
ENHANCING PATIENT INFORMATION SHARING THROUGH
SOCIAL NETWORKS
M. Poulymenopoulou, D. Papakonstantinou, F. Malamateniou and G. Vassilacopoulos
Department of Digital Systems, University of Piraeus, Karaoli & Dimitriou 80, Piraeus, Greece
Keywords: Social network, Personal health records, Access control services.
Abstract: Currently, there is an effort for empowering patient self-care and improving the traditional healthcare
delivery models by expanding the concept of healthcare though the provision of advanced online healthcare
services. Those services require increased level of information flow and collaboration among patients and
healthcare professionals. This collaboration and patient information sharing can be achieved by integrating
social networks functionality with personal health records, based on open standards. In fact, social
networking exists to facilitate communication and collaboration and make possible what was only recently
impractical in healthcare, such as trans-regional clinician collaboration through web-based broadcasting
systems, therefore integrating the information included into personal health records. Along these lines, this
paper presents a secure middleware that aims at enabling patient information sharing among patients and
healthcare professionals through social networks functionality and applications, giving particular emphasis
to a security architecture that enforces access control services for protecting the disclosure of patient private
information to unauthorized users.
1 INTRODUCTION
In healthcare the traditional “face-to-face”
healthcare delivery may not fully meet the new
requirements of “e-Patients”, who wish to sit at
home seeking healthcare consultancy or online help
instead of lining up hours just for a few minutes talk
with physicians in hospitals or clinics (Domingo,
2010); (Greene et al., 2011). However, the reality is
that few online healthcare services can be found.
Recently, the Health 2.0 movement aims at
promoting participatory healthcare by suggesting the
collaboration among patients, caregivers, medical
professionals and other healthcare stakeholders
through the use of Web 2.0 technologies like social
networks (SNs) (Domingo, 2010); (Gajanayake et
al., 2011); (Thompson et al., 2011).
The social-networking revolution is coming to
healthcare, at the same time that new Internet
technologies and software programs are making it
easier than ever for healthcare professionals to find
timely, personalized health information online and
for patients to self-manage their medical information
and share it with others (Domingo, 2010);
(Gajanayake et al., 2011). Moreover, several
healthcare social networks (HSNs) have emerged,
such as PatientsLikeMe, Inspire.com, MedHelp,
Sermo and Ozmosis. HSNs provide online technical
infrastructures for physicians to share clinical cases,
images, videos and medical knowledge and for
patients to promote disease awareness, and positive
and proactive behavior, in order to stay healthy
while living with a disease (Domingo, 2010);
(Greene et al., 2011).
Since communication is a critical weakness of
the healthcare delivery system, SNs could
potentially improve communication by establishing
permanent channels (network connections) among
multiple physicians and between physicians and
patients. Also SNs can make the health system more
available, responsive and personalized to the public
by providing access to eHealth services to both the
public and health professionals (Domingo, 2010);
(Thompson et al., 2011); (Williams, 2010). Most of
the eHealth services (e.g. diagnosis, self-treatment,
expert advice, second medical opinion) require the
availability of accurate and updated patient medical
information and therefore some HSNs support
quantified self-tracking by providing easy-to-use
data entry screens for condition, symptom, treatment
and other biological information.
378
Poulymenopoulou M., Papakonstantinou D., Malamateniou F. and Vassilacopoulos G..
ENHANCING PATIENT INFORMATION SHARING THROUGH SOCIAL NETWORKS.
DOI: 10.5220/0003772203780381
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2012), pages 378-381
ISBN: 978-989-8425-88-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

At the same time, there is an increasing interest
by patients on public web-based Personal Health
Records (PHRs) for coordinating their lifelong
health information and make appropriate parts of it
available to those who need it (Cushman et al.,
2010); (Shachak et al., 2010); (Sunyaev et al., 2010).
However, PHRs are mostly designed to meet the
needs of episodic clinical encounters between
patients and health care professionals, and around
the diagnosis and treatment of diseases (Greene et
al., 2011); (Shachak et al, 2010).
Sharing patient data existing on PHRs through
SNs can provide the required patient information to
healthcare professionals, administrators and other
using eHealth services. However, the issues of
patient information security and privacy are some of
the biggest concerns when exposing patient private
information to a social network. Many SNs allow
users to customize some privacy settings and some
online HSNs provide an opportunity to freely obtain
and disclose information about a health condition
without having to divulge one's identity. In addition,
most web-based PHRs like Microsoft Health Vault
and ICW LifeSensor, provide functionality for
filtering the medical data to be shared with others
(Gajanayake et al., 2011); (Sunyaev et al., 2010).
However, there are still open issues as concerns
PHRs and SNs privacy and security and therefore
patients and practitioners still worry about the
wrongful dissemination of medical information.
Nevertheless, currently there are no available
guidelines to help navigate these complex issues
(Cushman et al., 2010); (Thompson et al., 2011);
(Williams, 2010).
The focus of this paper is on the security aspects
of the middleware without compromising the
benefits of information sharing, thus increasing the
overall social value of SNs in healthcare. Hence, a
context-aware access control service is proposed that
extends PHR access control features and enables
sharing of patient data through SNs.
2 MOTIVATION
The basic motivation of this research stems from our
involvement in a recent project concerned with the
employment of a middleware-level solution to
enable patient medical information sharing from
PHRs to advanced eHealth services (online
diagnosis, expert advice, disease management) that
are provided through SNs using their functionality.
Among the requirements of this middleware was to
enable patients setting their access control sharing
preferences on their medical information existing on
PHRs. The security requirements of this middleware
motivated this work and provide the context for the
development of access control services for the
middleware based on a security architecture that
ensures authorized patient information sharing from
PHRs in the domain of SNs, according to specific
user context-based preferences.
To this end, according to the overall middleware
architecture a) advanced eHealth services are
provided using SN functionality (e.g. messaging
mechanisms), b) integrated patient information
(patients active medical problems, diagnosis,
treatment plans and latest medical tests results)
exists on PHR and controlled by patients, c) the
middleware provides functionality for retrieving
patient information from PHR, transforming this into
a standard format and sending it to requesting SN
users and d) the access control services of the
middleware enable setting and enforcing the users
access control policies for their medical information.
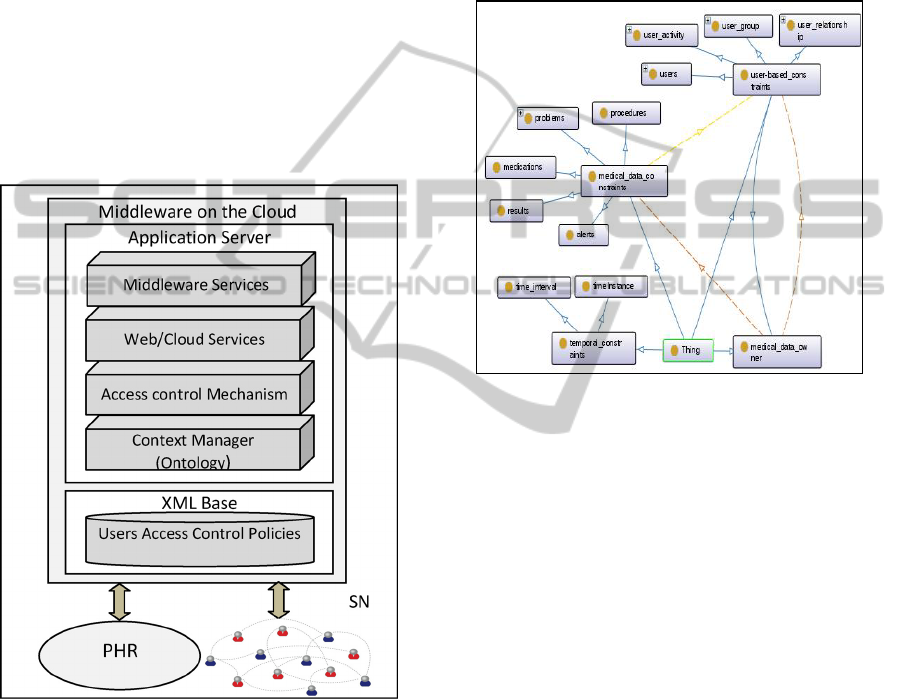
3 SECURITY ARCHITECTURE
According to the proposed cloud-based middleware
architecture, as presented in Figure 1, an application
server and an XML base are configured at cloud
servers. At the application server exist the
middleware services that encapsulate middleware
functionality, the web and cloud services used by the
access control services, the context-based access
control mechanism that takes context-based
authorization decisions for accessing (read access is
only allowed through the SN) patient medical data
existing on PHRs and the context manager that hosts
the ontology created to represent context
information. At the XML base are stored the user
access control policies. This architecture takes the
stance that the medical data of PHRs is retrieved in
the form of XML documents according to clinical
standards, as the Continuation of Care Document
(CCD) or the Continuation of Care Record (CCR).
As far as concerns the ontology, Ontology Web
Language (OWL) files have been created that enable
context information sharing in a semantic way and
also context reasoning. Additionally, Semantic Web
Rule Language (SWRL) rules have been written to
capture additional relationships among domain
classes (Beimel et al., 2011).
Context information involves a) user social
information, such as user profiles, relationships,
groups and activities on the SN (e.g. online/offline,
chatting), b) medical data information that includes
ENHANCING PATIENT INFORMATION SHARING THROUGH SOCIAL NETWORKS
379
data elements of PHRs as proposed by CCD/CCR
XML schemas and involves problems, medications,
alerts, procedures, results and other and c) temporal
information, such as time instances or time intervals.
In Figure 2 a small part of the ontology created
in OWL is shown. Context information of the
domain ontology is used to set contextual constraints
on user medical data (stored on PHRs) sharing
preferences. Hence, contextual constraints are
divided to a) user social based constraints that are
specified at user level, at user group level, at SN
relationship level (that links users), at user current
activity level (e.g. user participation on group online
chat), b) medical data based constraints that are
specified at the medical data element level and c)
temporal based constraints (e.g. time interval)
(Wrona et al., 2005).
Figure 1: The middleware architecture.
According to the security architecture, users set
through web service calls their context-aware
sharing preferences. Then, the access control
mechanism communicates with the context manager
to consult the ontology and the relevant SWRL rules
in order to result in new context information and
thus, (if any) new contextual constraints. The user
sharing preferences according to contextual
constraints (initial and inferred) are translated to
context-based access control rules and are stored by
cloud services to the cloud servers in the form of
user access control policy. Thus, for example, a user
access control rule can specify that his/her current
medications can be shared only with users that are
members of his groups named ‘mydoctors’ and
‘mypharmacists’. Another user access control rule
may specify that patient psychological profile can be
read during an online psychotherapy group without
disclosing patient identity, only by the authenticated
users of that group and only for the time period the
online group therapy takes place.
Figure 2: A small part of the OWL ontology.
On SN user request for accessing another (target)
SN user medical data, web services are called to
communicate with the context-aware access control
mechanism to retrieve the (target) user access
control policy, to evaluate the appropriate access
control rules and take decisions for the patient data
elements that should be viewed. Then, middleware
services are called that encapsulate functionality for
retrieving allowed patient data XML elements from
patient PHR, structuring this data in the form of a
CCD-based document and sending it to authorized
requesting user using SN messaging mechanisms.
For example, a physician might request through SN
(e.g. SN application) to view a patient latest
laboratory test results. Then, the appropriate web
services are called to evaluate patient access control
rules and if access is allowed the test results are
structured in the form of a CDD document that is
sent to the requesting user by SN message or email.
4 PROTOTYPE
IMPLEMENTATION
To illustrate the feasibility of the proposed security
HEALTHINF 2012 - International Conference on Health Informatics
380

architecture, a prototype implementation is
presented that is under development. Without the
loss of generality, for the purpose of the prototype
experimental implementation are used the public
cloud infrastructure of Amazon, the social network
of Facebook and the PHR of Microsoft called
HealthVault. Web services based on REST
technology were developed using the open source
Jersey to implement the access control services of
the middleware as well as the middleware
functionality. The HealthVault Application SDK
was used to access data from Microsoft HealthVault
PHR. Regarding the access control mechanism
implementation, the XML access control language
(XACML) is used and XACML policies are created
to represent user sharing preferences that are stored
to the cloud servers using Amazon S3 service
(Wrona et al., 2005). In addition, a web application
loaded in the context of Facebook is created to
provide the user application interface to access the
access control services and the middleware
functionality.
5 CONCLUDING REMARKS
This paper presents a security architecture that aims
at promoting secure patient information sharing
among users at anytime and from anywhere through
the use of SNs that are always available by any
device. In particular, the proposed access control
services ensure authorized patient information
retrieval from PHRs and its provision through SNs
messaging mechanisms and applications/tools
according to user’s access control preferences. To
realize this, there is a need to balance the urge to
protect individuals from potential harm that may be
caused by exposing personal information through
SNs and therefore to ensure that high quality
healthcare can be provided through the use of
eHealth services. In this paper, only the issue of
what other users can see has been addressed.
Questions of how to prevent the organisation in
control of the SN site using personal data which has
been freely shared for commercial gain through SN
functionality are left unanswered. Finally, there are
other problems not addressed here, such as legal and
ethical issues (Cushman et al., 2010).
The proposed security approach constitutes a
technological solution that is clearly implementable.
At present the development of the prototype is still
in the early stage. Thus, testing, user acceptance,
validation, evaluation and performance count on real
use of the eHealth services are still to be done.
REFERENCES
Beimel, D. and Peleg, M., 2011. ‘Using OWL and SWRL
to represent and reason with situation-based access
control policies’, Data and Knowledge Engineering,
vol. 70, pp. 596-615.
Cushman, R., Froomkin, M., Cava, A., Abril, P. and
Goodman, K., 2010. ‘Ethical, legal and social issues
for personal health records and applications’, Journal
of Biomedical Informatics, vol. 43, pp. S51-S55.
Domingo, M., 2010. ‘Managing healthcare through social
network’, IEEE Computer Society, vol. 43, no. 7, pp.
20-25.
Gajanayake, R., Iannella, R. and Sahama, T., 2011.
‘Sharing with care: An information accountability
perspective’, IEEE Computer Society, vol. 15, no. 4,
pp 31-38.
Greene, J., Choudhry, N., Kilabuk, E. and Shrank, W.,
2011. ‘Online social networking by patients with
diabetes: A qualitative evaluation of communication
with Facebook’, Journal of General Internal
Medicine, vol. 26, no. 3, pp. 287-292.
Shachak, A. and Jadad, A., 2010. ‘Electronic health
records in the age of social networks and global
telecommunications’, Journal of the American
Medical Association, vol. 303, no. 5, pp. 452-453.
Sunyaev, A., Kaletsch, A. and Krcmar, H., 2010.
‘Comparative evaluation of Google health api vs.
Microsoft Helathvault api’, International Conference
on Health Informatics - HEALTHINF 2010, Valencia,
Spain, pp. 195-201.
Thompson, L., Black, E., Duff, P., Black,
N., Saliba,
H.
and Dawson, K., 2011. ‘Protected health information
on social networking sites: Ethical and legal
considerations’, Journal of Medical Internet Research,
vol. 13, no. 1.
Williams, J., 2010. ‘Social networking applications in
health care: threats to the privacy and security of
health information’, Proceedings of the 2010 ICSE
Workshop on Software Engineering in Health Care,
Cape Town, South Africa, pp. 39-49.
Wrona, K. and Gomez, L., 2005. ‘Context-aware security
and secure context-awareness in ubiquitous computing
environments’, Proceedings of the XII Autumn
Meeting of Polish Information Processing Society
Conference, pp. 255-265.
ENHANCING PATIENT INFORMATION SHARING THROUGH SOCIAL NETWORKS
381
