
TWITTER IMPROVES SEASONAL INFLUENZA PREDICTION
Harshavardhan Achrekar
1
, Avinash Gandhe
2
, Ross Lazarus
3
, Ssu-Hsin Yu
2
and Benyuan Liu
1
1
Department of Computer Science, University of Massachusetts Lowell, Massachusetts, U.S.A.
2
Scientific Systems Company Inc, 500 West Cummings Park, Woburn, Massachusetts, U.S.A.
3
Department of Population Medicine, Harvard Medical School, Boston, Massachusetts, U.S.A.
Keywords:
Flu trends, Online social networks, Prediction.
Abstract:
Seasonal influenza epidemics causes severe illnesses and 250,000 to 500,000 deaths worldwide each year.
Other pandemics like the 1918 “Spanish Flu” may change into a devastating one. Reducing the impact of
these threats is of paramount importance for health authorities, and studies have shown that effective inter-
ventions can be taken to contain the epidemics, if early detection can be made. In this paper, we introduce
the Social Network Enabled Flu Trends (SNEFT), a continuous data collection framework which monitors flu
related tweets and track the emergence and spread of an influenza. We show that text mining significantly
enhances the correlation between the Twitter and the Influenza like Illness (ILI) rates provided by Centers
for Disease Control and Prevention (CDC). For accurate prediction, we implemented an auto-regression with
exogenous input (ARX) model which uses current Twitter data, and CDC ILI rates from previous weeks to
predict current influenza statistics. Our results show that, while previous ILI data from CDC offer a true (but
delayed) assessment of a flu epidemic, Twitter data provides a real-time assessment of the current epidemic
condition and can be used to compensate for the lack of current ILI data. We observe that the Twitter data is
highly correlated with the ILI rates across different regions within USA and can be used to effectively improve
the accuracy of our prediction. Our age-based flu prediction analysis indicates that for most of the regions,
Twitter data best fit the age groups of 5-24 and 25-49 years, correlating well with the fact that these are likely,
the most active user age groups on Twitter. Therefore, Twitter data can act as supplementary indicator to gauge
influenza within a population and helps discovering flu trends ahead of CDC.
1 INTRODUCTION
Seasonal influenza epidemics result in about three to
five million cases of severe illness and about 250,000
to 500,000 deaths worldwide each year (Jordans,
2009). In 1918, the so-called “Spanish flu” killed an
estimated 20-40 million people worldwide, and since
then, human to human transmission capable influenza
virus has resurfaced in a variety of particularly viru-
lent forms much like “SARS”, “H1N1” against which
no prior immunity exists resulting in a devastating sit-
uation with million of casaulties. Reducing the im-
pact of seasonal epidemics and pandemics such as the
H1N1 influenza is of paramount importance for pub-
lic health authorities. Studies haveshown that preven-
tive measures can be taken to contain epidemics, if an
early detection is made or if we have some form of
an early warning system during the germination of an
epidemic (Ferguson et al., 2005; Longini et al., 2005).
Therefore, it is important to be able to track and pre-
dict the emergence and spread of flu in the population.
The Center for Disease Control and Prevention
(CDC) (Centers for Disease Control and Prevention,
2009) monitors influenza-like illness (ILI) cases by
collecting data from sentinel medical practices, col-
lating reports and publishing them on a weekly basis.
It is highly authoritative in the medical field but as di-
agnoses are made and reported by doctors, the system
is almost entirely manual, resulting in a 1-2 weeks
delay between the time a patient is diagnosed and the
moment that data point becomes available in aggre-
gate ILI reports. Public health authorities need to be
forewarned at the earliest to ensure effective preven-
tive intervention, and this leads to the critical require-
ment of more efficient and timely methods of estimat-
ing influenza incidences.
Several innovative surveillance systems have been
proposed to capture the health seeking behaviour
and transform them into influenza activity. Some of
them include monitering call volumes to telephone
triage advice lines (Espino et al., 2003), over the
counter drug sales (Magruder, 2003), patients visit
61
Achrekar H., Gandhe A., Lazarus R., Yu S. and Liu B..
TWITTER IMPROVES SEASONAL INFLUENZA PREDICTION.
DOI: 10.5220/0003780600610070
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2012), pages 61-70
ISBN: 978-989-8425-88-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

logs to Physicians for flu shots. Google Flu Trends
uses aggregated historical log on online web search
queries pertaining to influenza to build a comprehen-
sive model that can estimate nationwide ILI activity.
In this paper, we investigate the use of novel data
source, Twitter, which takes advantage of the timeli-
ness of early detection to provide snapshot of the cur-
rent epidemic condition and make influenza related
predictions on what may lie ahead, on a daily or even
hourly basis. We sought to develop a model which
estimates the number of physician visits per week re-
lated to ILI as reported by CDC.
Our approach assumes Twitter users within United
States as “sensors” and collective message exchanges
showing flu symptoms like “I have Flu”, “down with
swine flu” as early indicators and robust predictors
of influenza. We expect these posts on Twitter to
be highly correlated to the number of ILI cases in
the population. We analyze tweets, build prediction
models and discover trends within data to study the
characteristics and dynamics of disease outbreak. We
validite our model by measuring how well it fits the
CDC ILI rates over a course of two years from 2009
to 2011. We are interested in looking at how the sea-
sonal flu spreads within the population across differ-
ent regions of USA and among different age groups.
In this paper, we extend our preliminary analy-
sis (Achrekar et al., 2011), and provide continuous
study of tracking emergence and spread of seasonal
flu in the year 2010-2011. Twitter data which demon-
strated high correlation with CDC ILI rate last year,
was suppressed by spurious messages and so text min-
ing techniques were applied. We show that text min-
ing can significantly enhance the correlation between
the Twitter data and the ILI data from CDC, providing
a strong base for accurate prediction of ILI rate.
For prediction, we build an auto-regression with
exogenous input (ARX) model where ILI rate of pre-
vious weeks from CDC forms the autoregressive por-
tion of the model, and the Twitter data serve as exoge-
nous input. Our results show that while previous ILI
data from CDC offer a realistic (but delayed) measure
of a flu epidemic, Twitter data provides a real-time
assessment of the current epidemic condition and can
be used to compensate for the lack of current ILI data.
We observe that the Twitter data are in fact highly cor-
related with the ILI data across the different regions
within United States.
Our age-based flu prediction analysis indicates
that for most of the regions, Twitter data best fit the
age groups of 5-24 and 25-49 years, suggesting that
these are likely the most active age groups using Twit-
ter. Using fine-grained analysis on user demographics
and geographical locations along with its prediction
capabilities will provide public health authorities an
insight into existing seasonal flu activities.
This paper is organized as follows: Section 2 de-
scribes applications that harness the collective intel-
ligence of Online Social Network (OSN) users, to
predict real-world outcomes. In Section 3, we give
a brief introduction to our data collection and mod-
elling methodolgy. In Section 4, we introduce our
data filtering technique for extracting relevant infor-
mation from Twitter dataset. Detailed data analysis
are performed to establish correlation with CDC re-
ports on ILI rates. Then we go one step further and
introduce our influenza prediction model in Section
5. In Section 6, we perform Region-wise and Age-
based analysis of flu activities in the population based
on the Twitter. Finally we conclude in Section 7 and
acknowledgements are provided in Section 8.
2 RELATED WORK
A number of studies have been conducted on different
forms of social networks like Del.icio.us, Facebook
and Wikipedia etc. Ginsberg et al. approach for es-
timating Flu trends suggests that relative frequency
of certain search terms are good indicators of per-
centage of physician visits in which a patient presents
influenza-like symptoms (Ginsberg et al., 2009). Cu-
lotta used a document classification component to fil-
ter misleading messages out of Twitter and showed
that a small number of flu-related keywords can fore-
cast future influenza rates (Culotta, 2010).
Twitter has been used for real-time notifica-
tions such as large-scale fire emergencies, earthquake
(Sakaki et al., 2010), downtime on services provided
by content providers (Motoyama et al., 2010) and
live traffic updates. There have been efforts in utiliz-
ing twitter data for measuring public interest/concern
about health-related events (Signorini et al., 2011),
predicting national mood, forecasting box-office rev-
enues for movies (Sitaram and Huberman, 2010), in-
formation diffusion in social media (Leskovec et al.,
2009), currency tracing, performing market and risk
analysis (Jansen et al., 2009) and analysing political
tweets to establish the correlations between buzz on
Twitter and election results (Nardelli, 2010) etc.
3 DATA COLLECTION
We describe our data collection methodology by in-
troducing SNEFT architecture, provide description of
our dataset, explore strategies for data cleaning, apply
filtering techniques in order to perform quantitative
HEALTHINF 2012 - International Conference on Health Informatics
62

Figure 1: The system architecture of
SNEFT
.
spatio-temporal analysis.
3.1 SNEFT Architecture
We propose Social Network Enabled Flu Trends
(
SNEFT
) architecture along with its crawler, predic-
tor and detector components, as our solution to pre-
dict flu activity ahead of time with certain accuracy.
CDC ILI reports and other influenza related data are
downloaded into “ILI Data” database from their cor-
responding websites (e.g., CDC (Centers for Disease
Control and Prevention, 2009)). A list of flu related
keywords (“Flu” , “H1N1” and “Swine Flu”) that are
likely to be of significance are used by OSN Crawler
as inputs into public search interfaces to retrieve pub-
licly available posts having mention of those key-
words. Relevant information about the posts are col-
lected along with the relative keyword frequency and
stored in a spatio-temporal “OSN Data” database for
further data analysis.
Autoregressive Moving Average (ARMA) model
is used to predict ILI incidence as a linear function of
current and past OSN data and past ILI data thus pro-
viding a valuable “preview” of ILI cases well ahead
of CDC reports. Novelty detection techniques can be
used to continuously monitor OSN data, and detect
transition in real time from a “normal” baseline situ-
ation to a pandemic using the volume and content of
OSN data enabling
SNEFT
to provide a timely warn-
ing to public health authorities for further investiga-
tion and response.
3.2 Twitter Crawler
In this section we briefly describe the methodology
for collecting our dataset. Based on the search API
provided by Twitter, we developcrawlers to fetch data
at regular time intervals.
The twitter search service accepts single or mul-
tiple keywords using conjunctions (“flu” OR “h1n1”
OR “#swineflu”) to search for relevant tweets. Search
results are typically 15 tweets (maximum 50) per
page up to 1,500 tweets arranged in chronologically
decreasing order, obtained from a real time stream
known as the public timeline. The tweet has the User
Name, the Post with status id and the Timestamp at-
tached with each post. From the twitter username, we
can get the number of followers, number of friends,
his/her profile creation date, location and status up-
date count for every user. The location field helps
us in tracking the current/default location of a user.
Geo location codes are present in a location enabled
mobile tweet. For all other purposes, we assume the
location attribute within the profile page to be his/her
current location and pass it as an input to Google’s lo-
cation based web services to fetch geo-location codes
(i.e., latitude and longitude) along with the country,
state, city with a certain accuracy scale. All the data
extracted from posts and profile page are stored in a
spatio-temporal “OSN data” Database.
We apply filters to get quantitative data within
Unites States and exclude organizations and users
who posts multiple times during the day on flu related
activities. This data is fed into the Analysis Engine
which has a detector and ARMA predictor model.
The visualization tools and reporting services gener-
ate timely visual and data centric reports on the ILI
situation. CDC monitors Influenza-like illness cases
within USA by collecting data about number of Hos-
pitalizations, percentages weighted ILI visits to physi-
cians etc and publishes it online. We download the
CDC data into “ILI data” database to compare our re-
sults.
4 DATA SET
In this section we briefly describe our datasets used
for influenza prediction. Since Oct 18, 2009, we have
searched and collected tweets and profile details of
Twitter users who mentioned about flu descriptors in
their tweets. The preliminary analysis for the year
2009-2010 is documented in (Achrekar et al., 2011).
For 2010-2011,so far we have4.5 million tweets from
1.9 million unique users. Twitter allows its users to
set their location details to public or private from the
profile page or mobile client. So far our analysis on
location details of Twitter dataset suggest that 22%
users on Twitter are within USA, 46% users are out-
side USA and 32% users have not published their lo-
cation details.
Initial stage analysis for the period 2009-2010, in-
dicated a strong correlation between CDC and Twit-
ter data on the flu incidences (Achrekar et al., 2011).
However results for the year 2010-2011 showed a sig-
nificant drop in the correlation coefficient from 0.98
to 0.47. In an attempt to investigate such a drastic
drop in correlation we looked at data samples and
found spurious messages which suppressed the actual
data. To list a few, tweets like “I got flu shot today.”,
TWITTER IMPROVES SEASONAL INFLUENZA PREDICTION
63
“#nowplaying Vado - Slime Flu..i got one recently!”
(slime flu is the name of a debut mixtape from an
artist V.A.D.O. released in 2010) are false alarms of
flu. In the year 2009-2010, swine flu event was so
evident that the noise did not significantly affect the
correlation that existed then. To mitigate this prob-
lem, we removed the spurious tweets using a filter-
ing technique that trains a document classifier to label
whether a message is indicative of flu event or not.
4.1 Text Classification
In an information retrieval scenario, text mining seeks
to extract useful information from unstructured tex-
tual data. Using simple “bag-of-words” text repre-
sentations technique based on vector space, our algo-
rithm classifies tweets wherein user mentions about
having acquired flu himself or having observered flu
among his friends, family, relatives, etc. Accuracy
of such a model is highly dependent on how well
trained our model is, in terms of precision, recall and
F-measure.
The set of possible labels for a given instance can
be divided into two subsets, one of which are consid-
ered “relevant”. To create such an annotated dataset
which demands human intelligence, we use Amazon
Mechanical Turks to manually classify a sample of
25,000 tweets. Every tweet is classified by exactly
three Turks and the majority classified result is at-
tached as the final class for that tweet.
The training dataset is fed as an input to different
classifiers namely decision tree (J48), Support Vec-
tor Machines (SVM) and Naive Bayesian. For ef-
ficient learning, some configurations that we did in-
corporate within our text classification algorithm in-
cludes setting term frequency and inverse document
frequency(tf-idf) weighting scheme, stemming, using
stopwords list, limiting number of words to keep (fea-
ture vector set) and reordering class. Based on the re-
sults shown in Table 1, we conclude that SVM classi-
fier with highest precision and recall rate outperforms
other classifiers when it comes to text classification
for our data set. Application of SVM on unclassified
data originating from within USA resulted in Twitter
dataset with 280K positively classified tweets from
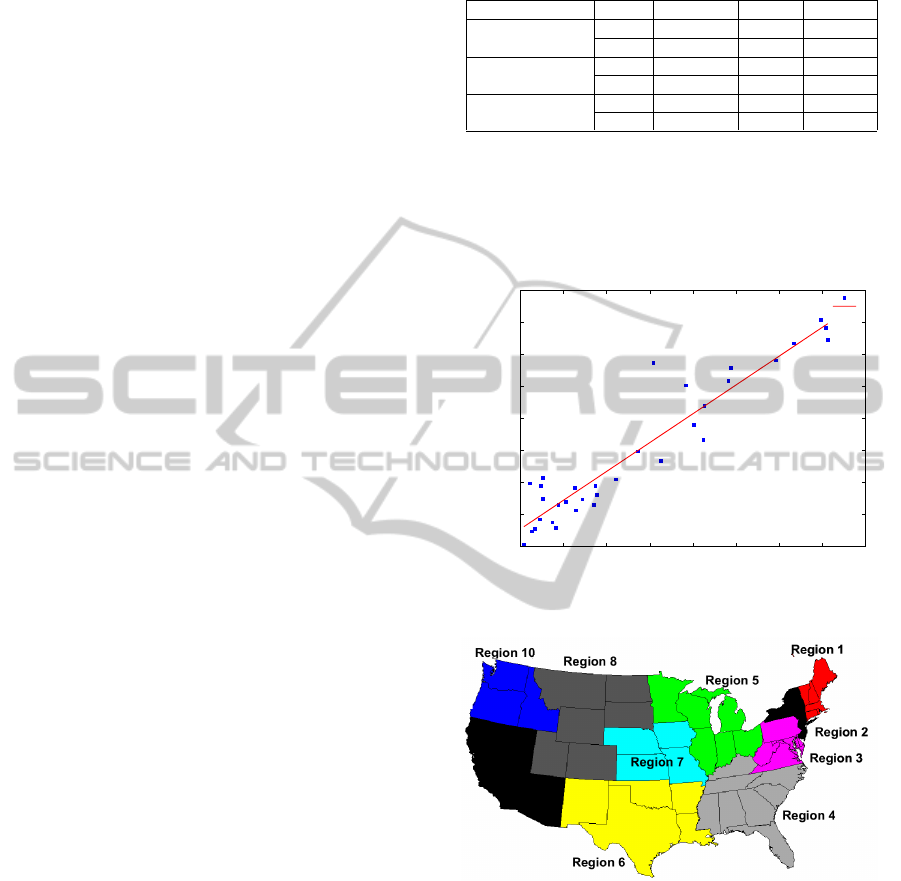
187K unique twitter users. In order to gauge if the
number of unique twitter users mentioning about flu
per week is a good measure of the CDC’s ILI re-
ported data, we plot (in Figure 2) the number of twit-
ter users/week against the percentage of weighted ILI
visits, which yields a high Pearson correlation coeffi-
cient of 0.8907.
Thus increase in the users tweeting about flu is ac-
companied by increase in percentage of weighted ILI
Table 1: Text Classification 10 fold cross validation results.
Classifier Class Precision Recall F-value
J48
Yes 0.801 0.791 0.796
No 0.813 0.704 0.755
Naive Bayesian
Yes 0.725 0.829 0.773
No 0.813 0.704 0.755
SVM
Yes 0.807 0.822 0.814
No 0.829 0.814 0.822
visits reported by CDC in the same week. However
the marked outlier present in Twitter data as identi-
fied in Figure 2 is coherent with Google Flu Trends
data when high tweet volume were witnessed in the
week starting January 2, 2011.
4000
5000
6000
7000
8000
9000
10000
11000
12000
1 1.5 2 2.5 3 3.5 4 4.5 5
Number of Twitter users posting per week
% ILI visit
Outlier
% ILI visit v/s Twitter users
Fitted line
Figure 2: Number of Twitter users per week versus percent-
age of weighted ILI visit by CDC.
Figure 3: Regionwise Division of USA into ten Regions.
CDC has divided USA into 10 regions as shown
in Figure 3. CDC publishes their weekly reports on
percentage weighted ILI visits collated from its ten
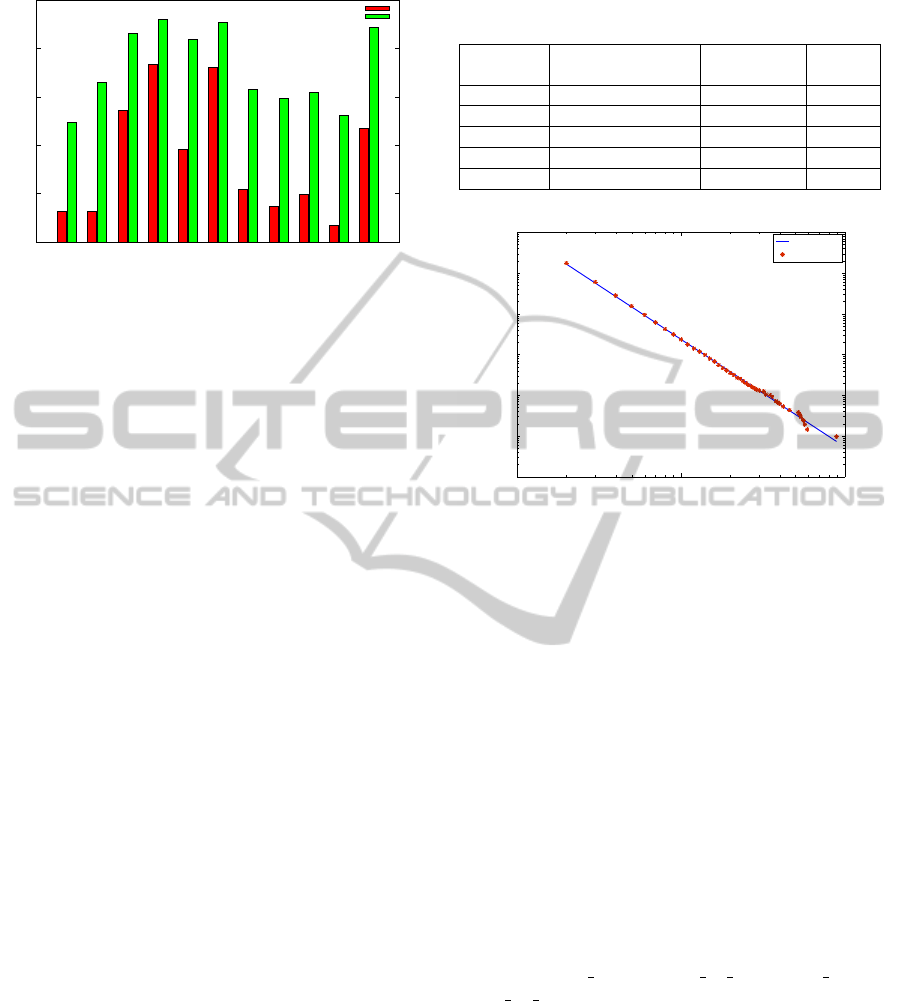
regions and aggregates for USA. Figure 4 compares
the Twitter dataset with CDC reports with and with-
out text classification for each of the ten regions de-
fined by CDC and USA as a whole. We observe
that the correlation coefficients have significantly im-
proved with text classification, across all the regions
and USA overall. Thus our text classification tech-
niques plays a vital role in improving the overall de-
tection and prediction performance.
HEALTHINF 2012 - International Conference on Health Informatics
64
0
0.2
0.4
0.6
0.8
1
Region 1
Region 2
Region 3
Region 4
Region 5
Region 6
Region 7
Region 8
Region 9
Region10
USA
Correlation Coefficient
CDC defined Regions and overall USA
Without Text Classification
With Text Classification
Figure 4: Classified Twitter dataset achieves higher correla-
tion with CDC reports on Nationwide and Regional levels.
4.2 Data Cleaning
The Twitter dataset required data cleaning to discount
retweets and successive posts from same users within
syndrome elapsed time.
• Retweets: A retweet is a post originally made by
one user that is forwarded by another user. For
flu tracking, a retweet does not indicate a new ILI
case, and thus should not be counted in the analy-
sis. Out of 4.5 million tweets we collected, there
are 541K retweets, accounting for 12% of the total
number of tweets.
• Syndrome elapsed time: An individual patient
may have multiple encounters associated with a
single episode of illness (e.g., initial consultation,
consultation 1–2 days later for laboratory results,
and follow-up consultation a few weeks later). To
avoid double counting from common pattern of
ambulatory care, the first encounter for each pa-
tient within any single syndrome group is reported
to CDC, but subsequent encounters with the same
syndrome are not reported as new episodes until
more than six weeks have elapsed since the most
recent encounter in the same syndrome (Lazarus
et al., 2002). We call this Syndrome Elapse time.
Hence, we created different datasets namely: Twit-
ter dataset with No Retweets (Tweets starting with
RT) and Twitter dataset without Retweets and with
no tweets from same user within certain syndrome
elapsed time.
When we compared different datasets mentioned
in Table 2 with CDC data, we found that Twitter
dataset without Retweets showed a high correlation
(0.8907) with CDC Data. As opposed to a common
practice in public health safety, where medical exam-
iners within U.S. observe a syndrome elapse time pe-
riod of six weeks, user behaviour on Twitter follows a
Table 2: Correlation between Twitter Dataset and CDC
along with its Root Mean Square Errors(RMSE).
Retweets Syndrome Elapse Correlation RMSE
Time coefficient errors
No 0 week 0.8907 0.3796
No 1 week 0.8895 0.3818
No 2 week 0.8886 0.3834
No 3 week 0.886 0.3878
No 4 week 0.8814 0.3955
10
0
10
1
10
2
10
−6
10
−5
10
−4
10
−3
10
−2
10
−1
10
0
Number of Tweets x
Pr(X>=x)
Fitted Line
CCDF
Figure 5: Complementary Cumulative Distribution function
(CCDF) of the number of tweets by same users.
trend wherein we do not ignore successive posts from
same user. Thus Twitter dataset without Retweets is
our choice of dataset for all subsequent experiments.
From Figure 5, we observe that Complemen-
tary Cumulative Distribution function (CCDF) of the
number of tweets posted by same individual can be
fitted by a power law function of exponent -2.6429
and coefficient of determination (R-square) 0.9978
with a RMSE of 0.1076 using Maximum likelihood
estimation. Most people tweet very few times (e.g.,
82.5% of people only tweet once and only 6% of peo-
ple tweet more than two times).
Most of these high-volume tweets are created
by health related organization, who tweet multi-
ple time during a day and users who subscribe
to flu related RSS feeds published by these orga-
nizations. “Flu alert”,“swine flu pro”, “live h1n1”,
“How To Tips”, “MedicalNews4U” are examples of
such agencies on Twitter.
5 PREDICTION MODEL
The correlation between Twitter activity and CDC re-
ports can change due to a number of factors. Annual
or seasonal changes in flu-related trends, for instance
vaccination rates that are affected by health cares, re-
sult in the need to constantly update parameters relat-
TWITTER IMPROVES SEASONAL INFLUENZA PREDICTION
65

ing Twitter activity and flu activity. However, partic-
ularly at the beginning of the influenza season, when
prediction is of most significance, enough data may
not be available to accurately perform these updates.
Additionally predicting changes in ILI rates simply
due to changes in flu-related Twitter activity can be
risky due to transient changes, such as changes in
Twitter activity due to flu-related news.
In order to establish baseline for the ILI activity
and to smooth out any undesired transients, we pro-
pose the use of Logistic Autoregression with exoge-
nous inputs (ARX). Effectively, we attempt to predict
a CDC ILI statistic during a certain week by using
Twitter activity and CDC data from previous weeks.
The prediction of current ILI activity using ILI ac-
tivity from previous weeks forms the autoregressive
portion of the model, while the Twitter data from pre-
vious weeks serve as exogenousinputs. By CDC data,
we refer to the percentage of visits to a physician for
ILI (also called as ILI rate).
5.1 Influenza Model Structure
Although the percentage of physician visits is be-
tween 0% and 100%, the number of Twitter users is
bounded below by 0. Simple Linear ARX neglects
this fact in the model structure. Therefore, we intro-
duce a logit link function for CDC data and a loga-
rithmic transformation of the Twitter data as follows:
Logistic ARX Model.
log
y(t)
1− y(t)
=
m
∑
i=1
a
i
log
y(t −i)
1− y(t − i)
+
n−1
∑
j=0
b
j
log(u(t − j)) + c+ e(t)
(1)
where t indexes weeks, y(t) denotes the percentage of
physician visits due to ILI in week t, u(t) represents
the number of unique Twitter users with flu related
tweets in week t, and e(t) is a sequence of indepen-
dent random variables. c is a constant term to account
for offset. In our tests, the number of unique Twitter
users u(t) is defined as Twitter users without retweets
and having no tweets from the same user within syn-
drome elapsed time of 0 week. The flu related tweets
are defined as tweets with keywords “flu”, “H1N1”
and “swine flu”. The rationale for the model struc-
ture in Eq. (1) is that Twitter data provides real-time
assessment of flu epidemic. However, the Twitter
data may be disturbed at times by events related to
flu, such as news reports of flu in other parts of the
world, but not necessarily to local people actually get-
ting sick due to ILI. On the other hand, the CDC data
provides a true, albeit delayed, assessment of a flu epi-
demic. Hence, by using the CDC data along with the
Twitter data, we may be able to take advantage of the
timeliness of the Twitter data while overcoming the
disturbance that may be present in the Twitter data.
The objective of the model is to provide timely
updates of the percentage of physician visits. To pre-
dict such percentage in week t, we assume that only
the CDC data with at least 2 weeks of lag is avail-
able for the prediction, if past CDC data is present in
a model. The 2-week lag is to simulate the typical de-
lay in CDC data reporting and aggregation. For the
Twitter data, we assume that the most recent data is
always available, if a model includes the Twitter data
terms. In other words, the most current CDC or Twit-
ter data that can be used to predict the percentage of
physician visits in week t is week t-2 for the CDC data
and week t for the Twitter data.
In order to predict ILI rates in a particular week
given current Twitter data and the most recent ILI data
from the CDC we must estimates the coefficients, a
i
,
b
j
and c in Eq. (1). Also, in practice, the model orders
m and n are unknown and must be estimated. In our
experiment, we vary m from 0 to 2 and n from 0 to 3
in Eq. (1) in order to obtain the best values of m and
n to use for prediction. Intuitively, this answers the
question of how many weeks of Twitter and ILI data
should be used to predict the ILI activity in the cur-
rent week. Within the ranges examined, m = 0 or n =
0 represent models where there are no CDC data, y, or
Twitter data, u, terms present. Also, if m = 0 and n = 1,
we have a linear regression between Twitter data and
CDC data. If n = 0, we have standard auto-regressive
(AR) models. Since the AR models utilize past CDC
data, they serve as baselines to validate whether Twit-
ter data provides additional predictive power beyond
historical CDC data.
Prediction with Logistic ARX Model. To predict
the flu cases in week t using the Logistic ARX model
in Eq. (1) based on the CDC data with 2 weeks of
delay and/or the up-to-date Twitter data, we apply the
following relationship:
log
ˆy(t)
1− ˆy(t)
= a
i
log
ˆy(t − 1)
1− ˆy(t − 1)
+
m
∑
i=2
a
i
log
y(t −i)
1− y(t − i)
+
n−1
∑
j=0
b
j
log(u(t − j)) (2)
log
ˆy(t − 1)
1− ˆy(t − 1)
=
m
∑
i=1
a
i
log
y(t −i− 1)
1− y(t − i− 1)
+
n−1
∑
j=0
b
j
log(u(t − j− 1)) (3)
where ˆy(t) represents predicted CDC data in week t.
HEALTHINF 2012 - International Conference on Health Informatics
66
It can be verified from the above equations that to pre-
dict the CDC data in week t, the most recent CDC
data is from week t − 2. If the CDC data lag is more
or less than two weeks, the above equations can be
easily adjusted accordingly.
5.2 Cross Validation Test Description
Based on ARX model structure in Eq. (1), we con-
ducted tests using different combinations of m and
n values. We currently have 33 weeks with both
Twitter activity and CDC data available (10/3/2010–
05/15/2011). Due to limited data samples, we adopted
the K-fold cross validation approach to test the predic-
tion performance of the models.
In a typical K-fold cross validation scheme, the
dataset is divided into K (approximately) equally
sized subsets. At each step in the scheme, one such
subset is used as the test set while all other subsets
are used as training samples in order to estimate the
model coefficients. Therefore, in a simple case of a
30-sample dataset, 10-fold cross-validation would in-
volve testing 3-samples in each step, while using the
other 27 samples to estimate the model parameters.
In our case, the cross-validation scheme is some-
what complicated by the dependency of the sample
y(t) on the previous samples, y(t − 1), . . . , y(t − m)
and u(t), . . . , u(t− n+ 1) (see Eq. (1) ). Therefore, the
first sample that can be predicted is y(max(m+ 1, n))
not y(1). In fact, since we are predicting “two weeks
ahead” of the available CDC data, the first sample
that can be estimated is actually y(max(m + 2, n +
1)). Since, prediction equations cannot be formed
for y(1), . . . , y(max(m+ 2, n+ 1) − 1), those samples
were not considered in any of the K subsets during
our experiment to be evaluated for prediction perfor-
mance. However, they were still used in the training
set to estimate the values of the coefficients a
i
and b
j
in Eq. (1).
Considering the above constraints, our K-fold val-
idation testing procedure is as follows:
1. For each (m, n) pair from m = 0, 1, 2 and n =
0, 1, 2, 3, repeat the following:
(a) Identify F, the index of first data sample that
can actually be predicted. F = max(m+ 1, n)
(b) Represent the available data indices as t =
1, . . . , T. Then divide the dataset into K approx-
imately equally sized subsets {S
1
, S
2
, . . . , S
K
},
with each subset comprising members that have
an approximately equal time interval between
them. For example, the first set would be S
1
=
{y(F), y(F + K), y(F + 2K), . . . }, the second
would be S
2
= {y(F + 1), y(F + K + 1), y(F +
2K + 1), . . .} and so on.
Table 3: Root mean squared errors from 10-fold cross vali-
dation. m and n are defined in Eq. (1). The m and n values
in the table specify the model that results in the RMSE in
the corresponding row and column respectively. The lowest
RMSE in the table is highlighed.
n = 0 n = 1 n = 2 n = 3
m = 0 0.5355 0.4814 0.4813
m = 1 0.6331 0.4107 0.4147 0.4314
m = 2 0.5395 0.3957 0.3986 0.4256
(c) For each S
k
, k = 1, . . . , K, obtain the values
of the model parameters a
i
and b
j
using all
the other subsets with the least squares estima-
tion technique. Based on the estimated model
parameter values and the associated prediction
equations in Eq. (2), predict the value of each
member of S
k
.
2. For each (m, n) pair, we have obtained a pre-
diction of the CDC time-series, y(t) for t =
F
mn
, . . . , T. Note that F still represents the first
time index that can be predicted. However, we
use the subscript mn to emphasize the fact that F
varies depending on the values of m and n. By
comparing the prediction with the true CDC data,
we calculate the root mean-squared error (RMSE)
as follows:
ε =
s
1
T − F
max
+ 1
∑
t
(y(t) − ˆy(t))
2
(4)
The RMSE is computed over t = F
max
, . . . , T, re-
gardless of techniques and model orders to ensure
fairness in comparison.
5.3 Cross Validation Results
According to the 10-fold cross validation results in
Table 3, the model corresponding to m = 2 and n =
1 has the lowest RMSE. This indicates that current
Twitter data and two most recent ILI data points are
most useful in accurate prediction of influenza rates.
In general, the addition of Twitter data improves the
prediction with past CDC data alone. For the 10-fold
cross validation results presented in Table 3, for ex-
ample, the AR model (m = 1, n = 0) comprising of
the y(t − 2) term and the constant term for the pre-
diction of y(t) has a RMSE of 0.6331. For the same
m = 1, the model with additional Twitter data u(t)
(i.e. n = 1) has a lower RMSE of 0.4107. We also
observe that using Twitter data (m = 0) alone is in-
sufficient for prediction and that the past ILI rates are
critical in predicting future values, as is evident from
our results. The addition of Twitter data improves the
prediction with past CDC data alone. Therefore, the
TWITTER IMPROVES SEASONAL INFLUENZA PREDICTION
67
Twitter data provides a real-time assessment of the flu
epidemic (i.e. the availability of Twitter data in week
t in the prediction of physician visits also in week t
as shown in Eq. (2)), while the past CDC data pro-
vides the recent ILI rates in the prediction model. As
shown earlier in the paper, there is strong correlation
between the Twitter data and the CDC data. Hence,
the more timely Twitter data can compensate for the
lack of current CDC data and help capture the cur-
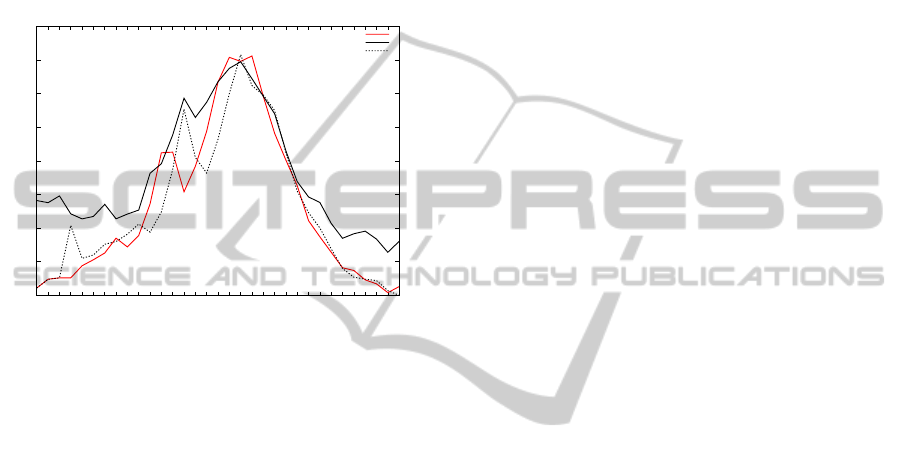
rent flu trend. Finally in Figure 6, we provide a sin-
1
1.5
2
2.5
3
3.5
4
4.5
5
w40
w41
w42
w43
w44
w45
w46
w47
w48
w49
w50
w51
w52
w1
w2
w3
w4
w5
w6
w7
w8
w9
w10
w11
w12
w13
w14
w15
w16
w17
w18
w19
w20
percentage of ILI visits
% physician visits (CDC)
Twitter Data
predicted % physician visits
Figure 6: Weekly plot of percentage weighted ILI visits,
positively classified Twitter dataset and predicted ILI rate
using CDC and Twitter
gle plot for percentage weighted ILI visits, positively
classified Twitter users and predicted ILI rate using
CDC and Twitter for the year 2010-2011. Note that
the original Twitter data alone would predict higher
ILI rates for the begining and ending parts of the flu
season. Using previous ILI data from CDC offers a
better assessment for making flu predictions.
6 FLU PREDICTION WITHIN
REGIONS AND AGE GROUPS
In this section we discuss the use of Twitter for flu pre-
dictions in specific population groups. Given the data
available, we are able to study the prediction perfor-
mance in specific regions of the United States. Also,
with ILI rates provided in different age groups we are
able to study the effectiveness of using Twitter data to
predict flu trends in these age groups. The advantages
of studying performance in subgroups are twofold:
• The differences in Twitter usage among differ-
ent population groups and similar differences in
response amongst people in different population
groups to ILI-like symptoms can result in very
different model parameters and prediction per-
formance when attempting to predict flu activity
among different sections of the population. It is
therefore important to adapt the prediction mod-
els for different population groups.
• In our previous study, it has been shown that there
exists significant correlation between Twitter re-
ports and the percentage of ILI cases reported by
CDC. However, much of our analysis is based on
a limited number of data points (31 overlapping
weeks for Twitter and CDC reports for the year
2009-2010 and 33 overlapping weeks for Twitter
and CDC reports for the year 2010-2011) avail-
able during our period of performance evaluation,
with Twitter and ILI data aggregated across the
entire United States. In the year 2009-2010, only
11 out of 31 data points occurred during the weeks
where the ILI rates were significant (>2%) and
during this interval, the ILI rates and Twitter re-
ports were steadily decreasing. During the period
2010-2011, 15 out of 33 data points occurred dur-
ing the weeks where the ILI rates were significant
(>2%) and during this interval, the ILI rates and
Twitter reports were simultaneously increasing till
they reached their peak in mid February 2011 and
then onwards they both started decreasing.
Due to this limited time frame any claim of high cor-
relation between the two data streams (ILI rates and
Twitter reports) may be viewed with skepticism. This
evaluation was performed as an experiment to see
which age groups the Twitter data fit best. The results
are interesting but not conclusive.
6.1 Regional Twitter and ILI Rates
We analyzed the relationship between the Twitter ac-
tivity and ILI rates across all geographic regions de-
fined by the Health and Human Services (HHS) re-
gions. For reference, the regions are shown on the
USA map in Figure 3.
In studying the regional statistics, we would like
to make some comparisons across regions. For in-
stance (i) when the ILI rate peaks later in a particular
region than the rest of country, do the Twitter reports
also peak later, (ii) is there in relationship between the
decay in ILI rates and the decay in Twitter reports.
Figure 7 shows, for both ILI and Twitter data, the
relative intensity across the ten Health and Human
Services (HHS) regions (columns) during successive
weeks (rows) in the year 2009-2010. The colormap
used is a scale with white representing low intensity
and black, high intensity. We are comparing ”trends”
among the ILI and Twitter data.
Regional analysis shows that ILI seems to peak
later in the Northeast (Regions 1 and 2) than in the rest
of the country by at least week. The Twitter reports
HEALTHINF 2012 - International Conference on Health Informatics
68
HHS Region
Week number
1 2 3 4 5 6 7 8 9 10
5
10
15
20
25
HHS Region
Week number
1 2 3 4 5 6 7 8 9 10
5
10
15
20
25
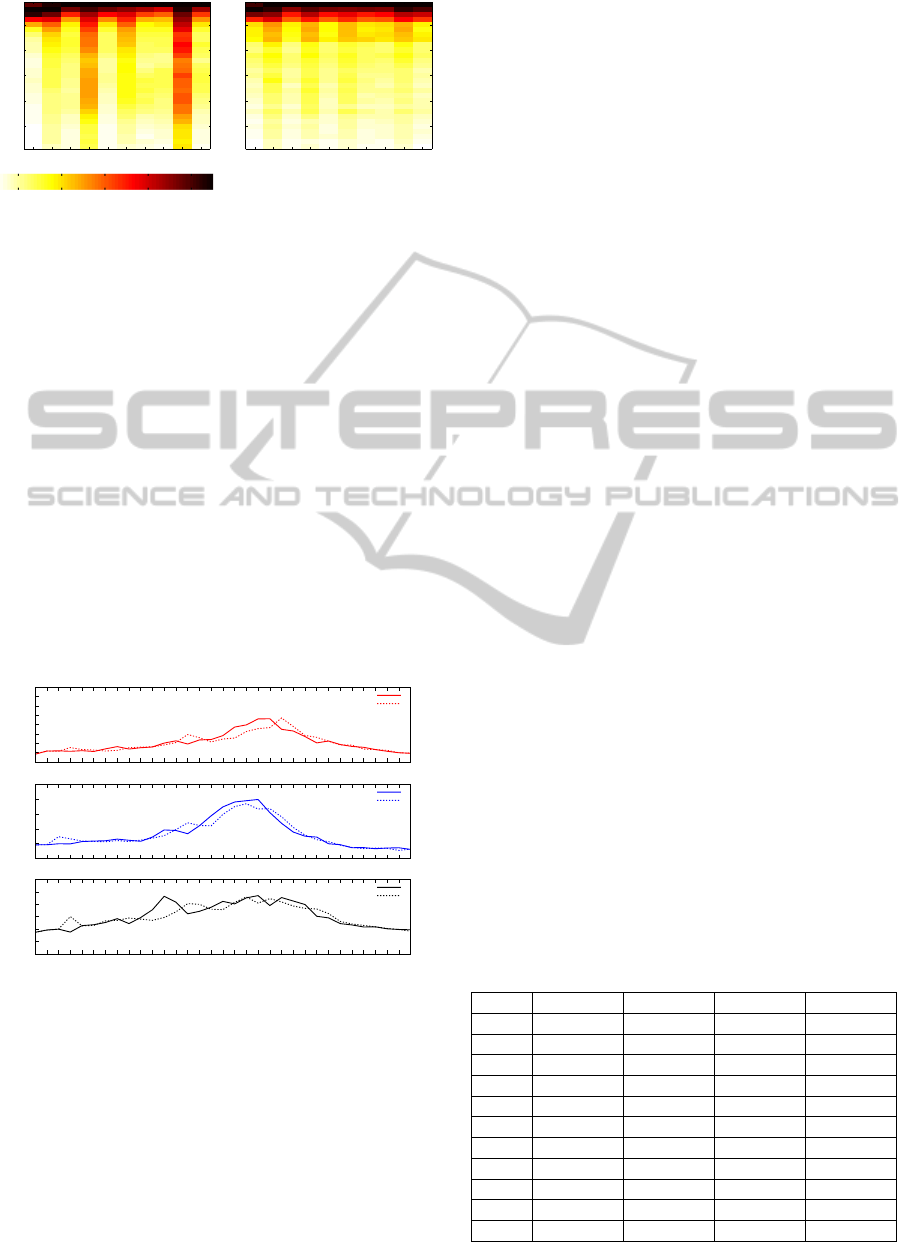
Figure 7: Heatmap of CDC’s Regionwise ILI data (left) and
Twitter data (right). Colormap scale included (below).
also follow this trend. In Region 9, Region 4 and the
Northeast, the ILI rates seem to drop off fairly slowly
in the weeks immediately following the peaks. This
is also reflected in the Twitter reports. Approximately
20-25 weeks after the peak ILI, the northern regions
have lower levels relative to the peaks in the southern
regions. This is also true of the Twitter reports. The
decline in ILI rates is slowest in Region 9.
Figure 8 depicts regionwise ILI prediction perfor-
mance for the year 2010-2011 using our logit model.
We arbitrarily select region 1, region 6 and region 9 to
represent the regions, one each from the East, South
and Western U.S. and plot the true and predicted ILI
values for each of these regions. We observe that
the Twitter reports and ILI rates are in fact correlated
across regions and therefore corroborate our earlier
findings that Twitter can improve ILI rate prediction.
0
0.5
1
1.5
2
2.5
3
3.5
4
w40
w41
w42
w43
w44
w45
w46
w47
w48
w49
w50
w51
w52
w1
w2
w3
w4
w5
w6
w7
w8
w9
w10
w11
w12
w13
w14
w15
w16
w17
w18
w19
w20
Region 1
actual % ILI rate
predicted % ILI rate
0
2
4
6
8
10
w40
w41
w42
w43
w44
w45
w46
w47
w48
w49
w50
w51
w52
w1
w2
w3
w4
w5
w6
w7
w8
w9
w10
w11
w12
w13
w14
w15
w16
w17
w18
w19
w20
% ILI visit
Region 6
actual % ILI rate
predicted % ILI rate
0
1
2
3
4
5
6
w40
w41
w42
w43
w44
w45
w46
w47
w48
w49
w50
w51
w52
w1
w2
w3
w4
w5
w6
w7
w8
w9
w10
w11
w12
w13
w14
w15
w16
w17
w18
w19
w20
Region 9
actual % ILI rate
predicted % ILI rate
Figure 8: Comparision between Actual and Predicted re-
gional data for Region 1, Region 6 and Region 9.
6.2 Age-based Influenza Analysis
The differences in Twitter usage and susceptibility to
flu among different demographics can result in very
different prediction model parameters and perfor-
mance when attempting to predict flu activity among
different sections of the population. While any num-
ber of population groups may be defined, the CDC
provides the number of ILI cases by age groups, from
which we can compute the unweighted ILI rates. This
then provides an opportunity to examine the predic-
tion performance amongst different age groups when
predicting ILI using Twitter data. Note that while ILI
rates broken down by age group are available, we do
not have Twitter activity broken down by age group.
Also, it is debatable whether attempting to correlate
Twitter and ILI activity within age groups is of any
value; a significant percentage of Twitter activity may
result from family members or friends of the affected
persons. Therefore, we attempt to study the relation-
ship between aggregate Twitter activity over all age
groups with ILI rates in different age groups.
Table 4 shows the Root Relative Squared Error
(RRSE) performance in different age groups for dif-
ferent geographical regions within USA. The RRSE
normalizes the errors to the magnitude of the ground
truth data (in this case the total number of ILI cases
relative to total patients seen by provider) in each age
group. We have highlighted the age groups with the
best match between ILI rates and Twitter data within
each region. In parenthesis, alongside the RRSE val-
ues are the model orders for the autoregressive and x-
components of the general model, (m-n). The ”best”
age-group for prediction in each region is highlighted.
The results indicates that for most of the regions,
Twitter data best fits the age-groups of 5-24 yrs and
25-49 yrs, which correlates well with the fact that
this likely is the most active age groups using Twit-
ter (Twitter, 2011). For Region 6 and 7, the Twitter
activity best fits ILI activity amongst the 0-4 yrs age
group. This is an interesting result which we currently
have no specific insight into. It should be noted that
for Region 6 and 7, the difference between the fits for
0-4 years and 25-49 years is marginal.
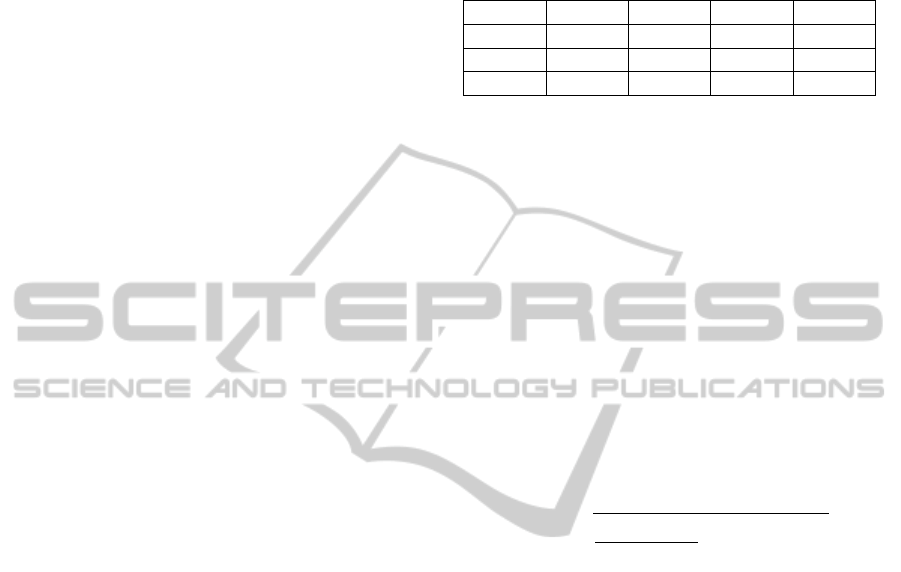
Table 4: Prediction performance (root relative squared er-
ror) using Twitter in different age groups for different geo-
graphical regions within the US. In parenthesis, alongside
the RRSE values are the model orders, (m-n), for the au-
toregressive and x-components of the general model in Eq.
(1) which yield the best performance.
0− 4yrs 5− 24yrs 25− 49yrs 50+ yrs
US 0.5285(0-2) 0.4261(2-2) 0.3577(1-2) 0.4320(1-1)
Reg1 0.5728(2-1) 0.6000(2-2) 0.5499(1-1) 0.7763(1-1)
Reg2 0.6954(0-3) 0.6005(2-1) 0.4965(0-3) 0.5171(1-3)
Reg3 0.4423(0-2) 0.3268(2-2) 0.3066(2-3) 0.3515(1-2)
Reg4 0.5281(0-3) 0.3719(0-1) 0.4792(0-1) 0.5192(0-1)
Reg5 0.6387(1-1) 0.4337(2-3) 0.4300(0-3) 0.5198(1-1)
Reg6 0.3032(0-2) 0.3407(1-2) 0.3564(0-3) 0.4469(0-3)
Reg7 0.5426(2-3) 0.5571(1-3) 0.5492(1-3) 0.6454(2-2)
Reg8 0.6511(1-1) 0.6133(1-2) 0.6649(2-2) 0.6445(2-3)
Reg9 0.7453(2-1) 0.4229(2-1) 0.4690(1-1) 0.6176(2-1)
Reg10 0.8548(2-1) 0.5746(2-1) 0.6462(2-2) 0.7347(2-1)
TWITTER IMPROVES SEASONAL INFLUENZA PREDICTION
69

The above results show that flu-related Twitter ac-
tivity is more correlated with flu activity with certain
age-groups within the USA population and the cor-
relation may be better in certain regions compared
to others. This does indicate that training prediction
models that are targeted to specific population seg-
ments is a worthwhile endeavor in a future effort.
7 CONCLUSIONS
In this paper, we have described our approach to
achieve faster, near real time detection and prediction
of the emergence and spread of influenza epidemic,
through continuoustracking of flu related tweets orig-
inating within United States. We showed that apply-
ing text classification on the flu related tweets signif-
icantly enhances the correlation (Pearson correlation
coefficient 0.8907) between the Twitter data and the
ILI rates from CDC.
For prediction, we build an auto-regression with
exogenous input (ARX) model where ILI rate of pre-
vious weeks from CDC formed the autoregressive
portion of the model, and the Twitter data served as
an exogenous input. Our results indicated that while
previous ILI rates from CDC offered a realistic (but
delayed) measure of a flu epidemic, Twitter data pro-
vided a real-time assessment of the current epidemic
condition and can be used to compensate for the lack
of current ILI data.
We observed that the Twitter data was highly cor-
related with the ILI rates across different HHS re-
gions. Our age-based prediction analysis suggested
that for most of the regions, Twitter data best fit the
age groups of 5-24 years and 25-49 years, correlating
well with the fact that these were likely the most ac-
tive age group communities on Twitter. Therefore, flu
trends tracking using Twitter significantly enhances
public health preparedness against influenza epidemic
and other large scale pandemics.
ACKNOWLEDGEMENTS
This research is supported in parts by the National
Institutes of Health under grant 1R43LM010766-01
and National Science Foundation under grant CNS-
0953620.
REFERENCES
Achrekar, H., Gandhe, A., Lazarus, R., Yu, S.-H., and Liu,
B. (2011). Predicting flu trends using twitter data.
IEEE Infocom, 2011 workshop on on Cyber-Physical
Networking Systems (CPNS) 2011.
Centers for Disease Control and Prevention (2009). Flu-
View, a weekly influenza surveillance report.
Culotta, A. (2010). Detecting influenza outbreaks by ana-
lyzing twitter messages. Knowledge Discovery and
Data Mining Workshop on Social Media Analytics,
2010.
Espino, J., Hogan, W., and Wagner, M. (2003). Tele-
phone triage: A timely data source for surveillance of
influenza-like diseases. In AMIA: Annual Symposium
Proceedings.
Ferguson, N. M., Cummings, D. A., Cauchemez, S., Fraser,
C., Riley, S., Meeyai, A., Iamsirithaworn, S., and
Burke, D. S. (2005). Strategies for containing an
emerging influenza pandemic in southeast asia. Na-
ture, 437:209–214.
Ginsberg, J., Mohebbi, M. H., Patel, R. S., Brammer, L.,
Smolinski, M. S., and Brilliant, L. (2009). Detecting
influenza epidemics using search engine query data.
Nature, 457:1012–1014.
Jansen, B., Zhang, M., Sobel, K., and Chowdury, A. (2009).
Twitter power:tweets as electronic word of mouth.
Journal of the American Society for Information Sci-
ence and Technology, 60(1532):2169–2188.
Jordans, F. (2009). WHO working on formulas to model
swine flu spread.
Lazarus, R., Kleinman, K., Dashevsky, I., Adams, C.,
Kludt, P., DeMaria, A., Jr., R., and Platt (2002). Use
of automated ambulatory-care encounter records for
detection of acute illness clusters, including potential
bioterrorism events.
Leskovec, J., Backstrom, L., and Kleinberg, J. (2009).
Meme-tracking and the dynamics of the news cy-
cle. International Conference on Knowledge Discov-
ery and Data Mining, Paris, France, 495(978).
Longini, I., Nizam, A., Xu, S., Ungchusak, K., Han-
shaoworakul, W., Cummings, D., and Halloran, M.
(2005). Containing pandemic influenza at the source.
Science, 309(5737):1083–1087.
Magruder, S. (2003). Evaluation of over-the-counter phar-
maceutical sales as a possible early warning indicator
of human disease. In Johns Hopkins University APL
Technical Digest.
Motoyama, M., Meeder, B., Levchenko, K., Voelker, G. M.,
and Savage, S. (2010). Measuring online service avail-
ability using twitter. Workshop on online social net-
works, Boston, Massachusetts, USA.
Nardelli, A. (2010). Tweetminister.
Sakaki, T., Okazaki, M., and Matsuo, Y. (2010). Earth-
quake shakes twitter users: real-time event detection
by social sensors. In 19th international conference on
World wide web, Raleigh, North Carolina, USA.
Signorini, A., Segre, A. M., and Polgreen, P. M. (2011).
The use of twitter to track levels of disease activity
and public concern in the u.s. during the influenza a
h1n1 pandemic. PLoS ONE, Volume 6 — Issue 5.
Sitaram, A. and Huberman, B. A. (2010). Predicting the
future with social media. In Social Computing Lab,
HP Labs, Palo Alto, California, USA.
Twitter (2011). Information on twitter users age-wise.
HEALTHINF 2012 - International Conference on Health Informatics
70
