
SCRIPT: Tele-robotics at Home
Functional Architecture and Clinical Application
G. B. Prange
1
, H. J. Hermens
1
, J. Schäfer
2
, N. Nasr
3
, G. Mountain
3
, A. H. A. Stienen
4
and
F. Amirabdollahian
5
1
Roessingh Research and Development, Roessinghsbleekweg 33b, Enschede, The Netherlands
2
User Interface Design, Ludwigsburg, Germany
3
School of Health and Related Research, University of Sheffield, Sheffield, U.K.
4
Department of Biomechanical Engineering, University of Twente, Enschede, The Netherlands
5
Adaptive Systems Research Group, The University of Hertfordshire, Hertfordshire, U.K.
Keywords: Remote Treatment, Remote Monitoring, Decision Support, Rehabilitation Robotics, Upper Extremity,
Hand, Stroke.
Abstract: After the event of a stroke, patients have at least 12 months during which their brains are highly susceptible
to the benefits of neuro-rehabilitation treatments. On the other hand, due to the high costs of clinical neuro-
rehabilitation, post-stroke treatments are limited in all countries to only a few weeks after the stroke event.
Hence, any system aimed at prolonging neuro-rehabilitation at patients’ homes, and with low-cost
treatments, addresses a major issue in the current health management systems. Recent developments have
revealed a great potential for robotic devices delivering repetitive training to improve arm function after
stroke, thus facilitating a high intensity and a large number of repetitive training. The SCRIPT project aims
to develop robotic technologies for the home as it would enable self-administration of more intense and
more frequent exercises, by enabling hand and wrist exercise that have great potential for contribution to
personal independence. Remote management and support of the patient is incorporated through a
communication platform that supports the remote adjustment of the therapy program. In this way, the
patient can exercise at home, while the exercise is remotely supervised without increasing therapist time,
while reducing the frequency of hospital or clinics visits.
1 INTRODUCTION
Functional recovery from stroke demands a long
period of physical and often cognitive rehabilitation.
Research into motor relearning and cortical
reorganization after stroke has provided a
neurophysiological basis for key aspects that
stimulate restoration of arm function (Schaechter,
2004; Krakauer, 2005). These key aspects include
high training intensity, active initiation and
execution of movements, and application of
functional exercises. Technological innovations
provided an opportunity to design interventions that
take many key aspects for stimulation of motor
relearning into account, of which rehabilitation
robotics is a well-known example. With such a
device, the required amount of movement support
can be provided, thereby allowing active practice
when this is not possible otherwise. This increases
the potential to train intensively, with the patient’s
active contribution to functional exercises.
The application of rehabilitation robotics has
been shown to be effective for the hemiparetic arm
(Prange, 2006; Kwakkel 2008; Mehrholz 2008).
However, transfer of robotic training effects to
activities in daily life is limited, as is observed for
most interventions in stroke rehabilitation, including
conventional therapy (Wagenaar, 1991).
Contemporary robot-aided therapy focuses mainly
on the proximal arm, and results in improvements in
the proximal arm only, without generalization to the
wrist and hand (Prange, 2006). This is while wrist
and hand play a major role in a person’s functional
independence. In order to maximize independent use
of the upper extremity in daily life, it is important to
include functional practice of the wrist and hand.
58
Amirabdollahian F., Schäfer J., Stienen A., Mountain G., Nasr N., Hermens H. and Prange G. (2012).
SCRIPT: Tele-robotics at HomeFunctional Architecture and Clinical Application.
In Proceedings of the Sixth International Symposium on e-Health Services and Technologies and the Third International Conference on Green IT
Solutions, pages 58-63
DOI: 10.5220/0004474100580063
Copyright
c
SciTePress

In the setting of the rehabilitation centre,
intensive training of arm and hand is supervised by
highly skilled professionals. However, the time that
can be spent on training in such intramural settings
is limited. Due to the high costs of clinical neuro-
rehabilitation, post-stroke treatments are limited to
only a few weeks with limited treatment resources
after the stroke event in many countries. Hence, any
system aimed at prolonging neuro-rehabilitation out
of the clinics, i.e. at patients’ homes and with low-
cost treatments, addresses a major issue in the
current health management systems.
While there is growing evidence that
rehabilitation technologies are beneficial to the
patients’ recovery of functional and motor outcome
(i.e., Prange, 2006; Kwakkel, 2008; Mehrholz,
2008), the uptake of these technologies has been
slow. This is thought to be caused by the lack of
stronger clinical evidence for usefulness, adherence
of carers/clinicians, lack of platforms designed along
clinically useful practice, limitations on post-
discharge practice frequency based on service or
motivation limits, absence of platform flexibility,
cost and weakness in addressing interoperability
issues among healthcare systems in the EU.
The SCRIPT (Supervised Care & Rehabilitation
Involving Personal Tele-robotics) project aims to
address several of these important issues: using
robotic technologies at home as it would enable self-
administration of more intense and more frequent
exercise, by enabling hand and wrist exercise that
have great potential for contribution to personal
independence. This is the concept of
telerehabilitation considered by many as the future
(Hermens, 2008).
However, telerehabilitation is still in its infancy.
In a recent review (Johansson, 2010), only very
limited amount of ICT-supported treatments were
available. Of the nine studies included in the review,
four studies focused on a teleconsultation service for
stroke patients. With respect to technology-
supported telerehabilitation, only three studies were
found: two utilizing the same virtual reality-based
system that provided motor tasks to the patients and
only one study, originating from the European HCad
and HelloDoc projects, utilising a sensitized exercise
table with synchronous video teleconsultation to
enable supervised arm/hand exercising at home. One
of the aspects reflecting the present immaturity of
telerehabilitation concerns the unavailability of a
decision support system. In order to make large scale
clinical application possible and to make such
systems cost-effective, it is required that a decision
support system is in place that supports clinical
decision making by doing a smart analysis of the
physiological and biomechanical data in its proper
context.
The aim of the present paper is to present the
functional architecture and future clinical directions
of the SCRIPT tele-robotics platform, which is
targeted at improving arm function after stroke by
enabling home-based, robot-supported arm and hand
training. Since designing such an interactive system
often doesn’t meet the criteria needed for a usable
system, user-centred design methods are applied
from the start of the development of the interactive
system (Abras, 2004). By applying four steps:
identifying needs and user requirements, developing
alternative designs, building interactive versions,
evaluating the different options (Sharp, 2006), the
end user is allowed to shape the design of the
SCRIPT tele-robotics system.
2 FUNCTIONAL
ARCHITECTURE
The SCRIPT project will create a system,
progressing beyond the present state of art, in a
number of aspects. The goal of developing a home
usable device for chronic stroke patient poses many
challenges. At its heart, safety during robotic
interaction is an elemental consideration. Passive-
actuation is chosen due to its superior and inherent
safety and importantly, its implications on reducing
cost. In addition, there is evidence that passive-
actuation can be as beneficial as active actuation
(Amirabdollahian, 2007). Therapeutic scenarios
detailed in user-driven design framework are to be
implemented in the prototype devices as meaningful
human-robot interaction. The idea is to identify and
tune, based on person’s capabilities, the percent
contribution required by the robot during human-
robot interaction. Figure 1 shows the functional
blocks of the complete system.
The project considers two different user
interfaces for the interaction with the system: one for
the patient and one for the clinician. The user
interface for patients provides motivational and
engaging content with an easy to use front end
(which supports multiple languages for interaction).
Patients’ therapy is facilitated using a series of
therapeutic games. In addition the system will allow
on-line support, assessment of instructional videos
and user friendly and motivating monitoring
functions of the progress made.
SCRIPT: Tele-robotics at Home - Functional Architecture and Clinical Application
59
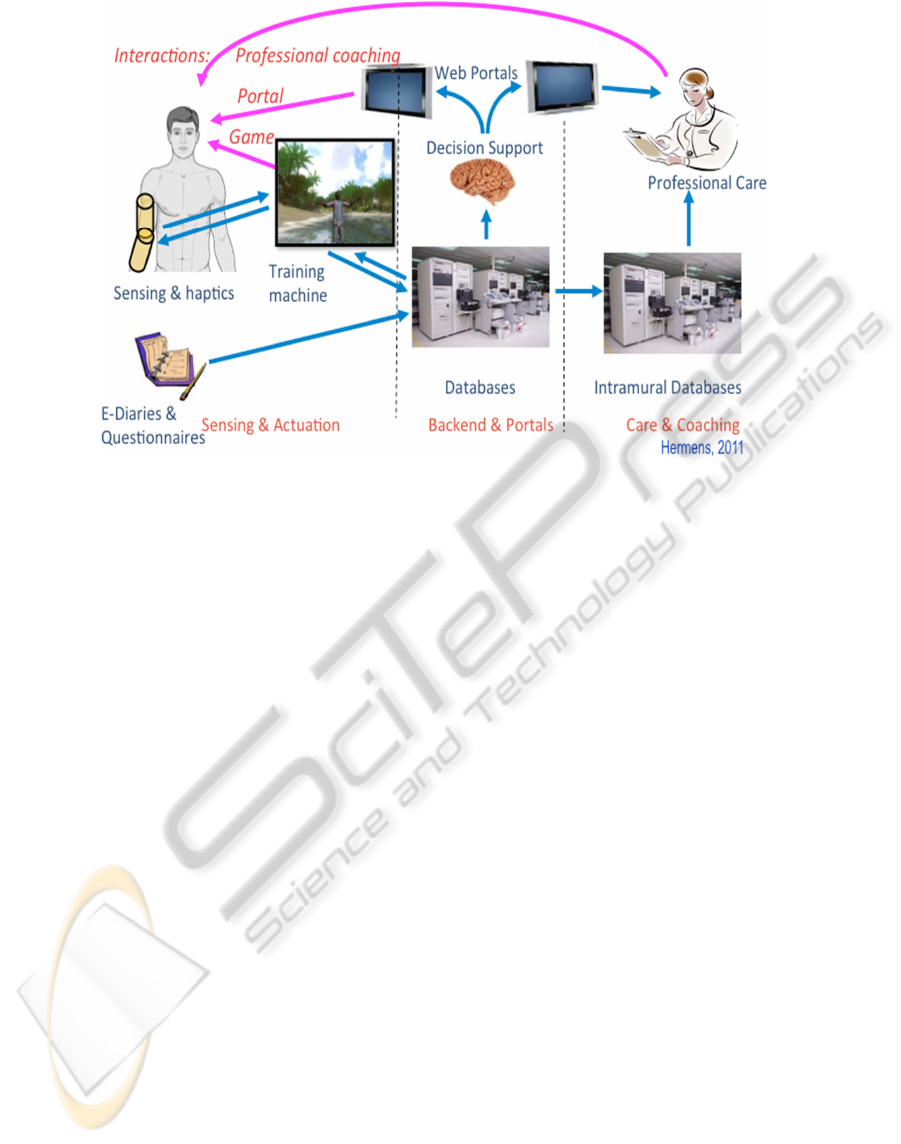
Figure 1: Functional architecture of SCRIPT system.
The user interface used by the clinicians will
include different features, required to remotely
manage or observe, and in the case of active device
provides a chance for remote tuning of the device.
Clinical users require to observe progress in a range
of different aspects but not necessarily using the
same progress indicators as seen by the patients.
Automated data collection will be supported on
the outcome variables of the exercises, subjective
data from questionnaires and diaries and
intermediate process variables for treatment. These
functions will be performed in a secure dependable
way, taking care that privacy and data integrity are
guaranteed. The training equipment generates large
quantities of data that cannot be monitored
continuously by the health care professional or by
the patient. A set of clinically relevant features will
be determined continuously and made available to
both the clinician and the patient. These will be
combined with contextual information and
reasoning, to result in a set of recommendations and
a comprehensive presentation of the most relevant
data.
2.1 Building Blocks
Considering the functional architecture of the
SCRIPT tele-robotics system, figure 2 displays its
building blocks. A short description of its main
components is presented below.
2.1.1 Robotic Device
The device consists of a commercially available
weight support mechanism (Saebo Mobile Arm
Support) on top of which a wrist and hand therapy
device is mounted. The device can be used for all
activities of daily living. The wrist and hand
component includes manipulation of wrist
flexion/extension and different grasping movements
with the thumb, fingers and palm of the hand.
Assist‐as‐needed is provided through passive and
active actuators, respectively springs and electric
motors. Combining passive with active actuators
provides an optimal balance between power output,
control opportunities and device weight. The
actuators and mounted sensors also allow for
interactive feedback and haptic object manipulation.
2.1.2 Adaptive Therapeutic
Human-robot-interaction
Therapeutic scenarios detailed in user-driven design
framework are to be implemented in the prototype
devices as meaningful human-robot interaction. To
do this, this block focuses on position lag and energy
transfer direction (from human to robot or vice
versa) towards benchmarking/guiding the interaction
between the person and the robot prototype. The
idea is to identify and tune, based on person’s
capabilities, the percent contribution required by the
robot during human-robot interaction. The under-
lying interaction is compared to established models
EHST/ICGREEN 2012
60
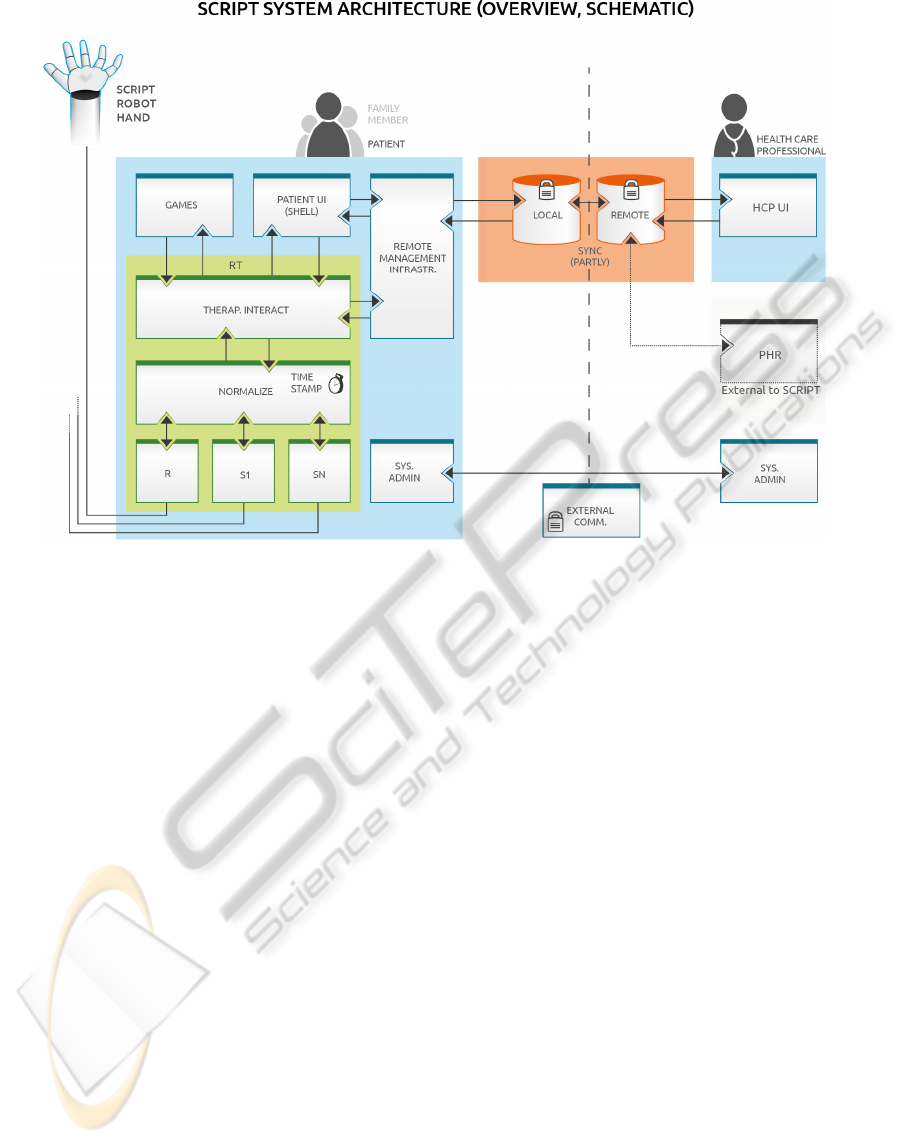
Figure 2: Building blocks of SCRIPT system.
such as minimum jerk (Hogan, 1984) providing
opportunities for new benchmarks for grasping.
Using these benchmarks, it is possible to adjust the
robot’s assistive or resistive forces automatically
providing an adaptive and therapeutic human-robot
interface.
2.1.3 Remote Interaction and Decision
Support
The sensor signals from the robotic device,
reflecting the human interaction during the game,
are sampled, processed and normalised to enable
real-time comparison with the pre-determined
therapeutic goals. A subset of the central database is
loaded in the local database at start-up, containing
patient history and specific game settings. During
the use of the SCRIPT system, new data is added to
the local database continuously and synchronised
with the main remote database. The data is also used
to generate reports to be included in the patient
health record.
A model will be developed that is able to
automatically process the sensor data in different
consecutive steps to obtain a set of dynamically
changing features. These will be combined with
contextual information and reasoning will result in a
set of recommendations and a comprehensive
presentation of the most relevant data.
2.1.4 User Interfaces
Portals will be developed that enable a
comprehensive and motivating presentation of the
data. This requires a very different presentation for
the patient and the clinician that coaches. Whereas
clinicians are used to interpreting graphs, this is
often not the case for the patient, so starting from the
user requirements (from the patient perspective)
special GUI’s have to be researched and developed.
In this way the loop will be closed at three
different levels, enabling adequate and efficient
monitoring and coaching: the patient gets direct
feedback during the exercise from the robotic
device, he is able to monitor his improvements via
the portal and he receives coaching from his care
professional, who is also able to monitor the
progress via the portal.
3 CLINICAL APPLICATION
3.1 Clinical Evaluation
The clinical study design applied in this project
involves two different types of evaluation,
underpinning technology development: Formative
Evaluation (FE) or user-engagement in design and
SCRIPT: Tele-robotics at Home - Functional Architecture and Clinical Application
61

system development and Summative Evaluation
(SE) or the evaluation of the finished (functioning)
product.
In Formative Evaluations, users of a technology
system can provide useful information during the
process of system development (Monk, 1993). Initial
engagement with the potential users of the system is
needed to create a clear understanding of the target
users and the context in which the users intend to
use the system. In the process of specification the
system is designed, developed and tested through an
iterative cycle in which the developers are able to
find out how easy/difficult the system is to use by
users and to help them understand what problems
the system poses and how these problems could be
improved. The outcome of evaluation is considered
and alterations made to the design for the next
iteration of the prototype. This set-up of formative
evaluations allows use and acceptance of the
developed systems to be evaluated in practical
situations.
The summative evaluation allows for assessing
whether use of self-administered tele-robotic devices
can influence improvement of arm and hand
function captured during home therapy. This is made
possible by recruiting volunteering patients at the
chronic stage of stroke recovery, and allowing them
to use the system at their comfort for a six-week
period. Patients are assessed clinically; prior to, after
and at two-month post-intervention using established
and validated clinical outcomes. This investigation
also allows validating usefulness due to involvement
of three user-evaluation centres (University of
Sheffield in the United Kingdom, San Raffaele
S.p.A. in Italy, Roessingh Research and
Development in the Netherlands) for each stage of
the evaluation. Analysis of the clinical outcomes, as
well as amount of use, intensity of training, usability
and user acceptance, allows for a comprehensive
analysis of the factors contributing to improved arm
and hand function and compliance to home-based
treatment.
At present, the SCRIPT project is in its initial
stages. The stage of user and system requirements
identification during FE is ongoing. In the next
stages of the project, these requirements will be
implemented during design of the SCRIPT system,
after which SE will be carried out.
3.2 Future Clinical Directions
The SCRIPT tele-robotic platform ultimately
enables application of robotic technologies at home.
This allows self-administration of more intense and
more frequent exercise, by enabling hand and wrist
exercise that have great potential for contribution to
personal independence. This is done by providing an
educational, motivational and engaging interaction,
which makes a therapy session more enjoyable while
having the capabilities to provide feedback to
patients (in support of relearning) and to the
healthcare professionals. To enable this, remote
management and support of the patient is
implemented, through a communication platform
that supports the remote adjustment of the therapy
program, thus reducing the frequency of hospital or
home visits. This is facilitated by incorporating
clinical workflows into user interfaces used by
patients and clinicians, while maintaining a
customisable and easy to operate front-end for users.
In this way, the patient can exercise at home, while
the exercise is remotely supervised.
4 CONCLUSIONS
Based on a multidisciplinary approach, the SCRIPT
tele-robotics system will be usable at stroke patients’
homes after their discharge from the hospital, in
order to improve personal independence. It provides
immediate feedback on user performance using a
decision support architecture. The feedback will be
provided to both the patient and the health care
professionals with in-depth considerations for
security and confidentiality. The SCRIPT tele-
robotics system will be beneficial to improve arm
and hand function of stroke patients, while reducing
hospital and home visits and having a large impact
on reducing hospital costs.
During design and development, the system is
adapted to user requirements. The project evolves
from focus on user feedback during technology
development (presently ongoing) and user
acceptance during initial phases of try-out and
testing, to analyses of added value and impact of
such services applied at the patient’s home, for
additional important insight in contributing factors
to success of home application.
ACKNOWLEDGEMENTS
All partners of the SCRIPT consortium are
acknowledged for their contributions and valuable
input to the project: University of Hertfordshire (F.
Amirabdollahian, K. Dautenhahn, S. Gorham, A.
Basteris, N. Rahman), RU Robots (G. Pegman, J.
EHST/ICGREEN 2012
62

Foley), University of Sheffield (G. Mountain, N.
Nasr), University of Twente (A. Stienen, S. Ates),
Roessingh Research and Development (J. Buurke,
G. Prange, S. Nijenhuis, H. Hermens, H. Rietman),
MOOG BV (P. Lammertse), San Raffaele S.p.A. (A.
Cesario, L. Rossini), User Interface Design (J.
Schäfer).
The SCRIPT (Supervised Care &
Rehabilitation Involving Personal Tele-robotics)
project is partially funded under grant 288698 of the
7
th
framework of the European Commission (theme
3; Information and Communication Technologies).
REFERENCES
Amirabdollahian, F., Loureiro, R., Gradwell E., Collin C.,
Harwin W., Johnson G., 2007. Multivariate analysis of
the Fugl-Meyer outcome measures assessing the
effectiveness of GENTLE/S robot-mediated stroke
therapy. J Neuroeng Rehabil 4: 4.
Hermens, H. J., Vollenbroek-Hutten, M. M. R., 2008.
Towards remote monitoring and remotely supervised
training. Journal of Electromyography and
Kinesiology 18(6): 908-919.
Hogan, N., 1984. An organizing principle for a class of
voluntary movements. Journal of Neuroscience 4:
2745-2754.
Johansson, T., Wild C., 2010. Telerehabilitation in stroke
care - a systematic review. J Telemed Telecare:
jtt.2010.100105.
Krakauer, J. W., 2005. Arm function after stroke: From
physiology to recovery. Seminars in Neurology 25(4):
384-395.
Kwakkel, G., Kollen, B. J., Krebs, H. I., 2008. Effects of
robot-assisted therapy on upper limb recovery after
stroke: A systematic review. Neurorehabil Neural Rep
22(2): 111-121.
Mehrholz, J., Platz, T.,, Kugler, J., Pohl, M., 2008.
Electromechanical and robot-assisted arm training for
improving arm function and activities of daily living
after stroke. Cochrane Database Syst Rev (4):
CD006876.
Monk, A., Wright, P., Haber, J., Davenport, L., 1993.
Improving your human-computer interface, Prentice
Hall.
Prange, G. B., Jannink, M. J. A., Groothuis-Oudshoorn, C.
G. M., Hermens, H. J., Ijzerman, M. J., 2006.
Systematic review of the effect of robot-aided therapy
on recovery of the hemiparetic arm after stroke. J
Rehabil Res Dev 43(2): 171-183.
Schaechter, J. D., 2004. Motor rehabilitation and brain
plasticity after hemiparetic stroke. Progress in
Neurobiology 73(1): 61-72.
Wagenaar, R. C., Meijer, O. G., 1991. Effects of Stroke
Rehabilitation: a critical review of the literature.
Rehabilitation Science 4(3): 61-73.
SCRIPT: Tele-robotics at Home - Functional Architecture and Clinical Application
63
