
HOW TO BUILD A MODERN PATIENT CARE APPLICATION
Dieter Gawlick, Adel Ghoneimy and Zhen Hua Liu
Oracle Corporation, 500 Oracle Parkway, Redwood City, CA 94065, U.S.A.
Keywords: Declarative programming, Data management, Knowledge management, Tagging, Meta-queries.
Abstract: Patient care is typically supported by several incompatible applications in terms of their data models and
semantics, ranging from support for surgery, to ICUs, to standard health care. These programs are focused
on specific situation and give doctors a very limited view at patient information. This paper argues that the
IT technology has evolved to a point that it is now possible to develop a generic patient care application that
manages all patient data for all situations. Furthermore, this application provides a framework for capturing
medical knowledge. With this knowledge the application is able to extract medically relevant information
from data, even if the extraction is outside of the medical expertise of a doctor or if the extraction is outside
of the capability of the human brain. Medical knowledge can be customized by domain, personal views, and
patient condition. Additional benefits are: alerting the right doctor of time critical situations, identifying
relevant information from a (new) patient’s history, and timely sharing of (new and codified) medical
knowledge and experience across the medical community. The ideas are based on prototype work between
the University of Utah, Health Science Center (UUHSC), the University of Coimbra, and Oracle (Guerra et
al., 2009).
1 INTRODUCTION
Today’s patient care applications are focused on
managing patient data using only the most basic
functionality of database systems. Operational tasks,
such as monitoring patient conditions, alerting
doctors for critical patient conditions, classifying
and extracting information from patient data and
developing and supervising treatment plans, are
considered to be beyond the scope of DBMS.
Therefore, a significant amount of procedural code
is written leading to limited functionality, lack of
customization, and extremely high development and
maintenance costs. Long development cycles are
another side effect.
In this paper we show that modern database
technology has matured to a point that even
operational tasks can be handled by databases based
on declarative specifications.
Databases can capture a wide variety of data
since they support variety of data models; SQL for
the management of highly structured data, XML for
the management of semi-structured data (Liu et al.,
2005), and RDF/OWL for formal semantics and
reasoning (Das, S.
et al., 1004); DICOM can be
used to manage medical images. Ad-hoc access to
single records is complemented by a rich support for
analytics, all the way to the support for the
development of (non-hypothesis) driven predictive
models and machine learning. Databases are also
able to automatically manage the history of patients
providing easy and fast access while minimizing
storage consumption; updated and deleted records
are simply remembered.
Databases have a variety of ways to extract
information from raw data in near real time.
Examples are triggers, real-time log-miners,
registered queries, online scoring, and RDF/OWL
rules (Oracle, 2010b). Any of these technologies can
be seen as a way to capture domain knowledge and
apply them to the data; i.e., databases not only
manage data but also manage knowledge and apply
this knowledge immediately to incoming data (
Motro
and Yuan, 1999). Extracted information can be stored
in the database as well, however, extracted
information will typically be represented by an
abstract vocabulary that most likely consists of a set
of tags; e.g., the vitals of a patient are critical. The
association of tags to data is often the core of
applying domain knowledge to captured data. Time
critical information will trigger alerts. New or
improved knowledge will trigger a re-evaluation of
existing data and trigger alerts as well.
427
Gawlick D., Ghoneimy A. and Liu Z..
HOW TO BUILD A MODERN PATIENT CARE APPLICATION.
DOI: 10.5220/0003298404270432
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2011), pages 427-432
ISBN: 978-989-8425-34-8
Copyright
c
2011 SCITEPRESS (Science and Technology Publications, Lda.)

Knowledge is widely shared among experts;
however, it is important that knowledge can be
tailored to the view of sub-domain specialities and
individuals. This can be done by integration of
knowledge management and consumer management.
The rest of the paper is organized as followings.
Section 2 describes the motivating example of
patient care. Section 3 describes important aspects of
advanced data management, knowledge
management, and consumer management, section 4
shows how these technologies are used
synergistically, section 5 compare this approach to
others and section 6 draws conclusions.
2 PATIENT CARE
The capturing of patient information with EMRs is
on its way to become the baseline for using IT
technology for patient care. Ideally, the medical
personnel and patients should have unobstructed
access to any information they are entitled to see;
e.g., they should have access to individual records –
present and past as well as support for higher level
functions such as trends and scoring against any
number of conditions.
This management of and access to patient
records has to be complemented by the management
of the medical knowledge, i.e.., the system has to
support the medical personal and patients in the
interpretation of data. Here are two examples: the
application should be able to determine if a specific
value, or a set of values indicate a risk, i.e., create if
necessary a tag indicating a serious or critical
condition. The application should also to able to
identify those models – diagnosis’s - for which a
patient scores high. This application of the medical
knowledge has to be done whenever new data
becomes available. If there is any urgency in the
computed information, the right members of the
medical personnel have to be alerted.
The interpretation of data is obviously a very
complex process; it depends not only on patient data
but also on the diagnosis, the speciality, as well as
the preferences of a doctor. Consequently, the
knowledge management has to capture shared and
generally accepted knowledge and also provide the
freedom for individual points of view.
The knowledge that is used to support an
individual doctor can be considered as a profile of
that doctor. Profiles should be used to significantly
improve query processing. Instead of looking just at
data, doctors should be able ask for important
information that are (hidden) in the patient data; as
of the time of the query or in the past. This would
allow doctors to find important information fast,
even in a large amount of data. Missing data (lab-
test) should also be identified.
Since the medical knowledge evolves extremely
fast; the application must not only be able to adapt
easily to new and improved knowledge but also help
doctors to improve their knowledge by referencing
background information about the applied
knowledge.
All information derived by the knowledge
management system has to be documented for
proper auditing, tracking, and provenance; data,
knowledge, and derived information have to be lined
up in time.
Such an application could provide a better
foundation for evidence-based medicine.
Today, knowledge is shared by writing papers.
There are just too many papers to read and the
information is often not precise enough. Papers have
to be complemented by a representation in machine
useable form. This representation – with the proper
precaution and adjustment – should be easily
importable into a knowledge base.
Models – applied to a large number of patients -
should be used to provide insight in the selection of
the best ‘standard of care’ even taking patients’
objectives into account.
3 THE TECHNOLOGIES
The development of new medical applications needs
to leverage these three core technologies: data
management, knowledge management, and
consumer management.
3.1 Data Management
3.1.1 Data Models and Extensibility
Medical applications require the management of
many types of data, far beyond classical SQL92,
which is used by most applications and only
supports simple structured relational data. Modern
DBMSs have evolved to a point that they can store,
manage, and query all kinds of data in one system,
including DICOM data that are specifically designed
for medical applications. Table 1 shows a few types
of data that healthcare applications need with the
corresponding support in modern DBMSs.
Storing data using these technologies without
any intervening application logic is the preferred
way of managing data. It provides an unobstructed
HEALTHINF 2011 - International Conference on Health Informatics
428
Table 1: Use of data types.
Data Model with Query
language supported by modern
DBMS
Data instance examples in
Healthcare Application
SQL92 relational data with
SQL
Patient id, name, birth-date
etc
XML with XQuery &
SQL/XML
Doctor notes, comments with
XML tagging
RDF/OWL with SPARQL Knowledge management
Domain specific data with
object SQL and extensibility
DICOM patient data
view at data.These technologies are typically built
on top of the database extensibility framework
(Stonebraker et al., 1998).
3.1.2 Data Mining and (Online) Scoring
Information can be extracted from records by
defining expressions (rules); however, what can be
done to extract complex information, i.e., I need to
assess the likelihood of one or more patients having
a cardiac arrest within the next 24 hours? It is close
to impossible to formulate the right expressions
(rules) manually; data mining can be leveraged for
the development of (non-hypothesis) models as well
as scoring these models based on patient
information. Modern DBMS can support data
mining efficiently (Milenova et al., 2005).
3.1.3 History Management
Capturing the history of specific patient data with
program logic is a very resource intensive in terms
of development effort (typically > 50% of this
effort) as well as storage and access cost.
Transactional temporal databases, i.e., databases that
keep previous and deleted versions of records and
make them easily accessible are a much better
approach. Additional benefits can be gained from
RDBMS with full ILM (Information Life Cycle)
support, including compression, access optimization,
and more. Data history support provides the base for
auditing, tracking, and provenance. A good example
for temporal support is Total Recall (TR) in the
Oracle database (Venkata et al., 2008).
3.1.4 Event Processing
Databases have significant support for event
processing. Trigger and (online) log mining are
widely available technologies (Chandy and Gawlick,
2007). A more recently introduced capability, is to
register queries and notify applications and/or users
if there is a change in an object or a result set
(Oracle, 2010a). While registered queries allow
extracting important information from databases in a
timely fashion. Materialized view capability can
handle more computational intensive extraction in
periodical fashion.
3.1.5 Tagging and Grouping
Annotating information with tags is a flexible way
of classifying and grouping information; e.g.,
normal, guarded, serious, and critical is a
meaningful tag set to classify a wide range of patient
data. Using this tag set one can ask for any data
values that are classified as serious. Another
important tag set is the diagnosis. These tags could
be complemented by information about uncertainty,
relevant data/tests to reduce any uncertainty, and
other information.
Tags reduce significantly the complexity and the
number of queries. This is due to the fact that a
valuable part of the domain knowledge is captured
in the selection of the tag attributes, the tag sets, and
the calculation of tag values. While there is a wide
consensus within a domain about these selections
and calculations, it is important that customization
for special areas, groups, and individual views is
well supported and easy to use.
Tagged data can be modelled using XML data
model and querying of tagged data can leverage
XQuery that is designed to query XML (Liu et al.,
2005) while RDF/OWL technology can be leveraged
to support customization.
3.2 Knowledge Management
The success of modern patient care applications
requires effective management of domain
knowledge. This section explains the essence of
(operational) knowledge lifecycle management, and
how such knowledge can be applied to data and
produce relevant timely information.
3.2.1 Knowledge Lifecycle
Knowledge Capture: Before knowledge is captured
in the form of logical assertions, an ontological
model (T-Box) must be specified, to provide the
logical foundation for the assertions to be captured.
Such model may initially be very simple. As Subject
Matter Experts (SMEs) gain more knowledge about
better ways of interpreting the facts in the database,
the model can be evolved to support such learning.
Support for personalized ontological model and
assertions are essential for lowering the barrier to
capturing knowledge. Community or institutional
knowledge is eventually derived from the
aggregated personalized knowledge. Also, allowing
HOW TO BUILD A MODERN PATIENT CARE APPLICATION
429

SMEs to record their subjective belief in a
generalized manner without restrictions, lower the
barrier to capture such belief. Such generalized
knowledge can be eventually specialized at a later
time by subjecting them to deductive rules and
machine learning techniques.
Knowledge Validation: Validating captured
knowledge and assigning pedigree to its models and
assertions is essential to the trustworthiness of such
knowledge. It can be achieved through ontology
validation heuristics, computing statistical
consensus, or social network analysis. Increasing the
trustworthiness and consistency of knowledge
content tend to increase the knowledge base
resistance to invalid or incorrect assertions and
models.
Knowledge Retrieval: Knowledge retrieval is
essential for sharing, transferring, and learning the
knowledge of a community of practice or an SME.
Database embedded RDF/OWL technology
simplified, to great extent, the browsing, querying,
and searching of such knowledge (Das, S. et al.,
1004), (Oracle 2010b). While an NLP based search
interface is not within the scope of this paper, it is
essential to effective knowledge search.
Knowledge Maintenance: Knowledge
maintenance is essential for the evolution of SMEs
and community understanding and interpretation of
the facts. The ability to specify defined classes and
infer membership and subsumption of such defined
classes is extremely important to evolving the
personal and institutional knowledge. Such
capabilities facilitate the refinement of the
knowledge and enable the encoding of deeper
understanding of the facts on ongoing basis.
3.2.2 Knowledge Application
In our approach, knowledge is maintained in two
representations; a formal model that is platform
independent and an executable model that is
platform specific. Both models are required to be
declaratively specified making it possible to
maintain consistency between the two models,
should one of them changes. As SMEs and
Knowledge curator maintain and evolve the
knowledge, a system would be able to reflect such
evolution on the platform specific model using
automatic transformation rules.
Similarly, changes to the platform specific model
by IT personnel and data mining specialist can be
reflected on the platform independent model. This
will also allow us to test the validity and consistency
of such change.
In the following section we will show that the
current database technology is able to encode
operational knowledge effectively and to process
data transactionally in real-time using deductive
reasoning, event processing pattern recognition, and
meta-queries.
Deductive Reasoning: Deductive database
research recognized the need for applying deductive
reasoning to deduce actionable information from the
database. It facilitated the application of logic and
inference to relational data (Tsur, 1991)
(Ramamohanaro, K. and Harland J. 1994). Modern
databases (Oracle, 2010b) can support the
transactional application of deductive reasoning in
real-time. Semantic Assisted Queries is one
example. Such capabilities have enabled the creation
of new breed of applications capable of applying
domain knowledge to the facts in the database to
extract humanly consumable information in real-
time (Universitaet Bonn, 2010).
Event Processing: Timely awareness of critical
incidents – alerting - is very important in the medical
and almost any other domain. Alerting requires users
to specify which information is important to
him/her. Database triggers represent the first
generation of active data supporting explicit event
processing paradigm (Chandy and Gawlick, 2007).
Though trigger support is effective, it is still too low
level and is not scalable with large number of
triggers. Instead, second generation event processing
in active data management enables user to register
large number of patterns and efficiently evaluate
them in a scalable manner via indexing over
conditional Expression. Patterns of interests can be
defined using conditional expressions
A data type that is of special interest for patterns is
the expression type (Yalamanchi et al., 2003
).
Expressions can be stored in tables with a column of
type expression. Given input data, one can find all
the stored expressions that are evaluated to be true
for these data. The scalable is achieved through a
specific index for expressions. Expression filter are
very effective in supporting personalized multi-level
pattern recognition preferences. Event Processing
facilitates the encoding of rules knowledge in the
form of Event-Condition-Action.
Continuous Query Notification (CQN) on the
other hand continuously evaluates the state of an
object or a query and alert users and application in
the event of occurrence of such change (Oracle,
2010a). Materialized view can be used to derive new
knowledge given new patterns are found.
Meta-Queries: As a large body of (medical)
knowledge is captured and encoded in declarative
HEALTHINF 2011 - International Conference on Health Informatics
430
rules and queries, it is important to apply such
knowledge to (newly arriving) patients with a large
medical history. Therefore, there is a need for
queries that reference the knowledge base as well as
the fact base to extract important information. We
call these queries meta-queries. The result of these
queries is a set of records that indicate which
elements of a knowledge base identified relevant
queries and what was found; e.g., a meta-query may
identify a set of diagnosis, their time, and even
associate probability.
It is not feasible to apply all rules to all patient
records due to the length of time it takes to apply all
known rules and queries to patient records. One way
to find such relevant queries is to treat the rules and
queries as an abstract data type, build an efficient
index, and identify relevant queries by using patient
data to traverse this index.
Meta-queries provide the same results as event
processing if the same queries and data are used.
The only difference is the time results become
available.
3.3 Consumer Management
An application that supports data and knowledge
management can deduce information from raw data
as soon as new information becomes available. This
interpretation of data, however, often depends on the
personal view and preferences of individual doctors
– the consumers of the information. Therefore it has
to be known which doctors are responsible for which
patients in order to apply the right profiles (of
knowledge) to incoming data. If the deduced
information is classified as being urgent doctors (or
other medical personal) have to be alerted
immediately. Obviously, the deduced information as
well as the urgency can be different for different
doctors –allowing doctors in a team to share each
other’s view may be beneficial.
This function requires up-to-date data about the
consumers (medical personnel), their assignment,
their availability, how to reach them, as well as their
(evolving) profiles; i.e., the status of all consumers
and their organizational context must be known at
any point in time.
4 PUTTING IT ALL TOGETHER
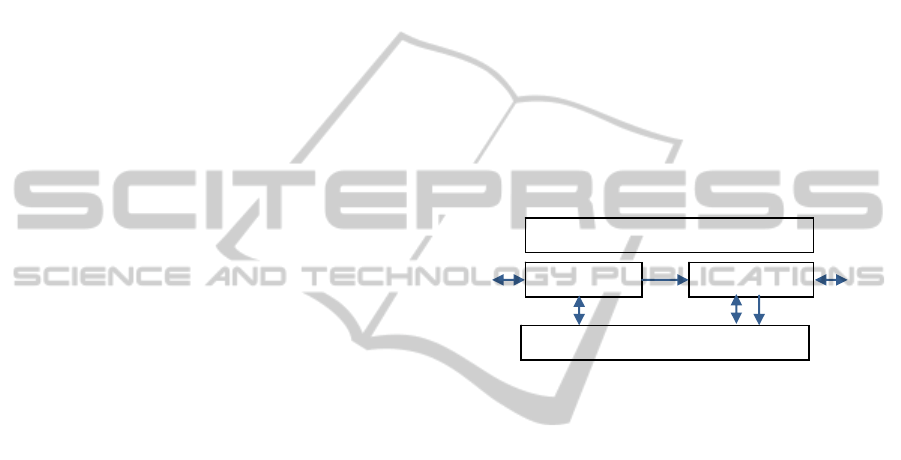
Applications depend on four main components;
knowledge, data, information, and consumers.
Knowledge Base contains the structure and
semantics of the data and all the codified domain
knowledge. The codified knowledge can be
represented in the form of rules, expression (if
expression then …), models or any other means
useful to extract information from data. The
knowledge base is highly customizable, it contains
the codified knowledge of the entire medical
community customized by views and interest of
doctors working in specific domains, as well as
customized by the view of individual doctors, and
even the way doctors looking at specific patients.
Data contains all the measurements and
observations that are captured by sensors and the
medical personal; here we will record the vitals, the
blood chemistry, and whatever else has been
observed. Data supports a wide range of data types,
history management, life cycle management as well
as all essential operational characteristics, such as
performance, scalability, availability, fault/disaster
tolerance, and security.
Data Information
KnowledgeManagement
Consumers
Figure 1: Application components.
Information contains insights that have been
derived from applying the operational knowledge;
here we will find a note if the heart beat is perceived
as critical or if a patient has a high risk of a cardiac
arrest within 24 hours. The underlying functional
and operation support is at the same level as for data.
Consumer contains details about the medical
personnel, such as who is on shift, who is available,
and how to reach a doctor or nurse. Most
importantly there is data on the customization of the
operational knowledge.
Raw data will be captured using OLTP or
protocols; export is possible as well.
Whenever new data are captured, they and the
previously captured data will be analyzed using the
operational knowledge, if anything of importance is
found, one or more entries in information base will
be made; e.g., data will be transformed into
information. It should be noted that information
entries could be created even if there is no change in
data. For example, the blood pressure has remained
high for an extended period. Doctors can add
informational notes as well.
Entries in the information base may be tagged as
time critical; so as to alert attending doctors/nurses.
In addition to being alerted, the medical
personnel can access data and information entries at
HOW TO BUILD A MODERN PATIENT CARE APPLICATION
431

any point in time. If a doctor gets an alert he/she
may be interested in the background leading to this
alert, the system will be able, not only to show
which data triggered the alert, but also which entries
in the knowledge base were used. This is especially
helpful if an alert is triggered by a knowledge base
entry representing medical knowledge a doctor is not
familiar with.
Obviously, doctors can ask questions referring to
information such as what is important to know about
this patient; rather than going through 1000’s of
EMRs.
5 COMPARISON
It may be interesting to compare our approach to
OLTP and (stream based) event processing. OLTP
only manages data; there is neither a knowledge
base, nor information, nor consumer management.
Event processing supports the data component only
in a very specific way; entries in data are transient
and ordered by a time stamp, there is no query
support and the focus for operational characteristics
is only on performance. Knowledge management is
implicitly represented as a set of rules or continuous
queries, results from queries/rules are thrown over
the wall; there is no information and consumer
management. Our approach is integrated and it is
based on deductive database concepts enhanced by
tagging, grouping, and consumer management. This
direction is aligned with the work in (Universitaet
Bonn, 2010).
6 CONCLUSIONS
The ISCU prototype has shown that it is possible to
develop a patient care application that can be
universally used in ICU environments and other
patient care departments in hospitals, institutions,
out-patient care, as well as long term home care.
This application manages data, knowledge,
information, and consumers. It captures data,
deduces information from these data based on
personalized knowledge, alerts if urgent actions are
required, and provides unobstructed access to data,
information, and knowledge.
Our approach of integrating data, information,
knowledge, consumer management enables medical
applications to be developed in declarative manner
so that domain experts, such as medical staff, can
share knowledge and experience – easily, flexibly
with little delay. Such application can evolve
without dependency on IT personal and adjust to
advances in IT technology.
ACKNOWLEDGEMENTS
We like to thank Ute Gawlick (MD/PhD) for
ensuring that the SICU prototype reflects the needs
and thinking of the medical community, Diogo
Guerra for developing a complex prototype in only 4
months, and Pablo Tamaya for developing a non-
hypothesis driven predictive model for cardiac
arrest. Their work is the base for this paper.
REFERENCES
Chandy, K., Gawlick D., 2007. Event processing using
database technology. SIGMOD Conference 2007:
1169-1170.
Das S., Chong E., Eadon G., Srinivasan, J., 2004.
Supporting Ontology-Based Semantic matching in
RDBMS. VLDB 2004: 1054-1065.
Guerra, D., Gawlick, U., Bizarro P., 2009. An integrated
data management approach to manage health care
data. DEBS 2009
Liu Z., Krishnaprasad, M., Arora, V., 2005. Native
Xquery processing in Oracle XMLDB. SIGMOD
Conference 2005: 828-833.
Milenova B., Yarmus, J., and Campos, M., 2005. SVM in
Oracle Database 10g: Removing the Barriers to
Widespread Adoption of Support Vector Machines.
VLDB 2005: 1152-1163.
Motro, A., Yuan, Q., 1990. Querying Database
Knowledge, ACM 069791 365 5/90/0005/0173.
Oracle, 2010a. Using Continuous Query Notification,
http://download.oracle.com/docs/cd/E11882_01/appde
v.112/e17125/adfns_cqn.htm#CHDIEHHJ.
Oracle, 2010b. Semantic Technologies, http://download.
oracle.com/docs/cd/E11882_01/appdev.112/e11828/to
c.htm.
Ramamohanaro, K. and Harland J., 1994. An Introduction
to Deductive Database Languages and Systems,
VLDB Journal, 3, 107-122.
Stonebraker, M., Moore D., Brown P., 1998. Object
Relational DBMSs: Tracking the Next Great Wave,
2nd edition. Publisher Morgan Kaufmann Publishers
Inc. San Francisco, CA, USA.
Tsur, S., 1991, Deductive Databases in Action, ACM 0-
89791-430-9/91/0005/0142.
Universitaet Bonn, 2010. Active and Deductive Database,
http://idb.informatik.uni-bonn.de/research.
Venkata, K. Kanth, R., Hanckel R., Yalamanchi, A., 2008.
Using Oracle Extensibility Framework for Supporting
Temporal and Spatio-Temporal Applications. TIME
2008: 15-18.
Yalamanchi A., Srinivasan J., Gawlick, D., 2003.
Managing Expressions as Data in Relational Database
Systems. CIDR 2003.
HEALTHINF 2011 - International Conference on Health Informatics
432
