
BRAKE RESPONSE TIME BEFORE
AND AFTER TOTAL KNEE ARTHROPLASTY
Tracking Possible Effects of the Surgery Technique on Motor Performance:
Report of Two Cases
Carlos J. Marques
1,2
, Rui Santos
4
, Hugo Gamboa
4
, Frank Lampe
3
, João Barreiros
1
and Jan Cabri
5
1
Faculty of Human Kinetics, Technical Universitty of Lisbon, Lisbon, Portugal
2
Physikal Therapy and Rehabilitation Department, ENDO-Klinik Hamburg, Hamburg, Germany
3
Joint Replacement Center, Schön Klinik Hamburg Eilbek, Hamburg, Germany
4
Physics Department of the Sciences and Technology Faculty, New University of Lisbon, Lisbon, Portugal
5
Department of Physical Performance at the Norwegian School of Sport Sciences, Oslo, Norway
Keywords: Total Knee Replacement, Minimally Invasive Surgery, Brake Response Time, Reaction Time, Automobile
Driving.
Abstract: After total knee arthroplasty (TKA) patients often ask when they can resume car driving. This question was
the aim of some studies in the past, however no study was found on the possible effects of different surgery
techniques on brake response time (BRT). A randomized controlled trial on the effects of two surgery
techniques (minimally invasive vs. standard approach) on BRT was designed. In this paper the motor
performance of two female patients was compared. Surgery had different effects on the mean BRT of both
Patients. The mean BRT of the MIS Patient wasn’t increased 7 days after surgery, while the BRT of the
Patient undergoing standard surgery was increased by 46.8% at the same time.
1 INTRODUCTION
Patients undergoing total knee arthroplasty (TKA)
frequently ask when they can resume car driving.
Six studies on this topic were published in the past
years (Dalury et al., 2010, Liebensteiner et al., 2010,
Marques et al., 2008a, Marques et al., 2008b,
Pierson et al., 2003, Spalding et al., 1994). All
studies investigated the effects of TKA on brake
response time (BRT), an important human factor
used in accident prevention research.
The results document a BRT increase after right
TKA. The time frame needed for the BRT to return
to preoperative values varied and ranged from 8
(Pierson et al., 2003) to 4 weeks (Dalury et al.,
2010). In the study by Dalury and colleagues (2010),
where the patients were submitted to “contemporary
TKA with less tissue disruption”, the BRT of all
patients returned to preoperative values 4 weeks
after surgery. A small group of patients reached the
preoperative values already 2 weeks after surgery.
The BRT can be fractionated in reaction time
(RT) and movement time (MT). The RT, also called
neurological time, is the time required for stimulus
perception, response selection and response
initiation. The MT can be subdivided in foot transfer
time (FTT) and brake pedal travelling time (BPTT).
In the studies where the components of the BRT
(RT and MT) were investigated (Spalding et al.,
1994, Marques et al., 2008b, Marques et al., 2008a,
Dalury et al., 2010) it was observed that ten days
after TKA the central components of the task were
not affected once RT was not changed.
Total knee arthroplasty seems to affect peripheral
aspects related with the execution of the movement
and the soft tissue lesion may be the cause of such
performance impairments.
Minimal invasive surgery (MIS) techniques for
TKA have been used for several years as an
alternative to standard approaches. Supporters of
MIS techniques go from the assumption that a
smaller soft tissue injury with a reduction of the
muscle quadriceps lesion leads to a faster
419
J. Marques C., Santos R., Gamboa H., Lampe F., Barreiros J. and Cabri J..
BRAKE RESPONSE TIME BEFORE AND AFTER TOTAL KNEE ARTHROPLASTY - Tracking Possible Effects of the Surgery Technique on Motor
Performance: Report of Two Cases.
DOI: 10.5220/0003790904190422
In Proceedings of the International Conference on Bio-inspired Systems and Signal Processing (BIOSIGNALS-2012), pages 419-422
ISBN: 978-989-8425-89-8
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

rehabilitation with better early functional outcomes,
less pain and shorter stay duration. To the best of our
knowledge we don’t know of any available data on
the effects of different surgery techniques on motor
performance while executing an emergency brake in
a car simulator. The purpose of this study is to
compare the effects of MIS and Standard approach
for TKA on BRT components. Once the study is
ongoing the data of two cases will be reported.
2 METHODS AND MATERIALS
2.1 Design
A randomized controlled trial with one between-
subject factor (surgery technique: MIS or Standard)
and one within-subject factor (time: one day before
and 7 days, 30 and 40 days after surgery) was
designed (Marques et al., 2011). After consent to
participate the patients were randomly assigned to
MIS or standard approach surgery. The patients
were blinded to the surgery technique they
underwent and they all received the same standard
physiotherapy treatments.
One experienced orthopaedic surgeon performed
all surgeries. In the operation room a concealed
envelope was opened and the surgeon got to know
which technique he would have to perform.
The MIS technique used was the mini-midvastus
approach (Haas et al., 2006). The peri-patellar
approach with inversion of the patella was standard.
Independently from the surgery technique all
operations were performed with the use of the
OrthoPilot navigation system and all patients got a
Columbus total knee endoprosthesis (BBraun
Aesculap, Germany).
The study protocol was approved by the Ethics-
Committee of the Federal State of Hamburg,
Germany (Project Nr.: PV3349). The trial
registration number at the German Clinical Trial
Database (DRKS) is: DRKS00000552.
2.2 Participants
The patient selection is taking place at the Schön
Klinik Hamburg Eilbek in Hamburg, Germany. The
patients addressed the clinic for elective primary
right TKA and were asked if they were car drivers.
If the patient drove regularly (at least once a week)
he/she was informed about the study and asked for
consent.
The patient selection started on January 10
th
2011 and is still ongoing. Eleven patients have
signed the informed consent until now, of which the
complete data of 8 Patients is available: MIS n=5 (4
male; 1 female); Standard approach n=3 (1 male; 2
female). Because the number of cases is still small
and the distribution of male and female patients in
the groups is unlike, we will present only the
primary outcome results of two female patients (Pat.
A and Pat. B).
2.3 Instruments/ Equipment
The patients performed the emergency brakes in a
car simulator (Fig.1) which was built based on a
European middle class car an already used in two
former studies (Marques et al., 2008a, Marques et
al., 2008b).
Figure 1: Car simulator with bioPlux Research system.
The data acquisition system consists of a bioPlux
Research system with wireless connectivity via
Bluetooth (Plux –Wireless Biosignals, S.A.), one
trigger to command the stimulus light (red LED)
turn on/off and two load cells connected with the
break and accelerator pedals.
2.4 Study Outcomes
The primary outcomes of the study are the brake
response time (BRT), which is time frame between
the onset of the red LED and the achieving of a
brake force on the brake pedal of 150N (ms). The
BRT was fractionated in reaction time (RT), foot
transfer time (FTT) and brake pedal travelling time
(BPTT).
2.5 Procedures
The assessments took place in a closed room to
avoid secondary distraction sources. A trained
physiotherapist performed all tests.
After sitting down in the car simulator the
patients were required to adjust the seat in order to
BIOSIGNALS 2012 - International Conference on Bio-inspired Systems and Signal Processing
420
find a comfortable position. A simple and a more
complex
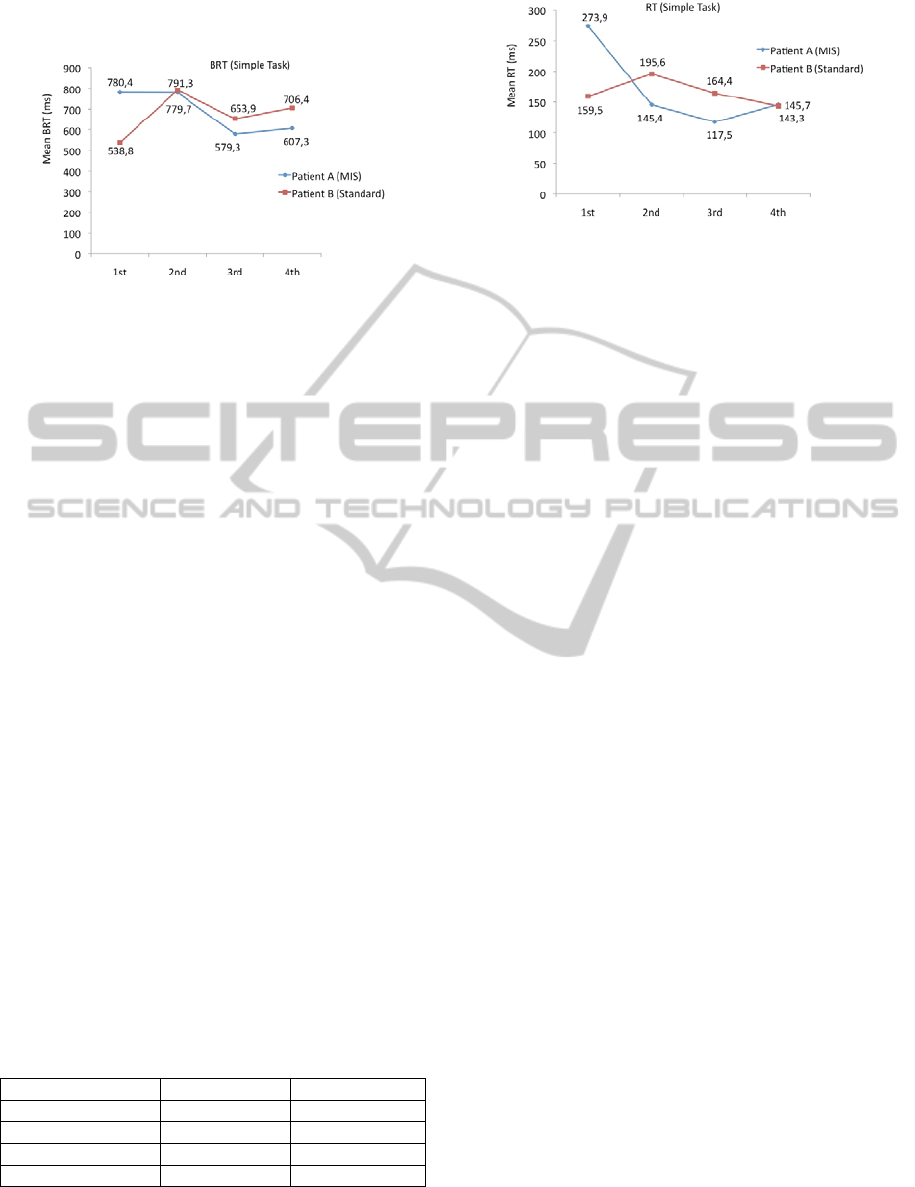
Figure 2: Mean BRT values across the four measurements.
task were used to assess the components of BRT. At
each measurement day patients performed 5 practice
and 10 test trials for each task.
2.6 Data Analysis
Two types of signals were collected: the digital
signal from the light trigger and the force signals
from the accelerator and brake pedal load cells. The
digital signal was used to slice the signals in the 10
break trials for each task. The force signals were
calibrated considering that in the initial instant the
foot is not pressing any of the pedals and the
acquired value in the initial 100ms was considered
the zero of the load cells.
After the pre-processing steps, the onset points of
the force signals were detected by applying a signal-
independent algorithm, which marks significant
events in a signal, based on a morphological analysis
approach (Santos et al., 2012) and the values of the
variables were detected.
3 RESULTS
Patient B is 15 years older then patient A. Despite
that difference patient B had faster baseline
performances in both tasks when compared with
patient A.
Table 1: Demographic data of both patients.
Patient A Patient B
Age (y) 61 76
Body weight (Kg) 71 74
Stature (cm) 167 175
Technique MIS Standard
The effects of TKA on BRT are different when
comparing the data of both cases in the simple task
Figure 3: Mean RT values across the four measurements.
(Fig. 2). Seven days after surgery the mean BRT of
Patient B (Standard) had increased by 46.8% while
the mean BRT of Patient A remained practically
unchanged (decreased 0.08% from the first to the
second measurement). From the second to the third
measurement the mean BRT had decreased by
25.7% and 17.3% for patients A and B respectively.
Thirty-two days after surgery patient A performed
on average 201.1ms quicker then at baseline, while
the mean BRT of patient B was still 115.1ms
increased when compared with baseline.
The BRT increased due to an MT increase. The
RT (Fig. 3) decreased for both patients across the
time, with exception of patient B, who’s RT had
increased by 22.6% from the first to the second
measurement.
The analysis of the MT components (FTT and
BPTT) revealed that the BRT increased mainly due
to an increase of the FTT. The FTT (Fig. 4) had
increased by 57.8% (189.7ms) and 53.7% (144.6ms)
from the first to second measurement respectively
for patient A and B. At 40 days the mean FTT
values of both patients were still over baseline (see
Figure 5).
The BPTT decreased across the time for Patient
A, however, it increased by 65% for patient B
between the 1
st
and second measurement (Fig. 6),
showing that surgery techniques might have had
different effects on this variable.
4 DISCUSSION
Total knee Arthroplasty reduces pain and increases
function and quality of live in patients with knee
impairments resulting from osteoarthritis. Many
patients undergoing TKA want to know when they
can resume car driving after surgery.
The preliminary data of two patients suggests
that the surgery technique might have an influence
on BRT recovery after TKA.
BRAKE RESPONSE TIME BEFORE AND AFTER TOTAL KNEE ARTHROPLASTY - Tracking Possible Effects of the
Surgery Technique on Motor Performance: Report of Two Cases
421
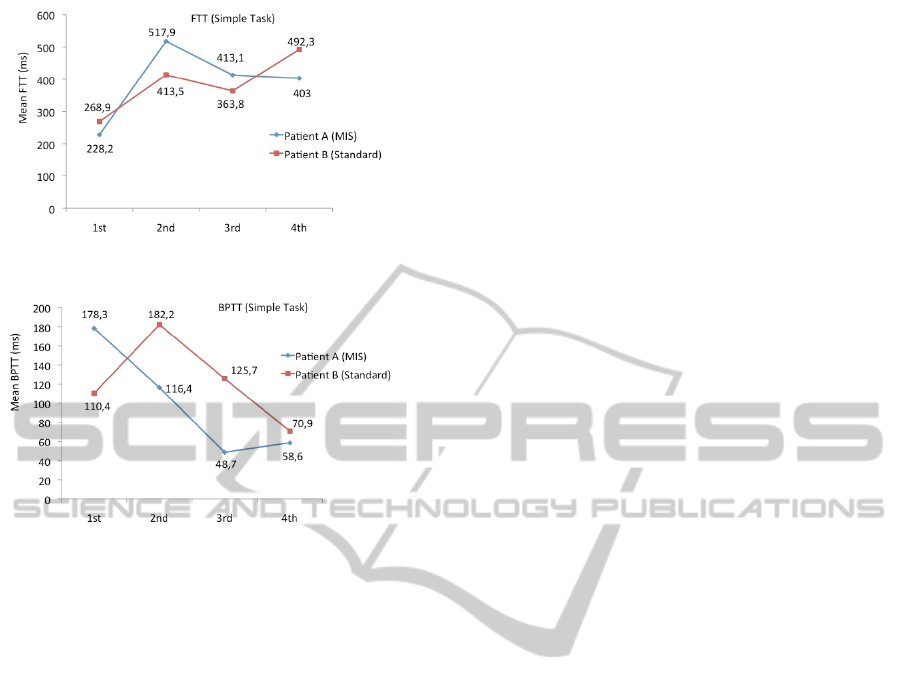
Figure 4: Mean FTT values across the four measurements.
Figure 5: Mean BPTT values across the four
measurements.
The mean BRT of the MIS Patient was not increased
7 days after surgery, while the BRT of the Patient
undergoing standard surgery was increased by
46.8% by same time. Our results reinforce the
results by Dalury and colleagues (2010).
The components of MT (FTT and BPTT)
characterize two distinguished parts of the leg
movement. While during the FTT the leg is being
moved in an open system, with the foot having no
contact with the pedals, during the BPTT the leg is
being moved in a closed system, with the foot
pressing the brake pedal and the knee making an
extension. The performance pattern of the patients in
the open system (FTT) is very similar (Fig. 4), with
both patients showing a performance increase after
surgery followed by a decrease. On the other hand,
in the closed system (BPTT), the patient’s
performance provides an interesting difference, with
the MIS patient having no performance impairments
after surgery (Fig. 5). The eversion of the patella
during the standard approach may be the reason
behind the BPTT differences (Majima et al., 2011).
In order to find out, whether the observed trends
are related with the surgery technique the patients
underwent and not due to inter-subject variations, a
bigger sample is necessary.
REFERENCES
Dalury, D. F., Tucker, K. K. & Kelley, T. C. (2010) When
Can I Drive?: Brake Response Times After
Contemporary Total Knee Arthroplasty. Clin Orthop
Relat Res.
Haas, S. B., Manitta, M. A. & Burdick, P. (2006)
Minimally Invasive Total Knee Arthroplasty: The
Mini Midvastus Approach. Clin Orthop Relat Res,
452, 112-6.
Liebensteiner, M. C., Kern, M., Haid, C., Kobel, C.,
Niederseer, D. & Krismer, M. (2010) Brake Response
Time Before And After Total Knee Arthroplasty: A
Prospective Cohort Study. BMC Musculoskeletal
Disorders.
Majima, T., Nishiike, O., Sawaguchi, N., Susuda, K. &
Minami, A. (2011) Patella Eversion Reduces Early
Knee Range Of Motion And Muscle Torque Recovery
After Total Knee Arthroplasty: Comparison Between
Minimally Invasive Total Knee Arthroplasty And
Conventional Total Knee Arthroplasty. Arthritis,
2011, 854651.
Marques, C. J., Barreiros, J., Cabri, J., Carita, A. I.,
Friesecke, C. & Loehr, J. F. (2008a) Does The Brake
Response Time Of The Right Leg Change After Left
Total Knee Arthroplasty? A Prospective Study. Knee,
15, 295-8.
Marques, C. J., Cabri, J., Barreiros, J., Carita, A. I.,
Friesecke, C. & Loehr, J. F. (2008b) The Effects Of
Task Complexity On Brake Response Time Before
And After Primary Right Total Knee Arthroplasty.
Arch Phys Med Rehabil, 89, 851-5.
Marques, C. J., Gamboa, H., Lampe, F., Barreiros, J. &
Cabri, J. (2011) Muscle Activations Thresholds Before
And After Total Knee Arthroplasty - Protocol Of A
Randomized Comparison Of Minimally Invasive Vs.
Standard Approach. Proceedings Of The International
Conference On Bio-Inspired Systems And Signal
Processing. Rome, Italy.
Pierson, J. L., Earles, D. R. & Wood, K. (2003) Brake
Response Time After Total Knee Arthroplasty: When
Is It Safe For Patients To Drive? J Arthroplasty, 18,
840-3.
Santos, R., Sousa, J., B., S., Marques, C. J. & Gamboa, H.
(2012) Biosignals Event Detection: A Morfological
Signal-Independent Approach. Proceedings Of The
International Conference On Bio-Inspired Systems
And Signal Processing. Vilamoura, Portugal.
Spalding, T. J., Kiss, J., Kyberd, P., Turner-Smith, A. &
Simpson, A. H. (1994) Driver Reaction Times After
Total Knee Replacement. J Bone Joint Surg Br, 76,
754-6.
BIOSIGNALS 2012 - International Conference on Bio-inspired Systems and Signal Processing
422
