
AUGMENTED REALITY BASED REHABILITATION SYSTEM
WITH SELF-DESIGNED DATA-GLOVE
S. K. Ong, Y. Shen and A. Y. C. Nee
Mechanical Engineering Department, Faculty of Engineering, National University of Singapore, Singapore, Singapore
Keywords: Human-computer Interaction, Augmented Reality, Data-glove, Rehabilitation.
Abstract: In this research, a rehabilitation system based on Augmented Reality has been developed to recover hand
motions. With the self-designed data-gloves and Augmented Reality technology, intuitive human-computer
interaction has been developed to provide entertaining and engaging rehabilitation programs. A self-
designed data-glove is used to detect the grasping movements of the patient’s hand, collect the physical
information of the patient and provide tactile feedbacks according to the performance of the patient. With
the advantages of seamless merging of virtual and real elements, controllable environment and intuitive
interface, Augmented Reality based rehabilitation systems can provide entertaining exercising programs to
the patients. In the developed rehabilitation system, multimodal feedbacks are provided to reduce the fatigue
and make the patients more engaged in the rehabilitation sessions.
1 INTRODUCTION
It is expected that the proportion of people aged
above 60 years old would reach 19% by 2050, and
there would be a growing proportion of individuals
who suffer from disabilities due to illnesses related
to ageing. Rehabilitation plays a huge part in the
recovering process to maintain and restore the
maximum movements and functional ability of the
body throughout the lifespan of the individuals.
With effective rehabilitation systems, motor
functions can be recovered, the independent living
ability can be enhanced and the cost in healthcare
can be reduced. There are three key factors in motor
functions recovery, namely, early intervention, task-
oriented training and repetition intensity (Malouin et
al., 2003). Therefore, an effective rehabilitation
system should be able to provide repetitive training
with affordable costs and easy monitoring of the
recovering progress with set goals.
Although conventional rehabilitation systems
have been proven to be useful in recovering of the
motor functions (Kwakkel et al., 1999), they have
disadvantages, such as boring content, high cost and
lack of digital monitoring. New technologies can
provide a novel paradigm for therapy methods to
address these issues. Augmented Reality (AR)
technology (Azuma, 1997) augments a user’s view
of the real world by superimposing virtual objects
with the physical world. With an AR-based
interface, the users can interact with the virtual
objects in a real environment.
In this paper, a rehabilitation system for hand
movements based on AR technology, sensors and
video games is presented. A sensor-based data-glove
has been developed to detect the grasping
movements and provide tactile feedbacks so as to
support intuitive human-computer interaction
allowing patients to interact with virtual objects in a
real environment using natural hand movements.
Virtual elements which can be interacted using the
data-gloves are designed in the video games based
on AR technology to provide the entertaining
exercising environment.
2 RESEARCH BACKGROUND
Traditional rehabilitation processes to recover motor
functions are usually carried out with external
devices, e.g., the nine-hole pegboards, the exercise
hand skate, and repetitive practices. In these
systems, the exercises are closely monitored by the
therapists. A limitation in these traditional
rehabilitation systems is boredom, which is usually
observed in rehabilitation programs requiring
73
Shen Y., Ong S. and Nee A..
AUGMENTED REALITY BASED REHABILITATION SYSTEM WITH SELF-DESIGNED DATA-GLOVE.
DOI: 10.5220/0003806100730078
In Proceedings of the 2nd International Conference on Pervasive Embedded Computing and Communication Systems (PECCS-2012), pages 73-78
ISBN: 978-989-8565-00-6
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)
intensive practice. Tedious practices without fun and
entertainment tend to reduce the motivation of the
patients. Another limitation is the high cost of these
rehabilitation systems, which would impose
considerable financial burden on the patients and
make it difficult for them to undergo the practices
needed to effect neural and functional changes.
There is no data collection function in these systems,
as conventional rehabilitation systems are designed
without sensors such that digital information of the
performance progress cannot be collected.
Providing an enhanced environment by
augmenting virtual objects into the physical world
seamlessly, AR technology can provide an intuitive
interface to rehabilitation systems. Luo et al.,
(2005a) developed rehabilitation system integrating
AR and assistive devices for hand opening actions of
stroke survivors. Dynamic feedbacks of the subject
performance are provided. Luo et al., (2005b) also
designed a rehabilitation system to facilitate the
rehabilitation of the grasp-and-release tasks, where
users without muscle strength can move virtual
objects without difficulties.
Sucar et al., (2008) developed a web-based
gesture therapy system using AR to provide
intensive motion training at low cost. Visual
feedback of the patient’s performance is provided
and the practice progress is illustrated through a
simple statistical chart. AR-REHAB (Alamri et al.,
2010) is an AR rehabilitation system to increase the
immersive feeling of the post-stroke patients.
Fiducial markers are used to track the hand
movements of the patients, which are analysed to
evaluate and monitor the performance of the
patients. AR-based games (Burke et al., 2010) have
been reported to support upper limb rehabilitation,
where AR markers are used to augment everyday
objects and track the movements of these objects.
This project takes into consideration the principles in
game designs to enhance the user engagement.
Wang et al., (2010) developed an AR system
with the use of air pressure detecting devices. Based
on the physical condition of the users, which is
measured using pressure sensing devices, the
parameters of the game are adjusted to ensure that
patients with different extents of hand impairments
can interact with the game. Correa et al., (2009)
created an AR system to facilitate accessing music
by the disabled patients, where patients without
muscle strength can use this system. The AR Piano
Tutor involves virtual objects augmented onto a real
MIDI keyboard in a video captured scene which
represents the user’s viewpoint (Barakonyi and
Schmalstieg, 2005). However, a patient with limited
finger strength and control may not be able to
depress the physical keys. Zhang et al. (2010)
projected a virtual piano onto the real environment
and a self-designed data-glove with flex sensors is
used to measure the flexing angles of the fingers.
3 METHODOLOGIES
3.1 System Architecture
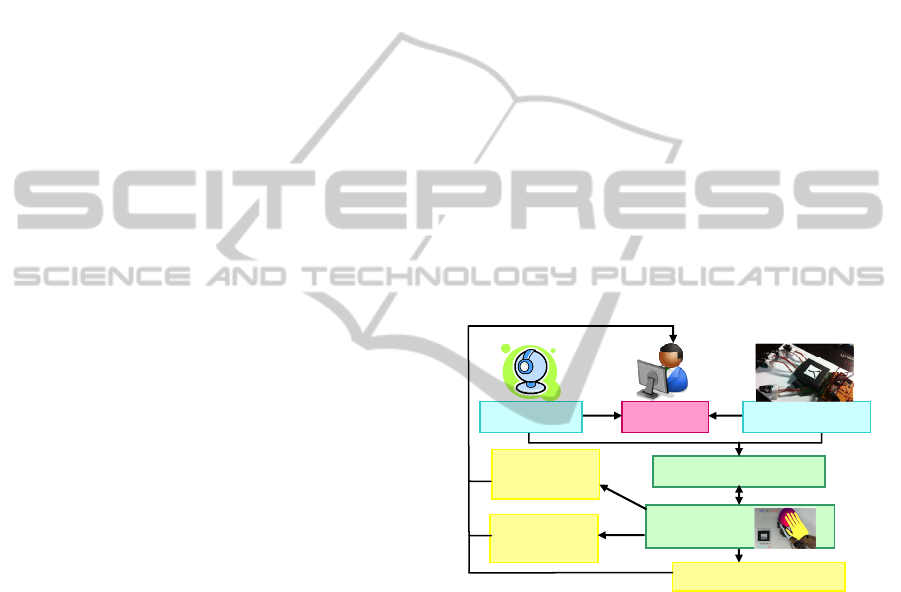
The proposed system shown in Figure 1 aims to help
patients to improve their grasping strength as well as
train their hand-eye coordination via AR-based
game play with a self-designed data-glove. The
system hardware includes a standard computer, an
off-the-shelf webcam and a self-designed data-
glove. With the force sensitive resistors sewn on the
glove, the data-glove can detect the grasping force
applied on the fingers. The multiple threading
method and the function of the playlist in the
OpenGL library are used to ensure that the system
would work in real time without any time lag.
Patient
Motion Capture
Visual
Feedbac
k
Audio Feedback
Data-glove
Camer
a
Video Game
Haptic
Feedbac
k
Figure 1: The system architecture.
A “burst the balloon” game has been developed
to train the grasping movements of the patient’s
hand. The virtual balloons are rendered in the real
environment by tracking a marker using ARToolKit
(ARToolKit, 2002). With another marker on the
data-glove, the virtual hand overlaid on the real hand
would interact with the virtual balloons. The
collision between the virtual balloon and the
patient’s hand is determined by detecting the
collision between the virtual balloon and the virtual
hand using the VCollide library.
Upon collision between the virtual balloon and
the virtual hand, the balloon will burst when a
sufficient amount of force is applied. Performance
will be based on the number of balloons burst out of
a total of twenty balloons. There are also different
PECCS 2012 - International Conference on Pervasive and Embedded Computing and Communication Systems
74
levels of difficulties that the user can choose to suit
their rehabilitation progress. With a higher difficulty
level, balloons will appear at faster speeds and a
greater force will be needed to burst the balloons.
Multimodal feedbacks, namely, visual, audio and
tactile feedbacks, are provided based on the
performance of the patients. These feedbacks are
important performance indicators. They can further
encourage the practice and maintain the interest
level of the patients. The feedbacks are provided
mainly in two aspects, viz., the change of the context
in the gaming environment and the display of the
quantitative information of the performance.
The scoring module in the system is designed to
record the accuracy of the patient interaction with
the system. Rendering the quantitative information
recorded by the scoring module onto the screen can
provide the patients with performance feedbacks.
The quantitative information can be stored, making
it convenient for the therapists to monitor the
recovering progress of the patients and analyse the
effectiveness of the rehabilitation system.
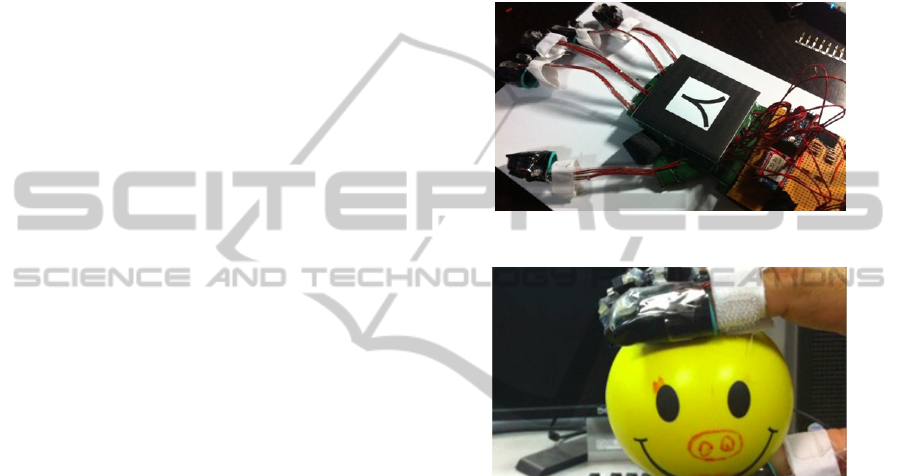
3.2 Self-designed Data-glove
The data-glove shown in Figure 2 is used to detect
the grasping forces of the fingers as the fingers
interact with the virtual objects in the AR
environment. The touching sense is applied to the
fingers with a real ball held in the user’s hand, as
shown in Figure 3. The force sensing resistors (FSR)
are sewn onto the glove to obtain the pressing forces
of the fingers. The grasping movements detected by
this data-glove can be transmitted wirelessly via
Bluetooth to the system.
The data-glove is designed to be used in the AR-
based rehabilitation system. Therefore, it should be
able to be worn on patients whose fingers cannot
move freely. Open-design is implemented to develop
the data-glove in which Velcro belts are used to affix
the data-glove to the hand, as shown in Figure 2.
This data-glove consists of five parts, i.e., the
FSR module, the computing module, the information
transmission module, the power supply module and
the feedback module. The FSR module is used to
detect the pressing forces of the fingers. The
computing module, i.e., the microcontroller
(Arduino Pro mini microcontroller) is used to collect
the analogue signals from the sensors. The
microcontroller also performs some preliminary
information processing, such as converting the
analogue signals into digital signals and basic
computation. The information transmission module
is based on the Bluetooth technology to achieve
wireless information communication between the
computer and the microcontroller. The power supply
module includes a battery and a voltage regulator to
ensure the microcontroller works under a stable
voltage of 3.3V and the Bluetooth works under a
voltage range of 3.3V~6V. For the feedback module,
miniature vibration motors are mounted on each
finger tip to provide tactile feedback when the hand
is squeezing to burst the balloon.
Figure 2: Self-designed data-glove.
Figure 3: A ball is held in the game.
When a larger pressure is applied to a FSR on the
data-glove, the resistance of the FSR will be lower.
In the circuit of the FSR, the microcontroller
provides the power supply. The current in the circuit
and the voltage between the two points of the
resistor will be changed accordingly. The voltage is
input into an analogue port of the microcontroller
and converted to a digital value through the Analog-
to-Digital converter in the microcontroller.
Calibrations have been conducted to obtain the
relationship between the voltage output in the circuit
and the force applied to the FSR. Due to the
limitation of the FSRs, the relation between the force
applied and the change in the resistance is not
directly proportional. In addition, there is only a
limited useful operating range. After a series of
calibrations, it is observed that all the FSRs on
different fingers exhibit similar trends; therefore,
only the limited range of 0N to 6N is used.
The self-designed data-glove is low cost and
affordable to normal users. It is not only a great tool
AUGMENTED REALITY BASED REHABILITATION SYSTEM WITH SELF-DESIGNED DATA-GLOVE
75
to improve on the user’s condition, but at the same
time monitor the patient’s progress throughout the
whole gaming process.
3.3 Burst the Balloon Interactions
The Burst the Balloon game is a simple and intuitive
game that does not require complicated instructions
and has a relatively short learning curve. When there
are virtual balloons flying from the marker into the
3D space, the patient is required to move his hand
with the data-glove to the position of the virtual
balloon and squeeze the real ball at the same time.
Therefore, the rehabilitation system can help patients
improve their grasping strength as well as train their
hand eye coordination ability.
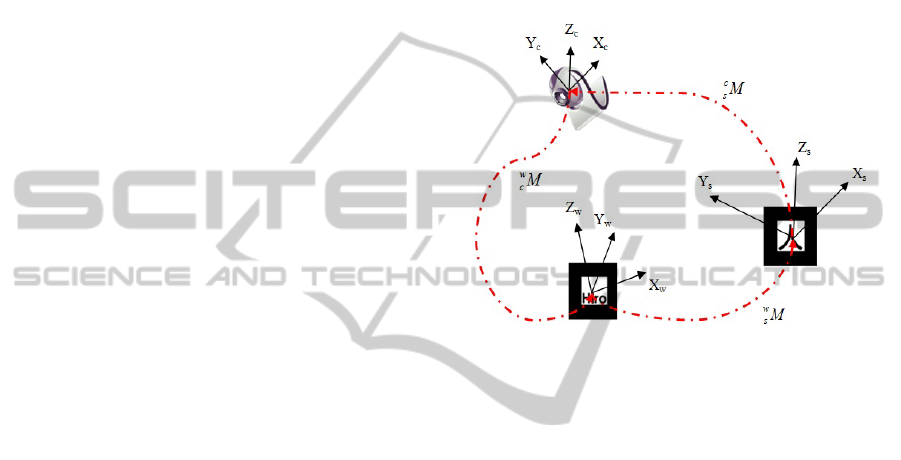
Interaction between the virtual hand and the
virtual balloons consists of two parts, i.e., coordinate
transformation and collision detection. Since the
virtual hand and the virtual balloons are rendered in
two different coordinate systems on two markers,
coordinate transformation is needed to compare the
relative positions of the two virtual objects, using the
camera coordinate system as a bridge between these
two different markers (Figure 4). The “Hiro” marker
associated with the virtual balloons is set as the base
coordinate system. The coordinates of the “Hiro”
and the “Kanji” markers in the camera coordinate
system can be determined through analysing the
images captured by the camera using the functions
provided by ARToolKit. When signals from the
FSRs show the fingers grasping, the position (i.e., x-
, y- and z-coordinates) of the virtual hand in the
“Kanji” marker coordinate will be transformed to a
position in the “Hiro” marker coordinate system, and
compared with the position of the virtual balloon
using the VCollide library. If the virtual hand
collided with the virtual balloon, it is assumed that
the balloon is about to burst. After a collision has
been detected, a balloon bursting sound is played,
and the colour of the virtual balloon is changed from
red to green, and the miniature vibration motors
mounted on the finger tips are activated to provide
tactile feedback. In this rehabilitation system, a real
ball is held by the patient to provide more realistic
touching sense and provide haptic feedbacks when
the patient is pressing the ball.
4 IMPLEMENTATION
The rehabilitation system has been implemented on
a P4 3 GHz PC equipped with 1 GB RAM, an
ordinary web camera and a display device. The self-
designed data-glove is used as the input device.
The rehabilitation system aims to allow the user
to have a more interactive interface, with different
levels of difficulty to choose from to provide
suitable challenges during the game playing process,
which needs to be considered when the patient’s
physical conditions have been improved. Therefore,
the user interface should be designed to be
interactive, user friendly, suitable for all ages and
have different levels of difficulty.
Figure 4: Coordinate transformation between two markers.
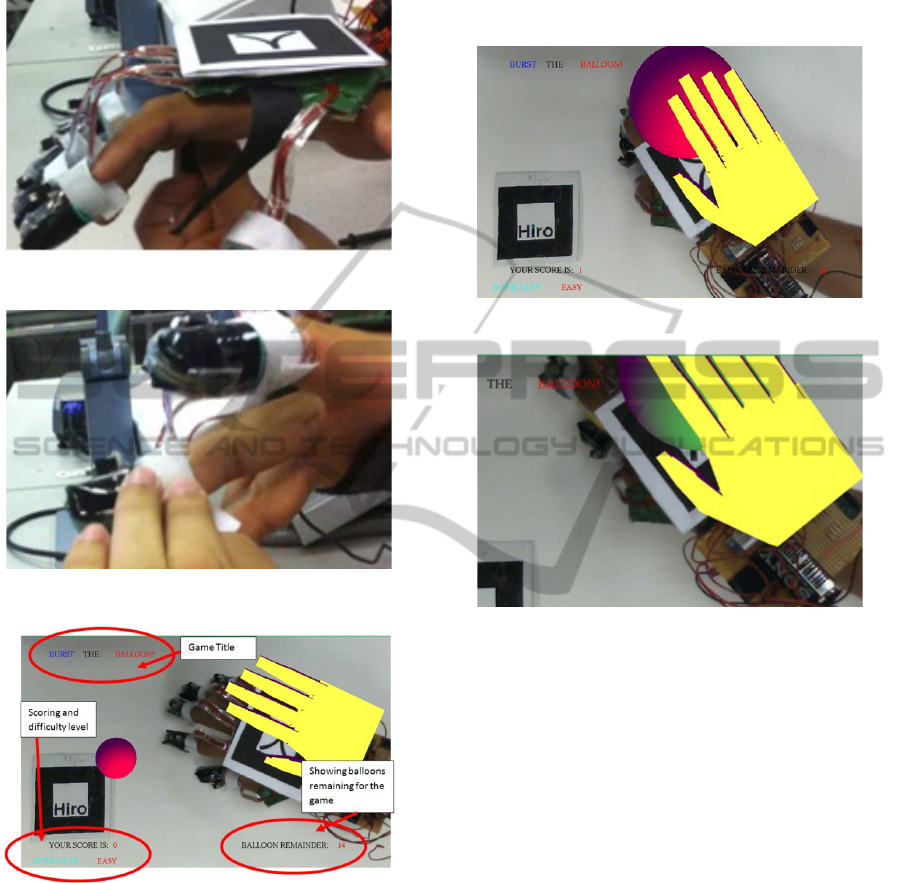
4.1 Preparation Stage
The data-glove is simple in design and ergonomic
for use. The instructions to put on the data-glove are
as follows: (a) Strap on the main Velcro across the
palm of one’s hand, as shown in Figure 5, (b) Slot in
the respective finger into the main finger
compartment, (c) Secure the finger compartment by
strapping on the white Velcro just below the finger
compartment to the respective finger, as shown in
Figure 6, and (d) Secure the rest of the four fingers.
4.2 User Interface
In order to facilitate usability, the user interface of
the rehabilitation system is designed to give the user
real time feedback on his/her current game play. The
interface consists of the game title, score, level of
difficulty and balloons remaining in the current
exercising session, as shown in Figure 7.
Three different difficulty levels of the game,
namely, easy, normal and hard, have been developed
to cater to different capabilities of the users. They
can be selected by pressing the ‘E’, ‘N’, ‘H’ key on
the keyboard respectively. The parameters that are
different between the levels of difficulty consist of
the flying speed of the balloons and the amount of
PECCS 2012 - International Conference on Pervasive and Embedded Computing and Communication Systems
76
force to burst the balloons, both of which increase as
the level of difficulty increases.
Figure 5: Put-on the data-glove.
Figure 6: Secure the finger compartment.
Figure 7: Interface of the rehabilitation system.
For each level of difficulty, twenty virtual
balloons will appear from the marker. The user
needs to move his hand to the position of the virtual
balloon and squeeze it, as shown in Figure 8. If the
pressure applied is larger than the force defined for
the selected level of difficulty, the balloon will burst,
playing a “pop” sound followed by vibrations from
the miniature motors. There will be a visual cue
where the balloon will turn from red to green, as
shown in Figure 9. For every successful action, the
score will be increased by 1. The final score will be
rendered to indicate the performance. To restart the
game, the user can select the level of difficulty using
the ‘E’, ‘N’, ‘H’ key on the keyboard, after which
the score and the balloon count will be reset.
Figure 8: A virtual balloon is rendered in 3D space.
Figure 9: The colour of the balloon becomes green.
4.3 Discussion
Comparing the developed system with existing
systems, the AR-based system presented in this
paper has a number of advantages. The data-glove is
low cost (SGD$150) as compared to commercial
force measurement gloves, such as the CyberGrasp
system with a cost of SGD$39000. The scoring
module as well as the multimodal feedbacks can be
monitored and indicate the patient’s progress easily.
The learning curve of the rehabilitation system is
short. This avoids the hassle of explaining the
instructions to the patients especially the elderly or
mentally challenged patients. The system activates
three main senses, namely visual, touch and hearing,
of the users during the exercising processes.
There are a few disadvantages of this proposed
system. The data-glove has limited force sensing
capability, which is only up to 6N. The accuracy is
also limited due to the natural property of the FSR.
More advanced sensors can be implemented to
overcome these limitations. Similar to other AR
games, lighting and visibility of the markers would
AUGMENTED REALITY BASED REHABILITATION SYSTEM WITH SELF-DESIGNED DATA-GLOVE
77

affect the rendering of the virtual objects.
5 CONCLUSIONS
In this research, a rehabilitation system based on AR
technology and sensors has been developed to
recover the grasping movements and the ability of
hand-eye coordination of the patients. The first
contribution of this research is the self-designed
data-glove to measure the grasping forces applied to
the fingertips. With this low-cost data-glove, the
grasping forces and the physical condition of the
patient can be estimated. The second contribution is
the integration of this data-glove with the AR-based
rehabilitation application to provide haptic, audio
and visual feedbacks to the patients using a game
play session. With a real ball held in hand, the
patient can receive haptic feedback, while the virtual
balloon rendered using AR technology can enhance
the effectiveness of the rehabilitation system in
engaging and entertaining the patients and facilitate
the training of the hand-eye coordination of the
patient. With this low-cost rehabilitation system, a
patient can take intensive exercises at home.
Future work will include developing more levels
of difficulty to make the rehabilitation system
suitable for patients with different physical
conditions. The developed system will be evaluated
with a set of criteria. A user study with a large
sample will be conducted to verify the effectiveness
of the developed system and collect more
quantitative information about the system
performance to determine how this rehabilitation
system can support and complement the
rehabilitation process of the users.
ACKNOWLEDGEMENTS
The authors acknowledge contributions from Toh
Wei-de.
REFERENCES
Alamri, A., Cha, J. and Saddik, A. E., 2010. AR-REHAB:
An augmented reality framework for post stroke-
patient rehabilitation. IEEE Transactions on
Instrumentation and Measurement, 59(10), 2010, pp.
2554-2563.
ARToolKit, 2002. ARToolKit2.61 Software. Retrieved 21
September 2011, from: http://www.hitl.washington.
edu/research/shared_space/download/.
Azuma, R., 1997. A Survey of Augmented Reality.
Presence: Teleoperators and Virtual Environments,
6(4), 355 – 385.
Barakonyi, I. and Schmalstieg, D., 2005. Augmented
reality agents in the development pipeline of computer
entertainment. In Proceedings of the 4th International
Conference on Entertainment Computer, Sanda,
Japan, 2005 September 19-21, pp. 345-356.
Burke, J. W., McNeill, M. D. J., Charles, D. K., Morrow,
P. J., Crosbie, J. H. and McDonough, S. M., 2010.
Augmented reality games for upper-limb stroke
rehabilitation. Second International Conference on
Games and Virtual Worlds for Serious Applications,
2010, pp. 75-78.
Correa, A. G. D., Ficheman, I. K., Nascimento, M. do and
Roseli de Deus, L., 2009. Computer Assisted Music
Therapy: a Case Study of an Augmented Reality
Musical System for Children with Cerebral Palsy
Rehabilitation. 2009 Ninth IEEE International
Conference on Advanced Learning Technologies, New
York, pp. 218-220.
Kwakkel, G., Wagenaar, R. C., Twisk, J. W., Lankhorst G.
J. and Koetsier, J. C., 1999. Intensity of leg and arm
training after primary middle-cerebral artery stroke: a
randomised trial. Lancet, 354(9174), 191-196.
Luo, X., Kline, T., Fischer, H. C., Stubblefield, K. A.,
Kenyon, R. V. and Kamper, D. G., 2005a. Integration
of Augmented Reality and Assistive Devices for Post-
Stroke Hand Opening Rehabilitation. In Proceedings
of the 2005 IEEE, Engineering in Medicine and
Biology 27th Annual Conference, Shanghai, China,
September 1-4, 2005, pp. 6855-6858.
Luo, X., Kenyon, R. V., Kline, T., Waldinger H. C. And
Kamper, D. G., 2005b. An augmented reality training
environment for post-stroke finger extension
rehabilitation. IEEE the 9th International Conference
on Rehabilitation Robotics. New York, 2005, pp. 329-
332.
Malouin, F., Richards, C. L., McFadyen, B. and Doyon, J.,
2003. New Perspectives of locomotor rehabilitation
after stroke. Médecine Sciences (Paris), 19(10), 994-
998.
Sucar, L. E., Leder, R. S., Reinkensmeyer, D., Hernández,
J., Azcárate, G., Casteñeda, N. and Saucedo, P., 2008.
Gesture Therapy - A Low-Cost Vision-Based System
for Rehabilitation after Stroke. HEALTHINF, Funchal,
Madeira, Portugal, January 28-31, 2008, pp.107-111.
Wang, H., Hsu, C., Chiu, D. and Tsai, S., 2010. Using
augmented reality gaming system to enhance hand
rehabilitation. 2nd International Conference on
Education Technology and Computer, Shanghai,
China, 22-24 June 2010, V3-243-V3-246.
Zhang, D., Shen, Y., Ong, S. K. and Nee, A. Y. C., 2010.
An Affordable Augmented Reality Based
Rehabilitation System for Hand Motions.
International Conference on CYBERWORLDS, 20-22
October 2010, Nanyang Technological University,
Singapore.
PECCS 2012 - International Conference on Pervasive and Embedded Computing and Communication Systems
78
