
IMPACT OF SEMANTIC TECHNOLOGIES TO HUMAN BEHAVIOR
MODELING
A Psychosocial Rationalization
Ana Bel
´
en Sanchez-Calz
´
on, Carlos Fern
´
andez-Llatas, Flavio Pileggi and Teresa Meneu
ITACA-TSB, Universidad Polit
´
ecnica de Valencia, Valencia, Spain
Keywords:
Semantic interoperability, Human behavior, Healthy habits, Psychology.
Abstract:
The promotion of healthy habits have lots of benefits. In this way, the discovery of human health habits will
allow to experts, among others advantages, evaluate the accuracy of the promotion models. Nevertheless,
to design and develop a model that correctly predict and anticipate the behavior of an individual or a group
is a difficult task, in the sense that the challenge of representing the behavior includes such diverse areas as
simulating the effects of making decision, modeling the cognitive processes that take place in making that
decision, or simulate the perception of motor skills. The design of an unified method to access the current
human behavior theories will facilitate the application of motivation technologies in an holistic way.
In this paper, a review about the factors involved on human behavior modeling, and the most important theories
on people health behavior is made and a first attempt for the creation of a unified health behavior model is
presented.
1 INTRODUCTION
The discovery of the human behavior is one of the
hardest current challenges in multiple research fields.
The difficulties that scientist find in their way are not
only the problem of detect what are the rules and fac-
tors that affects to human behavior, but also how that
knowledge can be represented.
The model of human behavior has been treated
from psychological and psychosocial research fields
from lots of years ago (Hochbaum, 1958), (Lewin,
1943). One of the fields where the human behavior
discovery has more applications is the healthy habits
promotion. The promotion of healthy habits have lots
of benefits, not only in the health of individuals of cur-
rent society, but also in economical situation, cause
the large account of money that could be saved in
treatments for illnesses directly related with the un-
healthy habits of people. For that, the governments
year by year, apply an important part of their budget in
healthy habits promotion. Nevertheless, despite these
waste of money it is very difficult to know what is the
exact impact of their promotion activities.
In literature, some emerging technologies in the
automatic human behavior modeling based on in the
pattern recognition research field could be used to test
the capabilities of health promotion techniques ap-
plied by governments and health professionals. Com-
plex Event Processing (Wasserkrug et al., 2008) tech-
niques allows process events and discover complex
patterns among multiple streams of event data; Plan
recognition Models (Phua et al., 2009) allows the
alignment of habits of individuals to detect unhealthy
situations and evaluate the compliance to promotion
campaigns. Process Mining (A. K. A., Workflow
Mining) (Fern
´
andez-Llatas et al., 2009) techniques al-
lows detecting changes in the behavior of individuals
or people as a whole detecting if the promotion cam-
paigns has enough impact over their.
Nevertheless the huge amount of factors and dif-
ferent theories make difficult to these techniques to
focalize what are the factors to be taken in to ac-
count. Although the different psychological and psy-
chosocial research lines seem to be theorically com-
plementaries it is needed an effort to create a com-
mon framework to condense the psychological theo-
ries. The use of ontologies to describe de concepts
and to provide an mechanism to semantically interop-
erate among them.
In this paper, a review about the factors involved
on human behavior modeling, and the most important
theories on people health behavior is made and a first
attempt for the creation of a unified health behavior
model is presented.
547
Belén Sanchez-Calzon A., Fernández-Llatas C., Pileggi F. and Meneu T..
IMPACT OF SEMANTIC TECHNOLOGIES TO HUMAN BEHAVIOR MODELING - A Psychosocial Rationalization.
DOI: 10.5220/0003886705470552
In Proceedings of the 4th International Conference on Agents and Artificial Intelligence (IWSI-2012), pages 547-552
ISBN: 978-989-8425-95-9
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

2 PSYCHOSOCIAL THEORIES IN
HUMAN BEHAVIOR
MODELING
Based on the human behavior factors previously de-
scribed the scientific community has implemented
some theories in order to explain in what way these
factors affects to human behavior in their Health mo-
tivation. The most important theories are the Health
Belief Model, the Theory of Reasoned Action, the So-
cial Action Theory and Self-Efficacy Theory
2.1 Health Belief Model
This theoretical development was first formulated by
Hochbaum (Hochbaum, 1958), and subsequently ex-
tended by Rosentock (Rosenstock, 1974) applied to
the explanation and prediction of a wide range of
health behaviors. The proposal is the explanation
of behavior by focusing on psychosocial variables,
from a body of psychological theories such as Field
Theory by Lewin (Lewin, 1943) (Lewin, 1946), Ex-
pected Value Theory, and the Theories of Decision
making Under Uncertainty. The initial hypothesis of
this model is in the following way: an individual does
not perform a healthy behavior if she dont have min-
imum levels of relevant motivation and information
to health, she sees herself as potentially vulnerable,
and she sees the disease (or risk) as threatening, she is
convinced of the effectiveness of the intervention, and
find little difficulty in the practical action of healthy
behavior (Rosenstock, 1974)).
In the first place, according to the Health Belief
Model, the probability of making a healthy behavior
depends on the subjective state of intention of the in-
dividual to do so. The intention is determined by the
threat of the disease in question (according to the be-
lief of the individual). The perceived threat is deter-
mined by: the perceived susceptibility for the disease,
perceived severity of the consequences of suffering
this disease, and keys to trigger action to an appropri-
ate health behavior. These keys may come from inter-
nal sources (symptoms etc.) or external (interactions
with other, media etc.) (Becker and Maiman, 1982).
Secondly, the probability that an individual devel-
ops and maintains a healthy behavior depends on an
assessment that makes such behavior in terms of prac-
ticability and effectiveness, countered with the per-
ceptions of the physical, economic costs and other
barriers involved in the proposed action. These per-
ceived costs have been assessed in different ways in
different studies: in terms of security on the effective-
ness of the treatment prescribed, the patient satisfac-
tion about the communication with the doctor, patient
satisfaction about matters such as the way in which
the health organization provides medical care, etc.
Third, the threat perception triggered by some key
event starting the process of making healthy behav-
ior. Health Belief Model is based on the premise that
socio-demographic, structural and individual factors
may influence health behaviors. However, it consid-
ered that these variables act through their effects on
individual health beliefs, and not so direct causes of
wholesome actions (Becker and Maiman, 1982).
Most explanatory research on the effectiveness of
Health Belief Model are retrospective and it isnt pos-
sible to determine, from them, if the health belief
existed before or it was created after the conclusion
of the studied behavior. Its an appropriate model as
an explanatory model of preventive behavior, and an
inappropriate model to explain behaviors oriented to
health promotion.
2.2 Theory of Reasoned Action
Fishbein (M. and Ajzen, 1975) developed the The-
ory of Reasoned Action, and then further developed in
the Theory of Planned Action (Ajzen, 1987) (Ajzen,
1988), which attempts to explain the behaviors that
are under conscious control of individuals from differ-
ent determinants that precede and explain them. For
the authors, the immediate determinant of behavior is
not the attitude itself, but the intention to do. In turn,
behavioral intention has two forerunners that explain
it: a single precursor, that is, the attitude about the be-
havior, and another social and collective that refers to
the socio-cultural context of the individual, named as
the subjective norm (M. and Ajzen, 1975). Both atti-
tude and subjective norm are determined by other fac-
tors that precede them, helping to better understand
the behavior. As regards the attitude, it is determined
by each of the beliefs that person has to an object and
the assessment based on those beliefs. This assess-
ment represents the affective component of attitude,
determining the motivation and the strength of behav-
ioral intention.
According to this theoretical construct, beliefs
vary according to their origin, and can be formed from
different processes:
• Direct experience regarding the attitude object,
through which information is collected on the
characteristics of the object (a person, thing etc.).
The attitudes formed from this process have
greater strength and they are more resistant to
change.
• Indirect experience regarding the attitude object,
which brings the same features of that object by
the similitude to other objects with which it has
ICAART 2012 - International Conference on Agents and Artificial Intelligence
548

had previous direct experience. Such beliefs are
called inferential.
• The information collected from other (media,
family, friends, etc.). Information is accepted as
real, unless it contradicts the beliefs formed from
the direct or indirect experience (M. and Ajzen,
1975).
Regarding to the subjective norm, it has deter-
mined by the perception of the beliefs that others have
about the conduct that the individual must perform
and, moreover, it is also determined by the individ-
ual’s motivation to meet the expectations that others
have about her. Its a differential process of beliefs
formation that contributes to each of the beliefs have a
particular weight and value according to each individ-
ual and the attitude object. Outstanding attitudes, to-
gether with their evaluation, will better predict the be-
havior intention (M. and Ajzen, 1975). Furthermore,
knowledge about the specific beliefs of what others
persons think of each of the specific behaviors (for
example smoking, physical exercise, healthy eating,
etc.) will Influence the intention to carry out or not
a general behavior (maintaining a healthy lifestyle),
depending on the motivation to please.
However, not all behaviors are consciously con-
trolled by the individual, because there are many situ-
ations in which contingency may occur, or in which it
requires skills or resources that could interfere with
the intention of performing a behavior. Its neces-
sary a third determinant of behavioral intention, the
perceived control (Ajzen, 1987) (Ajzen, 1988)). Al-
though the individual has a favorable attitude toward
a behavior, the probability of carrying it out will de-
pend on, among other factors, the perception of con-
trol by the individual about her behavior. A person
may have a favorable attitude toward health care, for
instance to give up smoking, but if that individual per-
ceives that she has low ability to control and to quit
smoking, either because she considers she hasnt ca-
pacity enough, or because she believes that behav-
ior of other people can interfere with her decision to
quit, this healthy behavior will not be performed. The
perception of control is a factor consisting of inter-
nal variables (perceived ability, skill of action etc.),
and external variables (opportunity to action, obsta-
cles, time, cooperation, etc.). This is a determinant
that helps to improve forecasting and modeling of the
behavior (Ajzen, 1987).
The Theory of Reasoned Action doesnt take into
account factors such as attitudes towards goals, per-
sonality characteristics, sociodemographic variables,
social role, etc. For this model, these factors are exter-
nal variables that can influence behavior, but no nec-
essary relationship between them.
2.3 The Social Action Theory
This model proposed by Ewart (Ewart, 1991) presents
the individual as a self-regulatory system that actively
trying to achieve goals, and also as a feedback sys-
tem consisting of a set of serially arranged elements,
or stages: a first input stage, which represents stimu-
lus field and sets the targets. A second output stage,
or production of response, which provides the plans,
the selection and development of responses. And a
third stage of supervision that involves the consider-
ation of the consequences of action in relation to the
initial set of objectives. This model stresses the role
of social context in the development and maintenance
of healthy routines and habits; it provides the causal
structure linking the self-change processes in inter-
personal environments; and it also specifies the social
and environmental influences that make possible per-
sonal change.
According to Social Action Theory, preventive in-
terventions involve the creation of protective habits in
the form of routines behavioral sequences that reduce
personal risk. The actions are guided by their conse-
quences in a control loop, and variations in the results
produce compensatory behavioral adjustments. The
result is a steady state-action, but constantly fluctu-
ating. The starting point for intervention is an anal-
ysis of the relations between the harmful or benefi-
cial behaviors to health and its effects experienced.
This is an analysis that allows extracting those as-
pects in which behaviors are more accessible to pre-
vention, and it also allows extracting effective pro-
cedures for the design of new schemes that promote
health (Ewart, 1991).
The Social Action Theory remarks that per-
sonal action schemes are socially interconnected to
schemes of close social environment (friends, family,
peers etc.) so they raise significant obstacles to long-
term changes. Its necessary to extend the concept of
state-action focused individually to include social in-
terdependence as a determinant of a change in be-
havior. Close social relations mean that the patterns
of action of each person are interconnected, thereby
increasing the likelihood of someone trying to mod-
ify a routine, influencing and conditioning routines of
other individuals.
This model implies the existence of mechanisms
that enable people to make transitions from old states-
action to other new, causing a change. According to
this theory, attitudes and reinforcements do not deter-
mine and cause behavior. People motivate themselves
by taking into account the possible outcomes, assess-
ing their capabilities and creating goals that guide
and energize the solution of various problems. The
IMPACT OF SEMANTIC TECHNOLOGIES TO HUMAN BEHAVIOR MODELING - A Psychosocial Rationalization
549

health related behaviors are included, according to
the Theory of Social Action, in a set of norms of
behavior focused toward some important goal. This
set of schemas is composed of individual’s personal
projects, it refers to basic tasks (such as getting social
influence, acquire material resources, be accepted by
others, etc.), and it affects to protective rules of behav-
ior making people generate aimed objectives to eval-
uate their own conduct.
The schemas represent organized sets of behav-
iors that focus our attention to specific aspects of sit-
uations and scenarios. They drive the encoding of ex-
perience in memory over the long term. And finally
they provide routines to make tasks. These ways of
knowledge integrate capabilities which allow to con-
sider alternative goals, and to create new action strate-
gies. Capacities are the mechanisms through which
physical and social contexts affect to self-regulatory
conducts. Cognitive control schemes influence the
choices of behavior, increasing trust in the individ-
ual’s ability to maintain or change a behavior. The
context or environment in which people live adjust
the personal capacities and the social relations, af-
fecting the establishment of goals, the consideration
of opportunities for action, and the design of rele-
vant health strategies. The physical characteristics
of the environment determine the access to material
resources, and they also influence in the behavioral
strategies. Social relationships involve a set of bene-
fits, expectations and obligations that likewise influ-
ence on the objectives aimed. In addition, social re-
lationships provide behavior models that facilitate or
inhibit the action guidelines (Rodriguez, 2001).
2.4 Self-efficacy Theory
Bandura (Bandura, 1977) (Bandura, 1988) developed
the Self-efficacy Theory to explain human behavior
and the factors involved in motivation. Self-efficacy
can be defined as the evaluation of the own personal
abilities in view of the possibility of action. There are
different processes that contribute to the configuration
and development of self-efficacy. They are elements
that describe how certain characteristics, both inter-
nal and external to the individual, which also help to
shape the beliefs that she has about what is able or
unable to do:
• Direct experience is the main source of formation
regarding the self concept that an individual has.
In this sense, the consequences obtained after ex-
ecuting the behavior make it possible to report
about one’s ability to carry out the same behav-
ior, and if is probable to control the situational
variables in which this behavior has to be done.
Thus, the experience and consequences obtained
contribute to the formation of self-concept, and
contribute also to develop of personal self-worth
feeling, both required to deal in different situa-
tions.
• Learning by observation is also a source of valu-
able information. To observe and analyze the con-
sequences that any action cause in another indi-
vidual executing such action can lead both to in-
hibit and to promote the own action, depending
on positive or negative assessment of the observed
consequences in other individuals. Its a process of
social comparison in which the individual shape
her perception of her own capabilities to deal with
different situations.
• Persuasive Messages. The attempts of people in
the environment to convince and encourage the
individual to take a specific action can provide se-
curity and support, in order to really produce a be-
havior. However, persuasion is a weaker resource
than previous ones, and it will vary depending on
different variables such as, for example, certain
features related to the personality of the individ-
ual who tries to persuade, the credibility that indi-
vidual has to pass on, or her ability to get another
individual execute the action.
• Physiological activation may also be an impor-
tant modulator of the capabilities that a person be-
lieves she has, can influencing in the process of
self valuation. According to (Bandura, 1988), the
information provided by the psycho-physiological
activation influences the perceived effectiveness
through assessment processes. Therefore, when
such activation happens in the view of the possi-
bility of executing a behavior, the individual eval-
uates different factors, stressing the sources that
cause the activation of behavior, the intensity of
activation, the circumstances in which that activa-
tion happens, and the way in which the activation
influences over the efficiency. When physiologi-
cal activation is successful after the execution of
a behavior on previous experience, this activation
is considered by individuals as a facilitator of the
action, while, in opposition, when it is unsuccess-
ful, it is considered as harmful or inhibitor of the
action (Bandura, 1988).
People increasingly develop their self-efficacy
perception based on executed behaviors, based on
said explanation in their environment, and on the rein-
forcements that other people around them do respect
the conduct has been made.
ICAART 2012 - International Conference on Agents and Artificial Intelligence
550
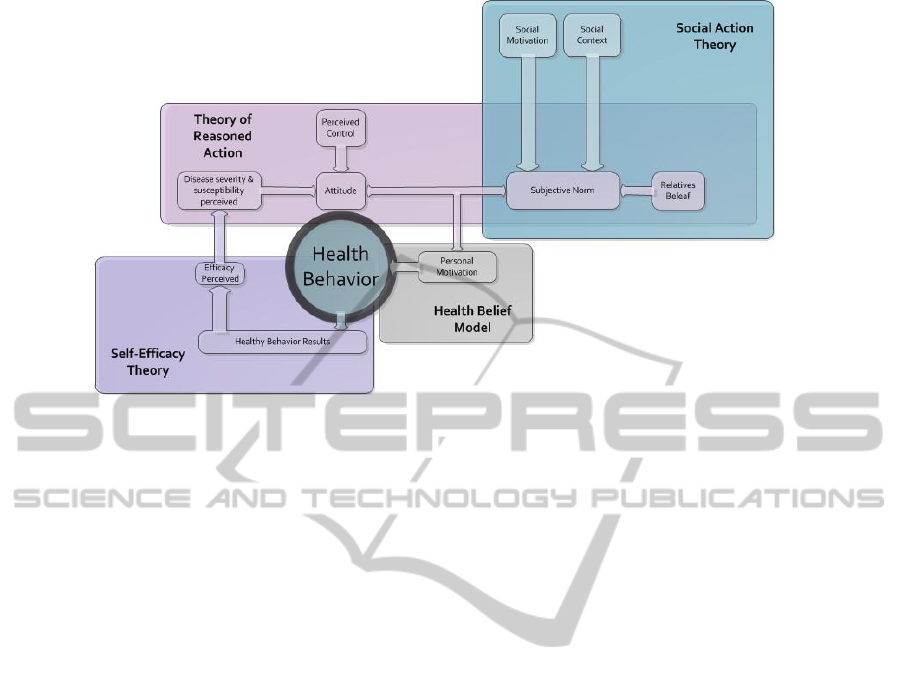
Figure 1: General Architecture of the unified semantical model.
3 TO AN UNIFIED SEMANTICAL
MODEL TO REPRESENT THE
PSYCHOLOGY OF HEALTH
BEHAVIOR
In literature, there are some examples of how the psy-
chology of patients is taken into account to help the
motivation of healthy behaviors (S. and Price, 2009),
(del Hoyo-Barbolla E. et al., 2006), (Hu and Sundar,
2010), (Gustafson et al., 2011). The research in that
field has been based on psychological and psychoso-
cial research fields that are limited to the theoreti-
cal framework that the authors follows. This is be-
cause, in practice, the health social psychology scien-
tific community follows those models in parallel, rep-
resenting the same knowledge from different points
of view. Nevertheles, although described models have
differences in the theoretic perspective, they seems to
be complementary. In figure 1 a general approach to a
collaborative model of the different research theories
is presented.
In that schema, the different models are intercon-
nected according to their main hypothesis in order to
resolve the psychological causes of health behavior
The Health Belief model, mainly based on per-
sonal motivation can be enriched by results achieved
by Theory of Reasoned Action. In this case, the per-
sonal motivation available data might be improved by
the attitude and Subjective Norm of the second theory.
At the same time, according the Self-Efficacy Theory
the attitudes can be continuously evolving depend-
ing on the health Behavior results perceived by the
user. Finally, the Subjective Norm user profile can be
enriched with the thesis of Social Motivation, Social
Context and Relatives Belief in Social Action Theory
The general concepts that these models handle are
equivalents. This allows that the result of the research
on one of the lines can be useful as an entry point
for the rest. In this way, the formal representation of
the results using ontologies allows their use not only
in the same research field but also in the others. In
addition, based on that unified model and representing
the knowledge of the thesis of those different theories
in a semantically tagged concepts it was possible to
perform automatic reasoning over the whole theories
in the psychology of health behavior research field.
The creation of an unified semantic framework to
represent the thesis of Psychology of health behav-
ior will suppose a great advantage in order to provide
a unified view of the knowledge in that field where,
psychologist, sociologist and health professionals not
only will allow to share their knowledge, but also will
be able to enrich their thesis with the direct result of
the investigation of their colleagues.
4 CONCLUSIONS
The use of ontologies to allow the semantic interop-
erability among systems that represent the different
health behavior models will enable de creation of an
unified model that explain the whole health behav-
ior of people. Experts will be able to share not only
in theory but also their knowledge might be used to
reason over the data available in order to create basic
IMPACT OF SEMANTIC TECHNOLOGIES TO HUMAN BEHAVIOR MODELING - A Psychosocial Rationalization
551

knowledge that could be used by other research fields.
These systems can offer a better knowledge that
can be used in conjunction with emerging pattern
recognition theories in order to validate the use of
health promotion techniques.
REFERENCES
Ajzen, I. (1987). Attitudes, traits, and actions: Disposi-
tional prediction of behavior in personality and social
psychology. Advances in Experimental Social Psy-
chology, 20(C):1–63. cited By (since 1996) 183.
Ajzen, I. (1988). Attitudes, Personality, and Behavior. The
Dorsey Press. cited By (since 1996) 1506.
Bandura, A. (1977). Self-efficacy: Toward a unifying
theory of behavioral change. Psychological Review,
84(2):191–215. cited By (since 1996) 6537.
Bandura, A. (1988). Self-regulation of motivation and ac-
tion through goal systems In Cognitive perspectives
on emotion and motivation. Kluwer Academic Pub-
lishers.
Becker, M. and Maiman, l. (1982). Models of Health-
Related behavior in Handbook of Health, Health Care
and the Health Profession. Free Press.
del Hoyo-Barbolla E., R., K., Arredondo, M., and Ortega,
M. (2006). A new perspective in the promotion of e-
health. Studies in health technology and informatics,
124:404–412. cited By (since 1996) 3.
Ewart, C. (1991). Social action theory for a public health
psychology. American Psychologist, 46(9):931–946.
cited By (since 1996) 124.
Fern
´
andez-Llatas, C., L
´
azaro, J. P., and Bened
´
ı, J. M.
(2009). Workflow mining application to ambient
intelligence behavior modeling. In Universal Ac-
cess in Human-Computer Interaction, volume 5615 of
Lecture Notes in Computer Science, pages 160–167.
Springer.
Gustafson, D. H., .and Bret R. Shaw, M. G. B., Isham,
A., McTavish, F., Richards, S., Schubert, C., Levy,
M., and Johnson, K. (2011). An e-health solution for
people with alcohol problems. Alcohol Research &
Health, 33:327–337.
Hochbaum, G. (1958). Public participation in medi-
cal screening programs: A sociopsychological study.
Technical report, PHS publication no. 572. Washing-
ton D.C.: U.S. Government Printing Office.
Hu, Y. and Sundar, S. S. (2010). Effects of online health
sources on credibility and behavioral intentions. Com-
munication Research, 37(1):105–132. Cited By (since
1996): 9.
Lewin, K. (1943). Defining the ’field at a given time.’. Psy-
chological Review, 50(3):292–310. cited By (since
1996) 116.
Lewin, K. (1946). Action research and minority problems.
Journal Social Issues, 2(4):34–46.
M., F. and Ajzen, I. (1975). Belief, Attitude, Intention and
Behavior: An Introduction to Theory and Research.
Addison-Wesley. cited By (since 1996) 6992.
Phua, C., Foo, V. S.-F., Biswas, J., Tolstikov, A., Aung,
A.-P.-W., Maniyeri, J., Huang, W., That, M.-H., Xu,
D., and Chu, A. K.-W. (2009). 2-layer erroneous-plan
recognition for dementia patients in smart homes. In
Proceedings of the 11th international conference on e-
Health networking, applications and services, Health-
com’09, pages 21–28, Piscataway, NJ, USA. IEEE
Press.
Rodriguez, J. (2001). Psicologia Social de la Salud. Sinte-
sis Psicologia.
Rosenstock, I. (1974). Historical origins of the health belief
model. Health Education Monographs, 2.
S., C. and Price, A. (2009). Healthy living with persua-
sive technologies: Framework, issues, and challenges.
Journal of the American Medical Informatics Associ-
ation, 16(2):171–178. cited By (since 1996) 10.
Wasserkrug, S., Gal, A., Etzion, O., and Turchin, Y. (2008).
Complex event processing over uncertain data. In
Proceedings of the second international conference
on Distributed event-based systems, DEBS ’08, pages
253–264, New York, NY, USA. ACM.
ICAART 2012 - International Conference on Agents and Artificial Intelligence
552
