
Accelerating Health Service and Data Capturing Trough Community
Health Workers in Rural Ethiopia
A Pre-requisite to Progress
Zufan Abera Damtew
University of Oslo, Informatics Department, Oslo, Norway
Keywords: Community Health Workers, Health Extension Package, Health Data, Knowledge Boundaries,
Communication, Brokering.
Abstract: Community based health service is escalating in many developing countries as a means to fulfill health
related millennium development goals. Community health workers provide primary health care, and collect
and compile health data in collaboration with different actors. This collaboration requires knowledge
communication. An interpretative case study was conducted in Ethiopia to understand the knowledge
communication across boundaries. Using transfer, translation and transformation framework of Carlile, this
study discuss how knowledge related to the health extension packages is communicated across syntactic,
semantic and pragmatic boundaries among health extension workers, their teachers, supervisors, community
volunteers and rural households. The study also describes the knowledge brokering role of health extension
workers and voluntary community health workers. They interact and negotiate with rural households to
facilitate communication of novel knowledge concerning the health extension packages. The study
identified impediments that preclude knowledge communication. In order to improve knowledge
communication across boundaries and enhance the implementation of health extension packages, it is
essential; to formulate apt target for health services, equip health extension workers training schools with
essential resources, offer trainings to community volunteers and make available standardized register and
report formats at health posts for proper recording and reporting.
1 INTRODUCTION
Community health workers are best positioned to
deliver health services at grass-root level as
countries around the globe strive to meet the
Millennium Development Goals (MDGs) (WHO
and Global Health Workforce Alliance, 2010). In
addition to health care provision, community health
workers are also playing an important role in
capturing and communicating the community health
data (Otieno, 2012). Information that is available in
most developing countries is derived from health
facilities, yet most illness and death occur outside
the health system. Presently, community health
workers are providing primary health care and
collect health status data at the community and
household level that helps for informed decisions
(ibid). Community health workers have been used to
collect health related data in many countries that
increases the health coverage, for example,
achieving high rates of case detection for
Tuberculosis in Bangladesh (Chowdhury et al,
2009). Although it is emerging, computerization of
HIS at all levels in the health care system of most
developing countries seems intricate with the
existing infrastructure and human resources. Thus,
data from the community service sites and primary
health care units are currently gathered manually.
This paper draws on empirical findings from
Ethiopia, a country striving to improve the health
service access and data capturing through salaried
community based health workers called health
extension workers (HEWs).
In Ethiopia, health extension program is
designed to improve the health status of families,
with their full participation, using community’s skill
and wisdom (FMOH, 2005). The main pillars for the
health extension program are HEWs. Their primary
role is to perform preventive health education to
households in their homes. Through close
interactions, HEWs improve the implementation of
innovative health extension packages by rural
168
Abera Damtew Z..
Accelerating Health Service and Data Capturing Trough Community Health Workers in Rural Ethiopia - A Pre-requisite to Progress.
DOI: 10.5220/0004135101680177
In Proceedings of the International Conference on Knowledge Management and Information Sharing (KMIS-2012), pages 168-177
ISBN: 978-989-8565-31-0
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)

dwellers. HEWs are supported by trained body of
voluntary community health workers (VCHWs),
who are members of a given community and they
volunteer to support HEWs.
Health care is a dynamic discipline whereby new
procedures, practices and treatments are introduced
very often, which demand in-service training,
mentoring and knowledge communication.
Nevertheless, providing in-service training for entire
HEWs will not be an easy for resource constraint
country like Ethiopia. Studies also indicated that
knowledge communication among the public health
actors is a challenging process. For instance, a study
conducted with the premise of target setting
procedure for immunization service in Ethiopia has
showed the gap between target given for health
services from districts to health posts (HEWs) and
head counted population by HEWs (Damtew and
Kaabøll, 2011). This gap created confusion and lack
of common understanding between HEWs and the
health authorities. The effort to scale-up the
innovative health extension packages requires close
interaction and negotiation between HEWs and rural
households. Moreover HEWs interact with their
colleagues, supervisors, VCHWs and traditional
birth attendants (TBAs) that require knowledge
communication.
In this study, the knowledge transfer, translation
and transformation (the 3-T) framework by Carilie
(2002; 2004) was used to understand the knowledge
communication across boundaries in day-to-day
practices of community health workers. In this
framework the author revealed that communicating
knowledge across three progressively complex types
of boundaries— syntactic (structure), semantic
(meaning), and pragmatic (practice) — requires
different processes that include transfer, translation
and transformation. In this framework, four
characteristics, which facilitate effective boundary
process and knowledge communication, are
specified. These characteristics include---establishes
a shared language; provides a concrete means of
specifying differences and dependencies; facilitates
the way for jointly transformation of knowledge and
enable multiple interactions. This framework helps
to analyze the knowledge communication process
across boundaries in the public health sector. In this
case, knowledge communication or sharing refers to
the way HEWs along with their teachers,
supervisors, colleagues, VCHWs, TBAs, and the
community transfer, translate and transform their
knowledge while performing their day-to-day
activities.
Different researchers also mentioned that
knowledge brokering can contribute to innovation
and knowledge communication (Hargadon, 2003;
Howells, 2006) and it is effective in improving the
service quality and decision making (Dobbins et al.,
2009). Brokering involves process of translation,
coordination, and alignment between perspectives
and it promotes interaction. The role of knowledge
brokers as intermediaries is widely documented.
The broker is constantly seeking knowledge
opportunities in his/her immediate environment,
capable of introducing promising new innovations
(ibid). Brokering knowledge thus means far more
than simply moving knowledge—it also means
transforming knowledge (Myer, 2010). Knowledge
brokering tends to happen in particular locations—in
spaces that privilege the brokering of knowledge
across boundaries. For instance,
Ward, V., House
(2009) indicated that individuals were employed to
act as “knowledge brokers” and their job was to
facilitate the transfer of knowledge between
researchers and practitioners in order to improve the
health outcomes. Within the same vein, this research
identifies the role of HEWs and VCHWs as
knowledge brokers in the expansion of the
innovative health extension packages.
This research addresses the following two
questions; what is the role of HEWs and VCHWs as
knowledge brokers to facilitate the implementation
of the innovative health extension packages by rural
households? And, how can knowledge
communications regarding the health extension
packages is facilitated across boundaries?
A qualitative case study through observation,
interviews, focus group discussion and document
analysis was conducted to answer the research
questions.
The rest of the paper is organized as follow. In
section two, I briefly discuss the literature reviewed.
In section three, I provide background of the
research context. This chapter also summarizes the
research methods adopted for the data collection and
analysis. Thereafter, in section four, the findings
will be presented. I then provide the discussion and
conclusion of the study in section five.
2 LITRATURE REVIEW
2.1 Knowledge Boundary and
Communication
This paper deals with the notion of knowledge
communication across boundaries between
communities. These communities consist of public
AcceleratingHealthServiceandDataCapturingTroughCommunityHealthWorkersinRuralEthiopia-APre-requisiteto
Progress
169

health actors from different specialized domain that
include HEWs, VCHWs, traditional birth attendants
(TBAs), health managers and rural dwellers.
According to Carlile (2004: 2002), the difference in
the knowledge domain, dependence (the degree to
which people take each other’s views into account to
meet their goals) and novelty of domain-specific
knowledge among people at the boundary determine
the complexity of communicating knowledge.
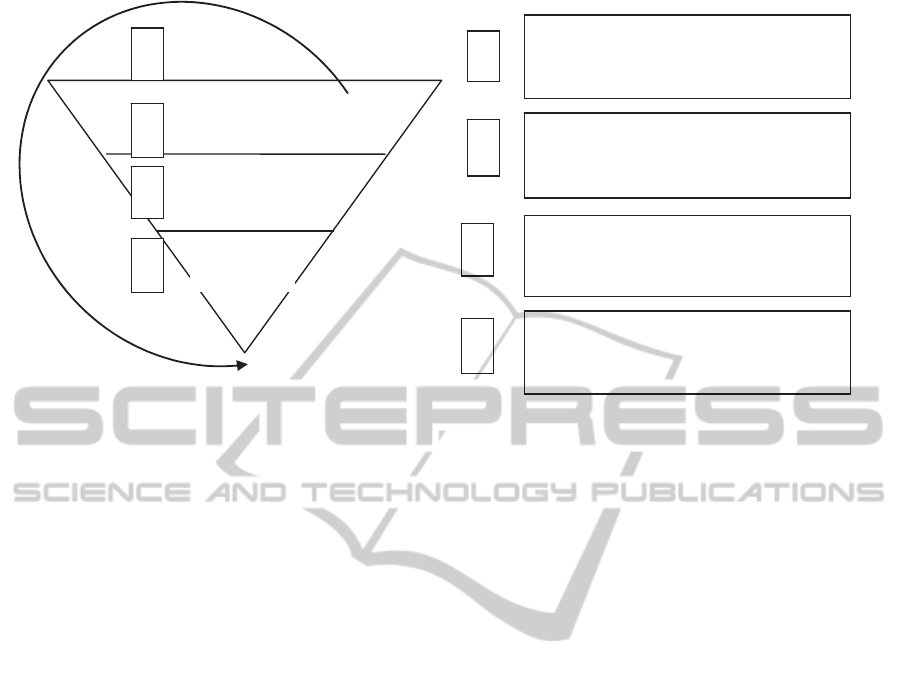
Carlile (2004) used an inverted triangle to show how
increases in the difference, dependence, and novelty
of knowledge between people create three
progressively complex boundaries— syntactic,
semantic and pragmatic (See figure1).
As shown in figure1, tip of the inverted triangle
represents situations where the syntax/language is
shared and sufficient, so knowledge can be
transferred across the boundary. Knowledge transfer
focuses on one-way movements of knowledge or
learning from one place to another or from sender to
receiver (Argote, 1999; Szulanski, 1996). The major
challenge of knowledge transfer is using a
communication medium that is capable of
transmitting the richness of the information to be
conveyed (Daferdst and Lengel, 1984). However, as
novelty increases and the gap grow, new differences
and dependencies arise that requires a semantic
boundary and translation to create new agreements.
This necessitates conversation or discourse to share
knowledge between actors. Discourse is needed to
create shared meanings as way to address the
interpretive differences among actors (Carlile, 2004;
2002). Through collaboration, the participants
produce common meanings and coordinate local
agreement, for instance when co-authors of a paper
simultaneously construct meanings of their work and
make sense of their interaction.
On the other hand, under conditions of
conflicting interests, creating common meanings
(translation) may not be possible: what is required is
a process in which participants negotiate and are
willing to transform their own knowledge and
interests to fit a collective domain (ibid). A
pragmatic boundary assumes the conditions of
difference, dependence and novelty are all present,
and requires transforming the existing knowledge.
Differing background and interest of
stakeholders who are commonly engaged in similar
work may face complex (pragmatic) boundaries to
communicate their knowledge that require multiple
iterations. This is why the knowledge a group
currently uses is such a problematic anchor point
when novelty arises across the knowledge boundary.
Carlile, (2002; 2004) also identified four
characteristics (see Figure1), which facilitate
effective boundary process that include: 1)
establishes a shared language to represent
knowledge; 2) provides a concrete means of
specifying differences and dependencies; 3)
facilitates a method in which individuals can jointly
transform the knowledge used and 4) the need of
multiple interactions. He stated that different
combinations of characteristics of a boundary
process are required depending on the type of
boundary faced.
If a syntactical boundary is faced, only
characteristics 1 and 4 are necessary because it is a
matter of transferring knowledge through a given
syntax. At a semantic boundary, characteristics 1, 2
and 4 are necessary. Here, with some shared syntax
and a negotiation on the differences and
dependencies, new agreements can be created to
reconcile the discrepancies. At a pragmatic
boundary, characteristics 1, 2, 3 and 4 are necessary.
The current and novel forms of knowledge have to
be jointly transformed to create new knowledge.
Hence, communicating at more complex boundaries
requires the capacity below them. For example,
knowledge translation assumes knowledge transfer,
and knowledge transformation also requires
knowledge transfer and knowledge translation
processes.
2.2 Knowledge Brokering
Knowledge brokers can facilitate the knowledge
communication by identifying, synthesizing and
adapting knowledge for the potential users (Meyer,
2010). Sverrisson (2001) also mentioned that
knowledge brokers can be individuals or
organizations that facilitate the creation, sharing, and
use of knowledge. An important task for the broker
is to foster the conditions where the level of
acceptance for any action is considerably higher than
the level of resistance (Jackson, 2003). This may
requires much iteration undertaken over a substantial
period of time.
According to Meyer (2010), brokering involves a
range of different practices: the identification and
localization of knowledge, the redistribution and
dissemination of knowledge, and transformation of
this knowledge.
The role of knowledge brokers as intermediaries
to facilitate knowledge communication is not new
(Hargadon, 2003). Over time, this role of knowledge
brokers has diversified and has often been adapted to
different contexts including the health sector (van
Kammen, et al., 2006). The authors discussed the
KMIS2012-InternationalConferenceonKnowledgeManagementandInformationSharing
170
Pragmatic
Semantic
Syntactic
1
2
3
4
1
2
3
4
Supportsaniterativeapproachwhere
individualsgetbetteratrepresenting,
specifyingandtransformingknowledge.
Allowsindividualstonegotiate,validateand
transformtheirknowledgeinorderto
createnewknowled
g
e
.
Provide individualsaconcretemeanso
f
specifyingtheirdifferences
and
dependencies.
Establish somesharedlanguage/syntaxfor
representingeachother’sknowledge.
Figure1: 3-T Framework and the four characteristics of a “Boundary Process”, adapted from Carlile (2004: 563).
importance of knowledge brokering to develop
evidence based health policy. In this context, we
want to explore the intermediaries (knowledge
brokering) role of HEWs and VCHWs between the
source of knowledge (the health extension package)
and users of knowledge (the rural community) that
may facilitate expansion of the innovative health
extension activities.
3 RESEARCH CONTEXT AND
METHODS
3.1 Research Setting
The case study site presented in this paper is based
in Ethiopia, a developing country located in the horn
of Africa. Organizational structure of the health care
system of Ethiopia comprises four tiers, primary,
secondary and tertiary levels of health care. The first
two tiers are the primary health care units consist of
health posts where HEWs are deployed and health
centers that provide basic curative services. The
health extension program in Ethiopia, which this
study is focused on, was introduced in 2004.
Accordingly, each household is expected to
implement sixteen health packages, which could be
broadly categorized into four areas--environmental
sanitation and hygiene promotion, family health,
major diseases prevention and control, and health
education and communication (FMOH, 2005). Two
HEWs are mostly responsible for a community with
about 5,000 populations where about 20 VCHWs
also work in cooperation with HEWs. Households
are motivated to practice health extension packages
that may lead them to healthy living. According to
the HEP national guideline, households graduate
within six month after implementing 75% of the
sixteen health extension packages.
3.2 Methods
This study employed an interpretive case study
approach (Walsham, 2006) with the use of
interviews, observations, document analysis and
focus group discussion. We have also attended the
primary health care unit meeting in one health
center. “Case studies emphasize detailed contextual
analysis of a limited number of events or conditions
and their relationships” (Soy, 2006). A case study
was chosen because this approach brings about an
understanding of a complex issue hence provide
insights in investigating the cooperation and
knowledge communication in day-to-day practice of
public health actors.
The empirical materials presented in this study
were collected during the periods from December
2009 to February 2010 and from June to July 2011.
Data gathering was carried out at two HEWs
training schools, Amhara region health Bureau, two
zonal health departments, four district health offices,
and eight health posts. Data were collected by the
author and informed consent was sought from each
study participant. Interviews were conducted with
four HEWs’ teachers, nine health managers at
regional, zonal and district health offices and 12
HEWs. We also conducted focus group discussions
AcceleratingHealthServiceandDataCapturingTroughCommunityHealthWorkersinRuralEthiopia-APre-requisiteto
Progress
171

with HEWs and VCHWs in three villages where
each group consisted of five to six participants.
Observation helped to get first hand information
about the organization of rural health posts, the tools
that HEWs using including the registers and health
communication support materials. Document
analysis was done on various sources such as,
working manuscripts, HEWs field note-books and
official registers and formats used to collect,
analyze, and transmit data.
A research diary was maintained throughout the
data collection to document interview notes,
observations and ideas raised during the meeting and
focus group discussions. Notes taken during data
collection were transcribed at the end of the day.
The data analysis was interpretative through
triangulating data from different sources and some
notes were cross-checked with respective
respondents. Theoretical concepts that include
knowledge boundary, communication and brokering
were used to analyze the empirical data. A list of
themes were constructed from the data and presented
in the finding section as follow;
4 CASE DESCRITION
4.1 The Role of HEWs and VCHWs in
Health Service Provision and Data
Management
More than 34,000 female HEWs are deployed in
rural Ethiopia. They are mainly engaged in creating
health awareness and support communities to
practice health actions. According to the national
guideline of the health extension program, HEWs
are supposed to spend 70-75% of their working time
on home based and outreach health services
provision modalities (FMOH, 2005). This was also
confirmed by interviewed HEWs as follow: “We
stay at health posts in the morning and
evening…during the day time we go to home visiting
and outreach”. Two HEWs are assigned in most
visited villages thereby they divided their catchment
area into two and conduct their activities. When the
number of population exceeds 7500 in a specific
village, the district health office deploys three to
four HEWs.
Interviewed HEWs noted that, there are VCHWs
in each village (Got) who usually help them for their
duties. As they are working at health post, household
and outreach level, HEWs are mostly over stretched
in scattered settlement hence they appreciated the
help of VCHWs. At the beginning of their job
assignment, HEWs collected the baseline health data
from their respective catchment villages and
prepared map of their localities. In the visited health
posts, they have collected data with the help of
VCHWs. HEWs, on the other hand, offer formal and
informal trainings for VCHWs. They do have
monthly meetings, as well as, informal gatherings,
which were found to be good media for knowledge
sharing. Besides, some HEWs also share experience
with TBAs and develop their skill related to
managing normal delivery. TBAs give delivery
service as most births occur at home in rural
Ethiopia. Some HEWs have gained skill on how to
assist delivery with the help of TBAs. However,
some TBAs were not interested in establishing close
contact with HEWs.
While conducting home visiting, HEWs hold
some essential equipments and supplies including
their ordinary register book which they call “field
note-book”. HEWs use their field notes for two
purposes; for follow-up of the implementation of
health extension packages by households and to
copy the data captured in the field to a main register
for reporting. While providing health services, they
record in the field note-book the services they
provided, next appointment date and health actions
to be performed for the next visit. Afterwards,
during the following visit, they check whether
households perform the health extension packages
based on the given advice. HEWs gather and
compile the community health data continuously.
The main registers serve for data recording and
preparing monthly and quarterly reports. However,
these registers are not standardized thus the data
collected across health posts were not consistent
and
there is redundancy of data elements. HEWs, even
within the same district, use different types of
formats for reporting that sometimes affect
comparison of health facilities performances and
constrain experience sharing. With the compiled
data, HEWs prepare minimum wall charts with key
health targets and indicators and post them on walls
of the health posts. They usually use the data to
monitor the progress of their services and one can
easily look at the profile of their catchment areas at
health posts. HEWs discuss with the VCHWs on the
monthly performance report and design strategies to
improve the health service coverage.
In practice, there are two population data source
for the health sector at lower level. One is the
official number of population projected based on the
national census and the second is head counted by
HEWs and VCHWs in their catchment area. In line
with Damtew and Kaasbøll (2011), the findings of
KMIS2012-InternationalConferenceonKnowledgeManagementandInformationSharing
172

this study show that the target for health services
given to health posts from the districts is mostly
different and higher than head counted population by
HEWs and VCHWs. In some visited villages,
however, HEWs and their supervisors made effort to
resolve the ambiguity created by the discrepancy
between the official target and head counted
population. They rather follow the notion such as
“There should be not unvaccinated infant, no
household without pit latrine, and so forth.” than
being overwhelmed by the inflated target given from
district authorities. For instance, to ensure that every
child is vaccinated, HEWs and VCHWs search for
defaulters in their vicinity and their supervisors also
conduct random revisits in selected villages.
4.2 Knowledge Sharing Mechanisms
4.2.1 The Input from Pre-service Training of
HEWs
The pre-service training provides basic knowledge
for HEWs which helped them to perform their tasks.
For example, community health documentation is
one course given during pre-service training.
Interviewed HEWs mentioned that this course
helped them to sketch village maps manually, and to
collect and analyze health data. However, in the
HEWs training institutions, the proportion of
trainees was higher compared to the number of
teachers and teaching facilities that challenged the
teaching learning process. Scarcity of supplies, such
as demonstration materials and standardized data
collection tools, and inadequate practical sessions
compromised the quality of pre-service training.
Lecturing was the main method of instruction in
HEWs training schools, where the role of teachers
was offering lecture to trainees. The language barrier
was highlighted as a hindrance for transferring
knowledge. HEW teachers mentioned that the
instructional media is English and most HEWs
appeared to lack English language proficiency that
preclude them from being fully engaged. Moreover,
all books in HEWs training schools library, as well
as, some training, and recording and reporting
formats were prepared in English. This caused
difficulties to HEWs to absorb them effectively.
Interviewed HEWs also commented that the pre-
service training does not equip them effectively to
implement tasks included in the health extension
packages.
4.2.2 Knowledge Sharing among Peers
Some additional tasks are shifted to health posts
(HEWs) recently that require additional on-the-job
trainings. The FMOH with support from partners has
tried to organize and offer complimentary on-the-job
trainings for HEWs, such as “clean delivery training
and integrated refresher training”. Clean delivery
training is provided for one month. It is skill based
training, which enables HEWs to manage normal
delivery, recognize danger signs for early referral
and to capture the required information across the
continuum of care. They get training at relatively
well-equipped health centers and district hospitals,
which have better set up compared to rural health
posts. For instance, health centers have ready-made
register books for delivery, albeit HEWs are
supposed to modify bare exercise books, draw lines
and write titles to prepare delivery register books.
According to our observation, the maternity rooms
of rural health posts are also ill-equipped. Integrated
refresher training, on the other hand, includes all
tasks supposed to be performed by HEWs. It is
comprehensive training given for one month in three
phases. There are also other on-the-job trainings for
HEWs organized by the health sector and other
stakeholders, especially when the new health service
is initiated at the health post level.
HEWs and their supervisors noted that mostly
one of the two HEWs from the same health post
attends on-the-job trainings alternatively. Then the
other one share the knowledge from her friend. In
six of the visited health posts, one of the two HEWs
working in the same health post trained on providing
clean delivery. The training helps them to offer
delivery service and register births as ascertained by
the following quote; “After I received clean delivery
training, I can able to identify high risk mothers,
manage delivery, give newborn and postpartum
care, and register data properly. I also showed the
procedure to my colleague. We adapted the delivery
register and record all the required information.”
HEW who received in-service clean delivery
training.
Similarly HEW at one of the visited health posts
who was not trained on prevention of mother to
child transmission of HIV/AIDS said; I did not
receive formal in-service training on HIV testing.
However, I learned from my colleague who had
training and currently I am offering the service in
her absence.
In most visited health posts, the two HEWs work
together and interact closely, which created an
opportunity for knowledge sharing. They mentioned
that they keep materials which were provided from
trainings in their health post and use them jointly.
HEWs stated that they meet on monthly bases at the
AcceleratingHealthServiceandDataCapturingTroughCommunityHealthWorkersinRuralEthiopia-APre-requisiteto
Progress
173

nearest health center with their workmates from
neighboring health posts and health center (primary
health care unit meeting) and they discuss their
monthly performances, constraints and future
actions to improve performance based on the service
statistics. In some health centers, they organize the
meeting with special coffee ceremony that may
strengthen the social bond among staff and trigger
informal discussion that promote knowledge sharing
(see picture1).
Picture 1: Staff meeting with coffee ceremony at Chara
health center.
There is also quarterly performance review
meeting and experience sharing sessions of HEWs
with district health office and health center staffs, as
well as, biannual review meeting with zonal health
office and annual review meeting at the regional and
national level. Other partners may also take part in
those meetings. Experience sharing sessions take
place during these meetings where best performing
districts and HEWs communicate their best practices
with their colleagues that may improve performance
of the health sector. Experience sharing usually
takes place through written reports or oral
presentation that may illustrate knowledge transfer.
Awards also were given for selected HEWs and
districts owing to their good performance. However,
sometimes the ambiguity of target set for health
services cause tense argument to select best
performing health posts and HEWs.
4.2.3 Knowledge Sharing with the
Community: The Role of HEWs and
VCHWs as Knowledge Brokers
In their day-to-day practices, HEWs discuss,
converse and negotiate with households thereby help
them to practice health actions and enjoy healthy
lives. They play a role of knowledge broker by
facilitating knowledge communication between the
rural community and the new initiative by the health
sector (the health extension packages) through
continuous interaction with households. During
home visiting, HEWs acknowledge, praise and
encourage the family that performed the
recommended health activities based on their
suggestions. If the household didn’t perform the
recommended actions, they keep on motivating,
demonstrating and negotiating with the household to
accomplish the intended task for the following visit.
This action is continued until a specific family
practiced at least 75% of the health extension
packages and graduated. HEWs revealed that some
households accept the health advice and guidance
promptly and some may implement the health action
following their friends or neighbors. However, some
households may resist changing thereby continuing
the usual way of doing. Some others, on the other
hand, may revert back and stop executing healthy
practices for themselves and their children. For
instance, an interviewed HEW stated; “There are
families who consider “having many children as an
asset”; it is difficult to convince them to use
contraceptive methods for birth spacing and fertility
control”.
Some other families may yet consider traditional
practices as best for their family health. Hence,
HEWs stressed the importance of continuous
negotiation, and the exemplary role of VCHWs to
bring the requisite progress in health action. The
following excerpts from HEWs illuminate the
intermediary role of VCHWs; When there is a
defaulter client for a health service, we inform a
VCHW then s/he explains the absentee about the
advantage of the service…..converse and negotiate
thereby help the defaulters to resume the service.
There are about 18 VCHWs in our vicinity; their
presence helped most households to implement the
health extension packages.
Sometimes, the health sector and other partners
organize trainings that include VCHWs, thus they
propel clients to seek health service. For instance,
one VCHW during focus group discussion
mentioned “We received training about community
mobilization for HIV counseling and testing service:
afterwards we advise pregnant women in our village
to take voluntary counseling and testing for HIV
before delivery”.
5 DISCUSSION AND
CONCLUSION
Our findings showed that HEWs provide basic
preventive, promotive and curative health services to
KMIS2012-InternationalConferenceonKnowledgeManagementandInformationSharing
174

rural households. Capturing and communicating the
community health data is also one of the major tasks
of HEWs as good health management highly relies
on accurate and relevant information to make health
services responsive to the demands of the
population. Meanwhile, knowledge sharing was
taking place during their day-to-day practices. In the
pre-service trainings of HEWs, the main mode of
instruction was lecture. It was mainly one way of
transferring information from sender to receiver,
which may fosters knowledge transfer according to
Carlile (2004). However, lack of the common syntax
between teachers and HEWs due to a language
barrier and shortage of facilities affected knowledge
transfer process negatively. Lack of discourse
because of the language problem also inhibited the
knowledge translation and transformation processes.
Interviewed HEWs stated that they did not get
sufficient knowledge and skill at their pre-service
training.
On the other hand, the experience sharing
sessions from best performing districts or HEWs to
others can indicate knowledge transfer from sender
to receiver through shared syntax. This resonates
with the knowledge transfer explanations by Argote
(1999) and Szulanski (1996). These authors
explained that knowledge transfer can occur when,
for example, a unit communicates with another unit
about a practice that it has found to improve
performance. Carlile (2004) explained how
transferring knowledge through shared syntax is
unproblematic. In this study, experience sharing
sessions among the health staff were found crucial
for knowledge sharing. The findings of the study
also showed that HEWs and VCHWs discuss,
converse and interpret the meaning of performance
reports thereby create common syntax. They
translate the meaning of performance reports in a
sense making way to their specific situation. HEWs
and their supervisors also make dialogue during
meetings and supportive supervisions, and create
common understanding. For example, to reconcile
the discrepancy created by the difference between
the official target and head counted population by
HEWs and VCHWs, they discussed and created
common syntax such as “there should be not
unvaccinated infant” to ensure every child got
vaccines. This process requires creating new
agreements through dialogue and collaboration
across a semantic boundary.
In their day-to-day practices, the two HEWs
assigned in the same health post interact with each
other thus share knowledge. They bring new
concepts and knowledge from in-service trainings,
and they converse each other and negotiate to create
syntactic, semantic and pragmatic understanding
among themselves. This may require changing of the
knowledge they currently use. For instance, after
taking clean delivery training, HEWs disregarded
the previous register for delivery and prepared new
register based on the new knowledge they acquired
from the training.
According to Carlile (2002), the knowledge a
group currently use may create problem when
novelty arises. In our study, the rural households
may have their own knowledge and ways of doing to
keep their family health, for instance, they may
follow traditional practices. The innovative health
extension package is a new initiative designed by the
health authorities to improve health status of rural
dwellers. The finding of this study showed the
knowledge that households used preclude them to
practice new actions in the health extension
packages. HEWs and households are specialized in
different knowledge domains and they have many
dependencies in completing a task, hence the
boundary is complex (pragmatic). The dependencies
between HEWs and households happen from the
need of their joint input to implement the health
extension packages. HEWs facilitate the
implementation of the health extension packages by
full participation of the rural households. As
(Carlile, 2004; 2002) put it, communicating
knowledge between people with different knowledge
domain and high dependency face pragmatic
boundaries that require close interaction and
negotiating of conflicting interests. Therefore, it was
not easy to transform the existing knowledge of the
rural community to accommodate the new health
initiatives.
In summary this paper has addressed processes
of communicating knowledge related to the health
extension packages and the community health data,
across syntactic, semantic and pragmatic boundaries
among public health actors in the context of a
developing country. From the case description, it
can be concluded that knowledge communication of
HEWs with their teachers, peers, VCHWs, TBAs,
supervisors and the community needed different
processes
. For example, experience sharing sessions
during meetings denoted knowledge transfer through
shared syntax. HEWs made dialogue with VCHWs
and their district supervisors thereby created shared
meanings across semantic boundaries. Pragmatic
boundaries were faced between HEWs and rural
households because of the difference in their domain
specific knowledge and high dependency to
accomplish the task related to the health extension
AcceleratingHealthServiceandDataCapturingTroughCommunityHealthWorkersinRuralEthiopia-APre-requisiteto
Progress
175

packages. This needed close interaction and
negotiation to transform the current knowledge of
rural households.
The findings also showed that some households
slip-back from implementing new ways underlining
the need of further research to identify the reasons to
sustain the required change and improve the health
of the community.
The research questions outlined in the
introduction section are addressed as follow;
1. What is the role of HEWs and VCHWs as
knowledge brokers to facilitate the implementation
of the innovative health extension packages by rural
households?
HEWs continuously communicate the new
knowledge (health extension packages) with
households. They repeatedly converse, negotiate and
renegotiate with households to influence them to
transform their current knowledge and practice.
Their efforts continue until the families accept the
advice and implement the health initiative.
Meanwhile, the undertaking of HEWs to advance
knowledge communication across pragmatic
boundary was intensified by the efforts of VCHWs.
Both HEWs and VCHWs can take the role of
knowledge brokers who are facilitating the
communication and use of knowledge regarding the
health extension packages. As to Sverrisson (2001),
they facilitate knowledge communication and use
between the source of knowledge (health extension
packages) and potential users (rural households).
New health services are introduced to rural Ethiopia
and as novelty increases, the gap at the boundary
grows (Carlile, 2002). Meanwhile, the knowledge
brokering role of HEWs and VCHWs will continue
to close the gap that emerged as a result of novelty.
Theoretically, the study contributes to the 3-T
framework (Carlile, 2002; 2004) by identifying the
role of HEWs and VCHWs as knowledge brokers
that strengthen the four characteristics of a boundary
process: establishes a shared language; provides a
means of specifying differences and dependencies;
facilitates jointly transformation of knowledge and
multiple interactions. The knowledge brokering role
of HEWs and VCHWs was noticeable throughout
the four characteristics of a boundary process. They
make dialogue and multiple interactions with
households thereby help the families to transform
their knowledge and follow the new health
initiatives in the health extension package.
2. How can knowledge communication regarding
the health extension package be facilitated across
boundaries?
The findings of this study have shown the
knowledge communication process across
boundaries in the efforts of expanding the health
extension packages, and capture and compile
community health data. The study also identified
constraints that preclude knowledge communication
across syntactic, semantic and pragmatic boundaries.
For instance, shortage of resources and language
barriers has affected the knowledge transfer process
at HEWs pre-service trainings. The obsolete target
also imposed a challenge on sharing and
multiplication of good experiences during meetings.
The collaboration and social network were also
hindered by lack of confidence and interest as seen
by absence of communication between HEWs and
some TBAs. The following recommendations are
proposed to facilitate the implementation of the
health extension packages and to make the context
more conducive to knowledge communication;
Provide Essential Resources to HEWs Training
Schools; HEWs training schools should be equipped
with essential teaching facilities to facilitate the
teaching-learning process.
Appropriate Target Setting Procedure; there is a
need to follow apt target setting procedure for health
services to increase understanding among the health
staff and other stakeholders.
Availability of Standardized Data Collection
Tools; appropriate supplies and standardized data
collection tools should be made available at health
posts for proper recording and reporting.
Training for Community Volunteers; providing
training to community volunteers (VCHWs and
TBAs) is required for boosting their confidence and
work motivation that increase service coverage.
While the analysis of this study has been drawn
from the findings of the public health sector in
Ethiopia, the study has also broader implication for
other disciplines and contexts where knowledge
sharing is crucial. Therefore, more comprehensive
studies are recommended in different settings to
strengthen the findings of this study.
ACKNOWLEDGEMENTS
The field work for the study was sponsored by the
Norwegian Research Council to which we are
grateful. We are also grateful to participants of the
study who spent their spare time for the study.
KMIS2012-InternationalConferenceonKnowledgeManagementandInformationSharing
176

REFERENCES
Argote, L., 1999. Organizational learning: Creating,
retaining, and transferring knowledge. Norwell, MA:
Kluwer.
Carlile. P. R., 2002. A pragmatic view of knowledge and
boundaries: Boundary objects in new product
development. Organ. Science. 13: 442-445.
Carlile, P. R., 2004. Transferring, translating and
transforming: an integrative framework for managing
knowledge across boundaries. Organization Science.
15. 555-568.
Chowdhury, A., Chowdhury S., Islam M., Islam A.,
Vaughan J., 2009. Control of tuberculosis by
community health workers in Bangladesh. The
Lancet.; 350 (9072):169–172.
Daferdst, R. L., Lengel, R. H., 1984. Information
Richness: A New Approach to Managerial
Information Processing and Organizational Design,
Research in Organization Behavior. Greenwich.
CT:JAI Press, P.6.
Damtew, Z., Kaasbøll, J., 2011. Target Setting procedures
for Immunization Services in Ethiopia: Discrepancies
between Plans and Reality. Journal of Health
Management. 13(1): 39-58.
Dobbins, M., Robeson, P., Ciliska, D., Hanna, S.,
Cameron, R., O'Mara, L., DeCorby, K., Mercer, S.,
2009. A Description of a Knowledge Broker Role
Implemented As Part of a Randomized Controlled
Trial Evaluating Three Knowledge Translation
Strategies. Implementation Science. 4: 23.
Federal Ministry of Health, 2005. Health Sector Strategic
Plan (HSDP-III) 2005/6-2009/10. Ethiopia.
Hargadon, A. B., Ed. 2003. How Breakthroughs Happen,
The Surprising Truth about How Companies Innovate.
Boston, Massachusetts.
Howells, J., 2006. Intermediation and the role of
intermediaries in innovation. Research Policy. 35(5):
715.
Jackson, N., 2003. Introduction to brokering in higher
education. In N. Jackson (Ed.), Engaging and
changing higher education through brokerage.
Aldershot , UK: Ashgate.
Meyer, M., 2010. The Rise of the Knowledge Broker.
Science Communication. 32: 118-127.
Otieno, C. F., Kaseje, D., Ochieng, B. M., Githae, MN.,
2012. Reliability of Community Health Worker
Collected Data for Planning and Policy in a Peri-
Urban Area of Kisumu, Kenya. J. Community Health.
37(1): 48-53.
Soy, S. K., 2006. The Case Study as a Research Method,
http://www.gslis.utexas.edu /~ssoy uses
users/l391d1b.htm “accessed on 01/03/2010”.
Sverrisson, A., 2001. Translation networks, knowledge
brokers and novelty construction: pragmatic
environmentalism in Sweden. Acta Sociologica. 44:
313-327.
Szulanski, G., 1996. Exploring external stickiness:
Impediments to the transfer of best practice within the
firm. Strategic Management Journal. 17: 27-43.
van Kammen, J., de Savigny, D., Sewankambo, N., 2006.
Using Knowledge Brokering to Promote Evidence-
Based Policy Making: the Need for Support Structure.
Bulletin of the World Health Organization. 84: 608-
612.
Walsham, G., 2006. Doing Interpretive Research.
European Journal of Information Systems. 15: 320-
330.
Ward, V., House, A., and Hamer, S., 2009. Knowledge
Brokering: The Missing Link in the Evidence to
Action Chain? Evidence and Policy: A Journal of
Research.
Ziam, S., Landry, R., and Amara, N., 2009. Knowledge
Brokers: a Winning Strategy for Improving
Knowledge Transfer and Use in the Field of Health.
International Review of Business Papers 5: 491-505.
AcceleratingHealthServiceandDataCapturingTroughCommunityHealthWorkersinRuralEthiopia-APre-requisiteto
Progress
177
