
INTERACTIVE VISUAL ANALYSIS OF INTENSIVE
CARE UNIT DATA
Relationship between Serum Sodium Concentration, its Rate of Change
and Survival Outcome
Kre
ˇ
simir Matkovi
´
c
1
, Heng Gan
2
, Andreas Ammer
1
, David Bennett
3
,
Werner Purgathofer
1
and Marius Terblanche
3
1
VRVis Research Center in Vienna, Vienna, Austria
2
Guy’s & St Thomas’ NHS Foundation Trust, London, U.K.
3
King’s College London and Guy’s & St. Thomas’ NHS Foundation Trust, London, U.K.
Keywords:
Interactive Visual Analysis, Coordinated Multiple Views, Intensive Care Unit Data.
Abstract:
In this paper we present a case study of interactive visual analysis and exploration of a large ICU data set. The
data consists of patients’ records containing scalar data representing various patients’ parameters (e.g. gender,
age, weight), and time series data describing logged parameters over time (e.g. heart rate, blood pressure).
Due to the size and complexity of the data, coupled with limited time and resources, such ICU data is often not
utilized to its full potential, although its analysis could contribute to a better understanding of physiological,
pathological and therapeutic processes, and consequently lead to an improvement of medical care. During the
exploration of this data we identified several analysis tasks and adapted and improved a coordinated multiple
views system accordingly. Besides a curve view which also supports time series with gaps, we introduced a
summary view which allows an easy comparison of subsets of the data and a box plot view in a coordinated
multiple views setup. Furthermore, we introduced an inverse brush, a secondary brush which automatically
selects non-brushed items, and updates itself accordingly when the original brush is modified. The case
study describes how we used the system to analyze data from 1447 patients from the ICU at Guy’s & St.
Thomas’ NHS Foundation Trust in London. We were interested in the relationship between serum sodium
concentration, its rate of change and their effect on ICU mortality rates. The interactive visual analysis led us
to findings which were fascinating for medical experts, and which would be very difficult to discover using
conventional analysis methods usually applied in the medical field. The overall feedback from domain experts
(coauthors of the paper) is very positive.
1 INTRODUCTION
The monitoring and management of patients in mod-
ern Intensive Care Units (ICU) is technology-driven
and use numerous high technology equipment. Each
of those has the ability to log various parameters.
Many physiological measurements (such as blood
pressure, body temperature, or heart rate, for exam-
ple), laboratory results, and treatment interventions
are routinely recorded. These measurements help in-
tensive care physicians to understand physiological,
pathological and therapeutic processes, and conse-
quently to improve medical care.
The data collected routinely in a modern ICU cre-
ates very large datasets containing in-depth time-var-
variant and time-invariant data. For various reasons
these datasets are generally not used to their full po-
tential. First, data is often stored on different propri-
etary systems each using difference storing and output
formats. Second, statistical models (particularly for
multi-level longitudinal data) are difficult to develop
and require large datasets to improve estimate preci-
sion. Third, most clinical researchers do not possess
the statistical skills to develop complex models, while
statisticians generally lack the contextual understand-
ing of the biological and clinical processes needed to
develop the conceptual constructs for testing.
The use of data visualization techniques to gain
insight into large ICU datasets is a novel concept.
Historically, standard single and multi variable re-
648
Matkovi
´
c K., Gan H., Ammer A., Bennett D., Purgathofer W. and Terblanche M..
INTERACTIVE VISUAL ANALYSIS OF INTENSIVE CARE UNIT DATA - Relationship between Serum Sodium Concentration, its Rate of Change and
Survival Outcome.
DOI: 10.5220/0003844506480659
In Proceedings of the International Conference on Computer Graphics Theory and Applications (IVAPP-2012), pages 648-659
ISBN: 978-989-8565-02-0
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

gression techniques are used to investigate associa-
tions between one or more predictor variables and an
outcome. The APACHE II (”Acute Physiology and
Chronic Health Evaluation II”) scoring system, for
example, is a severity of disease classification sys-
tem, which was introduced in 1985 (Knaus et al.,
1985), and modified in 1991 (Knaus et al., 1991). The
APACHE II score is computed based on several mea-
surements after a patient enters an ICU, and indicates
how severe a disease is and the risk of death of the
patient. There are other scoring systems as well.
While sophisticated, the conventional techniques
require a high degree of training and do not provide
intuitive insights in the within-data relationships and
linkages. Here we test the ability of interactive visual
analysis to analyze a large ICU data set. Our goal is to
test if such a method is suitable for medical data ex-
ploration. We wanted to see if some new, hidden, cor-
relation can be found in the data which is not present
in standard scores. Although it seems straightforward,
such an analysis is far from trivial.
Data for 1447 patients was collected in the ICU at
Guy’s & St. Thomas’ NHS Foundation Trust, Lon-
don, UK. The ICU is completely paperless and all
medical data, including medical notes and prescrip-
tion charts, are stored centrally. On admission and
during the patient’s stay all parameters are logged and
the data is stored in a central database. The data set
is broadly divided into time-invariant (e.g. ID, age,
gender, admission diagnosis, survival, etc.) and time-
variant data (e.g. sodium concentration, blood pres-
sure, etc.). As we have scalar data and time series data
for every patient we used a data model introduced by
Konyha et al. (Konyha et al., 2006). Instead of hav-
ing only scalar values as attributes in patients records
this model supports time series as attributes. All time
series of one kind (e.g. blood pressure values as a
function of time) for all patients represent a family of
curves.
In this paper we describe how we examined the
association between serum sodium concentration, its
rate of change, and survival outcome. The paper is
written together with domain experts. We use a pow-
erful data preprocessing and a coordinated multiple
views (CMV) system to explore and analyze the data
by means of interactive visual analysis. In order to be
able to perform the study we have improved the curve
view (Konyha et al., 2006) to support different curve
lengths, and to depict gaps in time series. We also in-
tegrated a new summary view along with a box plot
view into the system and introduced a new interac-
tion – the inverse brush. Finally, we have modified an
existing CMV system in order to suit domain experts
needs. All improvements were made after numerous
common sessions with the domain experts. Unex-
pected findings and a very positive feedback from the
domain experts indicated that our approach is feasi-
ble, and demonstrated how interactive visual analysis
can increase understanding of ICU data and poten-
tially contribute to better medical care. The approach
has been preliminary introduced to the medical com-
munity by a poster at a major intensive care medicine
congress (Gan et al., 2011).
2 RELATED WORK
Using coordinated multiple views (CMV) is a com-
mon practice in interactive visual analysis. An
overview of CMV is provided by Roberts (Roberts,
2007). The task of visualizing time-oriented data
however needs additional consideration, reflected
by Shneiderman’s ”Task by Data Type Taxon-
omy” (Shneiderman, 2002), where temporal data is
identified as one of seven basic data types. Aigner et
al. (Aigner et al., 2007b; Aigner et al., 2007a) give
a good overview of characteristics of time-oriented
data and different methods of visualizing it accord-
ingly. According to Aigner et al. (Aigner et al.,
2007b) the time-oriented data in our case can be cate-
gorized as multivariate abstract data at time-points in
linear time shown in a static 2D representation. An
example of interactive visualization and exploration
of time-dependent data is the TimeSearcher appli-
cation by Hochheiser and Shneiderman. (Hochheiser
and Shneiderman, 2002; Hochheiser and Shneider-
man, 2004), who also developed visual query mecha-
nisms for finding patterns in time series data. Visual
queries allow the user to directly compose queries in
the visualization without the need of dealing with ad-
ditional sliders or input fields.
Additionally our time series data contains miss-
ing values, which requires extra consideration. Time
series data which is sampled regularly but contains
missing values can be seen as unregular sampled, or
event-based data. Aris et al. (Aris et al., 2005) devel-
oped for the TimeSearcher application four methods
to deal with such unevenly spaced time series data;
namely: sampled events, aggregated sampled events,
event index and interleaved event index. Since nei-
ther method meets all the requirements of our case –
the first two methods introduce new data at the sam-
ple points, the latter two only consider the order of
events, not the specific time they appeared – we use a
different method in handling missing values.
There exist several approaches to visualize the
time-oriented data of a single patient record. Powsner
and Tufte (Powsner and Tufte, 1994) visualize time-
INTERACTIVE VISUAL ANALYSIS OF INTENSIVE CARE UNIT DATA - Relationship between Serum Sodium
Concentration, its Rate of Change and Survival Outcome
649
oriented data in small repeated graphs. LifeLines by
Plaisant et al. (Plaisant et al., 1996; Plaisant et al.,
1998) uses timelines with colored horizontal bars and
markers to indicate the point in time and the dura-
tion of actions or events (e.g. diagnosed symptoms
or treatments). However LifeLines lacks the ability
to visualize continuous data (e.g. fever curves). Bade
et al. (Bade et al., 2004) try to overcome this short-
coming by introducing height-coded timelines where
the height of the horizontal bar is depending of the
data of an associated time series. The approaches
mentioned in this paragraph seek to visualize many
or even all parameters and time series of one single
patient record as well as possible; we however are in-
terested in comparing parameters and time series of
multiple patient records and finding some relations
between them.
Multiple patient records were analyzed by Gresh
et al. (Gresh et al., 2002), who use information visual-
ization techniques to examine a large collection of pa-
tient records of bone marrow transplants at Hadassah
Hospital in Jerusalem, Israel. Gresh et al. generated
survivability curves for patients with mis-matched
transplant and fully matched transplant and compared
these for transplants received in the last five years
and prior to that. Surprisingly they initially found a
lower survival for the recent transplant patients, but in
subsequent discussions with the physicians they were
able to learn two of the reasons for that. First, the
hospital tends to be better at documenting death dates
than follow-up visits of surviving patients and second
the hospital specialized in the latter years in treating
more serious and complex cases. Although the sur-
vivability curves make use of time, there were no con-
tinuous time data in the dataset they investigated.
The mentioned before LifeLines were also used to
analyze multiple patient records by Wang et al. (Wang
et al., 2008) and Plaisant et al. (Plaisant et al., 2008).
They use aligning by sentinel events (e.g. the first oc-
currence of a symptom) to discover patterns in elec-
tronic health records. Again they are not considering
continuous time data.
Finally Trobec at al. (Trobec et al., 2008) used a
CMV tool and a complex data model to analyze dif-
ferent statistical characteristics and time series from
ECG and respiration measurements from patients af-
ter heart transplantation. They used interactive visual
analysis and other, more conventional approaches.
3 ICU DATA
The dataset that we used in our analysis was created
using a commercial clinical information system (CIS;
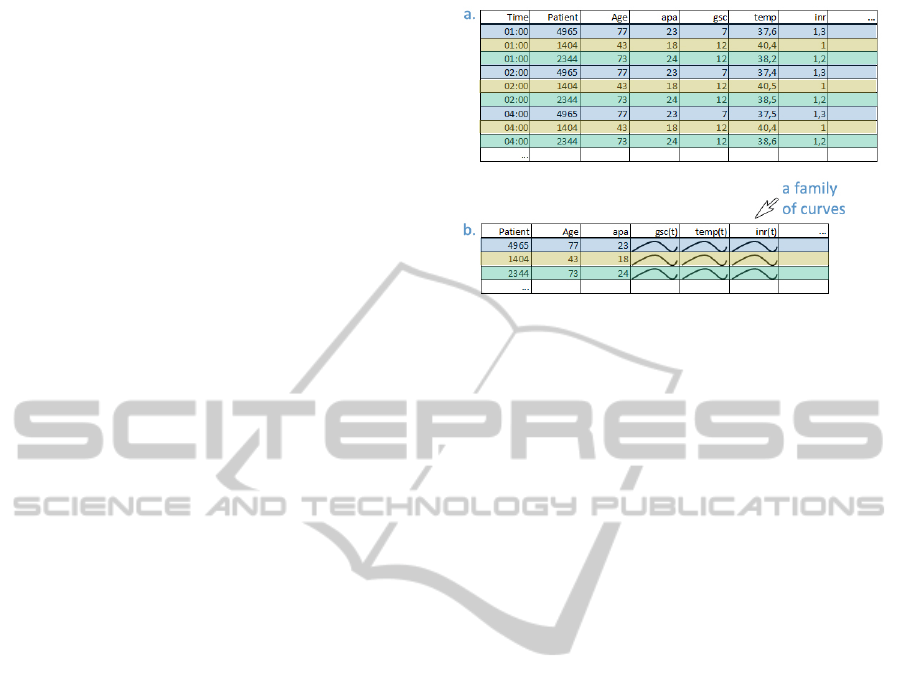
Figure 1: a. A conventional way of storing data. Each log
is a unique record containing patients data, time, and logged
parameters. b. A more complex data model allowing fami-
lies of curves. All records that belong to the same patients
form a single record. There is no time dimension, but in-
stead it is implicitly stored in a curve dimension. There is
gsc(t) now, e.g., in contrast to Time and gsc in the previous
case. We call all curves that belong to the same attribute a
family of curves.
CareVue, Phillips, The Netherlands) and contains one
record for each log. A record here contains patient
data and logged values together with logging time.
Figure 1a. shows such a case. In a simple data struc-
ture we would have a large table with as many rows as
there are records in the database, but since all records
of one patient belong together – they form a logical
unit – we group them to one record. Now a single
attribute is a time series and the number of rows is
equal to the number of patients. In this way we will
be able to follow data belonging to the same patient
more intuitively. Such a data organization reduces the
data size, but increases the data complexity (see Fig-
ure 1b.). At the same time it offers new possibilities
for analysis. The curves that emerged can be analyzed
using some advanced techniques which would be al-
most impossible (or very complicated) using conven-
tional queries and conventional data organization.
During the merging of the data, we noticed that
there are missing values in the time series, and that
time series are of different length. Some data (e.g.
physiological variables) are logged manually at least
hourly, while other data (e.g. laboratory results) are
logged via direct links with the institution’s computer
system. For various reasons missing data is com-
mon in clinical information systems (CIS). Reasons
include clinical need (e.g. a certain test is not clini-
cally indicate for a period of time), practical consid-
erations (e.g. a patient is temporarily transferred out
of the ICU for investigations), technical failure (e.g.
communication issues between the CIS and the insti-
tution’s computer network), or infrequently for main-
IVAPP 2012 - International Conference on Information Visualization Theory and Applications
650

Table 1: A subset of ICU data attributes.
Parameter Acronym Type
Age age numeric
ICU mortality idead numeric
APACHE II score apa numeric
Length of stay in ICU ilos numeric
Baseline venous oxy-
gen saturation
base
so2 numeric
Baseline plasma lactate
concentration
base lact numeric
Heart rate hr tsh time series
Mean arterial pressure map tsh time series
Plasma lactate concen-
tration
lact tsh time series
Venous oxygen satura-
tion
so2 tsh time series
Plasma sodium concen-
tration
na tsh time series
Plasma chloride con-
centration
cl tsh time series
C-reactive protein con-
centration
crp tsd time series
tenance/upgrades of the CIS itself. All time series
data start at the moment the patient enters the ICU,
and last for the time the patient is at the ICU, which
is different for each patient. As a consequence the
lengths of the time series in the dataset are different
for various patients. In order to cope with this issues
we have improved the curve view to support different
length time series.
During the data preprocessing step we have also
computed derived data needed in analysis. For the
time series data we have computed and stored: 1) the
number of small and large gaps; 2) the X and Y span
of time series; 3) the first derivative – in order to ex-
plore the rise or fall in the family of curves, and 4) ba-
sic scalar aggregates such as minimum or maximum
of original and of derived families of curves. Some of
those derived values are scalar values, which means
that a curve from a family is described using a scalar
(one curve is represented by one number) and some of
them are time series aggregates (the first derivative,
e.g.) where time series is represented with another
time series and a new family of curves is introduced.
We have even computed some scalar aggregates of de-
rived time series (maximum of the first derivation, for
example).
We have more than 40 attributes in the data set
(numeric and time dependent), and we have computed
about 20 aggregates in total. Table 1 lists the most
relevant subset used in the examples described in the
paper.
4 INTERACTIVE VISUAL
ANALYSIS OF ICU DATA
In our analysis we use a coordinated multiple views
system which supports iterative multiple brushes. The
main idea of coordinated multiple views is to use
more views to depict various data dimensions. User
can interactively brush (select) a subset of data in one
view and all corresponding items in all other, linked,
views are highlighted. Remember our records are pa-
tients based, so when some items are highlighted in
one view the items belonging to the same patients are
highlighted in all other views. The tool supports com-
posite iterative brushing, i.e. it is possible to combine
more brushes using basic logical operations, and the
last brush is always combined with the previous se-
lection. Such a system allows for a quick information
drill down, and it is especially suitable for data explo-
ration and analysis of hidden correlations. After just a
few sessions with our medical experts we realized that
we needed a quite fix view organization. We have di-
vided the main frame into four parts (Figure 2). We
have a data manipulation part on the left (”A” in the
Figure 2), exploration part (”B”) in the middle, sum-
mary part (”C”) on the right, and details on demand
part (”D”) in the lower part of the screen. The data
manipulation part shows all the dimensions with their
ranges and allows the user to easily filter out records
with unwanted values during the analysis. The explo-
ration part is the core part. It is often reconfigured
during the analysis. We will show excerpts from the
exploration part with a detailed description in the rest
of the paper. We mostly used four to six views in
this part, and if some tasks needed more views they
were depicted in additional floating views. The float-
ing views contain only exploration views and are usu-
ally shown on a second monitor. The summary part
shows some statistical moments of the most important
dimensions in a boxplot along with a quick overview
of the different brushes. By simple triangular glyphs
depicting the differences between the selected sub-
sets and the overall dataset, relations between subsets
and dimensions can easily be noticed. Finally, experts
need details at the end of the drill down process. All
the available data for selected patients is shown and
can be exported if needed in the details on demand
part.
The data described in the previous sections has
some characteristics that required improvements of
the existing visualization system. We improved the
curve view as proposed by Konyha et al. (Konyha
et al., 2006) and we have introduced a summary view
along with a box plot view in a coordinated multiple
views setup. During our analysis sessions the medi-
INTERACTIVE VISUAL ANALYSIS OF INTENSIVE CARE UNIT DATA - Relationship between Serum Sodium
Concentration, its Rate of Change and Survival Outcome
651
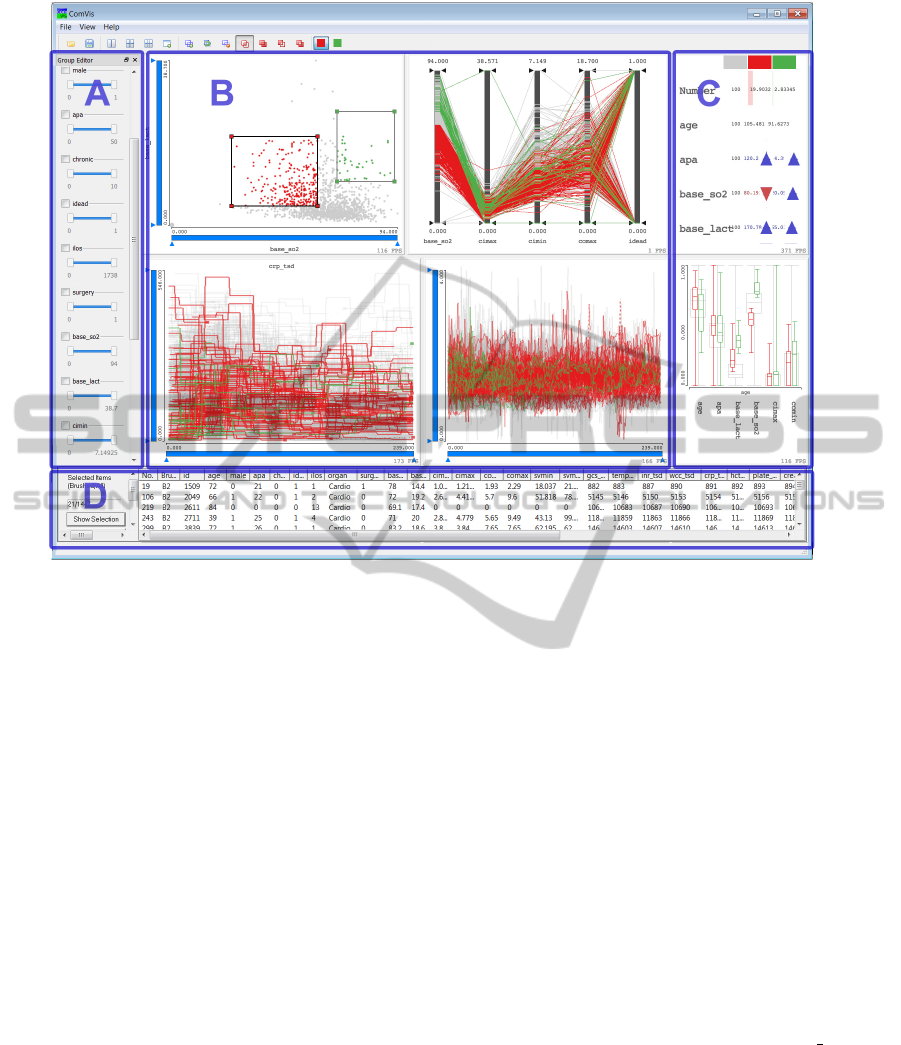
Figure 2: The coordinated multiple views system used. The views organization is fix and defined together with domain
experts. A. Data part shows all dimensions and their ranges. User can easily filter out records here. B. Exploration part used
for the interactive analysis. Views are freely configurable. There can be more views, and additional views can also be depicted
in a floating view. C. Summary part shows summary of selected dimensions. There are two views, summary overview and
box plot views. In case of multiple composite brushes a summary for each brush is shown. D. Details on demand – complete
data for each patient – are shown after drill down.
cal members of the team needed an ”inverse brush”.
In standard systems brushed items are usually shown
in contrast to a context, i.e. all items, but we wanted
to see the brushed items in context of all, along with
the non-brushed items in context of all, and the non-
brushed items in comparison to the brushed items. We
will describe each of our improvements to the CMV
system in the next subsections in more detail.
4.1 Depicting Gaps using a Curve View
The curve view as proposed by Konyha et al. (Konyha
et al., 2006) depicts all curves of a family simultane-
ously. In order to show the density of curves in a cer-
tain area a density based transparency is used. The
curves in our dataset have gaps, and the gaps cannot
be simply ignored. If gap start and end points would
be simply connected, values which might be wrong
are introduced without any warning. The user has to
know if data had been measured or if it is just miss-
ing. We propose to distinguish between small gaps
and large gaps (user can define the limits), and we de-
pict start and end points of all gaps using points (with
user defined colors and sizes, different for large and
small gaps, and start and end points). Furthermore we
let the user choose the line type which will be used
to ”bridge” the gap if the user decides to draw a line
in a gap at all. If lines are not drawn the notion of
which curve segments belong together might be lost
in the case of many gaps. A mouse over function-
ality solves this problem. The whole curve is high-
lighted when the mouse is pointing to any of the gap
points. Figure 3a. illustrates the new curve view with
small gap points depicted in green, large gap points
depicted in red, and a yellow curve highlighted us-
ing the mouse over functionality. The crp tsd pa-
rameter is depicted in this figure. Although the figure
might seem crowded and not informative, in a linked
view setup the user can quickly drill down and reduce
the curves to a subset in focus. Figure 3b. and c.
show such subsets of curves in focus (red) and all
curves in context (gray). The curves of interest can
be seen clearly now. Proposed improvements helped
us in cleaning the data and in understanding what is
IVAPP 2012 - International Conference on Information Visualization Theory and Applications
652
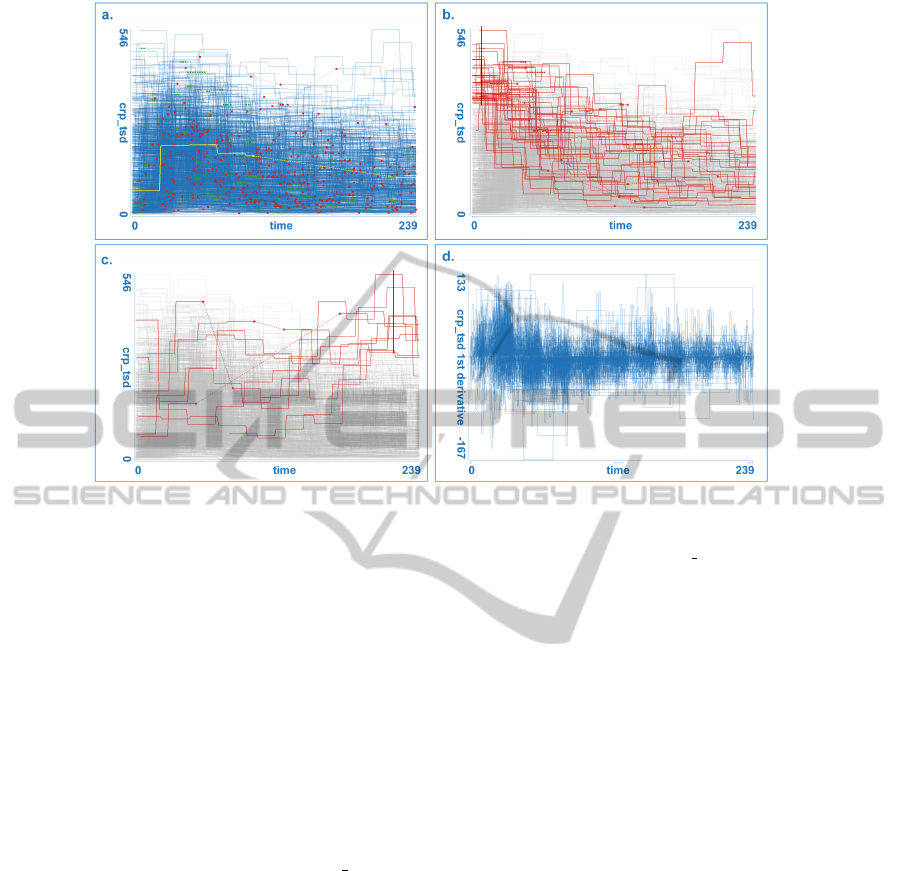
Figure 3: a. Enhanced curve view which shows all curves from a family simultaneously, with gap starting and ending points.
The yellow curve has been selected by simple mouse-over functionality. b. User selects all curves with high values at the
beginning (black line used for selection). Note that most of those curve sink with time, the crp tsd values become lower.
c. Curves with high values after 23 hours. Note one curve with a very long gap; values depicted using dashed line are most
probably wrong. d. Depicting the first derivation aggregate will be very useful in the analysis later. Straight horizontal lines
indicate gaps, and represent an alternative way to see them.
missing. We assumed there were some gaps when we
started the analysis, but the number of gaps showed to
be higher then expected by medical experts and intro-
duced improvements were very welcomed, especially
during the data preparation phase.
As stated in section 3 we have used various ag-
gregated dimensions in the analysis. The first deriva-
tion, primarily used to explore the rise and fall of cer-
tain parameters can be used to identify gaps as well.
Figure 3d. shows the first derivative of cr p tsd (pa-
rameter showed in Figure 3a. - c.). Note the straight
line segments which correspond to gaps. Such a vi-
sualization of gaps (which is not a primary use of the
first derivative aggregate) might be more useful some-
times.
4.2 Box Plot in the CMV
The medical experts in our team are used to the box
plot visualization. The box plot is a common and
convenient way to depict summaries of data (Tukey,
1977; McGill et al., 1978). In a multidimensional
data case, one box plot depicts summaries of one di-
mension (of course this is only possible for scalar di-
mensions). We have integrated a box plot view in the
CMV system. The view shows many adjacent box
plots. A relative scale (all box plots have the same
height) and an absolute scale is supported. Interest-
ingly, we used relative scale more often, as it was
clear to the experts that the overall ranges are not the
same. The box plot view is linked with all other views
and if something is brushed the box plot shows data
for context and for brushed data. Figure 4a. shows
a box plot view. Figure 4b. shows the same view in
a case where brushing is active. The box plots for
the brushed items are depicted in color (focus) and
are drawn on top of the gray box plots representing
all values (context). The user can easily compare the
values of the selection and the context. The focus is
a result of complex brushing in several other views.
User can combine brushes using boolean algebra, and
the box plot shows the distribution of the final brush.
4.3 The Brush Overview View
The brush overview allows a quick comparison be-
tween the different selected subsets and the overall
data (see Figure 5). In a table layout where each col-
umn corresponds to a brush (i.e. a subset of the data)
and each row corresponds to a dimension, glyphs
and numerical values are depicted. The first column
hereby corresponds to the overall dataset. The first
INTERACTIVE VISUAL ANALYSIS OF INTENSIVE CARE UNIT DATA - Relationship between Serum Sodium
Concentration, its Rate of Change and Survival Outcome
653
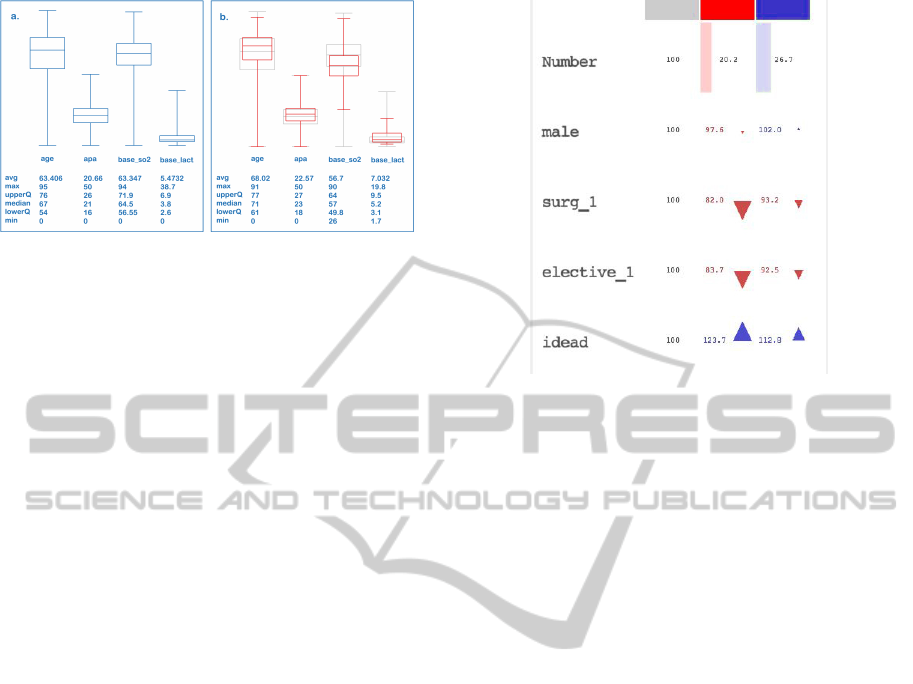
Figure 4: The newly introduced box plot view is integrated
into a CMV system. The view can show all dimensions us-
ing a relative scale, which means that all plots have the same
size although the minimum and the maximum values vary
significantly between dimensions. a. 4 parameters depicted
using absolute scale. b. brushed items plots depicted in red
and all items in gray plots.
row shows the actual number (and/or percentage) of
selected items per brush. Each cells shows the differ-
ence between an aggregate (e.g., average, mean, etc.)
of the brush in the corresponding dimension to the
according aggregate in this dimension of the overall
dataset. This can be indicated numerically by show-
ing the calculated values directly or by the percent-
age in regard to the overall aggregate. An additional
simple triangular glyph visualizing this differences al-
lows easy and fast comparing of different selections in
many dimensions and therefore facilitates the discov-
ery of relationships between them.
4.4 The Inverse Brush
The standard brushing makes it possible to combine
several brushes using boolean operations (and, or,
not). As described above, the brushed data is then
depicted simultaneously with the context. During our
analysis session medical experts often wanted to see
the distribution of not brushed data. Note that this is
different then showing the context which represents
all data. This is also different from a simple NOT
brush. We introduce an inverse brush, a brush that
is coupled to an existing composite brush and shows
always the not selected items. In this way, it is pos-
sible that the user drills down using a combination of
several brushes, and the inverse brush follows these
selections. The system will show the context, the
brushed items and the not brushed items. If the user
interactively changes any of the brush components of
a composite brush, the inverse brush will be auto-
matically updated. The inverse brush functions in all
views, although it is most useful for summary views.
Figure 5: The brush overview shows the differences be-
tween aggregates (e.g. average, mean) of the selected sub-
sets (brushes) and of the overall dataset. Each column cor-
respond to one brush. The first row shows the number of
selected items, further rows the aggregates by dimensions.
In this figure only percentages are shown. The arrow glyphs
allow fast perception of differences (e.g. the red brush se-
lects a subset where parameter idead is set 23,7% more of-
ten than in the overall dataset)
4.5 Supported Interaction
Besides above described views we have used par-
allel coordinates, histogram, scatter-plot, and tag-
cloud views during our analysis. All these views
are integrated in the CMV system, and they all sup-
port linking and brushing. We will briefly describe
various brush types supported by those views. In
the histogram view the user can select bins that are
brushed. All records that have a particular dimension
depicted using the histogram in the range defined by
the brushed bins will be highlighted. The brush can
be resized and freely moved to cover other bins. In
the scatterplot view we support a rectangular brush.
The user can select a rectangular area in the scatter-
plot and all points (patients) which are selected will
be highlighted. The brush rectangle can be moved and
resized. The parallel coordinates support axis brush-
ing, the user can brush a range on any axis. Just as in
the case of histogram, the user can resize or move the
brush, changing the range for one parameter. Finally,
the curve view supports the line brush. It is a simple
line drawn in the view. All curves that cross the line
are selected or brushed. The user can move the line or
move the line end points. Figure 6 shows four main
view types with various types of brushes.
IVAPP 2012 - International Conference on Information Visualization Theory and Applications
654
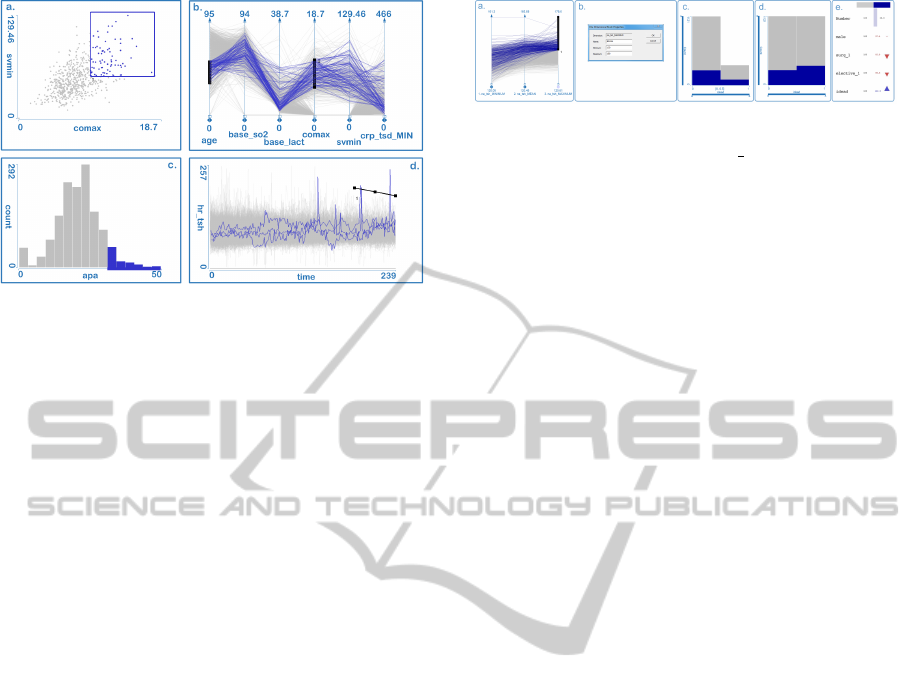
Figure 6: Various views support various types of brushing.
All items (patients) selected in one view are highlighted in
all other views. a. A rectangular brush in scatterplot selects
patients having two parameters in specified ranges. b. A
range on each axis of the parallel coordinates plot can be
selected. c. User can select neighboring bins in a histogram.
d. A simple line brush is used in the curve view. All curves
crossing the line are selected.
5 CASE STUDY
There has been increasing interest in recent years
within the critical care community in the role of serum
sodium in fluid management, acid-base balance and
ICU mortality. While both high and low serum
sodium concentrations are associated with increased
mortality, therapies that rapidly change sodium con-
centrations are also associated with an increase in
mortality (Lindner et al., 2007; Rocktaeschel et al.,
2003).
We use interactive visual analysis (IVA) to ana-
lyze the data. IVA and the use of the data model sup-
porting families of curves represent a premium sup-
port tool for deep analysis, sense making and getting
insight into the data. Seeing all curves of a family
at once, seeing their aggregates and all other dimen-
sions allow experts to quickly propose a hypothesis
and check it. Our main goal is to see if there are some
hidden, still unknown indicators in the data which can
improve predictions. We investigated the effect of ab-
normal serum sodium concentrations, variability of
sodium concentration, and rapid changes in sodium
concentration on ICU mortality.
5.1 Serum Sodium Concentration:
Confirming an Hypothesis
The medical experts were novice users at the begin-
ning and we started the analysis process with a well
known case. The analysis at this stage provides famil-
Figure 7: a. + b. Patients with hypernatraemia are selected
using the maximum aggregate of na tsh curves. For each
curve the maximum is computed and it is depicted using
parallel coordinates. The values above 150mmol/L are se-
lected. c. + d. The histograms shows the mortality rate for
this case (in absolute and relative scale). e. In the summary
view it can be instantly seen that the selected subset has a
higher mortality rate (parameter idead at the bottom of the
view).
iarization and reassurance to the medical team mem-
bers of the technique of interactive visual analysis, be-
fore we embarked on more complex analysis.
Normal serum concentration is typically defined
as 136 − 145mmol/L. Hyponatraemia can be defined
as a state where the serum sodium level is below
130mmol/L, and hypernatraemia as a state where the
serum sodium level is above 150mmol/L. Our expec-
tation is that patients with at least one recorded hyper-
natraemia or hyponatraemia have a higher mortality
rate.
To depict hypernatraemia patients, we can use a
simple line brush (user draws a line in the curve view
and all curves crossing the line are brushed) to se-
lect curves having values above 150mmol/L, or we
can compute the maximum aggregate for each curve
and depict the maximum values using, for example,
parallel coordinates. A brush on an axis of paral-
lel coordinates will be used for selection in this case
(Figure 7a). After drawing the brush with the mouse,
the user can adjust the brush limits precisely using a
brush properties dialog (Figure 7b). This is impor-
tant in cases where we want to have an exact range of
brushed data.
The histogram in Figure 7c shows the mortality
rates, the surviving cases on the left and the dead
cases on the right. To be able to visually compare the
mortality rate of the selection, we use a relative scale
on the histogram (Figure 7d), which gives the bins of
the overall data the same height and scales the high-
lighted selection data accordingly. If we had brushed
at random, or to be more precise, if we had brushed
any subset of the data with no inherent relation to
mortality, we would expect the selected bins to be the
same height. That there are relatively more cases se-
lected in the dead subset, shows that there may be an
association between hypernatraemia and higher mor-
tality rate. The same relation can be noticed instantly
in the brush overview view. In exact numbers the
overall mortality rate is 326/1447 or 22, 5%, but in
INTERACTIVE VISUAL ANALYSIS OF INTENSIVE CARE UNIT DATA - Relationship between Serum Sodium
Concentration, its Rate of Change and Survival Outcome
655

Figure 8: Exploring variability - a. Parallel coordinates
with the minimum, the maximum, and Y −SPAN aggregates
are shown. b. High variation curves are select first (high
values for Y − SPAN, meaning a large difference between
minimum and maximum). c. The selection is refined by
excluding the patients having hypo- or hypernatremia. d.
The corresponding histogram shows that mortality is higher
in those cases than in general (right dark blue bin is higher
in the relative histogram - a histogram where each bin is of
the same height used to show the ratio of brushed and non-
brushed items in each bin). e. The original curves depicted.
These patients have a higher risk, although they do not have
hypo- or hypernatremia.
patients with hypernatraemia, the mortality rate was
91/331 or 27,5%.
To compare the mortality rate (and other values)
of patients with and without hypernatraemia we used
the inverse brush to invert the selection. It shows us
a mortality rate of 21,1% in patients without hyper-
natraemia. The admission parameters such as age,
APACHE II scores, baseline serum lactate concentra-
tion and baseline venous oxygen saturation were quite
similar.
Likewise, by placing the threshold brush at
130mmol/L, we calculated the mortality of patients
with at least one recorded measurement of hypona-
traemia to be 25,2%, compared to a mortality of
20,0% in patients without hyponatraemia. Again, this
is despite very similar admission parameters. Both
these findings are consistent with conclusions drawn
using conventional methods of analysis and were ex-
pected by medical experts.
5.2 Exploring Variability of Sodium
Concentration
It is time now for more complex analysis. We ob-
served that the sodium concentration curves (na
tsh)
varied greatly for some patients and we therefore
explored whether these fluctuations were associated
with mortality. To do so we computed the differ-
ence between the highest and the lowest concentra-
tion of serum sodium for each patient (i.e. the max-
imum value of the curve minus the minimum value
of the curve) and stored this as a new scalar variable
(na tsh Y − SPAN). Our data table has one additional
scalar column now.
We then used parallel coordinates (Figure 8a.) and
brushed records with the largest concentration-span
values (Figure 8b.) to compare mortality rates of pa-
tients with with high and low sodium concentration
variability.
To investigate whether high variability without
hyper- and hyponatraemia (both of course lead to high
sodium concentration variability) also increases mor-
tality we excluded patient with hypo- or hyperna-
tremia by using two subtract brushes in the parallel
coordinates view (Figure 8c.). We detect that some
patients indeed have high variability in sodium con-
centration despite never being hypo- or hypernatremic
at any time. The histogram in Figure 8d. shows the
relative mortality for those patients. It appears that
high variability in sodium concentration is associated
with mortality despite the absence of hypo- or hyper-
natremia.
5.3 Rate of Change in Serum Sodium
Concentration
A general principle in ICU fluid management is
to prevent hyper- and hyponatraemia, and to avoid
rapid changes in sodium concentration. Once
hyper- or hyponatremia is established, correction
of sodium concentration is not without risks. We
therefore investigated the effects of rapid correc-
tion of sodium concentration in patients with ab-
normal sodium concentrations. To explore the ef-
fect of rate of change we computed a new variable
(na tsh 1ST DERIVATIV E) which is the first deriva-
tive (i.e. slope of tangents) of the na tsh curve for
each patient (it is calculated by taking the difference
between two consecutive values of sodium concentra-
tion and dividing it by the time difference between the
two recordings). This is again a new column in our
dataset, a time series column where positive values
correspond to a rise in the sodium concentration and
negative values to a fall in the sodium concentration.
5.3.1 Hypernatraemia with Rapid Fall in Serum
Sodium Concentration
To select hypernatremic patients we used a curve view
showing the original na tsh data and a line brush
to select all patients with values above 150mmol/L.
Since we want to explore the cases which experience
IVAPP 2012 - International Conference on Information Visualization Theory and Applications
656
a rapid fall in sodium, we used a curve view show-
ing na tsh 1ST DERIVAT IV E. Using a line brush
we selected only curves which have values below
−3mmol/L/hour. The brushed data set showed a
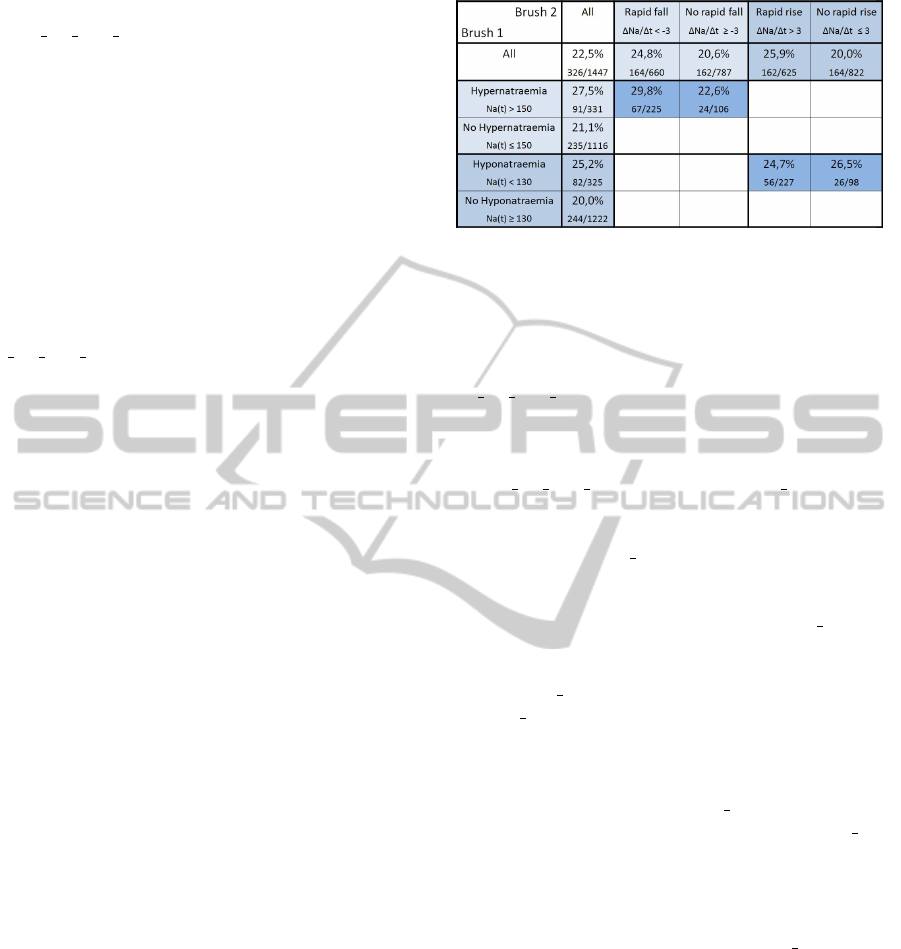
higher mortality rate of 29,8%. Interestingly, patients
with hypernatremia but without a rapid fall in sodium
concentration had a lower mortality rate (22,6%).
This suggests that hypernatraemia per se may not be
detrimental, but it may be the rapid correction that
leads to increased mortality.
That a rapid fall in sodium concentration of
over 3mmol/L/hour (regardless of hypernatraemia)
causes an increased mortality (24,8%) compared
to the mortality rate in those without (20,6%)
can be shown when applying only the brush on
na tsh 1ST DERIVATIV E.
5.3.2 Hyponatraemia with Rapid Rise in Serum
Sodium Concentration
We were also interested in the effect of a rapid in-
crease in sodium in hyponatremic patients. Using a
similar selection approach as in the previous section,
we found that a rapid rise in sodium concentration
(more than 3mmol/L/hour) is associated with a mor-
tality of 25, 9% compared to 20, 0%. In contrast to
the case with hypernatremia and rapid fall in sodium
concentration, this increased mortality with rapid rise
in sodium concentration is not pronounced in hy-
ponatraemic patients. We note that patients with a
sodium of under 130mmol/L and rise of sodium over
3mmol/L/hour have a mortality rate of 24,7% which
is quite similar (even a little lower) to patients with
hyponatraemia (25,2%), and also to patients with hy-
ponatramia and a sodium concentration rise of less
than 3mmol/L/hour(26,5%). These findings seem
to suggest that rapid rise in sodium concentration is
detrimental regardless of the concentration of sodium,
and that hyponatraemia itself is also detrimental re-
gardless of the rate of change of sodium concentra-
tion. The results are summarized in Figure 9.
5.3.3 Interactive Drill Down: A Detailed
Analysis
The next stage of analysis demonstrates the potential
of IVA to explore changes of sodium concentrations
in detail. Clinical research usually deals with popu-
lation aggregates, and time series data hereby is often
dealt by using aggregates. Interactive visual analysis
is a novel approach that medical experts are not ac-
customed to. However, the proposed data model and
the technology implemented here make it possible to
explore the data on a deeper level, as well as on the
individual patient level as on the time level.
Figure 9: The mortality rates in percent and absolute num-
bers for patients with hypernatraemia, hyponatraemia, rapid
rise and fall in sodium concentration along with interesting
combinations.
By simply making the line brush shorter on the
na tsh 1ST DERIVATIV E time series, we could eas-
ily select patients with a high rate of change in serum
sodium during specific periods of their stay at the
ICU. Figure 10 shows such an analysis. Curve views
for na tsh 1ST DERIVAT IV E and na tsh are de-
picted. Patients with a high rate of change at the be-
ginning of the ICU stay were selected (Figure 10a.).
It appears that the na tsh levels for all these patients
stabilized quite quickly after the initial fluctuations.
We note visually that some patients had high initial
values, and some had low initial values of na tsh, but
the individual curves are still not distinguishable. So
we refined the selection further by brushing a subset
with low na tsh values first, and then a subset with
high na tsh (Figures 10b. and c.). Note that there is
no patient which had low values and then high values,
or vice versa. This presents a reassuring indicator that
there was appropriate fluid management in these pa-
tients, leading to a normalized na tsh level.
Now we can examine a different set of na tsh
curves which had a rapid rise later in time. Fig-
ure 10d. and e. show these curves. Note the differ-
ence in curves shapes compared to the initial selec-
tion. Patients with a later rapid rise in serum sodium
had much higher oscillations in their na tsh curves
throughout their ICU stay. These oscillations may re-
flect an unstable clinical course associated with more
difficult fluid management or they may represent a
subgroup of patients with particularly organ dysfunc-
tions such as kidney failure. Further analysis and ex-
amination of other parameters would be necessary to
confirm and refute such a hypothesis.
Further investigation showed us that patients with
the highest rates of rise in sodium were those who also
suffered from severe hyponatraemia, which seemed to
suggest that rapid rises in sodium were mostly not pri-
mary problems, but reactions (either treatment or pa-
tient’s own relayed response) to low sodium concen-
INTERACTIVE VISUAL ANALYSIS OF INTENSIVE CARE UNIT DATA - Relationship between Serum Sodium
Concentration, its Rate of Change and Survival Outcome
657
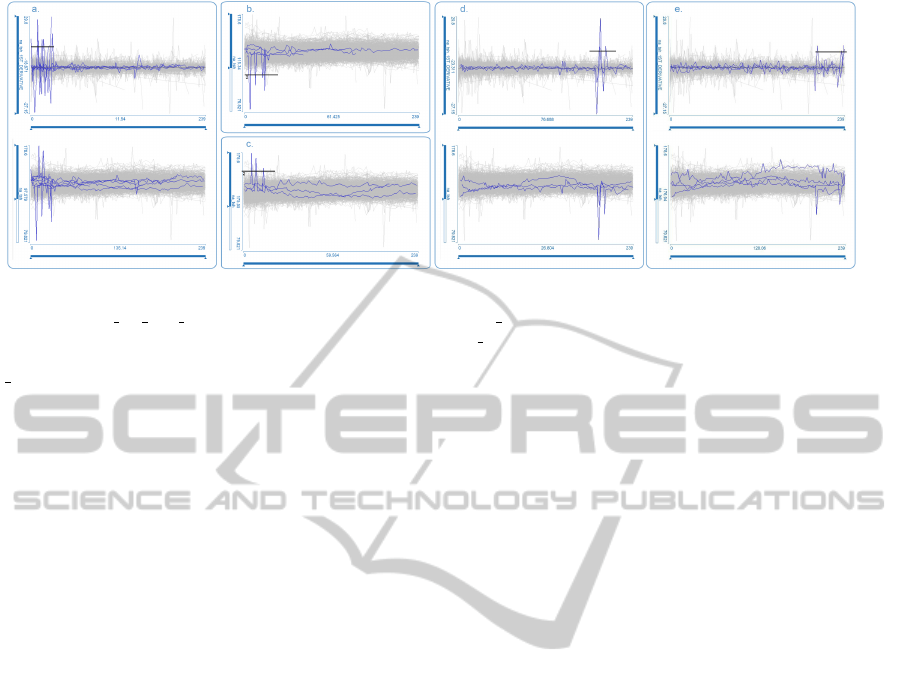
Figure 10: a. Patients which had a rapid rise in serum sodium concentration at the beginning of the ICU stay are selected by
a line brush in na tsh 1ST DERIVAT IV E (top); the corresponding na tsh curves (bottom) show patients with high and low
initial values b. and c. By applying an additional line brush at the na tsh curves we can verify that high and low initial values
correspond to different patients d. and e. Patients which had a rapid rise later in time are selected (top), the corresponding
na tsh curves (bottom) show higher oscillations.
trations. This can clearly be seen from the time series
views. Interestingly, the opposite seemed to be true
for the patients with the highest rates of fall in sodium.
The rapid falls were often the primary problem, not a
reaction to high sodium concentrations. Another ob-
servation from the drill down analysis was that pa-
tients with the lowest sodium concentrations have big-
ger oscillations on the 1st derivative time series graph
compared to patients with the highest sodium concen-
trations. These phenomen are consistent with above
described findings – hypernatraemia per se is proba-
bly well tolerated, but not rapid fall in sodium con-
centration, so patients with hypernatraemia may have
had their sodium corrected slowly. Conversely hy-
ponatraemia itself is probably harmful, so it may have
been corrected more rapidly, despite the risk of a rapid
rise in sodium concentration.
Drill down analyses as this would be very com-
plicated and almost impossible to perform using only
conventional statistical methods and aggregates. The
application of a complex data model with curves and
an interactive setup supports this discovery and explo-
ration process.
6 CONCLUSIONS
In this case study we demonstrated the usefulness of
interactive visual analysis (IVA) in analyzing a large
dataset of ICU data and helping the physicians to get
a fast and intuitive overview of the data, quickly test
hypotheses and identify relations which are worth fur-
ther examination. Furthermore, the interactive ex-
ploratory process helps domain experts to gain insight
during the analysis.
The main tasks for the interactive visualization ex-
pert reside, besides communicating the various exist-
ing visualization concepts and techniques to the do-
main experts, in providing a somehow sophisticated
data preprocessing, identifying the requirements of
the case and providing the following additional func-
tionality, tailored to the very case of application. In
our case we quickly came to the desired view config-
uration and we identified needs for improvements of
existing techniques – a curve view supporting time se-
ries with variable length and missing data, a box plot
view with multiple brushes, a summary view which
allows comparison of multiple brushes, and an easy
to use inverse brush, all fully integrated in the CMV
system.
The ICU data is a valuable source of information.
Understanding this data can contribute to improve-
ments in our comprehension of complex biological
and physiological systems, to refinement of models,
for risk prediction and monitoring at both individual
and systemic levels, and ultimately to improvement in
quality of care. We have here presented how complex,
longitudinal clinical data obtained from a routinely
used clinical information system can be explored by
means of interactive visual analysis. We applied a
complex data model which, in combination with in-
teraction and various coordinated views, supports an
in-depth visual analysis. Such an analysis would not
be possible using conventional data model and con-
ventional analysis tools.
This initial exploratory study produced several in-
teresting findings. We plan to further explore these
findings and to continue to use and improve the inter-
active visual analysis tool to facilitate the analyses of
complex clinical datasets. The feedback from domain
experts is very positive, and this study resulted in an
on-going collaboration. There are many aspects we
IVAPP 2012 - International Conference on Information Visualization Theory and Applications
658

have not tackled yet, and the amount of data available
represents a huge potential for future research, both,
in visualization and in the medical domain.
ACKNOWLEDGEMENTS
The authors thank St. Thomas Hospital for data and
Zoltan Konyha for converting the data first time. Part
of this work was done in the scope of the K1 program
at the VRVis Research Center (http://www.VRVis.at).
REFERENCES
Aigner, W., Miksch, S., M
¨
uller, W., Schumann, H., and
Tominski, C. (2007a). Visual methods for analyzing
time-oriented data. IEEE Transactions on Visualiza-
tion and Computer Graphics, pages 47–60.
Aigner, W., Miksch, S., M
¨
uller, W., Schumann, H., and
Tominski, C. (2007b). Visualizing time-oriented
data–A systematic view. Computers & Graphics,
31(3):401–409.
Aris, A., Shneiderman, B., Plaisant, C., Shmueli, G.,
and Jank, W. (2005). Representing unevenly-spaced
time series data for visualization and interactive ex-
ploration. Human-Computer Interaction-INTERACT
2005, pages 835–846.
Bade, R., Schlechtweg, S., and Miksch, S. (2004). Con-
necting time-oriented data and information to a co-
herent interactive visualization. In Proceedings of the
SIGCHI conference on Human factors in computing
systems, pages 105–112. ACM.
Gan, H., Matkovic, K., Ammer, A., Purgathofer, W., Ben-
nett, D., and Terblanche, M. (2011). Interactive visual
analysis of a large icu database: a novel approach to
data analysis. Critical Care, 15(Suppl 1):P135.
Gresh, D., Rabenhorst, D., Shabo, A., and Slavin, S. (2002).
Prima: A case study of using information visualiza-
tion techniques for patient record analysis. In Visual-
ization, 2002. VIS 2002. IEEE, pages 509–512. IEEE.
Hochheiser, H. and Shneiderman, B. (2002). Visual queries
for finding patterns in time series data. University of
Maryland, Computer Science Dept. Tech Report, CS-
TR-4365.
Hochheiser, H. and Shneiderman, B. (2004). Dynamic
query tools for time series data sets: timebox widgets
for interactive exploration. Information Visualization,
3(1):1–18.
Knaus, W., Wagner, D., Draper, E., Zimmerman, J.,
Bergner, M., Bastos, P., Sirio, C., Murphy, D.,
Lotring, T., and Damiano, A. (1991). The apache
iii prognostic system. risk prediction of hospital mor-
tality for critically ill hospitalized adults. Chest,
100(6):1619–36.
Knaus, W. A., Draper, E. A., Wagner, D. P., and Zimmer-
man, J. E. (1985). APACHE II: a severity of dis-
ease classification system. Critical care medicine,
13(10):818–829.
Konyha, Z., Matkovic, K., Gracanin, D., Jelovic, M., and
Hauser, H. (2006). Interactive visual analysis of fami-
lies of function graphs. IEEE Transactions on Visual-
ization and Computer Graphics, 12(6):1373.
Lindner, G., Funk, G.-C. C., Schwarz, C., Kneidinger, N.,
Kaider, A., Schneeweiss, B., Kramer, L., and Druml,
W. (2007). Hypernatremia in the critically ill is an in-
dependent risk factor for mortality. American journal
of kidney diseases : the official journal of the National
Kidney Foundation, 50(6):952–957.
McGill, R., Tukey, J. W., and Larsen, W. A. (1978). Vari-
ations of box plots. American Statistician, 32(1):12–
16.
Plaisant, C., Lam, S., Shneiderman, B., Smith, M., Rose-
man, D., Marchand, G., Gillam, M., Feied, C., Han-
dler, J., and Rappaport, H. (2008). Searching Elec-
tronic Health Records for temporal patterns in patient
histories: A case study with Microsoft Amalga. In
AMIA Annual Symposium Proceedings, volume 2008,
page 601. American Medical Informatics Association.
Plaisant, C., Milash, B., Rose, A., Widoff, S., and Shneider-
man, B. (1996). LifeLines: visualizing personal histo-
ries. In Proceedings of the SIGCHI conference on Hu-
man factors in computing systems: common ground,
pages 221–227. ACM.
Plaisant, C., Mushlin, R., Snyder, A., Li, J., Heller, D.,
and Shneiderman, B. (1998). LifeLines: using vi-
sualization to enhance navigation and analysis of pa-
tient records. In Proceedings of the AMIA Symposium,
page 76. American Medical Informatics Association.
Powsner, S. M. and Tufte, E. R. (1994). Graphical summary
of patient status. Lancet, 344(8919):386–389.
Roberts, J. (2007). State of the art: Coordinated & mul-
tiple views in exploratory visualization. In Coordi-
nated and Multiple Views in Exploratory Visualiza-
tion, 2007. CMV’07. Fifth International Conference
on, pages 61–71. IEEE.
Rocktaeschel, J., Morimatsu, H., Uchino, S., and Bellomo,
R. M. (2003). Unmeasured anions in critically ill pa-
tients: Can they predict mortality? Critical Care
Medicine, 31(8):2131–2136.
Shneiderman, B. (2002). The eyes have it: A task by data
type taxonomy for information visualizations. In Vi-
sual Languages, 1996. Proceedings., IEEE Sympo-
sium on, pages 336–343. IEEE.
Trobec, R., Matkovic, K., Skala, K., Depolli, M., and Av-
belj, V. (2008). Visual Analysis of Heart Reinervation
after Transplantation. In Proceedings of the MIPRO
2008.
Tukey, J. W. (1977). Exploratory data analysis. Addison
Wesley.
Wang, T., Plaisant, C., Quinn, A., Stanchak, R., Murphy, S.,
and Shneiderman, B. (2008). Aligning temporal data
by sentinel events: discovering patterns in electronic
health records. In Proceeding of the twenty-sixth an-
nual SIGCHI conference on Human factors in com-
puting systems, pages 457–466. ACM.
INTERACTIVE VISUAL ANALYSIS OF INTENSIVE CARE UNIT DATA - Relationship between Serum Sodium
Concentration, its Rate of Change and Survival Outcome
659
