
A MOBILE COLLABORATION AND DECISION SUPPORT SYSTEM
FOR THE MEDICAL EMERGENCY DEPARTMENT
Dominique Brodbeck
1
, Markus Degen
1
and Maximilian Reiß
2
1
University of Applied Sciences Northwestern Switzerland, Olten, Switzerland
2
Technical University of Munich, Munich, Germany
Keywords:
Mobile technologies for healthcare applications, Medical informatics.
Abstract:
A hospital emergency department is a complex work environment, where the availability of the right informa-
tion at the right time is crucial for efficient and safe operation. The current technology in use for communica-
tion and information management is mostly based on telephones and stationary personal computers. Modern
smartphones with their computational power, voice, image, and video capabilities have the potential to play
a significant role in improving the flow of information in the emergency department. We developed a system
that explicitly supports the work flows of an emergency department. In addition to mobile access to patient
data and notifications about the availability of diagnostic findings, it provides the possibility to supply media
captured on-site to the patient record, and directly supports the consultation process.
1 INTRODUCTION
The treatment of emergency patients is an important
function of hospitals. The operation of an emergency
department is different from that of other departments
in several ways. Events are not foreseeable and ac-
tions are often time-critical. Furthermore, doctors
typically treat emergency patients in a parallel way.
After the anamnesis, diagnostic test (x-ray, lab test,
MRI, etc.) are administered. Patients need to wait un-
til the results are ready and then a doctor sees them
again to decide on treatments. Meanwhile, the doctor
is caring for other patients. During this process, the
doctors on duty in the emergency room need to con-
sult with experts from specialized disciplines (e.g. or-
thopedics). The experts are typically difficult to reach,
not present on site or in a mobile situation. Another
aspect of hospitals is that doctors’ competence devel-
opment is not based on formal acts of education, but
rather embedded in daily practice and brought on by
cooperation and communication with colleagues and
experts. Because of these characteristics, the efficient
operation of an emergency department is highly de-
pendent on the availability of the right information at
the right time, and the availability of multimedia com-
munication channels.
At the University Hospital Basel, we encountered
several issues where the flow of information is not op-
timal. The problem with standard diagnostics is that
processes are still paper-based or server-centric. Doc-
tors don’t receive information about the results - or
even about the availability of the results - at the time
it is available at the place where they currently are, but
instead have to remember and go and look for it. The
problem with expert consultations is that experts are
often not available (especially at off-hours) or remote.
The consultations however are carried out by phone or
paper-based channels (fax) with no support for media
such as images or video. All these processes are not
integrated well, and the generated knowledge can not
be captured or managed to support doctors’ learning.
We presume that the situation is similar in other
hospitals as well. We therefore set out to conceptu-
alize, develop, and evaluate a distributed, mobile de-
cision support system for the emergency department.
The system has the following goals:
• Improve the flow of information by pushing no-
tifications about new information to doctors and
making it available in mobile contexts
• Support the consultation process by providing
workflow-aware and multimedia enriched com-
munication
• Provide integrated access to the system on differ-
ent mobile and stationary platforms
In the following sections we describe related
work, the techniques we used to develop the concept,
and the system that we built based on this concept.
237
Brodbeck D., Degen M. and Reiss M..
A MOBILE COLLABORATION AND DECISION SUPPORT SYSTEM FOR THE MEDICAL EMERGENCY DEPARTMENT.
DOI: 10.5220/0003780102370242
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2012), pages 237-242
ISBN: 978-989-8425-88-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

2 BACKGROUND
The main technology for communication in a typical
hospital today is still the voice-based telephone.
With smartphones (e.g., iPhones) becoming more
and more widespread among medical doctors work-
ing in hospitals, they not only begin to replace the
”phone-only” devices for every-day work use, but
with the possibility to tailor them with specialized ap-
plications, they are now also becoming an information
access tool.
There are a number of medical applications avail-
able for the iPhone today. They range from electronic
versions of compendia (PSPsmartsoft, 2011), over
mobile viewers for DICOM images (Pixmeo SARL,
2011), to specialized software packages for emer-
gency doctors (Pepid, 2011).
Mor
´
an et al. showed (Mor
´
an et al., 2007) that a
typical hospital worker is using more time to man-
age information than on direct patient care. Also their
work showed, that there is a constant need for access
to relevant information in a heterogenous device en-
vironment.
Several publications researched the use of Per-
sonal Digital Assistants (PDAs) and smartphones in
hospitals (Gamble, 2010), (Fischer et al., 2003) and
identified a big potential for their use in clinical daily
work. The work of (Carroll et al., 2002) discusses
some important issues that can arise when using PDA
devices to access patient records and inputing data,
primarily due to the physical limitations of the devices
(e.g. small screen, input of long texts is tedious).
Banitsas et al. showed in (Banitsas et al., 2006)
and (Banitsas et al., 2004) the potential of the use
of mobile video conferencing devices in the process
of medical consultations. They also showed, that
the current available speed of wireless transmission
networks is sufficient for most tele-consultation pro-
cesses.
Two major trends seem to emerge in the mobile
device market:
• With the smartphones adapting more and more of
the traditional PDA (Personal Digital Assistant)
functionality, they will replace the PDA-only de-
vices eventually.
• Because telecom providers offer products that al-
low the use of mobile phones on a campus set-
ting for unlimited cost-free internal calls, they will
take over the role of the traditional cordless phone
systems
The system described in (Hameed et al., 2008)
is somewhat similar to the one presented here, with
one major difference: Instead of focusing on plat-
form independence and using web technologies, our
approach is to make best use of the native user inter-
face elements available on the client target platforms.
This approach allows to create an optimal user expe-
rience on every platform.
(Choi et al., 2006) proposed a mobile information
system that is integrated in the clinical IT environ-
ment, and uses the HL7 message stream to generate
notifications (e.g., when new lab results for a given
patient are available).
3 DEVELOPING THE CONCEPT
In order to account for the transformative potential
of the system and the wide range of stakeholders in-
volved, we chose a decidedly user-centered approach
to developing the concept and building the system.
Contextual observations and inquiries were per-
formed by spending several days in the emergency
department, following doctors as they performed their
duties. This resulted in a good understanding of the
existing user tasks and workflows, and formed a ba-
sis for the development of scenarios. We developed
both text and video scenarios that show a series of en-
visioned use cases for the new system (Pimmer et al.,
2011).
The scenarios were presented to the doctors and
their feedback captured in semi-structured interviews.
Analysis of the interviews showed (Pimmer et al.,
2011) that features such as
• mobile access to patient data and findings,
• notifications about the availability of diagnostic
findings,
• possibility to supply media captured on-site to the
patient record,
• possibility to ”bookmark” cases with associated
data for later use in different contexts,
• and dedicated support of the consultation work-
flow
were considered the most useful by the doctors. Other
features such as three-way video conferencing, white-
board functionalities, or video streaming were as-
signed less potential.
From these insights we were able to extract a list
of prioritized requirements. For the implementation
of these requirements we chose an agile development
process with four-week iteration cycles. The mobile
and desktop user interfaces were conceptualized and
verified using paper prototypes. The prototypes were
evaluated with doctors on duty in the emergency de-
partment using think-aloud protocols.
HEALTHINF 2012 - International Conference on Health Informatics
238
3.1 Consultation Process
Consultation is one of the key processes to be sup-
ported by the system. Emergency departments are of-
ten staffed with junior doctors. If they encounter a
situation outside of their medical expertise, they need
to consult with a senior doctor or a medical expert
from a specialized discipline. At the hospital that we
observed, this consultation process is currently per-
formed through phone calls and paper forms. Obser-
vations about injuries or symptoms need to be com-
municated with written or spoken words.
We analyzed the consultation process and identi-
fied the four different states shown in Figure 1.
!"#$%&"'"(
)**"+&"(
,"($*-./(0*&0'/'"12"%&%
*03%2.&-&$03
4$3$%5"(
603%2.&-&$03
(0*27"3&-&$03
8$."(
,"($*-./*03%2.&-3&
'"-(%/12"%&$03/
,"($*-./*03%2.&-3&
-**"+&%/*03%2.&-&$03
9""3
,"($*-./*03%2.&-3&
&'-3%8"'%/*03%2.&-&$03/&0/
0&5"'/*03%2.&-3&
,"($*-./*03%2.&-3&
*.0%"%/*03%2.&-&$03
Figure 1: The consultation process modeled as a state-
machine.
The functionality to support the consultation pro-
cess in our system was modeled after this concept,
and is fully integrated with the rest of the function-
ality. Requests for consultation can be initiated and
received directly on the smartphone. The inquiring
doctor is able to see the current state of a consultation
at all times. The medical consultant is reminded by
the system if an action is outstanding. Consultations
can be enriched by media files to facilitate the voice
communication.
4 HIGH-LEVEL ARCHITECTURE
OF THE SYSTEM
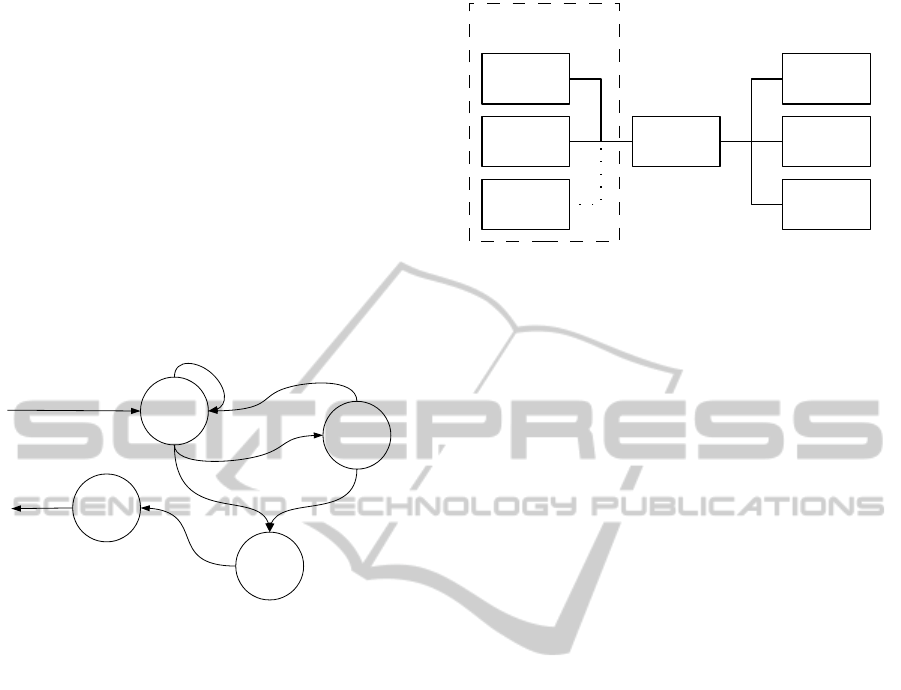
Figure 2 shows the high level architecture of the sys-
tem. The communication between the backend sys-
tem and the end-user clients was realized using a cus-
tom message protocol, based on an efficient wire pro-
tocol (See Section 4.5).
One of the non-functional key requirements was,
that the system should be accessible by different
clients. We therefore defined a message protocol
and implemented several different clients for the sys-
tem. In order to increase acceptance and usability,
!"#$%&
'(!&%)
*%+,$!+
'(!&%)
-&./)$0
'(!&%)
123/&%+
45.)&6
784
-94
"1:
7$.0!)2(
8%;,2.),<3)<,&
Figure 2: High-level architecture of the system, and inte-
gration into the hospital IT infrastructure. The backend sys-
tem connects to the Hospital Information System (HIS), the
Document Management System (DMS) and the Telephone
System (PBX, planned)
the client applications were developed to have the
look&feel of their respective platforms, rather than a
”one for all GUI”.
4.1 Backend
The backend provides several functions:
• Aggregation of the data of several hospital IT sys-
tems
• Bi-directional data transformation for the hospital
IT systems’ data from and to the mobile devices
• Authentication for the mobile devices via the hos-
pital IT authentication system
• Support for the discussion conference feature as
well as the enhanced consultation feature
• Sending of notifications to the clients, e.g., if new
data is available or if some action is overdue
The reason for the data aggregation of the different
IT systems of the hospital is that the mobile devices
should present one aggregated access to the patient,
in contrast to the legacy desktop approach in which
every data supplier has its own interaction user inter-
face. On a mobile device where one app is a men-
tal equivalent to a tool for a specific task, different
apps to access the patients’ data would break with the
users’ expectation. Given the two choices to aggre-
gate the data either on the mobile device or in the
backend, the system was designed to aggregate in the
backend. The reason for this decision was the heavy
load (CPU, memory and storage) that this operation
causes.
The second backend part, the bi-directional data
transformation, is needed for several reasons. There
are several data formats that the mobile device cannot
display directly, and even if it can display the format,
it might have issues with the large size of the data
A MOBILE COLLABORATION AND DECISION SUPPORT SYSTEM FOR THE MEDICAL EMERGENCY
DEPARTMENT
239

(e.g., there is a limitation on the mobile device for
how large an image can be). Another reason for the
data adaptation is, that depending on the network con-
nection (and other factors) the data might not be avail-
able fast enough on the mobile device, even though a
reduced version of this data (that can be transferred
faster) would still be sufficient for the current use case
of the doctor. In the other direction, the mobile de-
vices might produce data in a format that the IT sys-
tems of the hospital do not understand. In this case
the backend would transcode the data into a format
that the hospital systems can understand.
Since the backend is the one place to monitor all
events and notifications in the system, it observes
these and can issue special notifications for a mo-
bile device of a specific doctor, e.g., ”New MRI im-
ages are available for patient X”. In case that a mo-
bile device client is not reachable, most notifications
are queued until the mobile device becomes available
again. If the notification passes an ”importance” fil-
ter, a short version of the notification is additionally
sent to the mobile device as push notification, via the
platform’s push notification service.
4.2 Mobile Client on iOS (iPhone)
The primary mobile client was developed for the iOS
platform, mainly focused on the iPhone. With the
iPhone client it is possible to participate in the three
main activities that our system supports:
• It is possible to view patient record data aggre-
gated from several backend systems (document
management system, RIS, etc.),
• it is possible to actively supply diagnostic findings
(images, videos, audio recordings, etc.),
• and it is possible to participate in the medical de-
cision making process by helping with the con-
sultation workflow, and by providing audio con-
ferences with the possibility to share and discuss
patient data in this conference.
Figure 3(a) shows the typical listing of a doctor’s
current patients. In this view and the views reachable
from this list, the doctor can access the patient record
data, the patient master data, the previous cases with
their diagnostics and documents, and the lab record
and current consultations, as shown in Figure 3(b).
The third main activity is the discussion support.
On a shared document, the doctor can mark regions,
as shown in Figure 3(c). These markers are visible to
the other doctors participating in the discussion con-
ference. In this way, our system uses a distributed
discussion model - each doctor can supply her own
data, and if she wants to show the data to others, then
she can draw their attention to the data supplied by
her. This can be done via the audio connection.
4.3 Mobile Client on Android
Since not only iOS-based smartphones but also
Android-based ones are present in the clinical land-
scape, it was a requirement to also implement a mo-
bile client for Android systems, at least as a ”proof of
concept”.
We opted to not simply port the user interface
of the iPhone to the Android platform, but reimple-
mented the interface using the look and feel of An-
droid applications. Because the implementation lan-
guage for the desktop client was also Java, much of
the code talking to the backend system could simply
be reused in the Android client.
4.4 Desktop Client
While doctors are frequently on the move, there are
still situations where they sit near a desktop computer,
or where larger input and output hardware is more
convenient for a task (e.g. text entry), or where pa-
tient cases are discussed in front of larger audiences
(e.g. morning status report). We therefore decided to
develop a desktop client for stationary use that takes
advantage of the increased computational resources
compared to the mobile clients.
In particular, there are less screen space limita-
tions for the desktop client, and the most important
information can always be shown on the main screen,
providing an ”at a glance” overview while at the same
time allowing quick and easy access to details.
Figure 4 shows the user interface of the desktop
client. On the left side, a list with all current patients
in the emergency department is shown. More infor-
mation can be obtained by simply hovering over a pa-
tient entry. In the lower left, a spatial overview of all
beds in the emergency department is shown, together
with the current state (red: occupied, green: free).
The right side shows a patient’s details, including the
master data, data from the current as well as from pre-
vious cases, and all the information about pending and
finished consultations. All the views are tightly linked
through interactions to provide the big picture.
4.5 Communication Protocol
The communication between the clients and the back-
end is twofold:
• A set of control messages were defined to syn-
chronize the application data between the clients
HEALTHINF 2012 - International Conference on Health Informatics
240
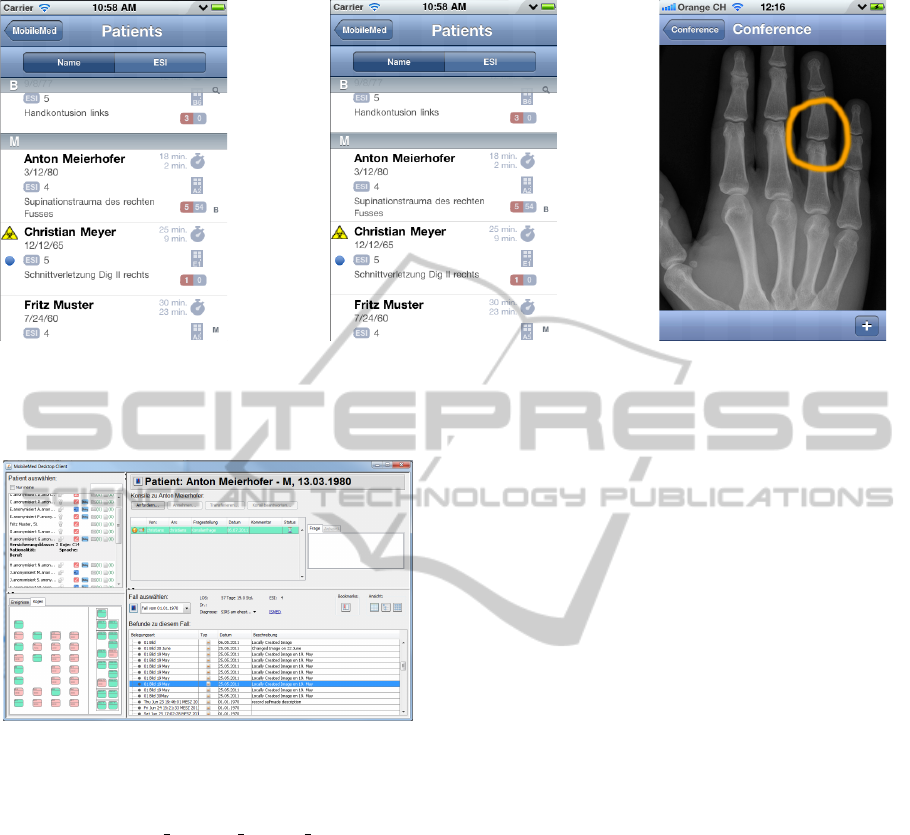
(a) Patient Overview (b) Patient Case Data (c) Conference discussion
Figure 3: (a) Screenshot of the iPhone UI showing the patient overview (b) Screenshot of the iPhone UI showing the patient’s
data sections. The actual document group names are pulled from the hospital systems. (c) Screenshot of the iPhone UI
showing a media discussion in a conference.
Figure 4: User interface of the desktop client.
and the backend. These messages were transmit-
ted via socket connections, and Google Protocol
Buffers (Google Protocol Buffers Team, 2011)
were used for efficient bit stuffing.
• Since there would be little gain to transfer media
data (images, audio, video etc.) via the bit stuffing
channel, it is retrieved via an HTTPS connection
by the clients. Sending JPEGs etc. encoded with
Protocol Buffers would only marginally improve
the message size with some conversion overhead.
4.6 Connection to the Hospital IT
Since our system relies on live data, it has to be con-
nected to the hospital’s IT systems. The connections
are made via ”adapters” in the backend that are in-
terchangeable, should the system be used in another
hospital with a different IT infrastructure.
4.6.1 Hospital Information System (HIS)
The ”information backbone” of a typical hospital con-
sists of an HL7 message stream connecting all subsys-
tems, and parsing this stream is the best information
source, if live data of a patient is needed. We wanted
to know the current location (i.e., bed) of every pa-
tient, in order to provide a graphical layout of the
load of the emergency department. In our case how-
ever, this information is not communicated via HL7
but handled within the HIS directly. We therefore had
to connect to the HIS instead of listening to the HL7
stream, using a database connection with read-only
access, and polling it regularly by the backend to de-
tect changes in patient location.
4.6.2 Document Management System (DMS)
A major part of the clients handles the visualization of
documents stored in the Document Management Sys-
tem (DMS). The DMS provides SOAP Web services
that can be used to upload documents and to search
and retrieve documents stored in the DMS. The doc-
uments retrieved from the DMS are stored in a smart
cache in the backend for some time. Also, lower size
versions of the images for the mobile clients are gen-
erated in the backend.
5 EVALUATION
The system will be evaluated in a trial in early 2012
in the emergency department of the University Hos-
pital Basel. It is planned to involve several medi-
A MOBILE COLLABORATION AND DECISION SUPPORT SYSTEM FOR THE MEDICAL EMERGENCY
DEPARTMENT
241

cal doctors that will be provided with smartphones
running the application. The participants will follow
their daily routine, treating patients in the emergency
department, and use our system to record and store
media files (photos, videos, audio files) and issue re-
quests for consultations via the functions of our sys-
tem.
Also several senior doctors and medical experts
will be equipped with the desktop version of the client
on their workstation. This ensures that they can be
reached by requests for consultation.
All involved medical doctors will be asked to par-
ticipate in a structured interview after the trial. The
data from the interviews will allow us to evaluate the
usability of the system as a whole, and of the specific
client user interfaces in particular.
6 CONCLUSIONS AND FUTURE
WORK
We have built a mobile collaboration and decision
support system that can enhance and speed up the pro-
cesses in an emergency department of a hospital.
The features of the system were defined and devel-
oped in close collaboration with the end users (med-
ical doctors) and the first feedbacks were encourag-
ing. The system will be evaluated in a trial in early
2012 in the University Hospital Basel. The data gath-
ered from log files during the trial and the findings of
the interviews conducted after the trial with involved
medical doctors, will allow us to examine and judge
the usefulness of the system.
ACKNOWLEDGEMENTS
This work was supported by funding from the
Swiss Innovation Promotion Agency CTI. The au-
thors would like to thank the University Hospital in
Basel, the Academy for medical training and simula-
tion AMTS and Agfa Healthcare for their support.
REFERENCES
Banitsas, K., Georgiadis, P., Tachakra, S., and Cavouras, D.
(2004). Using handheld devices for real-time wireless
teleconsultation. Conf Proc IEEE Eng Med Biol Soc,
4.
Banitsas, K., Georgiadis, P., Tachakra, S., and Cavouras, D.
(2006). Mobile consultant: combining total mobility
with constant access. In Engineering in Medicine and
Biology Society, 2006. EMBS ’06. 28th Annual Inter-
national Conference of the IEEE, pages 5248 –5251.
Carroll, A. E., Saluja, S., and Tarczy-Hornoch, P. (2002).
The implementation of a Personal Digital Assistant
(PDA) based patient record and charting system:
lessons learned. Proceedings / AMIA ... Annual Sym-
posium. AMIA Symposium, pages 111–5.
Choi, J., Yoo, S., Park, H., and Chun, J. (2006). Mo-
bileMed: a PDA-based mobile clinical information
system. IEEE transactions on information technology
in biomedicine : a publication of the IEEE Engineer-
ing in Medicine and Biology Society, 10(3):627–35.
Fischer, S., Stewart, T. E., Mehta, S., Wax, R., and Lapin-
sky, S. E. (2003). Handheld computing in medicine.
Journal of the American Medical Informatics Associ-
ation, 10(2):139–149.
Gamble, K. H. (2010). Wireless Tech Trends 2010. Trend:
smartphones. Healthcare informatics the business
magazine for information and communication sys-
tems, 27(2):24, 26–27.
Google Protocol Buffers Team (2011). Google
Protocol Buffers Project Page. Avail-
able online at http://code.google.com/intl/de-
DE/apis/protocolbuffers/ Visited on September,
6th, 2011.
Hameed, S. A., Hassa, A., Shabna, S., Miho, V., and Khal-
ifa, O. (2008). An efficient emergency, healthcare, and
medical information system. International Journal of
Biometrics and Bioinformatics (IJBB), pages 1–9.
Mor
´
an, E. B., Tentori, M., Gonz
´
alez, V. M., Favela, J., and
Mart
´
ınez-Garcia, A. I. (2007). Mobility in hospital
work: towards a pervasive computing hospital envi-
ronment. International Journal of Electronic Health-
care, 3(1):72–89.
Pepid (2011). iPhone Emergency Physicians SW. Available
online at http://www.pepid.com/products/iPhone-
Emergency-Physicians-Software.asp Visited on
September, 6th, 2011.
Pimmer, C. P., Pachler, N., and Genewein, U. (2011).
The potential of smartphones to mediate intra-hospital
communication and learning practices of doctors. pre-
liminary results from a scenario-based study. Pro-
ceeding oft he Mobile learning conference: Cross-
ing boundaries in convergent environments, Bremen,
pages 151–4.
Pixmeo SARL (2011). Osirix HD Product Page. Available
online at http://itunes.apple.com/app/id419227089
Visited on September, 7th, 2011.
PSPsmartsoft (2011). iKomp Product Page. Available
online at http://www.appannie.com/ikomp/ Visited on
September, 7th, 2011.
HEALTHINF 2012 - International Conference on Health Informatics
242
