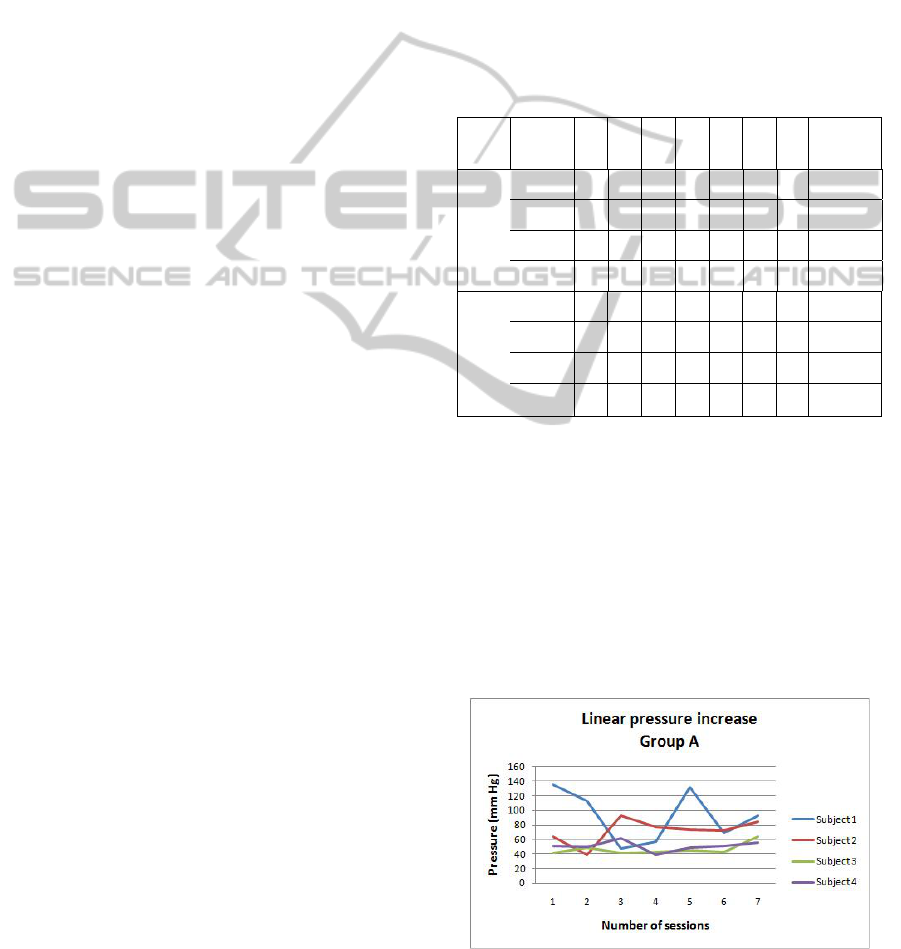
The measured pressure at the beginning of each
session for each subject of group A is showed in
Figure 2 and for group B in Figure 3. These results
suggests a trend of increased strength between
successive sessions for subjects stimulated with the
mobile electrode (group A), and a trend of strength
loss in subjects stimulated with the fixed electrode
(group B). The mobile electrode was expected to
provide higher strength gain, because force
production is directly related to the number of
stimulated motor points [8].
Figure 2: Measured muscle pressure at the beginning of
each session for each subject of group A.
BIODEVICES 2011 - International Conference on Biomedical Electronics and Devices
258

Figure 3: Measured muscle pressure at the beginning of
each session for each subject of group B.
Treatment with intracavitary electrode is not
indicated for patients with altered sensitivity because
it might cause injury which will not be perceived by
the therapist and/or by the patient, on the other hand
with the conventional electrode (fixed) it might
cause injure due to the static positioning on the skin
surface during the therapy without the visualization
of the skin surface of the patient with altered
sensitivity, Figure 1B.
With the new mobile electrode (pen), the electrical
load is greater at the tip of the conductor with an
intense electric field which can trigger faster the
action potential in the injured muscle, and because
of being mobile and external even with changing
sensory of the patient, the therapist is able to
visualize the muscle contraction even though the
patient does not notice, and monitor the dermal
reaction of it to prevent injury, Figure 1B.
4 CONCLUSIONS
Preliminary results suggest that the pen-electrode is
more effective than the fixed electrode in providing
gain of perineum muscle strength. The comparison
was performed using similar protocols with respect
to duration and current administration, differing only
for the fact that, with the pen-electrode, each point
received 14 stimulated impulses during the thirty-
minute pulse therapy, while seventy impulses were
used for each of the four points during the sessions
with the fixed electrode.
The preliminary results suggest that the pen-
electrode may be a better option for electrotherapy
than the fixed electrode in the prevention and in the
treatment of perineal dysfunction of, highlighting the
possibility of the use in patients with reduced
sensitivity, for example, the spinal cord injured.
The group that received stimulation with fixed
electrodes showed a reduction in strength,
suggesting a slower perineal muscle response due to
muscle fatigue, which occurs during prolonged
simultaneous stimulation of the four fixed points.
The mobile pen-electrode stimulates five points non-
simultaneously. The increased strength resulting
from a minor muscle fatigue can possibly shorten
the therapy duration and reduce the financial costs to
the patient.
REFERENCES
Berghmans B. The role of the pelvic physical therapist.
Acta Urol Esp, 2006. 30:110-22.
Castro,R. A. Arruda,R. M.,Takano,C.C.,Girão,M. J. B.
C.,Sartori,M. G.,Baracat,E. C.,Lima,G. R. Tratamento
da incontinência urinária com eletroestimulação. In:
Gineco.Obstet.Atual. v.7. n.4, abr.1998. p. 49-50.
Galhardo,C.,Katayama,M. Anatomia e fisiologia do trato
urinário inferior feminino. In:Chiarapa,T. R.,Cacho,
D. P.,Alves,A. F. D. Incontinência urinária Feminina:
Assistência Fisioterapêutica e Multidiciplinar. São
Paulo: Livraria Médica Paulista Editora, 2007.
Godec C, Cass A. S, Ayala G. F. Bladder inhibition with
functional electrical stimulation. Urolog, 1975.
6:663-6.
Kisner, Carolyn, Fundamentos da exercícios terapêuticos e
técnicas, 5° edição, Editora Manole, 2009.
Marques, A. A. A estimulação do nervo tibial posterior no
tratamento da bexiga hiperativa. Unicamp. Campinas,
SP: [s.n.], 2008.
Modotte,W. P.,Moreira,E. C. H.,Pascon,A.
M.,Dias,R.,Pascotini,C.,Filho,C. I. S.,Braga,M. A.
Incontinência urinária – trabalho conservador. In:
ginecol.Obstet.Atual. v.8. n.6, 1999. p. 6-13
Moreno, Adriana L. Fisioterapia em Uroginecologia,
Barueri, SP, Manole, 2004.
Nielsen M, Samuelsson S. M. Maximal electrical
stimulation of patients with frequency, urgency and
urge incontinence. Acta Obstet Gynecol Scand,
1992. 71:629-31.
Okada N, Igawa Y, Nishizawa O. Functional electrical
stimulation for detrusor instability. In: Urogynecol J,
1999. 10:329-35.
Sand P. K, Richardson D. A, Staskin D. R, Swift S. E,
Appel RA, Whitmore KE et al. Pelvic floor electrical
stimulation in treatment of genuine stress
incontinence: a muticenter placebo-controlled trial. Am
J Obstet Gynecol: 1995. 173:72-9.
Yamanish T, Yasuda K, Hattori T, Suda S. Randomized,
double-blind study of electrical stimulation for urinary
incontinence due to detrusor overactivity. Urology.
2000, 55:353-7.
EVALUATION OF A MOBILE ELECTRODE FOR ELECTRICAL STIMULATION OF THE PERINEAL MUSCLE -
Preventive or Therapeutic Treatment
259
