
DESIGN AND EVOLUTION OF HOME-CARE WORKFLOWS
USING ONTOLOGIES AND MODEL TRANSFORMATIONS
Sabrina Zefouni
1,2
, Elyes Lamine
1,2
, Rémi Bastide
1
and Hervé Pingaud
1
1
ISIS - CUFR J.F. Champollion, Campus Universitaire, Rue Firmin Oulès, Castres, France
2
EMAC, Centre de Génie Industriel, Jarlard, Route de Teillet, Albi, France
Keywords: Workflow, Ontologies, Homecare, Coordination.
Abstract: This paper investigates the use of workflows to automate the delivery, coordination and monitoring of
home-care processes. Workflow models of these processes need to be customized, resilient to change,
collaborative and also need to account for the temporal aspects of care (treatment duration, frequency of a
medical acts, etc.). To this end, an approach based on ontologies (home-care ontology and BPMN
ontology), rules and patient’s profile is proposed for the construction of workflows supporting the
coordination and continuity of home-care processes.
1 INTRODUCTION
Home-care presents two majors problems, namely
coordination and continuity of care. These problems
have been highlighted by the document
MIN/DHOS-/DSS-CNAMT/2002/n°610, and
several others (Arundel et al, 2001) (Bricon-Souf et
al., 2005) and (Woodward et al., 2001). From our
studies in the home-care area, these drawbacks are
still valid. 1) Lack of inter-organizational
communication or coordination of care: there are
several associations, organizations, stakeholders that
manage employees to work at the patient's home.
However, there is no well-established means of
communication between these different stakeholders
(Arundel et al., 2001) and (Helleso et al., 2005).
Indeed, the only means used by many home-care
organizations to enable this communication, is the
so-called "liaison logbook" i.e. a physical notebook,
usually unstructured and kept at the patient's home
(Bastide et al., 2010) and (Lamine et al., 2010). 2)
Problem of care continuity: in the literature, there
are a multitude of definitions for continuity of care
like (Woodward et al., 2004) and (Shortell, 1976). In
homecare, the need for continuity stands at two
levels: the intervention level where the stakeholders
must ensure continuity and consistency of care
provided. But also, over time, during different steps
of patient treatment: moving from one institution to
another.
To ensure the coordination and continuity of
home-care, workflow management systems appear
to be appropriate. WfMC (Workflow Management
Coalition) (Hollingsworth, 1995) has defined
workflow. The role of a workflow management
system, in home-care, is to coordinate the work
involved by transmitting the necessary information
and tasks, with different stakeholders, depending on
the condition of the patient's intervention plan and
the role of the interveners. For example, the nurses’
day-to-day tasks vary according to the patients’
intervention plan, and the storage and exchange of
the relevant information would improve the
continuity of care.
However, the specific characteristics of
processes involved in homecare make the design of
their workflow a challenge. The use of ontology to
help in the design and evolution of these workflows
is proposed in this paper
In section 2 we discuss the need for workflow in
automating the home-care processes and we point
out the challenges for this. Section 3 is focused on
the presentation of proposal approach to design a
workflow for home-care. We discuss the related
work and our objectives on the section 4. Finally, we
conclude with a summary and outlook.
2 PROCESSES IN HOME-CARE
The activity of home-care gives rise to
communication and coordination problems. To
ensure the coordination and continuity of care, and
to improve its quality, the caregivers involved on
231
Zefouni S., Lamine E., Bastide R. and Pingaud H..
DESIGN AND EVOLUTION OF HOME-CARE WORKFLOWS USING ONTOLOGIES AND MODEL TRANSFORMATIONS.
DOI: 10.5220/0003779302310236
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2012), pages 231-236
ISBN: 978-989-8425-88-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

home-care are mandated to: 1) ensure the accuracy
of information, by automating the transmission of
information and by avoiding several transcriptions
for the same information; 2) Guarantee the timely
transmission of information to the appropriate
stakeholders, be it information about the patient's
condition or other logistical information; 3) Ensure
the transmission of information about the actual
medical or paramedical interventions performed by
the caregivers; 4) Ensure the storage of information
about the evolution of patient's health conditions.
2.1 Home-care Processes
In the literature, there are many research works
about home-care processes and particularly on
medical home-care (Jebalia, 2008), (Ben Bachouch
et al., 2009), (Lunn et al., 2003), (Hamek, 2005) and
(FNEHAD, 2009). In (FNEHAD 2009) the
"National federation of institutions hospitalization at
home" (FNEHAD) provides a mapping process for
patients under medical home-care, considering that
computer support is still underdeveloped in
institutions of medical homecare. This work aims to
structure information systems for home-care and
stands as a reference in this area, as it encompasses
all processes presented in other works. Figure 1
shows the main processes involved in home-care,
following ISO 9000: 2000 (ISO, 2000) which
classifies processes into three types: management,
operational (management of patient) and support
(Human resources, purchasing and logistics...).
Figure 1: Home-care mapping processes.
2.2 Workflow in Home-care
To cope with the drawbacks addressed above, we
suggest the automation of some processes of patient
management. In this paper, we focus on the delivery,
coordination and monitoring of care.
We distinguish two sets of processes: The first
set includes the "admission request",
"preadmission", "billing stays" and "discharge"
processes, which are prone to be automated by a
classical workflow management system. The second
set of processes includes "delivery of care" and
"coordination and monitoring of care" that are the
main topic of the present paper. The characteristics
of these processes make the design of workflows for
their automation a difficult task. This set of
processes has the following characteristics: 1) High
degree of customization (Dadam et al., 2000),
(Dazzil et al., 1997) and (Quaglinia et al., 2001):
each patient is a specific case due to particular health
conditions, social networking, geographic location,
etc. 2) Collaborative nature: (Arbaoui, 2008) and
(Cunin, 2000). The homecare processes present a
strong human component. Such a process is usually
long-running, distributed among several actors with
various levels of autonomy, and subject to dynamic
change (Liu et al., 2008). This collaborative process
is made of the assembly of distributed business
processes in partner organizations. Its behaviour is
related to the effective contributions of partners,
implemented jointly to achieve a common goal. 3)
Dynamicity: (Dadam et al., 2000) according to the
changing health of the patient and his environment.
In general, the process it required to quickly and
easily adapt to a changing environment. 4) Temporal
aspects: (Dadam et al., 2000) the tasks in homecare
have frequency and duration which are inconvenient
to represent in conventional workflow models.
3 PROPOSITION
3.1 Context
A workflow to deliver, monitor and coordinate
home-care is a sequence of interventions, as shown
in figure 2. This workflow depends on the
intervention plan defined by the professionals that
manage home-care institutions, and depends on the
profile of patient: diseases of patient, the presence of
family caregiver, etc.
Figure 2 shows - using BPMN (Business Process
Management Notation) - the sequence of
interventions performed within a two-days’
timeframe for a specific patient (Mrs Bissière that
has peritonitis vesicular, the case study detailed on
section 4), with the distribution of interventions
amongst stakeholders (nurse, physiotherapist, etc.).
The intervention plan defines the list of provisional
care to be performed, including actions and
treatment, prescribed or not, as well as the frequency
and schedules, and specify the appropriate
takeholders (nurse, cleaning agent, etc.) to perform
each actions.
HEALTHINF 2012 - International Conference on Health Informatics
232
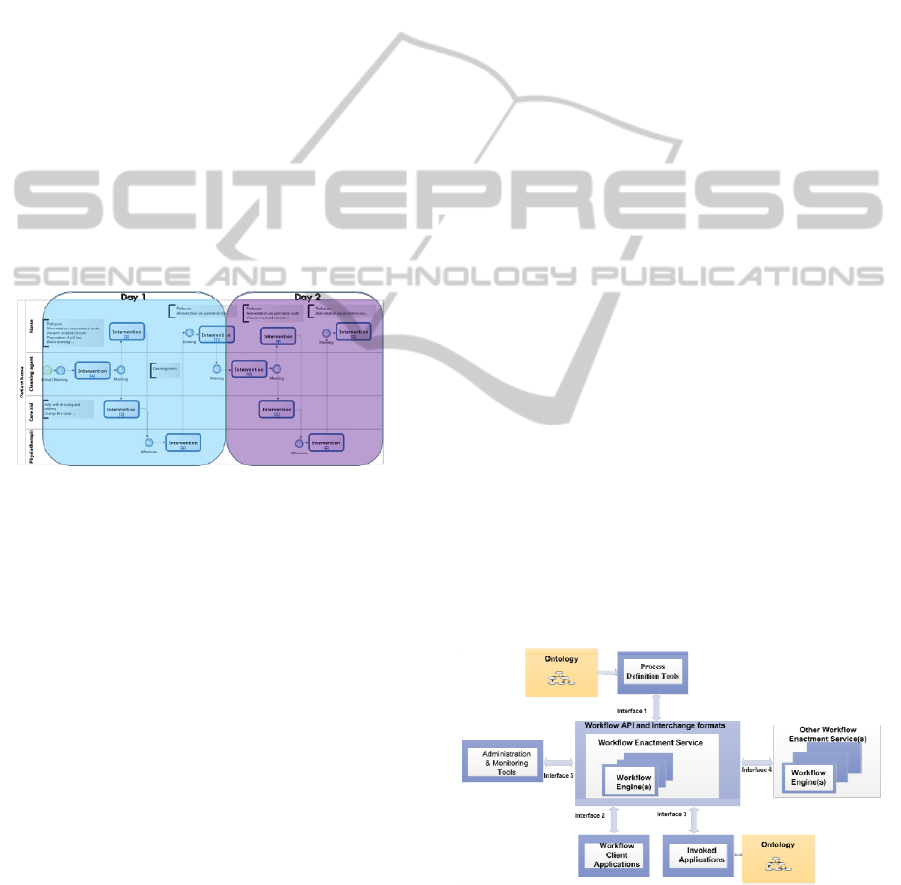
Figure 2 shows one pool representing the
patient's home, containing four lines representing
four different categories of actors involved in the
home-care of a specific patient: Nurse, Cleaning
agent, care aid and Physiotherapist. The first day
features five interventions: In the morning, the
Nurse has to perform perfusion, alimentation via
parenteral route, vacuum assisted closure,
preparation of pill box and blood drawing. In the
evening, she performs perfusion and alimentation
via parenteral route. Cleaning agent performs
cleaning room, Care aid performs help with dressing
and bathing and changes the cover, and
Physiotherapist performs physiotherapy. Second day
features the same five interventions but a difference
appears at tasks level of nurse in the morning, when
she performs only three tasks that are perfusion,
alimentation via parenteral route and vacuum
assisted closure. Each of these interventions is done
at a specific moment, e.g. the intervention of
cleaning agent must be performed in the morning
and be followed by the intervention of nurse.
Figure 2: Home-care Workflow.
An intervention is a sequence of three actions,
namely: 1) consult transmissions: consist in
consulting eventual transmissions (remarks, alert,
etc.) noted by a precedent stakeholder. 2) Inform on
performed acts: display the acts to be performed
during this intervention. It is the dynamic and
adaptable part of the intervention. It changes each
day, and for each stakeholder. 3) Transmit
information and alerts to other stakeholders: consist
in writing information about patient to inform or
alert others stakeholders about any change on
patient’s state or environment.
3.2 Proposed Approach to Design
Home-care Workflows
In recent years the concept of ontology has been
largely studied in computer science. Ontologies
allow for the sharing of knowledge to solve
problems of semantic heterogeneity. There are
several definitions of the concept ontology amongst
which we choose "ontology is a formal, explicit
specification of a shared conceptualization"
(Thomas, 1993).
The works we mostly refer to is that of (Valls et
al, 2001). The authors propose ontologies for
medical home-care. The design of these ontologies
is based on a model of home healthcare defined by a
European consortium of professional homecare,
European project K4Care.
Figure 3 shows the position of our proposal
within the reference architecture of workflow
management systems proposed by the WfMC
(Hollingsworth, 1995). This architecture consists of
five interfaces with the following components: 1)
process definition tools: tools for graphical
modelling of the process to automate and deploy.2)
Workflow client applications: any applications to
communicate to-do lists, messages, etc. to actors.
There are applications that interact with the user. 3)
Invoked applications: any application: DBMS, web
service, etc. called or invoked during the deployment
process automatically without intervention or
interaction of a user. 4) Other workflow enactment
services: any other workflow management system
able to communicate with the workflow
management system. This ensures the
interoperability between different workflows
management systems on the market. 5)
Administrative and monitoring tools: provides
access to admin tasks, such as suspension of a task,
stopping a process, etc.
Based on this reference architecture for
workflow management systems, we propose the use
of ontologies at level 1 and 3: 1) in the process
definition tool, the goal is to help the construction of
patient personalized care workflow. 2) At the
invoked applications, the goal is to guaranty
interoperability and flexibility of workflow at run
time.
Figure 3: Position of our proposition in the reference
architecture for workflows systems.
In this paper, we discuss workflow design. The
idea is to use ontologies for help designing the
workflow models for delivery, monitoring and
DESIGN AND EVOLUTION OF HOME-CARE WORKFLOWS USING ONTOLOGIES AND MODEL
TRANSFORMATIONS
233
coordination of homecare. The definition of an
intervention plan maps to the definition of a
workflow model. They both define the distribution
of tasks (care intervention) to actors (homecare
stakeholders) in order to achieve the specific goal to
improve the quality of home-care. But an
intervention plan defines frequency of intervention
and their duration over the treatment period.
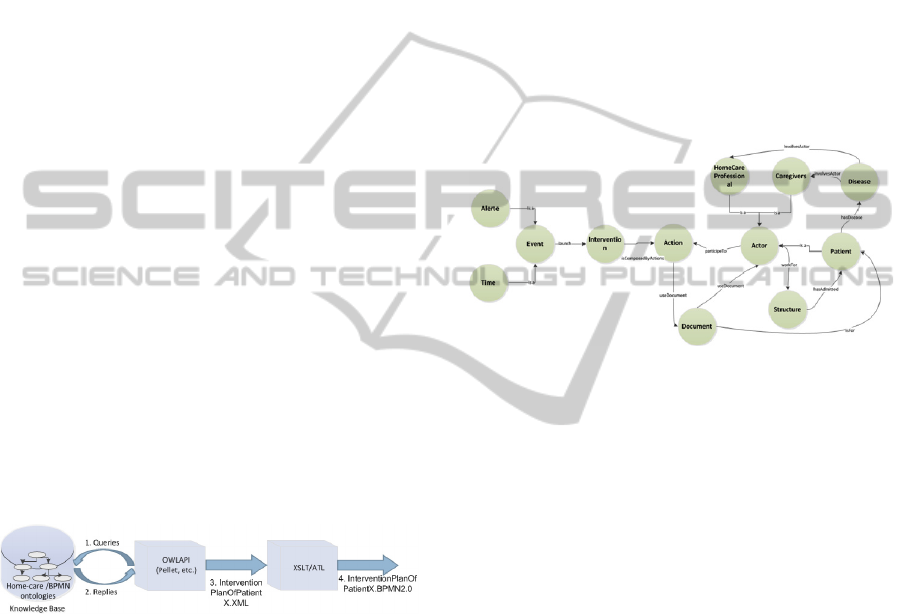
Transformation Process. Figure 4 shows the steps
to design customized BPMN process models for
each patient. The resulting process models will be
executed on workflow system.
We use these components: 1) a knowledge base
is a fusion of the home-care ontology (presented in
the next sub-section) and the BPMN ontology
(Ghidini et al., 2011). This knowledge base contains
patients’ profiles and rules about actors and actions
involved in treatment of a specific disease. 2) A Java
application is based on OWLAPI. OWLAPI is a java
API and reference implementation for creating,
manipulating and serializing OWL Ontologies. This
application queries the knowledge base about an
intervention plan of specific patient. The output of
this application is an XML file. The XML file
defines an intervention plan of specific patient as a
BPMN process model. 3) Tools are used for model-
transformation. The XML file resulted in the last
step must be transformed in a format suitable to be
interpreted by a workflow engine. Tools such as
ATL or XSLT are well suited, and allow
transforming the XML file into a standard BPMN
2.0 file.
Figure 4: Methodology for customized workflow design.
Embryo of Ontology for Home-care. Little
ontologies have been built in the home-care area, we
present here two projects: ABAH: An Agent-Based
Architecture for a Cooperative Information System
(Zarour et al., 2007), an Algerian project with the
goal to ensure interoperability in a multi agent
system. K4CARE European project (presented
above) with their two ontologies APO: Actor Profile
Ontology and CPO: Case Profile Ontology: CPO is
for representing symptoms, diseases, syndromes, etc.
Based on these ontologies, and our own surveys
of current practices in homecare, we propose a high
level ontology of home-care. It is represented as the
usual RDF triples where circle represent class
(concepts of home-care domain) connected by
relationship arrows (figure 5). For ease of
reading we have not presented the inverse functions
(relationship)
This ontology contains global information about
a structure and organization of home-care (actors,
roles, etc.) as well as profile of patients and the task
and actors needed for each disease.
To build this ontology of the home-care domain,
we followed a synthesis of different methodologies
in literature such as the ones proposed in (Uschold
and King, 1995), (Staab, 2001). The ontological
engineering process for building the home-care
ontology has been performed under four steps: 1)
Step 1: this step consists in identifying the goal to
define the ontology, the users of this ontology and
scenarios of using this ontology.
Figure 5: Main classes and relations of the ontology for
home-care.
2) Step 2: based on the result of the first step, we
define the basics concepts and relationships for this
ontology. 3) Step 3: we choose a tool to design the
ontology and start buiding frome the general
concepts to the more specific. 4) Step 4 is an
iterative step, consisting in maintiaining the the
consistency of the ontology.
4 CASE STUDY
The proposition consists in indicating the profile of
the patient: pathology, family caregiver, etc. The
application, based on the ontology and the patient
profile, proposes an intervention plan: set of actors
involved in home-care, tasks, sequence of
interventions and frequency of these interventions.
The solution is based on populating the ontology by
information of patient.
The case study concerns Mrs Bissière. She is 72
years old and has a Peritonitis Vesicular.
In the knowledge base we have this information.
Data that the professional introduces on the
Knowledge base
MrsBissière hasDisease
PeritonitisVesicular
HEALTHINF 2012 - International Conference on Health Informatics
234

Data that models general domain knowledge:
PeritonitisVesicular InvolvesActor:
Nurse, CleaningAgent, CareAid,and
PhysicalTherapist
We distinguish between two kinds of rules
(expressed in SWRL): 1) rules that relate to concepts
of home-care ontologies. 2) Rules that make a
mapping between the two ontologies (home-care
ontology and BPMN ontology).
These two types of rules are illustrated by the
example below: the first rule indicates that, if patient
X has a disease Y and disease Y involves the
intervention of actor Z, then we deduct actor Z. The
second rule indicates that, if there is an actor X then
there is a lane X (actor that is a concept from the
home-care ontology, mapped to the equivalent
concept of lane in the BPMN ontology).
Patient(?x),hasDisease(?x,?y),InvolvesAct
or(?y,?z)->Actor(?z)
Actor (?x)-> Lane (?x)
We request the knowledge base to include the
BPMN concepts to generate the home-care
processes. An example of query is presented below
Query
: lane and (Actor and
isInvolvedToCareDisease some (Disease and
(isDiseaseOfPatient value MrsBissière)))
Results: Nurse, CleaningAgent,CareAid and
PhysicalTherapist
In this case study, the knowledge base includes the
details of the patient profile: Mrs Bissière has
vesicular peritonitis. Then, we query the knowledge
base about the concepts of BPMN (lane) involved in
the process of home-care of Mrs Bissière. It is
possible to answer to this query based on knowledge
and rules contained in the knowledge base.
5 RELATED WORK
There are several studies on the use of workflow in
health-care, especially at the hospital. In the study of
(Dadam et al., 2000), the authors discuss the
challenges to elaborate workflow on clinical
domains. They point out the critical role of
workflows in the clinical area. Like Song and al
(Song et al, 2006) where the authors note that
improving healthcare workflows is very important
for improving healthcare quality and efficiency. The
authors of (Quaglinia et al., 2001) propose to design
of a flexible workflow for the management of a
stroke at hospitalization. This work is focused on a
specific problem (stroke case) whereas in the case of
home-care, each patient may suffer from various
diseases including stroke. In addition, the issues of
home-care differ from those encountered in the care
in the hospital, where all stakeholders work within
the same organization and use the same information
system, with the ability to see to discuss the status of
patients.
Many authors use ontologies combined with
workflow in order to enhance flexibility or agility. In
(Bouzguenda et al., 2008) the authors are interested
to a collaborative environment to implement the
WIO (Workflow Inter-Organizational). The authors
propose a solution based on multi-agents systems for
the execution of flexible web services to facilitate
partner search and ontologies for searching and
selecting the partners. In (Vieira et al., 2004) the
authors suggest use of ontologies to achieve flexible
execution of workflow. In our work, we are
interested in the design of customized workflow
models for each home-care patient. In our
knowledge there are no others works with the same
goals.
6 CONCLUSIONS
In order to improve communication and continuity
in home-care, we propose system architecture based
on a workflow engine to distribute tasks among
home-care stakeholders. However, the
characteristics of home-care processes make the
design and enactment of home-care workflow a
challenge. The goal of this architecture is to respect
the reference architecture for workflow management
systems while relying on ontologies to overcome
these identified obstacles. We propose an approach
using two ontologies (home-care ontology and
BPMN ontology) to help designing home-care
workflows. Our on-going work consists in
completing the transformation pipeline in order to
generate process model suited to be interpreted by a
workflow engine.
REFERENCES
Arundel C., Glouberman S., Kun L. 2001. Telehealth and
the global health network. In the 21st century, From
home care to public health informatics in Computer
Substudy, vol. 15.
Bricon-Souf N., Anceaux F., Bennani N., Dufresne E.,
Watbled L., 2005. A distributed coordination platform
for home care: analysis, framework and prototype.
International Journal of Medical Informatics.
Woodward C., Abelson J., Hutchison B., 2005. My home
is not my home anymore: improving continuity of care
DESIGN AND EVOLUTION OF HOME-CARE WORKFLOWS USING ONTOLOGIES AND MODEL
TRANSFORMATIONS
235

in homecare. The Canadian Health Services Research
Foundation web site, (online: www.chrsf.ca).
Helleso R., Sorensen L., Lorensena M., 2005. Nurses’
information management across complex health care
organizations. International Journal of Medical
Informatics
Bastide R., Zefouni S., Lamine E., 2010. The Homecare
Digital Ecosystem: an Information System Support
Architecture. In: IFIP Conference on Personal
Wireless Communications, Knowledge Village, Dubai,
UAE, IEEE
Lamine E., Zefouni S., Bastide R., 2010. A system
architecture supporting the agile coordination of
homecare services. In : IFIP Working Conference on
Virtual Enterprises (PRO-VE), St-Etienne, 2010, Vol.
336, Springer
Woodward C. A, Abelson J., Tedford S., Hutchison B.,
2004. What is important to continuity in home care?.
Perspectives of key stakeholders Social Science &
Medicine 58 177–192
Shortell, S., 1976. Continuity of Medical Care:
Conceptionalization and measurement. Medical Care,
14(5), 377–391.
Hollingsworth D., 1995. TheWorkflow Reference Model.
Technical report wfmctc- 1003, 1995, Workflow
Management Coalition.
Jebalia S. C., 2008. Modélisation et analyse de
l’organisation du fonctionnement des structures
d’hospitalisation à domicile. Thèse de doctorat,
l’Ecole Centrale des Arts et Manufactures Spécialité :
Génie Industriel.
Ben Bachouch R., Guinet A., Hajri-Gabouj S., 2009.
Certification des HAD VS certification ISO 9000.
Congrès International de Génie Industriel (CIGI09),
Bagnère de Bigorre, France, 10-12 Juin, Actes
CDROM.
Lunn K., Sixsmith A., Lindsay A., Vaarama M., 2003.
Traceability in requirements through process
modelling, applied to social care applications.
Information and Software Technology, 2003, p. 1045-
1052.
Hamek S., Anceaux F., SOUF N., Flahou S., 2005. La
prise en charge des soins lors de l’hospitalisation à
domicile : une analyse de la coopération asynchrone.
Journées Francophones d’Informatique Médicale.
FNEHAD:Fédération nationale des établissements
d'hospitalisation à domicile "Livre blan des systèmes
d'information en hospitalisation à domicile "Juin 2009.
ISO (2000). "International Organization for
Standardization:ISO 9000:2000: Quality Management
Systems" – Fundamentals and Vocabulary.
Beuth,Berlin.
Dadam P., Reichert M., Kuhn K., 2000. Clinical
Workflows - The Killer Application for Process-
oriented Information Systems? Proc. of Int'I
Conference on Business Information Systems, Pozan,
Poland, April 2000, Springer-Verlag, 2000, pp.36-59.
Dazzil L., Fassino C., Saracco R., Quaglini S., Stefanelli
M., 1997. A Patient Workflow Management System
Built on Guidelines. Proc. of AMIA, 146-150,
Nashville, TN.
Quaglinia S., Stefanellia M., Lanzolaa G., Caporussob V.,
Panzarasab S., 2001. Flexible guideline-based patient
careflow systems. Artificial Intelligence in Medicine
22.
Arbaoui S., Lamine E., Di Mascolo M., 2008. Les
systèmes d’information pour la prise en charge de
patients à domicile: Besoins, Usages et Verrous. 4e
conférence francophone en Gestion et Ingénierie des
systèmes hospitaliers (GISEH), ISBN 978-2-8399-
0316-5, CD-ROM,Lausanne.
Cunin P., 2000. The PIE Project: An Introduction. In
Proceedings of the 7th European Workshop in
Software Process Technology – EWSPT’2000,
Kaprun, Austria.
Liu C., Li Q., Zhao X., 2008. Challenges and opportunities
in collaborative business process management:
Overview of recent advances and introduction to the
special issue. Springer Science and Business Media,
LLC.
Thomas R. Gruber., 1993. Towards Principles for the
Design of Ontologies Used for Knowledge Sharing. In
N. Guarino and R. Poli, editors, Formal Ontology in
Conceptual Analysis and Knowledge Representation,
Deventer, The Netherlands, 1993. Kluwer Academic
Publishers.
Valls A., Gibert K., Sánchez D., Batet M., 2010. Using
ontologies for structuring organizational knowledge in
Home Care assistance. In international journal of
medical informatics 7 9 (2010) 370.
Ghidini, C. D., Francescomarino, M. Rospocher, P.
Tonella,and L. Serafini, 2011. Semantics based aspect
oriented manage-ment of exceptional flows in business
processes. IEEE Transactions on Systems, Man, and
Cybernetics, Part C:Applications and Reviews.
Zarour, K., and Zarour, N., 2007. Vers un système
d'information coopératif pour la prise en charge des
soins à domicile: une architecture basé agent. Memoire
de magister, Université Mentouri de Constantine,
laboratoire LIRE.
Uschold, M., and King, M., 1995. Towards a
Methodology for Building Ontologies. In D. Skuce
(Ed.), IJCAI’95 Workshop on Basic Ontological Issues
in Knowledge Sharing, (pp. 6.1-6.10). Montreal,
Canada.
Staab, S., Schnurr, H. P., Studer, R., and Sure, Y., 2001.
Knowledge Processes and Ontologies. IEEE
Intelligent Systems, 16 (1), 26–34.
Song X., Hwong B., Matos G., Rudorfer A., Nelson C.,
Han M., Girenkov A., 2006. Understanding
Requirements for Computer-Aided Healthcare
Workflows: Experiences and Challenges. ICSE’06,
May 20-28, 2006, Shanghai, China. ACM 1-59593-
085-X/06/0005.
Bouzguenda L., Bouaziz R., Andonoff E., 2008. Using
ontologies for coordination in loose Inter-
Organizational Workflow. RCIS, 2008, p. 123-132.
Vieira, T. A. S. C., M. A. Casanova, and L. G. Ferrao,
2004. An Ontology-Driven Architecture for Flexible
WorkflowExecution. In WebMedia & LA-Web Joint
Conference. 2004.
HEALTHINF 2012 - International Conference on Health Informatics
236
