
Knowledge Engineering Requirements for Generic Diagnostic
Systems
Andreas Mueller
1
, Ingmar Hofmann
1
, Heiner Oberkampf
2
and Sonja Zillner
2
1
Siemens AG, Industry Sector, Advanced Technologies & Standards, Nuremberg, Germany
2
Siemens AG, Corporate Technology, Munich, Germany
Keywords: Diagnostic Knowledge, Knowledge Representation, Knowledge-based Diagnostics, Domain-specific
Language, Requirements Analysis, Knowledge Engineering, Reasoning, Knowledge Interchange.
Abstract: Diagnostics is the process of determining the nature of malfunctions or faults of systems in various domains.
With regard to the complexity of systems and their composition of different subsystems or subcomponents,
for which different diagnostic approaches are optimal, no means exist for seamless and agile cooperation
and information exchange between currently isolated diagnostic approaches. However, we consider this
essential for an integrated diagnostic mechanism covering complex systems in their entirety. Hence, in this
paper, we show the basic requirements for a generic diagnostic knowledge representation language (DKRL)
by investigating typical diagnostic examples from different domains, namely industry and medicine. DKRL
is intended to facilitate the generic representation, handling, and interchange of diagnostic knowledge
required for performing diagnostics without regard to specific diagnostic approaches.
1 INTRODUCTION
We are concerned with the efficient representation
of diagnostic information.
Being the process of analytically determining the
nature and cause(s) of a malfunction of a technical
or biological system using structural, functional and
causal knowledge about the system, diagnostics is
used in various disciplines, with variation in the use
and representation of the underlying knowledge. On
malfunctions, a useful diagnostic mechanism must
be able to determine defective parts of the system
and also the root cause of these failures, which may
sometimes lie outside the system’s boundaries. This
determination relies on observations delivering more
details on the system’s current behavior.
Various diagnostic mechanisms address isolated
diagnostic problems. However, the seamless and
agile cooperation between them is currently not
possible. A truly integrated diagnostic mechanism
for analyzing complex systems requires a high-level
exchange of diagnostic information across isolated
diagnostic mechanisms. For this, a vast amount of
different information has to be managed in a precise
and standardized manner. These challenges can be
met by a generic diagnostic representation language
providing means for handling diagnostic knowledge.
Current computer-based diagnostic systems use
established reasoning methods, e.g. rule-based
reasoning (Ligeza, 2006), case-based reasoning
(Kolodner, 1993) or probabilistic reasoning (Pearl,
2005). However, there is little common ground
regarding the formalisms for representing the
diagnostic knowledge. In fact, these are tightly
coupled to each approach. A good survey regarding
such knowledge representation is provided in (Van
Harmelen, Lifschitz and Porter, 2008). This,
however, causes a semantic gap between the
perception of a diagnostic problem and its formal
representation. Also, this causes the diagnostic
knowledge to be bound to the employed diagnostic
approach. The flexible exchange of information
about the structure of the system being diagnosed,
about malfunctions, and observations requires an
explicitly specified terminology of a generic
diagnostic process in an unambiguous manner.
Our overall research goal is to develop a generic
diagnostic knowledge representation language
(which will be referred to as DKRL) that addresses
this lack of a coherent diagnostic formalism in the
form of a domain-specific language (DSL). Intended
to facilitate the representation of diagnostic
problems as such with all relevant diagnostic
aspects, but independent of any reasoning approach.
184
Mueller A., Hofmann I., Oberkampf H. and Zillner S..
Knowledge Engineering Requirements for Generic Diagnostic Systems.
DOI: 10.5220/0004124601840189
In Proceedings of the International Conference on Knowledge Engineering and Ontology Development (KEOD-2012), pages 184-189
ISBN: 978-989-8565-30-3
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

DKRL could eventually become the basis for
machine-processable diagnostic lexicons for
arbitrary domains. Hence, we regard two aspects as
being equally important: representational
capabilities for the diagnostic knowledge itself as
well as facilities for the efficient handling of
represented knowledge. This paper discusses the
analysis and gathering of requirements that need to
be addressed by such a DSL for diagnostics.
The paper is organized as follows. Section 2
describes previous work. Section 3 illustrates aspects
of diagnostics in different domains. Section 4
investigates diagnostics in the domains and
introduces the requirements for generic knowledge
representation. Section 5 concludes the paper and
provides an outlook.
2 RELATED WORK
As one basic distinction of diagnostic systems, we
have model-based (Lucas, 1998) or first principles
(Reiter, 1987) diagnosis, and heuristic classification
(Lucas, 1998) or heuristic diagnosis (Reiter, 1987).
Model-based diagnosis as consistency-based
diagnosis and abductive diagnosis (Lucas,
1998)(Poole, 1994) mainly proved useful in the
technical/industrial domain, whereas in the medical
domain, heuristic diagnosis is often used. In model-
based diagnosis we have a description about how the
system is meant to operate, together with
observations. In heuristic diagnosis, information like
“rules of thumb, statistical intuition and past
experience” are more important and “the real world
system being diagnosed is only weakly represented”
(Reiter, 1987). Even in model-based diagnosis, there
are many different formalisms for similar problems.
Existing approaches for a generic representation
language for diagnostic knowledge focus on only
one of the diagnosis problems. (Reiter, 1987) and
(Poole, 1994) focus on model-based diagnosis. In
(Poole, 1994), a further distinction of system-driven
diagnosis in Consistency-Based Diagnosis and
Abductive Diagnosis is made. It is shown that for a
certain class of problems both formalisms reach the
same diagnosis. In (Lucas, 1998) an attempt is made
to create a generic diagnosis language. “Evidence
functions” are used to represent the knowledge
common to all diagnostic systems, the interactions
among defects and findings (Lucas, 1998). The
experience-driven (heuristic) approach is realized in
Bayesian networks (probabilistic dependencies),
default logic (rules of thumb) etc. However, there is
still no overall diagnosis representation language
able to represent the full spectrum of different
diagnostic knowledge.
As our overall goal, DKRL is intended to cover
both model-based and heuristics-based diagnosis.
Showing typical features of the respective diagnosis
types, in the following the industrial and the medical
domain were selected for a requirements analysis.
3 DIAGNOSTICS IN DIFFERENT
DOMAINS
We exemplarily consider the domains “industry”
and “medicine” since these substantially differ in
complexity and availability of reliable factual and
causal knowledge, yet in both domains reaching a
correct diagnosis quickly is critical.
The proposal to capture the notion of diagnostic
reasoning has been considered by two extreme poles
of the diagnosis problem (Poole, 1994): Firstly, the
overall aim may be to describe how components are
structured and work normally, however information
on the origin and the manifestation of malfunctions
is missing. This holds true for the industrial domain,
thus, diagnostic algorithms aim to isolate deviations
from normal behavior. Secondly, knowledge about
faults and symptoms may be used to interpret the
relevance of abnormalities. This holds true for the
medical domain: medical diagnostic knowledge is
typically about “incorrect functioning”.
For a comprehensive set of requirements needed
to represent diagnostic knowledge generically, we
analyze typical diagnostic use case scenarios from
the industrial and the medical domains. The
following examples illustrate the aspects relevant in
diagnostic processes in the selected domains and
show the requirements to be met in order to perform
the described diagnostics. When gathering the
requirements, we discussed with experts and
analyzed existing systems to identify roadblocks and
shortcomings. The medical examples are taken from
interviews with our clinical partners.
3.1 Diagnostics in Industry
Typically, the industry domain shows a high degree
of engineered knowledge, with an adequate
understanding of the considered plant or component
and corresponding diagnostic knowledge being
possibly available from the beginning of the
respective lifecycle. Thus, observations can often be
performed directly and symptoms can often be
treated as directly identifiable causes of observed
KnowledgeEngineeringRequirementsforGenericDiagnosticSystems
185
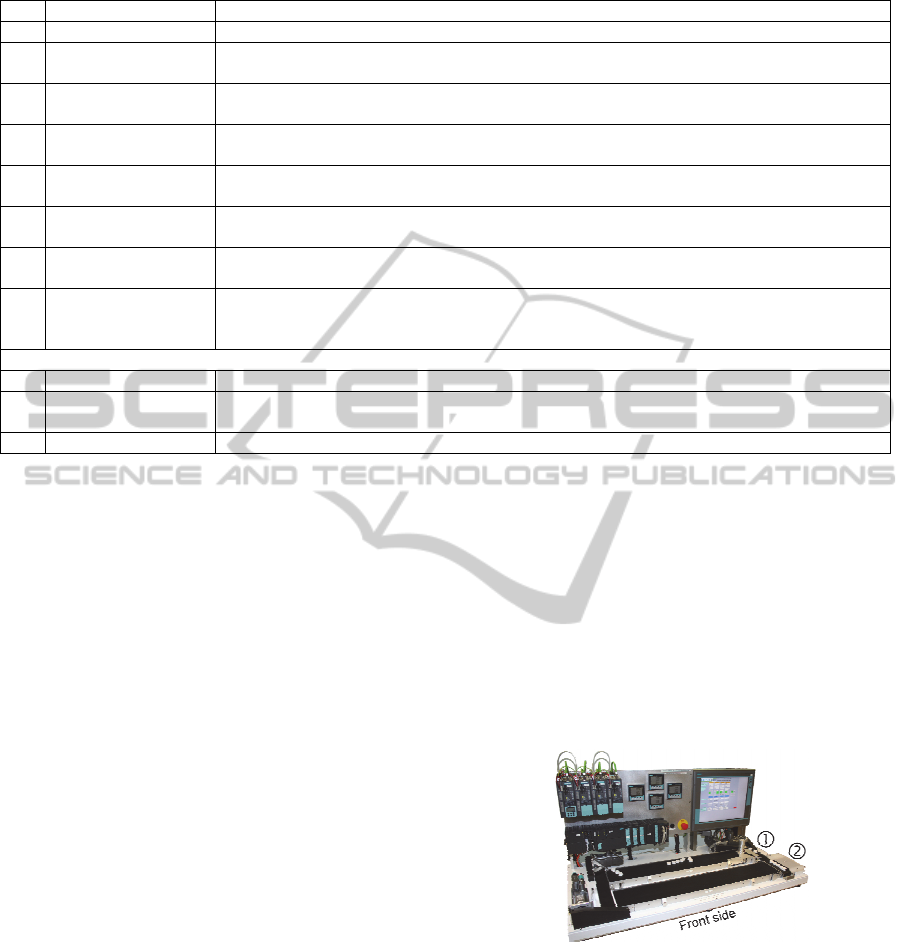
Table 1: Entities from the industrial domain.
# Entity Explaining remark
I1. Causal relationships In many cases it is possible to state the potential causes for symptoms.
I2. Causes and effects
(symptoms)
Sensors as well as the human operator’s sense provide information that can be interpreted as a
manifestation of a malfunction or fault.
I3. Context-dependent
interpretation
Nominal values for operating parameters need to be interpreted with regard to e.g. the currently
selected mode of plant operation or environmental influences.
I4. Likelihood of
occurrence
As shown in the example of the feeder malfunction, of two possible causes one might occur less
likely than the other.
I5. Localization Recognizing components or functions of a plant where a given effect typically occurs is important
in order to direct service technicians.
I6. Probabilistic causality Causal relations are not necessarily absolute. Instead, there would be more than one possible, but
not equally likely, causes for an observed symptom..
I7. Significance of a
symptom
Certain observed symptoms are typical for certain causes, due to the respective system’s structure
or functionality.
I8. Temporal correlation Some causes and effects become relevant only in correlation to the amount of time passed. Also,
due to aspects such as the system’s structure or functionality, the effect of an occurred cause
might become visible only after some time has passed.
Additionally important functional aspects
I9. Extensibility Knowledge is subject to change due to plant modifications during the lifecycle.
I10. Incomplete knowledge A lack of knowledge at the system level and instance level must be handled. Exact probabilistic
knowledge about the causal relations is not always available.
I11. Reusability Knowledge about symptoms, etc. may be relevant for different faults, thus should be reused.
faults by applying sensors to critical positions in the
structure or the process. Also, the causality behind
symptoms is usually rather easy to determine.
3.1.1 Example 1: Process Industry
(Abdul-Wahab et al., 2007) give examples of
troubleshooting in the domain of multi-stage flash
seawater desalination, with focus on the brine heater
component. Considering the process value of
“condensate conductivity” as a representation of the
salt ratio in low pressure steam after condensation,
the plant operator might observe a gradual increase.
The degree of increase might be a symptom of
leaking tubes in the brine heater, since this would
cause seawater to mix with the condensate, resulting
in an increase of conductivity due to a higher salt
ratio. Hence, the “leakage” needs to be ruled out by
maintenance actions. If the conductivity continues to
rise, automatic valve operation measures would be
taken. Similarly, the conductivity of the distillate
might also show a symptomatic, differently located
increase. Here, a possible cause might be an
increased “top brine temperature”, which can be
responsible for increased brine flashing, causing the
conductivity to rise due to a higher salt ratio.
3.1.2 Example 2: Manufacturing Industry
At Siemens in Nuremberg a research facility is
operated, producing a running text made from small
plastic disks using a series of conveyor belts (see
Figure 1) as an exemplary manufacturing process.
Normally, the disks are separated from the rear-side
storage belt and transported onto the right-hand-side
“column belt” (1), where the next required disk
column is prepared according to the control system.
The column is then pushed onto the front-side “text
belt” by a properly triggered proximity switch (PS)-
controlled feeder (2), positioning the column at the
correct distance in relation to the previous one.
Considering the “text belt”, the symptom of
“irregular positioning patterns” might occur.
Figure 1: Siemens research facility for the manufacturing
process of mechanical running text production.
This can be caused by a wrong feeder mode
(continuous instead of on-demand). Currently, the
reason may be either a broken PS cable connection,
so trigger signals can no longer be received, or a
broken PS, which can be treated as less likely.
3.2 Diagnostics in Medicine
In the medical domain, direct observations are often
KEOD2012-InternationalConferenceonKnowledgeEngineeringandOntologyDevelopment
186

Table 2: Entities from the medical domain.
# Entity Explaining remark
M1. Context-dependent
interpretation
Standard intervals for measurements like blood pressure or blood counts need patient-specific
interpretation regarding, e.g. the patient’s age.
M2. Functional dependencies
and localization
For instance, an artery functionally supplies blood to a number of organs. Such information allows the
physician to anticipate phenomena and to imagine an internal situational picture of the disease he is
confronted with.
M3. Patient history For many diseases risk factors are known. They influence the probability of certain diseases and allow
the clinician to check for such diseases first.
M4. Probabilistic causality The disease-symptom-relation is typically a probabilistic causal relation – e.g. lymphoma has the
associated symptom enlarged lymph nodes in 80% and the symptom enlarged spleen in 30% of all
cases (Herold, 2011).
M5. Relations between
symptoms
Symptom descriptions are fuzzy, e.g. elevated temperature vs. mild fever. Also, some symptoms form
groups like e.g. the B-symptoms - occurring together they constitute a cardinal symptom for lymphoma.
M6. Symptom significance Cardinal symptoms help to focus on certain diseases in the initial diagnosis phase. Additional
occurrence of pathognomonic symptoms allow an immediate diagnosis.
M7. Symptoms There are symptoms that can be observed on a patient during a diagnostic process without being able to
immediately draw conclusions about the actual disease. This situation is typical when recording a
patient's medical history, where symptoms are collected as reported by a patient before being
interpreted.
M8. Temporal progression Diseases may show a characteristic development of symptoms over time. Another temporal factor is the
“novelty” of a symptom.
M9. Urgency of symptoms Diseases and their symptoms are not equally dangerous for the patient’s health. Thus, highly dangerous
diseases and related symptoms have to be checked first.
Additionally important functional aspects
M10. Extensibility Knowledge is subject to change, so it must be represented in an extendable way.
M11. Incomplete knowledge A lack of knowledge at the system level and instance level must be handled. Exact probabilistic
knowledge about the causal relations between diseases and symptoms is not always available. Similarly,
the complete patient situation is seldom known.
M12. Reusability Diagnostic knowledge may be relevant for various diseases, thus should be reused.
impossible, so conclusions about the actually desired
biological characteristics have to be drawn based on
observable characteristics and presumed or
confirmed interrelations. Because of the domain’s
inherent complexity, medical diagnostic knowledge
contains a high degree of uncertainty.
3.2.1 Example 1: Differential Diagnosis
Differential diagnosis is a standard diagnostic
approach in clinical practice. We illustrate the
process along an example: first, the observation of
an initial set of (unspecific) symptoms, say “fever”,
“night sweats”, “feeling weak” and “changes in
bowel patterns”, leads the clinician to suspect a set
of likely diseases which might have caused the
symptoms. Second, the set of likely diseases is turned
into a ranked list based on information about
cardinal symptoms, incidence proportion of a
disease and other factors. Since “changes in bowel
patterns” is a cardinal symptom for “diverticulitis”
and “colorectal cancer”, we may obtain a ranked list
like “diverticulitis”, “colorectal cancer”, “cold”,
“lymphoma” etc. Third, the clinician aims to
differentiate between the likely diseases by checking
for further symptoms that might strengthen or
weaken diagnoses on the list. At first, he will check
other (cardinal) symptoms of top-ranked diseases. In
this case he might identify “weight loss” and
“enlarged lymph nodes” but does not find evidence
for “blood in stool” and “thickened intestinal wall”.
Fourth a more precise list of likely diseases is
obtained, with “lymphoma” now at the top as both
cardinal symptoms (“enlarged lymph nodes”) and B
symptoms (correlation of “fever”, “night sweats”,
and “weight loss”) are present. “Diverticulitis” and
“colorectal cancer” become less likely as important
symptoms “blood in stool” and “thickened intestinal
wall” are absent. The process continues until a
plausible diagnosis is found.
3.2.2 Example 2: Lyme Borreliosis
As an infectious disease, Lyme borreliosis has
exactly one cause: the patient has been infected by
bacteria of genus Borrellia after a tick bite (Masuhr,
1996). Depending on both the part of the body the
infection took place at, and the time passed since the
infection, different symptoms occur. The course of
borrelliosis is divided into three stages after
KnowledgeEngineeringRequirementsforGenericDiagnosticSystems
187
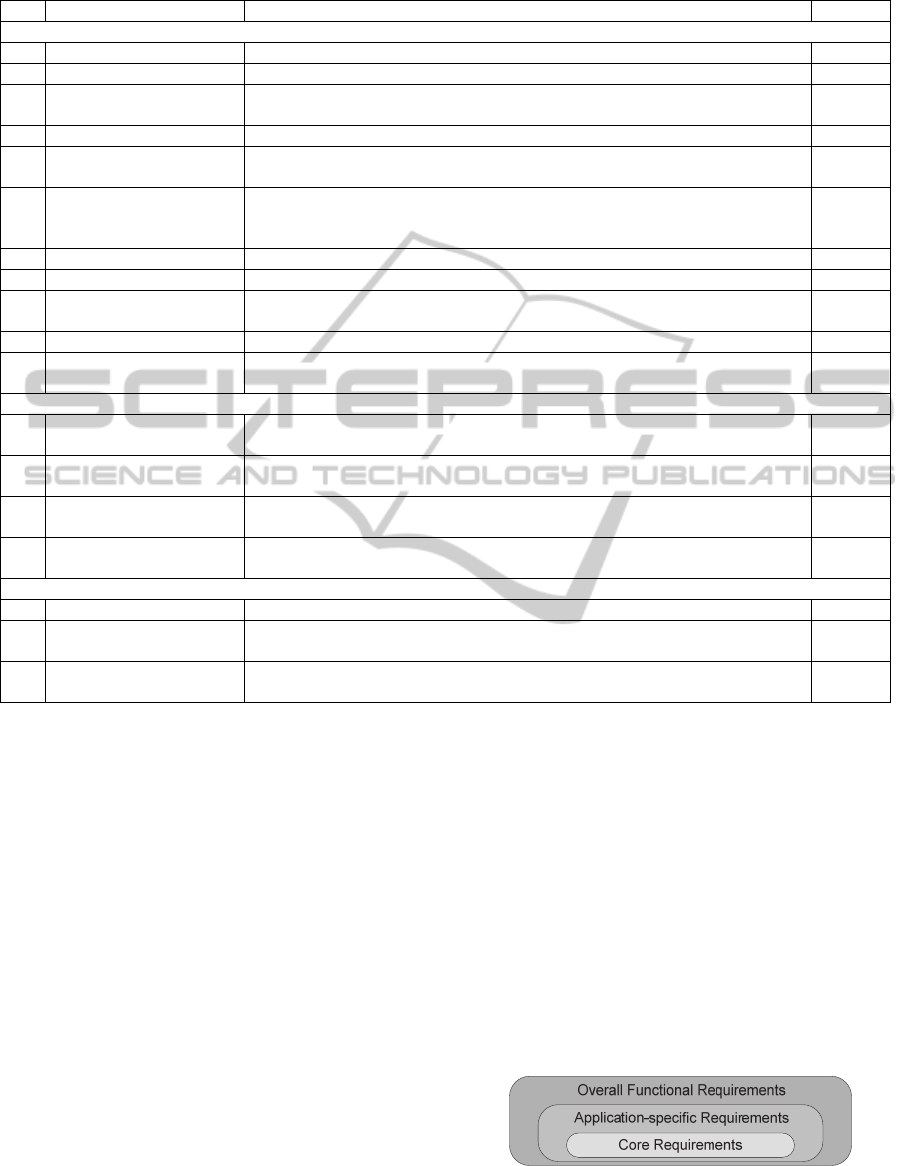
Table 3: Requirements and classifications.
# Requirement Explaining remark Based on
Core requirements: mandatory for the intended representation language
R1. Causality DKRL must represent causality (cause-effect-relationships). I1, M4
R2. Causes and effects DKRL must represent causes and the effects of causes. I2, M7
R3. Context-dependent
interpretations
DKRL must represent information about the interpretation of measurements taking into
consideration DO-specific influences.
I3, M1
R4. Faults DKRL must represent faults that may (have) occur(ed) on a DO. I2, M3
R5. Likeliness under error
conditions
DKRL must represent the likeliness of symptoms and faults for each of the DO’s components
as well as for the DO as a whole to occur under error conditions.
I4, M6
R6. Likeliness under nominal
operating conditions
DKRL must represent the probability that symptoms and faults occur under nominal
operating conditions, since even under optimum conditions there is possibility of spontaneous
malfunctions that might spread throughout the DO.
I6, M4
R7. Localization (physical) DKRL must represent where a symptom or fault is located physically . I5, M2
R8. Localization (functional) DKRL must represent where a symptom or fault is located functionally. I5, M2
R9. Significance of causal
relationships
DKRL must represent that a symptom or cause may have a different significance to a fault or
an effect, respectively, than another symptom/cause.
I6, I7, M4
R10. Symptoms DKRL must represent symptoms that may occur on a DO. I2, M7
R11. Temporal classification DKRL must represent information that effects might become observable only after some time
has passed after the occurrence of a cause.
I8, M8
Application-specific requirements: optional for the intended representation language
R12. Novelty of symptoms DKRL must represent information that the new occurrence of symptoms during the course of
a fault may be of special importance.
M8
R13. Relationships between
symptoms/causes/effects
DKRL must represent information that certain symptoms, causes, or effects have a special
relationship to other symptoms, causes, or effects, respectively.
M5
R14. Temporal relevance of
symptoms
DKRL must represent the temporal relevance of symptoms, i.e. the period of time a symptom
is of significance for a certain fault.
M8
R15. Urgency DKRL must represent information that certain symptoms need to be investigated prior to
others.
M9
Overall functional requirements: mandatory for effective and efficient knowledge management
R16. Extensibility DKRL must represent knowledge in an easily modifiable manner. I9, M10
R17. Incompleteness of knowledge DKRL must represent knowledge so that valid descriptions can be created, even though there
might be information missing.
I10, M11
R18. Reusability DKRL must represent knowledge in a manner that allows reuse or
referencing of knowledge once it has been captured.
I11, M12
infection. The cardinal symptom of the first stage (3
days to 3 weeks) is a circular rash called erythema
chronicum migrans at the region of the tick bite. In
the second stage (1 to 4 months) different body parts
will be affected and the patient might show
symptoms of a meningopolyneuritis like radicular
pain or even facial paralysis. Here, for anamnesis the
physician would ask the patient if he remembers a
tick bite, but also needs to conduct several tests,
since these symptoms might be caused by other
diseases. In the third stage (>5 months) untreated
patients might show colored areas of skin
(acrodermatitis chronica atrophicans) or joint
disorders as a possible symptom of Lyme arthritis
and diagnosis is even more complex. The common
underlying reason for this diversity of symptoms is
the spreading of the bacteria in the body together
with the initiated pathomechanism (comprising the
effects of “cellular invasion” and consequently
“inflammatory reactions”), which progresses at
different rates depending on the affected tissues.
4 REQUIREMENTS ON
KNOWLEDGE
REPRESENTATION
From these examples, we obtain the aspects to be
represented and derive the requirements for DKRL.
We distinguish between core requirements (most
basic and essential; inherent to all diagnostic
decisions), application-specific requirements (only
relevant within applications for special diagnostic
problems), and overall functional requirements (for
effective and efficient handling of knowledge) (see
Figure 2).
Figure 2: Requirement layers.
KEOD2012-InternationalConferenceonKnowledgeEngineeringandOntologyDevelopment
188

4.1 Relevant Entities from the
Considered Domains
In the following sections we describe the knowledge
entities and aspects typical for each domain. The
representation language must be able to represent
these either implicitly or explicitly.
4.1.1 Entities from the Industrial Domain
The examples illustrate that diagnostics in the
industrial domain strongly uses pre-engineered
domain knowledge. If available, systemic
information about the representatives of the
respective domains (i.e. components used in process
technology or in the manufacture of discrete parts)
in terms of structure and functionality is rather
certain and complete. Hence, symptoms and often
their causes are well-known and thus can be directly
captured. To represent the required diagnostic
knowledge, we have identified the entities in Table 1
to be required.
4.1.2 Entities from the Medical Domain
The examples illustrate that medical diagnosis is
largely based on the clinician’s experience and
statistical information: he knows from experience
which disease might cause certain general and
cardinal symptoms, and he knows about the
significance of symptoms for certain diseases. Based
on statistics, more frequent diseases will be
considered first. On the other hand, systemic
information about the human organism is less certain
and complete, and processes in the human body are
highly interconnected and not yet understood well
enough to facilitate correct model-based diagnosis.
We consider the entities in Table 2 to be important
in order to represent medical diagnostic knowledge.
4.2 Requirements and Classifications
From the entities listed for each domain, in Table 3
we now derive the requirements that the intended
representation language has to meet (representatives
from the domains are generically referred to as
diagnostic objects, abbreviated DO).
5 CONCLUSIONS AND
OUTLOOK
In this paper we have derived the requirements for a
generic diagnostic knowledge representation
language (DKRL) by investigating diagnostic
knowledge from the exemplary domains of industry
and medicine. DKRL is intended for use with any
diagnostic system, for handling diagnostic
knowledge in an easily reusable way. We have
shown that the majority of requirements holds true
in both domains. Application-specific requirements
are mainly induced by the medical domain. Still, this
does not restrict their relevance to the medical
context. In fact, we consider that fulfilling these
requirements step-by-step forms a suitable basis for
gradual extension of the diagnostic functionalities
addressable by DKRL. Hence, the identified
requirements allow for the development of DKRL as
well as a corresponding software infrastructure.
The future development of DKRL will focus on a
prototypical implementation with full coverage of
the core requirements and the overall functional
requirements, followed by adding application-
specific representational capabilities.
ACKNOWLEDGEMENTS
The authors are grateful to Dr. Kristina Bayerlein,
senior physician at the University Hospital of
Erlangen, for details on the interpretation of the
medical terminology.
REFERENCES
Abdul-Wahab, S., Elkamelb, A., Al-Weshahic, M. & Al
Yahmadia, A., 2007. Troubleshooting the brine heater
of the MSF plant using a fuzzy logic-based expert
system. In Desalination, vol. 217, no. 1-3, pp. 100-
117.
Herold, G., 2011. Innere Medizin, Herold.
Kolodner, J., 1993. Case-Based Reasoning, Morgan
Kaufmann Publishers Inc., San Mateo, CA.
Ligeza, A., 2006. Logical Foundations for Rule-Based
Systems, Springer, Berlin Heidelberg.
Lucas, P., 1998. Analysis of notions of diagnosis. In
Artificial Intelligence, vol. 105, no. 1-2, pp. 295-343.
Masuhr, K., Neumann, M., 1996. Neurologie,
Hippokrates. Stuttgart.
Pearl, J., 2005. Causality, Cambridge University Press,
New York.
Poole, D., 1994. Representing Diagnosis Knowledge. In
Annals of Mathematics and Artificial Intelligence, vol.
11, pp. 33-50.
Reiter, R., 1987. A Theory of Diagnosis from First
Principles. In Artificial Intelligence, vol. 32, no. 1, pp.
57-95.
Van Harmelen, F., Lifschitz, V., Porter, B., 2008.
Handbook of Knowledge Representation, Elsevier
Science.
KnowledgeEngineeringRequirementsforGenericDiagnosticSystems
189
