X-REPORT BREAST: IT TOOLS TO EARLY DETECT BREAST
CANCER THROUGH OPTICAL IMAGING
Dynamic Optical Breast Imaging, DOBI
Fulvio Casali, Cinzia Mambretti, Silvia Bellini and Mirella Bernabò
Socrate Medical srl, Via R. Sanzio 18, Cesano Boscone, MI, Italy
Keywords: Interpretation software, DOBI (Dynamic Optical Breast Imaging), Breast cancer, Angiogenesis.
Abstract: Breast cancer is the second leading cause of cancer deaths in women today; according to the American
Cancer Society, about 1.3 million women will be diagnosed with breast cancer annually worldwide and
about 465,000 will die from this disease. In the western world, its incidence in females in premenopausal
status results similar or superior to the incidence in females in postmenopausal status. Therefore, it is
imperative to identify diagnostic tools able to detect breast cancer in young women from the very early
stages. This paper presents an IT application developed to support Medical Doctors in diagnosing and
reporting with an innovative non-radiating, non-invasive optically-based breast cancer detection system,
suitable for scanning of young women. This system - ComfortScan - relies on a methodology – DOBI,
Dynamic Optical Breast Imaging - based upon the use of a red monochromatic light beam and able to
identify neoangiogenetic areas related to the onset of cancer. The application – X-Report Breast – interprets
the images captured by ComfortScan and provides automatic reporting and diagnosis. X-Report Breast
proves to be highly valuable in supporting the early diagnosis of breast cancers with ComfortScan,
increasing the survival probability and diminishing the invasive surgical impacts.
1 INTRODUCTION
Breast cancer is the second leading cause of cancer
deaths in women today (after lung cancer) and is the
most common cancer among women, excluding non
melanoma skin cancers. According to the American
Cancer Society, about 1.3 million women will be
diagnosed with breast cancer annually worldwide
and about 465,000 will die from this disease. Breast
cancer death rates have been dropping steadily since
1990, according to the Society, because of earlier
detection and better treatments. However, breast
cancer is dramatically growing in the western world:
the lifetime probability of developing breast cancer
in developed countries is about 4.8%, according to
the American Cancer Society (the probability is
about 13% for any type of cancer), while in
developing countries is about 1.8%.
Today, the largest majority of this inauspicious
events is diagnosed in females aged above 50, but
the new female generations are exposed during their
entire life to the phenomena responsible for the
increase of the risk factors (environmental pollution,
estrogens through food or pharmaceutical products,
cigarette smoke); consequently the breast cancer
incidence in females in premenopausal status
already results similar or even superior to the
incidence in females in postmenopausal status
(Ferlay et al., 2004; American Cancer Society, 2005-
2006) (Table 1).
Table 1: Probability to Develop Breast Cancer Within the
Next 10 Years.
Probability of Developing Breast Cancer Within
the Next 10 years
By age 20 1 out of 1,985
By age 30 1 out of 229
By age 40 1 out of 68
By age 50 1 out of 37
By age 60 1 out of 26
By age 70 1 out of 24
Lifetime 1 out of 8
It is therefore imperative to decrease the age of
the first breast scan, which calls for the adoption of
long term riskless technologies, protocols and
diagnostic methods. This paper presents an IT
application purposely developed to ease and
173
Casali F., Mambretti C., Bellini S. and Bernabò M..
X-REPORT BREAST: IT TOOLS TO EARLY DETECT BREAST CANCER THROUGH OPTICAL IMAGING - Dynamic Optical Breast Imaging, DOBI.
DOI: 10.5220/0003771401730178
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2012), pages 173-178
ISBN: 978-989-8425-91-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

harmonize diagnosis and reporting in an innovative
optically-based breast cancer detection system.
2 DIAGNOSTIC METHODS
Currently, breast cancer detection encompasses three
stages. First, a physical examination or screening
mammography identifies an abnormality in the
breast tissue. Second, additional imaging modalities
may be used to help deciding if the third step, a
biopsy, is required (Nass et al., 2001).
Today, mammography is the most popular
diagnostic tool, however it has two main drawbacks:
(i) it is radiating, which can induce long term
negative effects on young women; (ii) it is
inefficient on dense breasts, which is typically the
case for young women.
Although most studies demonstrate a substantial
reduction in death rates from breast cancer among
women screened by mammography, women over
age 50 benefit the most. In fact, below age 50, the
value of mammography screening is less clear
(Eliceiri and Cheresh, 1998) because the greater
density of breast tissue in younger, premenopausal
women makes mammography results more difficult
to interpret, reaching the 50% of false negative or
positive reports.
Further investigation methods are breast
ultrasound, MRI and PET.
According to the National Cancer Institute,
however, about half of cancers detected by
mammography appear as a cluster of
microcalcifications and ultrasound does not
consistently detect it, nor detects very small tumors
(Angiogenesis Foundation, 2001).
Theoretically speaking, Breast MRI (Magnetic
Resonance Imaging) is a powerful imaging modality
in anatomical and physiological detection But the
drawback is that it is uncommon to use Breast MRI
in screening or follow-up because of the timing, cost
and sophisticated environment. Moreover, MRI
cannot detect microcalcifications (National Cancer
Institute, 2011).
Positron Emission Tomography (PET), that
requires radioactive substance injection into the
body, is an expensive and very invasive alternative.
Consequently, optical technology appears to
offer the best perspectives as far as scanning of
young women is concerned. Optical breast
examination (Dynamic Optical Breast Imaging,
DOBI) (Zhang et al.) is an innovative, non-invasive
methodology based upon the use of a red
monochromatic light beam. The DOBI method is a
functional examination of the breast that aims to
identify neoangiogenetic areas related to the onset of
cancer.
The system based on DOBI – ComfortScan - is
digital, operator-independent and easy-to-integrate
with any other diagnostic systems; it allows quick,
painless examinations and makes available new
functional physiological data.
3 DOBI
DOBI is based upon the tissue deoxyemoglobin light
absorption principle. Dynamic volumetric changes
in blood and deoxyhemoglobin absorption changes
are commonly found in malignant tumors and result
in a unique angiogenic “signature.” The DOBI
method allows to measure these changes by applying
mild uniform pressure to the breast. The change in
pressure traps blood in the tortuous angiogenic
structures that form around the tumor. This trapped
blood becomes deoxygenated up to four times faster
than normal tissue. ComfortScan, the DOBI-based
system, displays the effects of the changes in volume
and/or the changes in deoxyhemoglobin over time.
These changes appear as areas of low light level in
the ComfortScan images because of greater light
absorption. Normal or benign tissue, which has
normal vascular structures and a slower metabolic
rate, does not absorb as much light. Consequently, it
has a higher light level than malignant tumors.
3.1 ComfortScan Operation Principles
ComfortScan (Figure 1) is a system based on DOBI
and designed to detect dynamic (physiologic)
changes, increased blood volume levels and depleted
oxygen levels (deoxygenated haemoglobin), that
characterize malignancies. It consists of the
following primary components:
Figure 1: The ComfortScan System.
BIODEVICES 2012 - International Conference on Biomedical Electronics and Devices
174
Soft breast holder: a silicon membrane used to
impress the necessary compression to the breast and
achieve acceptable image contrast in the area of
pathologic influence (API). Rise, fall and
maintenance of pressure are managed and monitored
by a custom-programmed microcontroller.
Breast platform with LED array: used both to
hold the breast in the right position and to emit light
in the single visible-red band through a flat-plane
array of 127 light emitting diodes (LEDs). The
custom programmed microprocessor precisely
controls the optical exposure time and the intensity
profile of the LED array.
Digital CCD camera, a high-gain, low-noise
device used to capture the slight changes in light
intensity within the illuminated breast.
System electronics and software to process the
measured incremental changes by using a variety of
subtraction and contrast enhancement techniques to
produce the diagnostic functional image. A
proprietary algorithm generates the breast
angiogenic region unique vascular profile that stands
out in marked contrast to other portions of the
breast. By displaying a contrasting appearance, the
system has the potential to confirm the suspect of
cancer and differentiate cancer from both benign
lesions and normal tissue within the breast,
particularly matching this report with echograms,
clinical findings, and also mammograms in over
forty women. These images supply physicians with
new information associated with cancer
development.
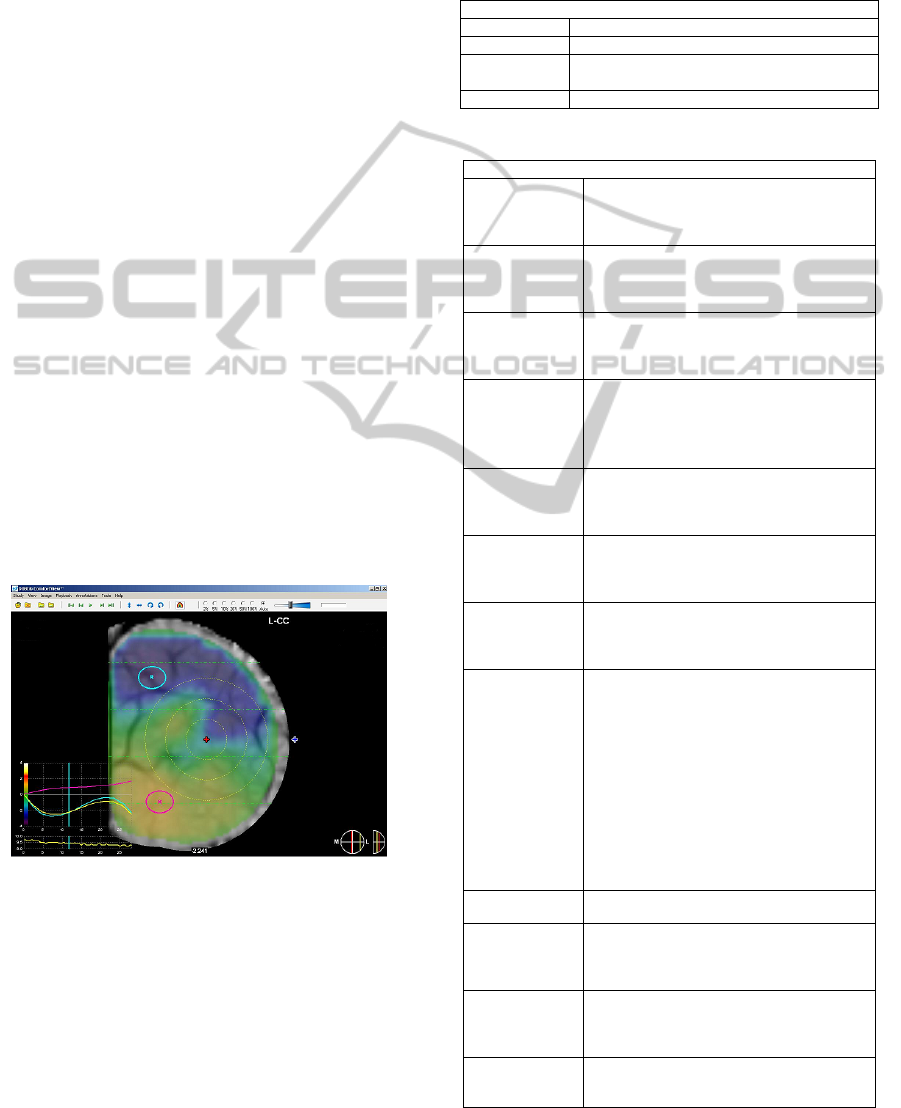
Figure 2: Comfortview Breast Chromatic Mapping.
Since vascular changes take place from the
earliest stages of cancer development, the ability to
image these changes can lead to earlier detection
and, therefore, earlier treatment of developing
cancers.
The dynamic analysis of the captured images is
performed by means of a post-processing application
– ComfortView- which provides a chromatic
mapping, highlighting the zones of increased
vascularisation (Figure 2).
ComfortView provides information about 4 main
dynamic diagnostic parameters (Table 2) and several
decision supporting parameters (Table 3).
Table 2: Main Assessment Criteria.
Main Assessment Criteria
LOCATION proximity to epicenter
SPATIAL focal or diffuse lesion
TEMPORAL
downward trend and study as the software
select the optimal contrast
CONTEXT similar/dissimilar curve
Table 3: Secondary Assessment Criteria.
Secondary Assessment Criteria
Margins
0 pt: non-assessable and indistinct;
2 pt: feathered;
4 pt: clearly defined and located
Diameter
0 pt: > 4 cm and not defined
1 pt: between 3 and 4 cm
3 pt: between 1 and 3 cm(well defined)
Distance from
nipple
1 pt: non –assessable and distance < 1,5 cm
2 pt: between 1,5 and 3
4 pt: > 3 cm
Localization vs
ROI
0 pt: external lesion
2 pt: inside 3rd ring
3 pt: inside 2nd ring
4 pt: inside 1st ring
Max saturation
Intensity
2 pt : if < -2
4 pt : if between -2 and -4
6 pt : if > -4
Time for AIP to
become violet
0 pt: never and > 20 sec
1 pt: between 10 and 20 sec
2 pt: if <10 sec
AIP
Visualization
time (sec)
0 pt: if < 10 sec
2 pt: between 10 and 20 sec
4 pt: if > 20 s.
I/T curve score
(AUTO)
0 pt: non -assessable
1 pt(negative): positive only curve
2 pt(benign): mainly positive, fluctuating curve
3 pt(doubtful): fluctuating curve with both
negative and positive values (slightly
descending, curved shape)
6 pt(suspicious): rapidly descending (still
curved shape)
9 pt(positive): rapidly descending , negative
values (straight descending line)
I/T curve score
(Range 10)
Same as previous (I/T curve score (AUTO))
I/T curve score
(AUTO)
0 pt: non-assessable, indistinct, feathered,
broadened
3 pt: well defined and centered on the lesion
AIP Curve score
(similar/dissimil
ar)AUTO
0 pt: similar
3 pt: variable non clearly dissimilar
6 pt: dissimilar
AIP Curve score
(similar/dissimil
ar) Range 10%
0 and 3 pt: as above (AIP Curve score AUTO)
6 pt: dissimilar(with increasing divergence)
X-REPORT BREAST: IT TOOLS TO EARLY DETECT BREAST CANCER THROUGH OPTICAL IMAGING -
Dynamic Optical Breast Imaging, DOBI
175
Each parameter has a weight, represented by an
associated value which depends upon its importance
in the evaluation process (weighted score). The
weighted sum of the values obtained for each
considered parameter during an examination
provides an overall score (called DOBI Level) which
corresponds to a diagnosis, as reported in Table 4.
Table 4: DOBI Level.
DOBI Level
DL 1 no actual signs of attenuation of the light beam
DL 2
no actual clearly abnormal signs of attenuation of
the light beam
DL 3
actual attenuation of the minimally abnormal light
beam
DL 4
actual attenuation of the abnormal and suspicious
light beam
DL 5
actual attenuation of the clearly abnormal light
beam
4 X-REPORT: AN IT TOOL TO
SUPPORT DIAGNOSING
Although the dynamic analysis and the post
processing activities are operator independent, the
final step, represented by the valorization of each
measured parameter, depends on the subjectivity of
the Medical Doctors (MDs).
MDs with substantial DOBI experience produce
completely similar diagnoses, often restricting the
evaluation to the 4 main parameters. On the
contrary, MDs with limited DOBI experience, which
represent the large majority, may have slightly
different interpretations, often due to their
background and previous experiences. A large
deployment of the DOBI diagnostic method cannot
ignore this fact.
Moreover, having in mind the objective to extend
the use of the DOBI method to screening, it is
imperative to shorten the time to diagnose
automating the valorization of the parameters, the
calculation of the overall DOBI Level and the
reporting.
Socrate Medical has developed an interpretation
and reporting application software that, based upon
interpretation rules agreed by a team of worldwide
renown experts, allows to free the diagnostic process
from operational factors, speed up and unify
reporting procedures and presentation to patients.
This application, called X-Report Breast, has
been developed in cooperation with the researchers
of the Pascale Hospital in Naples (Italy) and
validated by senior developers of ComfortScan in
the USA.
X-Report breast has been developed building
upon Socrate Medical’s experience in reporting
software for different medical sectors, mainly
gynaecologists and obstetrics. The system is
composed by the modules in Figure 3.
Figure 3: X-Report Flowchart.
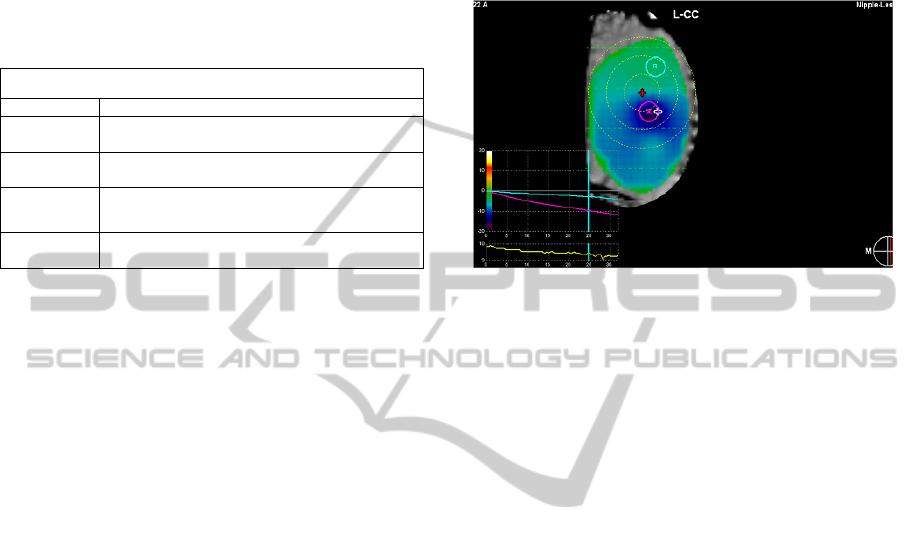
The Execution block is where the automatic
calculation process takes place. Within the
calculation package, the numerical values and curve
shapes obtained from the examination are compared
with the standard values and shapes stored within
the system. This permits to valorize each measured
parameter, qualify (e.g. similar or dissimilar, Figure
4) and valorize the curves. Obtained values are
summed and the overall result provides
automatically the response based on DOBI Level as
explained above and shown in Table 4.
All results are collected in a central data base and
used to feedback and tune the weighted score
system.
Although the X-report software and the working
procedure are the same in all systems, the weighted
scores may slightly differ, depending on
environmental and feminine specific characteristics
(e.g. skin color, average breast density and size, etc).
The impact of these differences on the weighted
score system has to be further investigated to define
whether a unique classification can be uploaded or
specific settings have to be foreseen.
X-Report Breast offers further investigation
options to MD’s: the Event/Visit block allows to
compare subsequent visits in order to evaluate the
progress or regression of the cancer.
The Lesion block allows, among other functions,
to compare the right and left breasts against lesions.
This feature is of paramount importance because
symmetry of nodules and lesions is a strong positive
indicator, able to exclude any malignancy with high
probability.
BIODEVICES 2012 - International Conference on Biomedical Electronics and Devices
176
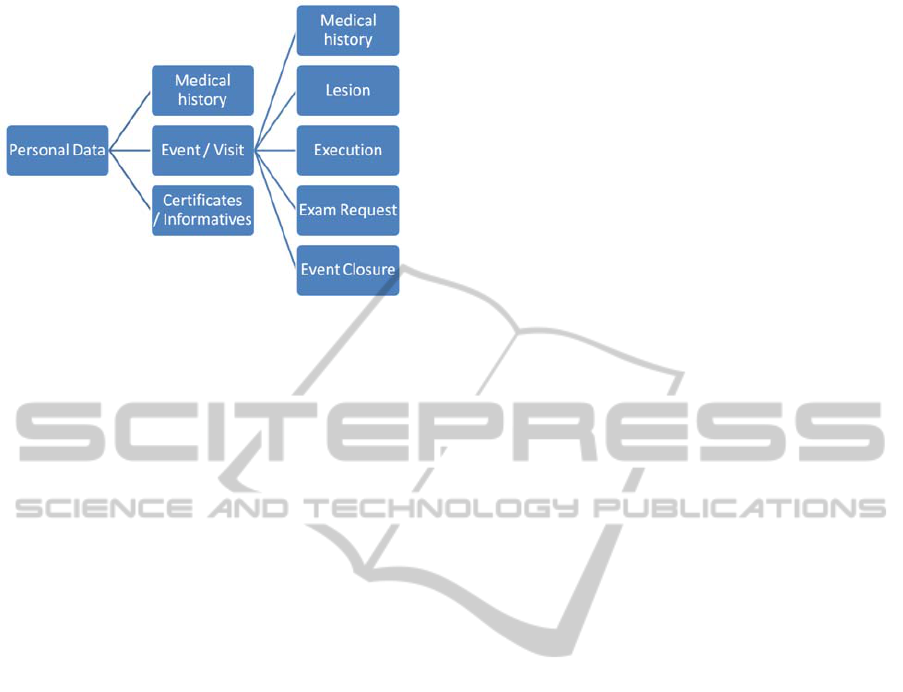
Figure 4: Measured vs Standard Haemodynamic
Response.
5 CLINICAL CASES
The experience built so far demonstrates that X-
Report Breast is highly valuable to support MDs in
early diagnosing breast cancers with ComfortScan.
In order to evaluate the effectiveness of the X-
Report tool in assessing the DOBI Level criteria, all
participant to the DOBI Group ethical committee
institutes, are going to participate to the method
evaluation, reporting the same 46 cases in double
blinded. Results shown same DOBI Level
classification thank to X-Report software tools.
First results on 113 women treated with X-Ray,
US, DOBI and surgery demonstrated 80% sensitivity
and 88% specificity using the cut off DOBI Level
30,5pt. Further evaluations are ongoing.
Other DOBI user results report that using X-
Report software and the DOBI Level method high
specificity, and high sensibility are obtained: both
values are higher than 80%.
6 CONCLUSIONS AND FUTURE
PLANS
Today, X-Report Breast is installed in all the
ComfortScan systems deployed in Italy and offered
as additional feature worldwide. The automatic
DOBI Level calculation package will ease the work
of the MDs, allowing non fully experienced MDs to
use ComfortScan and make the diagnosing times
compatible with the examination pace requested for
screening.
The next steps will see the DOBI community to
build a common reference data base where all
worldwide available patient data will be stored and
analyzed with the objective to draw conclusions of
general validity and usefulness beyond the specific
needs of X-report. This powerful tool will accelerate
the acquisition of further experience on the impact
of the assessment parameters, possibly suggesting
reductions and/or simplifications of the present set.
It will also continue the comparison between
results obtained through automatic diagnosing and
human evaluation by senior MD’s, with the
objective to improve the assessment and valorization
phases of the process.
X-Report Breast will be enriched with new
features and functionalities to support these tasks.
ACKNOWLEDGEMENTS
G. J. Zhang, CEO DOBI Global, Massachusetts:
who provided senior advisory on evaluation criteria
and their weighted level
All DOBI Group ethical committee members:
Dr. G. Ciuffo, Dr. F. Musco, Clinica Zucchi; Dr. I.
Guidi, Physios; Dr. V. Frattini, Centro Chirurgico
Magentino; Dr. S. Orefice. They have provided both
their valorization of the weighted Level mechanism
and the results of their clinical cases examinations.
Dr. M. D’Aiuto, Pascale Hospital: who had a
primary role in the development and validation of X-
report Breast.
REFERENCES
J. Ferlay, F. Bray, P. Pisani and D.M. Parkin.
GLOBOCAN 2002. Cancer Incidence, Mortality and
Prevalence Worldwide. IARC CancerBase No. 5,
version 2.0. IARCPress, Lyon, 2004.
American Cancer Society Breast Cancer Facts & Figures,
2005-2006
Nass S. J., Henderson C., Lashof J. C., eds.
Mammography and Beyond: Developing
Technologies for the Early Detection of Breast Cancer.
Washington, DC: National Academy Press. 2001.
Prepublication copy:16.
Eliceiri B. P., Cheresh D. A. The role of αv integrins
during angiogenesis. Molecular Medicine 1998; 4:741.
Angiogenesis Foundation, Understanding Angiogenesis,
www.angio.org, April 2001.
National Cancer Institute, Cancer Information, CancerNet,
Types of Cancer, Breast Cancer www.nci.nih.gov,
April 2001
G. John Zhang, Weiping Wang, Deqi Yang, Hongchuan
Jiang. DYNAMIC OPTICAL BREAST IMAGING -
A New Technique to Detect Breast Cancer at Early
Stage Results of investigational use of DOBI
ComfortScan in China
X-REPORT BREAST: IT TOOLS TO EARLY DETECT BREAST CANCER THROUGH OPTICAL IMAGING -
Dynamic Optical Breast Imaging, DOBI
177

Angiogenesis Foundation, Understanding Angiogenesis,
www.angio.org, April 2001
Li W. W., Li V. W., Tsakayannis D., Casey R., Jaffe M.,
Atwater L. A., eds. Market Study and Analysis of
Angiogenesis-Dependent Diseases. Cambridge, MA:
Angiogenesis Foundation, 2001:17.
Folkman J.: Tumor angiogenesis: therapeutic implications,
New England Journal of
Medicine 1971; 285:1182-
1186.
Weinberg R. A., One Renegade Cell: How Cancer Begins.
New York, NY: Basic Books. 1998:143-146.
APPENDIX
Angiogenesis Definition
Angiogenesis is the key biological process that
occurs into formation and growth of new blood
vessels and it is necessary for reproduction,
embryonic development and wound repair. The
complex angiogenic process is maintained in careful
balance by a variety of factors, but if this balance is
tipped in favor of too much or too little
angiogenesis, a variety of pathological conditions
can be the result, in particular, the role of
angiogenesis in breast cancer has been documented
(Folkman, 1971).
The cells of an incipient tumor require constant
nourishment and oxygen as well as a way to remove
waste products. To grow beyond the “one-millimeter
limit,” the tumor cells must develop their own blood
circulation system – mimicking the circulatory
system of healthy tissue nearby.
BIODEVICES 2012 - International Conference on Biomedical Electronics and Devices
178
