
Health@Home Scenario: Creating a New Support
System for Home Telerehabilitation
Ant
´
onio Teixeira, Carlos Pereira, Miguel Oliveira e Silva, Nuno Almeida,
Joaquim Sousa Pinto, Cl
´
audio Teixeira, Fl
´
avio Ferreira and Andr
´
e Mota
DETI/IEETA, University of Aveiro, Campus Universit
´
ario de Santiago, Aveiro, Portugal
Abstract. The creation of innovative methods and technologies for elderly is the
main purpose for Ambient Assisted Living. This paper provides a description on
all the associated stages and development questions required for the establish-
ment of a new telerehabilitation service. The service intends to provide elderly
people with the possibility of performing rehabilitation sessions in their houses,
with constant medical supervision via video surveillance. Following the princi-
ples of a new conceptual architecture for services, and developed according to
user-centric paradigms such as multimodality and high usability criteria, early
evaluation results point the service as an asset for remote rehabilitation.
1 Introduction
The enhancement of domestic environments with technology is nowadays a reality.
Technology creates a positive impact on quality of life especially on older generations
since technological solutions can facilitate the daily life of the elderly, by fighting iso-
lation and exclusion, and by increasing their pro-activity and autonomy.
The Living Usability Lab (LUL [1]) project is a collaborative effort for R&D be-
tween academia (University of Aveiro/IEETA and FEUP/INESC Porto) and portuguese
industry (Microsoft, Micro IO and Plux). Fueled by technologies such as distributed
computing, next generation networks, natural interfaces and universal design while fo-
cused on usability rates, the project aims at having impact at general population, espe-
cially on elder and special need citizens, by envisioning the creation of a Living Lab
capable of providing support for the creation of innovative applications, services and
technologies for them.
To enable the existence of a geographically distributed lab for new AAL services
creation, evolution and evaluation - our Living Lab -, suitable architectures for the Liv-
ing Lab and its middleware - supporting creation and deployment of new services - were
needed. To conduct research and test associated ideas, a number of scenarios based on
real necessities were conceptualized.
This paper presents the associated research and development for Health@Home.
The Health@Home scenario envisions the creation of a home telerehabilitation ses-
sion with remote medical supervision. Telerehabilitation has been introduced in several
fields, from neuropsychology to occupational therapy and physical therapy. It allows
Teixeira A., Pereira C., Oliveira e Silva M., Almeida N., Sousa Pinto J., Teixeira C., Ferreira F. and Mota A..
Health@Home Scenario: Creating a New Support System for Home Telerehabilitation.
DOI: 10.5220/0003879000370047
In Proceedings of the 2nd International Living Usability Lab Workshop on AAL Latest Solutions, Trends and Applications (AAL-2012), pages 37-47
ISBN: 978-989-8425-93-5
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)
for remote populations to improve their quality of life by decreasing the constant need
to travel to the healthcare centers while permitting for health professionals to be more
aware of their patients by facilitating their interaction [8]. At a technical level, a tel-
erehabilitation service poses many demands being a distributed application with a high
focus on components such as video, speech, user modeling, environment properties and
real-time communication [7].
To provide support for such components, an infrastructure was built in addition
to a conceptual architecture for service provisioning. These became the basis for the
telerehabilitation application which was later developed and evaluated. Also, given the
special necessities of AAL applications, a variety of services were also introduced to
fasten development.
This paper is structured as follows. In Section 2, we provide an overview on the
conceptual architecture followed by LUL. In Section 3 we describe the infrastructural
definitions required for the completion of the Health@Home scenario. Section 4 gives
insight into specific services that were required for the scenario. Section 5 provides
an overview on the telerehabilitation applications. In Section 6 we provide some early
evaluation results and point out future work possibilities.
2 Conceptual Architecture
The Service Oriented Architecture created on the scope of LUL adopts a less centered
view allowing for important gains in both modularity and availability. The choice for
a service oriented approach derives from its ability to achieve loose-coupling abilities
without much effort. All together, our intention was to provide developers with better
conditions to be able to create innovative AAL applications and services using the pro-
posed architecture as a basis and have at their disposition a number of services that may
assist them in creating their intended business logic.
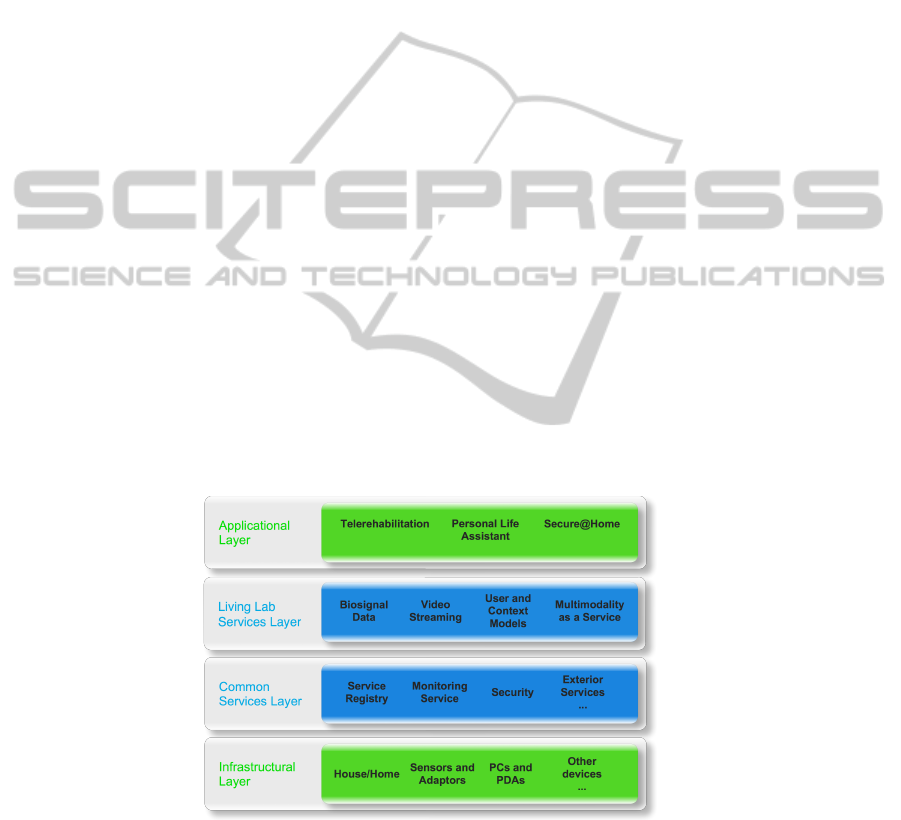
Fig. 1. Conceptual Ambient Assisted Living architecture for LUL.
38

Infrastructural Layer. The architecture is composed by four main layers as seen in
Figure 1. AAL applications often use devices such as sensors, adapters, mobile devices,
desktop computers, among others. These kind of devices represent the Infrastructural
Layer. Given that devices may be added or removed from the system dynamically, we
impose that devices included in this layer must be made accessible via Web Services,
to be encapsulated and accessed from a service level layer. For this, devices should
be introduced via a “Device as a Service” paradigm [2], which allows devices to be
accessible via a well defined interface.
Common Services Layer. The Common Services Layer is responsible for providing
services such as access between nodes, monitoring, security and user management. We
intended for services in this layer to include third-party services which may be needed
by certain applications. In order to facilitate the location of certain business logics, we
established that any service within the architecture must advertise itself in the service
registry. Technologically, the registry, running at a central server accessible to all nodes,
functions like a WSDL [9] repository.
Living Lab Services Layer. The Living Lab Services layer aims to involve all pos-
sible services that may arise, either from the implementation of certain devices, (for
instances, a video capture service), either from the development of new services (like
a sensor service), or either from the inclusion of already existing exterior services (a
monitoring service) that may be needed in the development of certain applications. To
comply with the user-centric paradigm associated to the project, it is expected that built
applications follow user-friendly and user-adaptable paradigms. To help them, this layer
includes services like context and user modeling providing applications with means to
better know the end user and achieve user adaptation.
Applicational Layer. In the top layer, the architecture includes an Applicational layer
where developed applications should be “placed”. An important requirement that ex-
isting SOA proposals didn’t meet was the inclusion of multimodal capabilities. In our
view, to establish maximum usability, multimodality must be also included. The telere-
habilitation application which will be later explained is one such example.
3 Infrastructure
In the conceptual architecture, a layer of services was established exclusively focused
on integrating specialized services to be developed as part of the LUL project - Liv-
ing Lab Service Layer. These services require a physical location where they can be
deployed. In this sense, two options came up: to use a central server accessible by all
project nodes (scalable to a large increase in a more realistic AAL scenario) or to use
a smaller home based server. We selected a subset from both due to the differences in
the envisioned services. While some are generic and must be made available at a well
known address, others are more “house oriented”.
Our option for LUL is divided into two parts, to have a central server (named LUL
server) where generic services can be deployed and published being complemented by
39

at least a small server at each house (designated as home server). This separation en-
ables local concerns to be treated only in the home server simplifying communications
between both servers, increasing their modularity.
Due to the heterogeneity inherent to Living Lab, it was established that Next Gen-
eration Networks (NGN) would be adopted into the infrastructure given its open in-
terfaces support to a wide range of services, applications, and mechanisms based on
service building blocks. For communication and in order to assure high interoperabil-
ity and integration rates, all communications within the proposed architecture use the
Internet Protocol, both UDP (for RTP [5] transmissions) and TCP.
To provide support for the rehabilitation applications, additional devices such as a
pan and tilt camera as well as a sensor from Plux [4] capable of obtaining measures
from several electrodes on the patient and communicating them to an application via
Bluetooth, were introduced.
4 Support Services
In order to help developers create new applications associated with the objectives of
LUL, a set of services were made available so that they can rapidly integrate business
logics in their applications without much effort. These services were deployed within
the Living Lab infrastructure and their interfaces made available on the service registry.
An important aspect common to all deployed services is tolerance to failures. Services
cannot be fully dependent on others and not continue to function in case of a depen-
dency issue.
4.1 Application Registry
Many new AAL applications will need to created following a distributed logic (i.e., ap-
plications divided in a number of locations but in constant communication). Because of
the critical aspects associated with some of these applications it is necessary to ensure
that connectivity is not lost, and in such a case, automatically restore it as soon as pos-
sible. As such, and to accomplish a highly dynamic distributed architecture, a specific
service must be provided to applications allowing them to easily find, connect and know
the current status of others.
Due to these issues, a service for Application Registration was implemented and
deployed in the LUL server. The service is similar to a broker. Applications must reg-
ister themselves at the startup on the registry and also inform the registry of any status
change. With this information, client applications obtain the necessary information to
connect and to regain connectivity taking in consideration the status of its partners. In
case of a failure, the service will help in the reestablishment of the communication in
an easier and faster manner.
Fault Tolerance. The application registry service as presented provides a solution for
connectivity losses. But to achieve a truly fault tolerance environment, the effort must
be extended to the applications as well. Applications need to able to continue to operate
in cases where services that they require become unavailable. They must be able to
40

self-adapt to current conditions, which may implicate simply to cease a functionality or
even shutdown graciously.
To obtain this, we’ve established a set of rules to be performed within the architec-
ture, with a special focus on the application registry as its core:
1. Applications notifies the broker for which services should they be alerted in case of
failures. The broker stores this information in a registry.
2. The broker isn’t 100% fail proof. As such, applications need to frequently “ping”
the broker to know that it remains fully functional. In case it fails, applications must
possess safeguards so they can maintain their autonomous execution.
3. The broker needs to guarantee that all services within the system are functional. To
do this, the broker performs pooling routines on the services.
4. Based on the registry, the broker notifies all interested parties in case of a service
failure. These must be able to adopt mechanisms to guarantee their functioning. It
will be the broker’s responsibility to try and regain connectivity with the service
alerting the interested parties when it occurs.
With this set of rules adding to the application registry, services and applications
achieve better fault tolerance rates. Connections to the broker however are critical to-
wards the functionality and robustness of the overall system. To minimize effects of
possible broker failure, redundancy must be applied to the broker itself.
4.2 Video Streaming and Camera Control Service
Many potential AAL applications make use of video for surveillance and detection of
events or simply for communication. Additionally, it is also often important to allow
remote real-time control of the camera, enabling the retrieval of images on a moving
subject.
The video service is based on a producer-consumer approach. The service handles
all connections/sessions and video is transmitted using RTP. After the session is estab-
lished, the client can also use service functionalities directly regarding camera control,
such as pan, tilt and zoom.
4.3 Service for Actuators and Sensors
Information from sensors and control actuators are fundamental aspects for a typical
AAL application. Usually this information is used by the application’s own business
logic to infer with conditions relating with the user. In the developed service, all sensors
and actuators are available through web services based on a “Device as a Service”
paradigm.
The Figure 2 represents how the service was deployed and subsequently used by
a remote client application. Each generic sensor service has an interface, monitoring
capabilities and a set of devices.
41
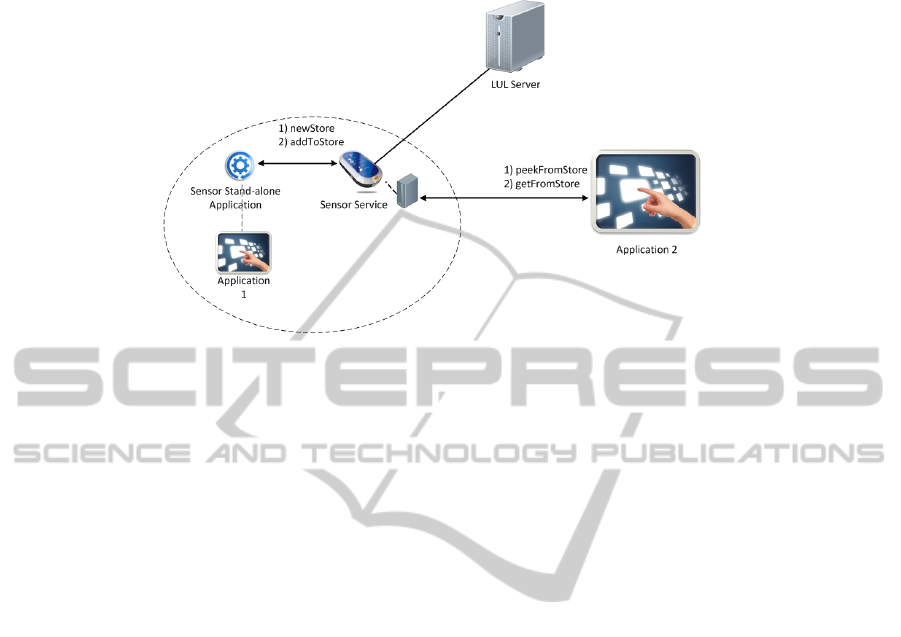
Fig. 2. Conceptual view of Sensor and Actuator Service.
4.4 Multimodal Support Service
Multimodality represents an important aspect in the Living Lab ideals since it can be
used as a paradigm for achieving higher rates of usability and accessibility [3]. Cur-
rently, and in order to facilitate the integration of multimodal logics within applications,
a multimodal service is in development. This service will allow for complex algorithms
such as fusion and fission to be accessible via a web service.
Fusion will be made available to clients by requesting that initially applications
invoke the service so that a specific instance is created for them. Communication is
established between the created instance and the application. Then, by providing a con-
figuration file where it declares all possible input options, the service will wait for events
which it can fuse.
Fission on the other hand requires information of all available output modalities
which includes knowing their characteristics and current availability. With it, and in-
spired by a algorithm called Adapto [6], it uses context data such as distance to a screen
or the user’s hearing capabilities, to decide on what modalities should be used or which
are indicated at the time.
An important aspect regarding the multimodal service is its almost full local auton-
omy capability. The service uses local information for its processing with the exception
of user aspects and characteristics which are centralized. This becomes important in the
sense that communications between the server and the application are reduced resulting
in increased responsiveness on the interaction.
5 Telerehabilitation Application
A telerehabilitation application allows for the execution of rehabilitation services to re-
mote and underserved populations, improving quality of life and preventing secondary
complications. With such a service, the need and frequency of the patient having to
42
travel to the healthcare centers is decreased allowing medical staff to not only interact
with patients on a more regular basis but also be able to stay in touch with them after
discharge [8].
5.1 Requirements
The first step on constructing the application was to be able to specify what its require-
ments were. Given the goal of a telerehabilitation system, the first requirement is that
the system must be used simultaneously at two different and possibly distant places:
one being the health professional current location, the other the elder home.
The second requirement is related to operating services. In a telerehabilitation ses-
sion, information like sensor data, video and feedback communication become critical
to a health professional for successful monitorization. In addition, exercise information,
instructions and user adaptation are indispensable on a patients perspective.
Most of these requirements are already answered by the development architecture,
particularly the Living Lab service layer. As such, development focused on the human-
computer interfaces in the applications. Given the different logics associated with the
two participants, the need for the two different interfaces became apparent - one for the
patient and another for the health professional.
5.2 Multiple Patient Sessions
Ideally, in order to provide maximum attention to a patient, medical supervision should
be focused on a single patient at a time. This however can only be applied in theory.
In practice, it becomes impossible to devise constant rehabilitation sessions following
a one to one basis since sessions can consume considerable time and the number of
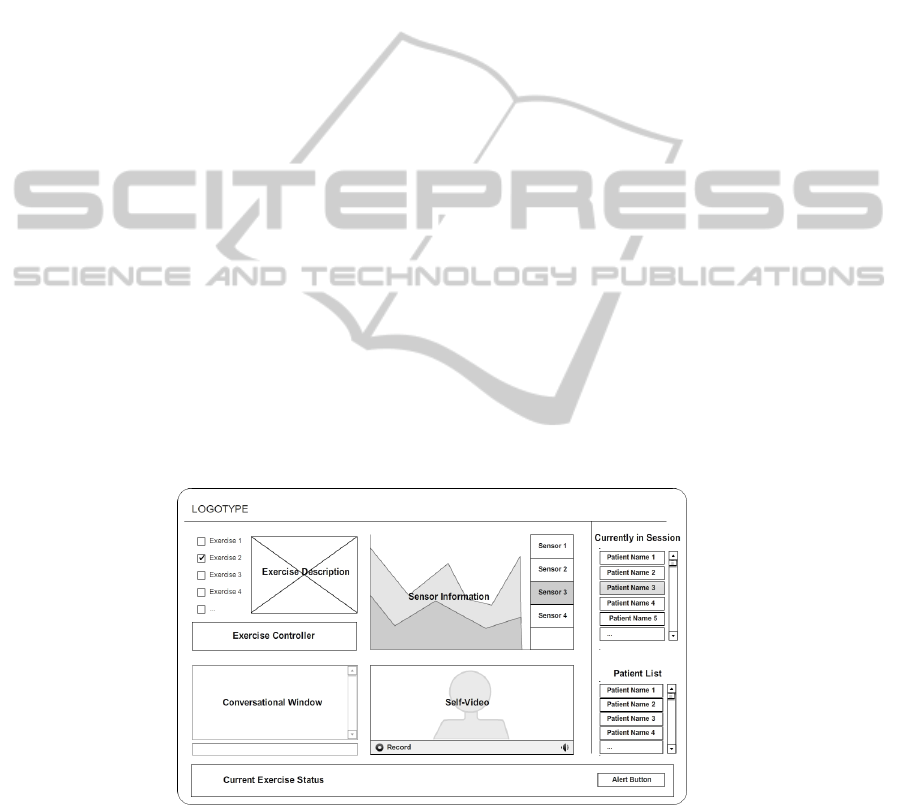
patients are vastly superior to the number of available supervisors. Figure 3 presents a
mockup screen for the health professional application ideals.
Fig. 3. Conceptual screen on a multi-patient application for the health professional.
We’ve established a need to built the applications following a set of properties that
allows for two very specific functionalities to be achieved. First, each professional ap-
43

plication must be able to connect to several patient applications concurrently, that is, the
supervisor should be able to perform several sessions simultaneously, shifting his atten-
tion to one in specific for a particular reason (right bar on Figure 3). In truth, depending
on the type of rehabilitation session, some times the full attention of a supervisor is
simply not required. Second, in such cases, what is required is a “safeguard” mecha-
nism, that is, a method that alerts the supervisor in case of need. When an event such
as this happens, the medical application simply needs to shift its attention to the proper
one (alert button on Figure 3). Additionally, Adapto may be used to maximize the alert
notification (by using several interaction modalities).
At this time, current implementation doesn’t yet fully reflect these characteristics,
but they will be considered for future scenarios.
5.3 Health Professional Application
The health professional application has the goal of providing information regarding an
ongoing rehabilitation session while allowing for feedback to be given if necessary. As
such, the developed application allows the health professional to:
– remotely monitor the elderly using video and biosensors information.
– plan, apply and control an exercise program.
– provide the elderly with feedback regarding their performance
Fig. 4. Health Professional Application Interface.
The interface shown in Figure 4 responds to these necessities by being composed by
five components. The first component, session planning (number 1 in Figure 4), allows
the health professional to monitor the exercise session by choosing the exercises to be
performed.
In the second component (marked with number 2 in the figure), sensor information
is provided to the health professional so that he can visualize and analyze biological
data such as heart rate throughout the session.
44

In component three, the health professional can communicate and provide feedback
to the patient via textual messages. The video component, four in the figure, is an im-
portant tool for monitoring a session, as it enables the health professional to visualize
the performance of the user and check the completion of the exercises, allowing him to
correct errors and give different indications to the patient.
Finally, in component five, the professional is allowed to track an ongoing session,
such as details about the connection and the status of the current exercise.
5.4 Patient Application
Creating an application for elders is more demanding due to certain limitations as-
sociated with them. Their average expected physical limitations, different capabilities
(hearing and vision acuity, for example), context conditions (such as light and noise
levels, or distance from the devices), and even the freedom of movements intrinsic to
physiotherapy must all be taken into account.
With such aspects in mind, the main user interface was deployed into a large size
computer monitor (acting as a large size TV) given the need for exercises to be executed
a couple of meters away from the screen. A set of biosensors were introduced to provide
the health professional with additional information and input and output devices such
as microphones, speakers and video cameras, required for the interaction between the
users and the platform, and sensors to detect environment factors were included.
Fig. 5. Patient Application Interface
Figure 5 demonstrates the overall aspect of the patient’s application. The user inter-
face of the application is composed by seven visual components, which can be divided
into three blocks:
– A monitoring block placed on top corresponding to components 1, 2 and 3;
– A reception information block, placed in between. It is composed by components
4 and 5;
– And a user input block, at the bottom, constituted by components 6 and 7.
45

The monitoring block presents a summary of the current session’s state. Its goal is
to provide information to the user of what is happening by including the description of
the session state (indication of whether a session with the professional is in progress or
not), time and date given by component 1; a logging area describing the latest actions
taken by the health professional and the elder (component 2); and showing a list of
exercises planned for the current session, highlighting the current one (component 3).
The reception information block shows all information provided from the health
professional or from the service to the elder. This includes two components: an animated
presentation illustrating the current exercise (component 4) and video screening of the
user, allowing the patient to view in real-time his/her current performance and perform
self-correcting aspects on the exercises (component 5).
Finally, the user input block presents some interaction options for the patient by
providing a conversation area (component 6), where the user can directly communicate
with the health professional via messages; and a command list area (component 7)
where the user can issue commands to the system.
6 Early Evaluation Results and Future Work
The new service was recently tested in a simulated environment by a small set of end
users in order to assess their acceptance rates and gain feedback for future improve-
ments. Evaluation aimed aspects such as the subjects’ participation, activities pace, use
of resources and identification of missing functionalities. Data collection on these sub-
jects was achieved by recording critical incidents (in loco) and, at the end of the session,
by answering a questionnaire (post-evaluation). The service assessment questionnaire
assesses: graphical user interface (layout), usability and satisfaction.
Participants were satisfied with their session, mainly due to the fact of having suc-
ceeded in accomplishing the indications of the physiotherapist and feeling comfortable
using the service. Participants reported being receptive to the use of such a service at
home. Some improvements were suggested by the introduction of speech capabilities
and minor adjustments to the interface (especially when away from screen).
In the next iterations for the service, we intend to give answer to these aspects and
provide new features and adaptability capabilities by introducing already underdevel-
opment services such as user and context modules and new multimodal paradigms. We
expect for the next iteration of the service to be fully tested with real users in a real
environment (either in an elderly institution or a hospital) for a longer period of time.
Additionally, we also envision further tests being performed to the support architecture
by the creation of other scenarios within the Living Lab scope.
References
1. Microsoft Corporation, Universidade de Aveiro, IEETA, FEUP, INESCPorto, MicroIO, Plux,
and Assoc. Salvador. Living usability lab. http://www.livinglab.pt/.
2. Scott de Deugd, Randy Carroll, Kevin Kelly, Bill Millett, and Jeffrey Ricker. SODA: Service
oriented device architecture. IEEE Pervasive Computing, 5(3):94–96, c3, July 2006.
46

3. Bruno Dumas, Denis Lalanne, and Sharon Oviatt. Human machine interaction. chapter Mul-
timodal Interfaces: A Survey of Principles, Models and Frameworks, pages 3–26. Springer-
Verlag, Berlin, Heidelberg, 2009.
4. Plux. Plux wireless biosignals. http://www.plux.info/, 2011.
5. The Internet Society. Rtp: A transport protocol for real-time applications. http://www.ietf.org/
rfc/rfc1889.txt, 1996.
6. A. Teixeira, C. Pereira, M. Oliveira e Silva, O. Pacheco, A. Neves, and J. Casimiro. Adapto.
adaptive multimodal output. In Proceddings of the International Conference on Pervasive and
Embedded Computing and Communication Systems (PECCS) 2011, 2011.
7. Ant
´
onio Teixeira, Nelson Rocha, Carlos Pereira, Jorge Sousa Pinto, et al. The living usabil-
ity lab architecture: Support for the development and evaluation of new aal services for the
elderly. In Ambient Assisted Living Book. Taylor and Francis, 2011.
8. Deborah G. Theodoros. Telerehabilitation for service delivery in speech-language pathology.
Journal of Telemedicine and Telecare, 14(5):221–224, July 2008.
9. W3C. Web services description language (wsdl). http://www.w3.org/TR/wsdl, 2001.
47
