
Flexible Array of Active Concentric Ring Electrodes for Surface
Bioelectrical Recordings
Application to Non-invasive Recordings of EEnG
J. Garcia-Casado
1
, V. Zena
1
, G. Prats-Boluda
1
, Y. Ye-Lin
1
and E. Garcia-Breijo
2
1
Grupo de Bioelectrónica, I3BH-UPV, Camino de Vera SN, Valencia, 46022, Spain
2
Centro de Reconoc. Molec. y Desarrollo Tecnológico. Ud Mixta UPV-UV,Camino de Vera SN, Valencia, 46022, Spain
Keywords: Ring Electrode, Laplacian Recording, Non-invasive Myoelecrical Recording, Electroenterogram.
Abstract: The estimation of laplacian potential on the body surface obtained by means of concentric ring electrodes
can provide bioelectrical signals with better spatial resolution and less affected by bioelectrical interferences
than monopolar and bipolar recordings with conventional disc electrodes. These ringed electrodes are
usually implemented on rigid substrates which cannot adapt to body surface curvature. In this paper an array
of flexible concentric ring electrodes for non-invasive bioelectrical activity recordings is presented. The
array contains three tripolar electrodes in bipolar configuration (TCB, inner disc and external ring are
shorted) which is suitable for body surface mapping. A preconditioning circuit module is directly connected
to the electrode array to perform a first stage of filtering and amplification as close as possible to the
recording area. Simultaneous recordings of intestinal myoelectrical activity (electroenterogram, EEnG) by
means of the flexible array of ringed-electrodes and by disc electrodes with gel were carried out in healthy
volunteers in fast state. Signals from the developed array of electrodes presented lower electrocardiographic
and respiratory interference than conventional bipolar recordings with disc electrodes. The small bowel’s
slow wave myoelectrical activity can be identified more easily in the ringed-electrodes recordings.
1 INTRODUCTION
1.1 Bioelectrical Laplacian Recordings
Surface recordings of bioelectrical signals are
usually recorded by means of disc electrodes in
bipolar or unipolar configuration. In the first method
the potential difference between a pair of electrodes
is measured. In the latter method the potential of
each electrode is compared either to a neutral
electrode or to the average of several electrodes. One
drawback of using conventional disc electrodes in
bioelectrical surface recordings is their poor spatial
resolution which is mainly caused by the blurring
effect of the different conductivities of the volume
conductor (Bradshaw et al., 2001). In this respect,
Laplacian has been shown to reduce the smoothing
effects caused by the volume conductor and to
increase the spatial resolution in localizing and
differentiating multiple dipole sources (Wu et al.,
1999); (Besio et al., 2006).
There are different approaches to estimate the
laplacian potential on the body surface. The first
ones to be used were discretization techniques like
the one introduced by Hjorth as early as in 1975
(Hjorth, 1975). In that study, the laplacian of the
EEG signal was estimated as the difference between
the average potential of four disc electrodes in the
form of a cross and the potential of a fifth disc
electrode placed in the center of the cross. In the late
80s, analytic solutions to estimate the laplacian of
the surface potential were proposed in order to
reduce discretization errors (Perrin et al., 1987).
These are complex discrete computational
techniques, generally not suitable for real-time
applications. Nevertheless, laplacian potential can
also be directly estimated by means of concentric
ring electrodes in tripolar, bipolar or tripolar in
bipolar configuration (TCB, where the outer ring
and the center disc were electrically shorted) (Lu
and Tarjan, 1999); (Besio et al., 2006); (Koka and
Besio, 2007).
TCB ring electrodes have already been used to
estimate the Laplacian potential of bioelectrical
signals such as the electrocardiogram (ECG),
21
Garcia-Casado J., Zena V., Prats-Boluda G., Ye-Lin Y. and Garcia-Breijo E..
Flexible Array of Active Concentric Ring Electrodes for Surface Bioelectrical Recordings - Application to Non-invasive Recordings of EEnG.
DOI: 10.5220/0004196500210027
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2013), pages 21-27
ISBN: 978-989-8565-34-1
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

electroencephalogram (EEG), electroenterogram
(EEnG) and the electrohysterogram (EHG), so as to
increase the spatial resolution of and the signal
quality of conventional surface potential recordings
(Li et al., 2005); (Prats-Boluda et al., 2011); (Koka
and Besio, 2007). These electrodes are usually active
since the signals sensed by concentric ring
electrodes in laplacian configuration are weaker than
the ones obtained my conventional monopolar or
bipolar recordings, and the output impedance is
bigger. Nevertheless, the ringed-electrodes used in
these studies were developed on rigid substrates like
printed-circuit boards, what can provoke a poor
skin-to-electrode contact and discomfort to the
patient.
Therefore, the aim of this study is to develop
concentric ring electrodes on a flexible substrate to
join the advantages of laplacian recordings with the
comfort and better adaptation to the body surface
curvature of conventional disposable disc electrodes.
1.2 Intestinal Myoelectrical Activity
The study of intestinal motility is an outstanding
field in gastroenterology due to the fact that
abnormal motility patterns are related with several
intestinal pathologies (Quigley, 1996). This is the
case in irritable bowel syndrome, intestinal
obstruction, paralytic ileus, and bowel ischemia. The
main problem in monitoring intestinal activity is the
difficult anatomic access, hence most methods of
studying this activity are considered to be invasive.
One possible solution would be the recording of
intestinal myoelectrical activity on abdominal
surface. This signal is named Electroenterogram
(EEnG) and it is composed of two waves: slow
waves (SW) and spike burst (SB). The former are
periodical, omnipresent electrical potentials that
regulate the maximum rate of intestinal muscle
contractions. The latter are fast action potentials
which are located in the plateau of the SW. They are
only present when contractions appear. Whereas SW
are related to the frequency and propagation velocity
of the contractions (Weisbrodt, 1987), SB determine
the presence and the intensity of the contractions.
The frequency of the SW changes along the small
intestine from about 12cpm at duodenum to
8cpm at ileum (Fleckenstein and Oigaard, 1978)
There are few studies about abdominal surface
recordings to identify the EEnG in humans (Chen et
al., 1993); (Chang et al., 2006); (Prats-Boluda et al.,
2007); (Prats-Boluda et al., 2011). The main reason
is that human EEnG is a very weak signal, which is
severely attenuated especially in the SB frequency
range, because of the insulation effects of the
abdominal layers and spatial filtering (Garcia-
Casado et al., 2006). Surface EEnG is also very
sensitive to physiological interferences such as ECG
and respiration, being difficult to identify the SW
component of the EEnG by visual inspection of
abdominal surface recordings. The ECG spectral
frequency range overlaps the SB frequency range,
therefore it is necessary to eliminate it from
abdominal recordings to identify the SB component
of the EEnG (Garcia-Casado et al., 2006). As
regards to respiration interference, the typical
breathing frequency range (12cpm to 24cpm) is very
close to the frequency of the SW (8cpm to 12cpm),
so it is not possible to use conventional filters to
remove this interference.
Laplacian recordings of the EEnG by means of
active concentric ring electrodes on rigid substrates
have proven to enhance signal quality in comparison
to conventional monopolar and bipolar recordings
with disc electrodes. Therefore, a second objective
of this work is to test and study the possible benefits
of the flexible concentric ring electrodes to be
developed in this study, on the surface recordings of
the EEnG.
2 MATERIAL AND METHODS
2.1 Active Electrode Array Design and
Implementation
2.1.1 Sensing Part
In this work it has been decided to design an array of
electrodes rather than an individual electrode for
surface bioelectrical recordings, since this kind of
recordings are usually multichannel and moreover
laplacian recordings are often used for body surface
mappings. Specifically an array of three concentric
ring TCB active electrodes was developed. The
sensor is made out of two parts: a disposable sensing
part with three TCB electrodes and a reusable
battery-powered signal conditioning circuit. Each of
the three sensing electrodes consist of an inner disc
and two concentric rings in bipolar configuration i.e.
the disc and the outer ring are shorted together
(TCB).
The outer diameter of the external ring was set to
24mm which is a compromise between bigger
electrodes that would yield signals of higher
amplitude and smaller electrodes that would provide
better spatial resolution. The rest of dimensions of
the electrode are designed considering the following
BIODEVICES2013-InternationalConferenceonBiomedicalElectronicsandDevices
22
criteria:
- The sum of the areas of the outer ring (Aout) and
the inner disc (Ain) should be equal to the area of
the middle ring (Amid) so as to provide similar input
impedances, improving the common mode rejection
ratio.
- The distance between the inner disc and the
middle ring should be the same as the distance
between the middle and outer rings to reduce
common mode interferences.
Other issues such as a minimum recording area of
50mm
2
and the limitations of the implementation
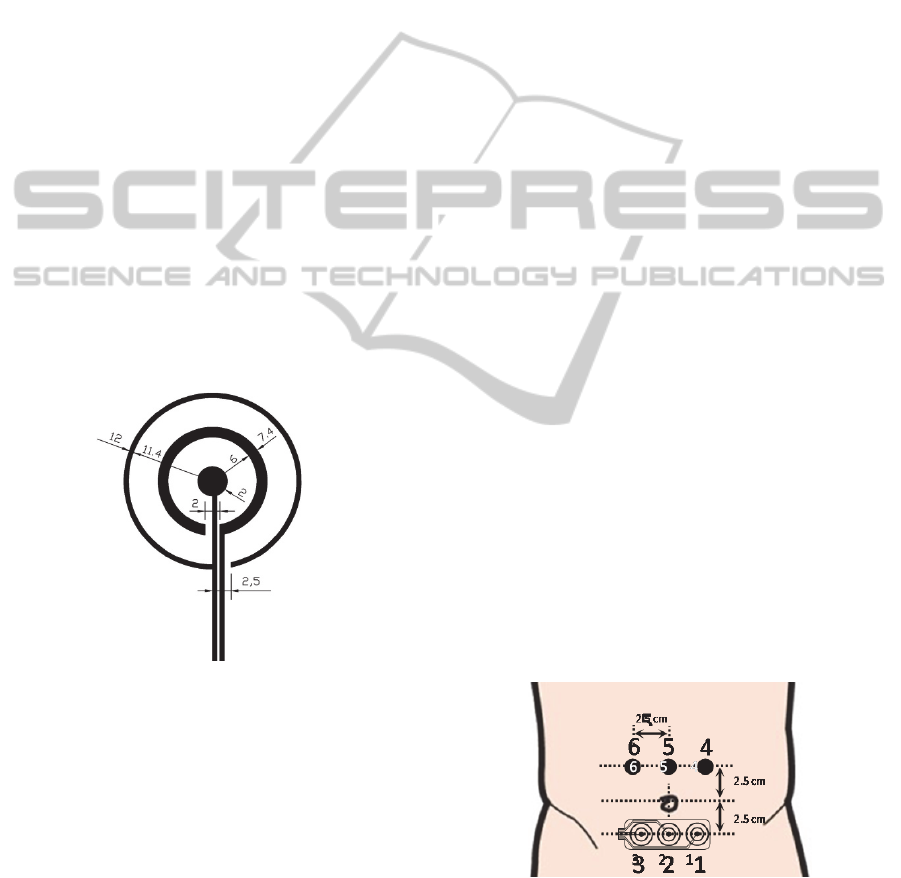
technique were considered. The dimensions of each
ringed-electrode of the array are shown in figure 1.
As it can also be appreciated in this figure, an
opened-ring version has been designed in order to
avoid shorts in the layout of the traces from the
electrodes to the connectors. The flexible electrode
array was implemented by screen-printing
technology on polymer substrates. Specifically, a
biocompatible silver paste was printed (Dupont 5064
Silver conductor, thickness 17 μm) on Polyester
Melinex ST506 substrate (thickness 175μm). The
serigraphy was made by using an AUREL 900 High
precision screen stencil printer. Cured period of inks
was 130ºC for 10 minutes.
Figure 1: Dimensions (mm) of the concentric ring
electrode to be implemented in the array.
2.1.2 Signal Conditioning Part
As stated before, signals from concentric ring
electrodes are of very low amplitude, especially in
the cases that the bioelectrical signal to be recorded
on the body surface is weak. Therefore it is highly
recommended to include an amplification stage as
close as possible to the sensing electrode.
In this work a battery-powered conditioning
circuit was developed and directly connected to the
electrode array. Precisely, a 12 bias (only six are
used) flexible-flat-cable-to-flexible-printed-circuit
connector (TE Connectivity/AMP-1-84953-2
FFC/FPC) was used for the connection. The circuit
is composed of a preamplifier (gain 31.9), followed
by a coupling circuit (high pass cut off frequency
0.05Hz) and an additional differential amplification
stage (gain 106.1) for each of the three TCB
electrodes of the array. Specifically, the integrated
circuits used were 3 OP747 for the operational
amplifiers and 3 AD620 for the instrumentation
amplifiers. The signal conditioning circuit weights
less than 15 grams. Its main electrical characteristics
were experimentally checked and are shown in the
next section.
2.2 Signal Recordings
Five recording sessions, of about three hours, were
carried out in healthy volunteers in fast state (>8h).
Subjects were in a supine position inside a Faraday
cage. Firstly the abdominal body surface was
exfoliated to remove dead skin cells to reduce
contact impedance. The abdominal surface was also
shaved in male subjects.
Figure 2, shows the location of electrodes for the
EEnG recordings. The developed flexible electrode
array was placed horizontally 2.5 cm below the
umbilicus, providing three laplacian signals. Three
monopolar Ag-AgCl floating electrodes of 8mm of
sensing diameter were placed 2.5cm above the
umbilicus. Interelectrode distance was also 2.5cm.
Two bipolar recordings of EEnG were obtained from
adjacent monopolar electrodes.
The main sources of physiological interferences
usually present on surface EEnG were
simultaneously recorded. Specifically, ECG was
monitored by Lead 1 using disposable electrodes;
respiration was recorded by an airflow transducer
(1401G Grass), and movements were measured by
means of 3-axis accelerometer (ADXL 335).
Figure 2: Location of electrodes for EEnG recordings.
All signals, except from acceleration signals,
were amplified and band-pass filtered (0.1-100Hz)
by means of commercial bioamplifiers (Grass P511).
A disposable electrode placed on the left ankle of the
FlexibleArrayofActiveConcentricRingElectrodesforSurfaceBioelectricalRecordings-ApplicationtoNon-invasive
RecordingsofEEnG
23
subject was used as reference for the bioelectrical
recordings. Signals were simultaneously recorded at
a sampling rate of 1kHz.
2.3 Signal Analysis
In order to study the activity of the low-frequency
component of the EEnG i.e. the slow wave, EEnG
and respiratory signals were low-pass filtered
(fc=0.5Hz) and resampled at 4Hz.
The power spectral density (PSD) of signals was
estimated by means of autoregressive parametrical
techniques (AR, order 120). PSD was estimated for
moving windows of 120s every 15s of the recorded
signals. The dominant frequency (DF) over 8 cpm of
the PSD of every window was determined. The
parameter %Resp was defined as the ratio between
the number of windows in which the DF of the
surface signal (bipolar or laplacian) is within the DF
of respiration ±0.5 cpm and the total number of
windows. Similarly, %TFSW is defined as the ratio
of analysed windows whose DF is inside the typical
frequency range of intestinal slow wave (8-12 cpm).
The rest of cases are included in the parameter
%Other.
3 RESULTS
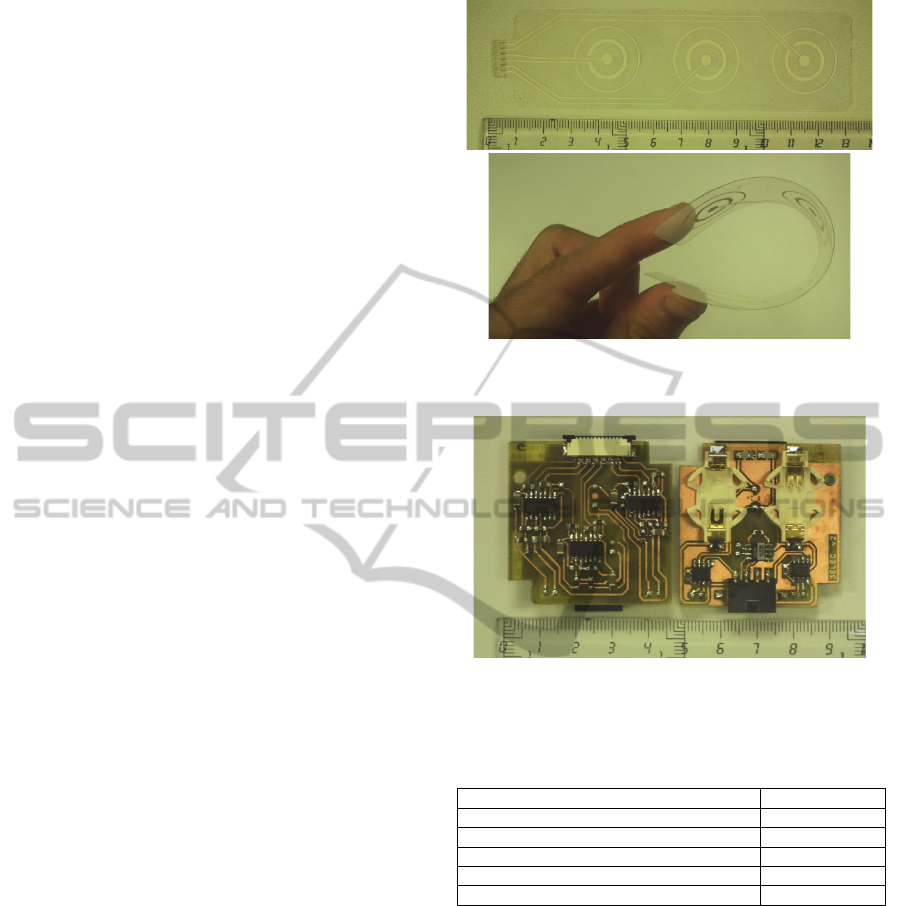
3.1 Active Electrode Array
Figure 3 shows the sensing part of the array of active
concentric ring TCB electrodes. It can be
appreciated that the substrate is flexible enough to fit
the body surface curvature. Moreover the adhesion
of the conductor paste to the substrate was checked
by means of a sticky tape (8915 Filament APT, 3M).
The paste took off after more than 30 cycles proving
the good adherence.
Both sides of the signal preconditioning circuit
of the active electrode array can be seen in figure 4.
The small size and weight of the circuit and the
flexible nature of the array makes it possible to place
this part above the electrodes. With the proper fixing
strategy, the active electrode array could be used for
ambulatory monitoring. Table 1 summarizes the
main electrical characteristics of the developed
signal conditioning circuit. It can be observed that
the battery life is adequate for the recording
sessions, and the CMRR and output noise are also
appropriate for bioelectrical applications.
Figure 3: Implemented flexible array of three TCB
concentric ring electrodes.
Figure 4: Signal preconditioning circuit: bottom side (left)
and top side (right).
Table 1: Main electrical parameters of the signal-
preconditioning circuit.
Cut-off frequency of high pass filter 0.049 Hz
Differential gain at medium freq. 3386 V/V
CMRR at medium frequencies 116 dB
CMRR at 50 Hz 103 dB
Output noise 0.195 mVrms
Battery life 280 min.
3.2 EEnG Monitoring
Figure 5 shows an example of the biosignals
simultaneously recorded. It can be appreciated that,
as expected, the amplitude of the signals picked up
by the ringed-electrodes of the array is smaller than
that of the bipolar recordings with disc electrodes.
Nevertheless, the conventional bipolar recordings
present stronger ECG interference as it can be easily
observed in this figure. In the signals from
concentric ring electrodes the electrocardiographic
interference is almost null. It can only be hardly
appreciated in the signal corresponding to electrode
1 (Lp1) which is placed on the left side of the
BIODEVICES2013-InternationalConferenceonBiomedicalElectronicsandDevices
24
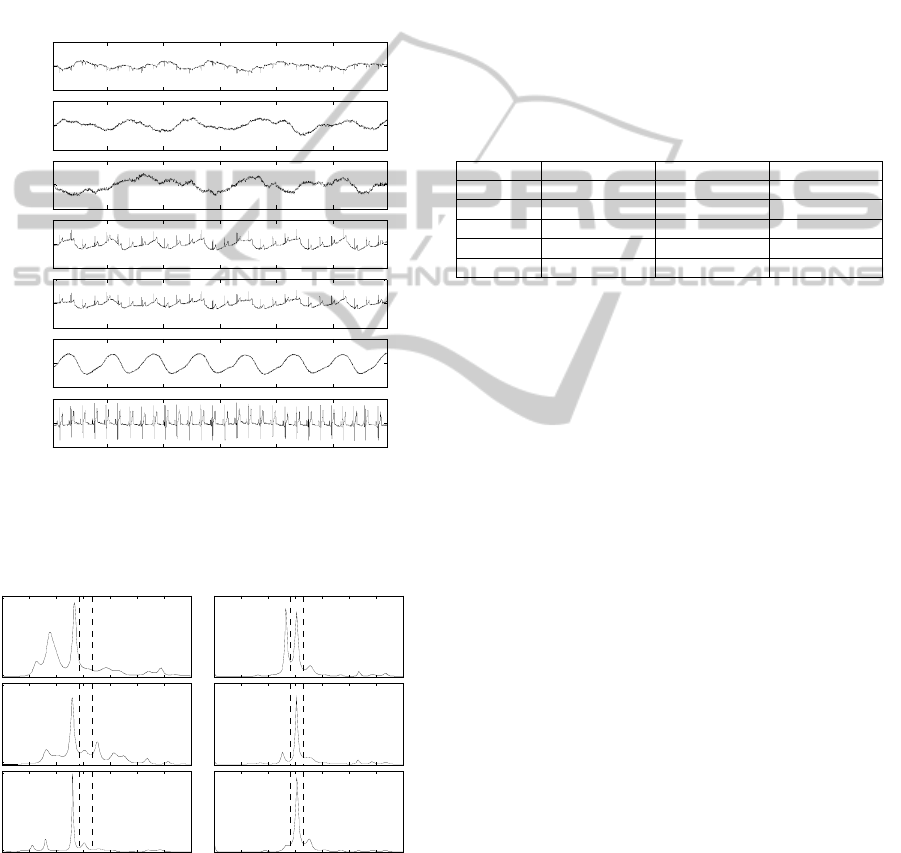
subject. Regarding the intestinal SW activity,
approximately five waves can be identified on the
laplacian recordings. In bipolar recordings this is
difficult to identify by visual inspection since it
seems they are strongly corrupted by the respiration.
This can also be observed in the example of PSD of
signals shown in figure 6. In bipolar recordings the
dominant frequency (DF) corresponds to the
respiratory frequency; whereas the DF of laplacian
recordings is around 10.5 cpm which fits the normal
SW frequency in human jejunum.
Figure 5: Simultaneous recording of biosignals: Lp1-3:
laplacian signals from the electrode array; Bp1-2: bipolar
signals from disc electrodes; Resp: respiration; ECG:
electrocardiogram
Figure 6: Example of power spectrum density (AR120) of
a 120s window of recorded biosignals.
The results of the %TFSW, %Resp and %Other
parameters, which are presented in table 2, confirm
this behaviour. It is shown that in around 25% of the
signal windows studied, the respiratory interference
masks the intestinal SW activity. In contrast, this
ratio is only around 10% for the laplacian
recordings. Furthermore, around 75% of the cases
the DF of laplacians recordings the DF is in the
frequency range associated to the intestinal SW,
whereas it is about 65% for the conventional bipolar
recordings. Finally to say that the number of cases
whose DF is associated to SW armonics or other
components is slightly higher in laplacian recordings
than in conventional bipolar recordings.
Table 2: Percentage of dominant frequency in the
bandwidths of the different components (mean±standard
deviation); N=3385, Lp1-3: laplacian signals from the
electrode array, Bp1-2: bipolar signals from disc
electrodes.
Channel %TFSW %Resp %Other
Lp1 76,6±8,6 11,3±5,6 12,0±5,8
Lp2 72,8±8,2 9,5±7,0 17,7±6,2
Lp3 71,2±6,9 11,6±8,0 17,2±3,8
Bp1 63,0±12,1 27,3±12,0 9,7±4,8
Bp2 65,6±13,8 25,2±13,8 9,2±6,0
4 DISCUSSION
To the authors’ knowledge, the flexible array of
active concentric ring electrodes presented in this
paper is the first one of these characteristics. Other
authors have developed active concentric ring
electrodes but on rigid substrates (Li et al., 2005);
(Prats-Boluda et al., 2011); (Koka and Besio, 2007).
This new sensor is more comfortable for the subject
under study and provides a better contact since it
adapts to the body surface curvature. Our group has
recently developed other flexible concentric ring
electrodes (Prats-Boluda et al., 2012). However such
electrodes require the screen-printing of three layers,
alternating conductor and dielectric pastes. In
flexible substrates it is very complicated to use bias
between layers, and the solution proposed in the
present work favours an easier manufacturing.
Moreover, in contrast to individual electrodes (Prats-
Boluda et al., 2012); (Li et al., 2005); (Koka and
Besio, 2007), the electrode array developed in this
work is a more compact solution that reduces the
signal preconditioning cost and space, and it is more
suitable for bioelectrical mapping of the body
surface. Furthermore, the modularity of the
developed sensor permits to reuse the signal
conditioning circuit while the sensing part can be
disposed for hygienic reasons.
Signal recording experiences of this work show
that active concentric electrodes of the flexible array
-50
0
50
Lp1
(
V)
-50
0
50
Lp2
(
V)
-50
0
50
Lp3
(
V)
-100
0
100
Bp1
(
V)
-100
0
100
Bp2
(
V)
-50
0
50
Resp
(
V)
0 5 10 15 20 25 30
-1
0
1
Time (s )
ECG
(mV)
PSD (a.u.)
PSD (a.u.)
PSD (a.u.)
PSD (a.u.)
0 4 8 12 16 20 24 28
PSD (a.u.)
Frequency (cpm)
0 4 8 12 16 20 24 28
PSD (a.u.)
Frequency (cpm)
Lp1
Bp1
Lp3
Resp
Bp2Lp2
FlexibleArrayofActiveConcentricRingElectrodesforSurfaceBioelectricalRecordings-ApplicationtoNon-invasive
RecordingsofEEnG
25

enhance the quality of non-invasive EEnG signals in
terms of electrocardiographic and respiratory
interferences, in comparison to bipolar recordings
with conventional disc electrodes. This is in
agreement with previous studies that used this kind
of electrodes implemented on rigid substrates (Prats-
Boluda, 2011). On one hand, the reduction of
respiratory interference permits to identify more
easily the activity of intestinal slow wave. On the
other hand, the reduction of ECG interference could
help the identification of spike bursts activity. This
could provide more robust systems to non-invasively
monitor intestinal myoelectrical activity which could
bring close the clinical application of this technique.
Nevertheless, this should be confirmed in future
studies.
Moreover, although it has not been tested in this
work, according to other authors (Besio and Chen,
2007); (Soundararajan and Besio, 2005) the
laplacian potential mapping can enhance spatial
sensibility for surface bioelectrical activity. This can
be of great importance for the studies of propagation
maps of cardiac, electroencephalographic or uterine
activity which can provide electrophysiological
information of clinical relevance. The developed
flexible array of active concentric ring electrodes
would be very suitable for these applications.
5 CONCLUSIONS
The flexible array of active concentric ring
electrodes developed in this paper joins the benefits
of laplacian techniques in terms of enhancing spatial
resolution, with the comfort and adaptation to body
surface curvature of conventional disposable
electrodes.
The non-invasive recordings of intestinal
myolectrical signals with this new kind of electrodes
provide enhanced bioelectric signals in terms of
robustness to physiological interferences such as
ECG and respiration, and permit to identify more
easily the intestinal slow wave activity.
ACKNOWLEDGEMENTS
Research supported in part by the Ministerio de
Ciencia y Tecnología de España (TEC 2010-16945)
and by Universitat Politènica de València (PAID
2009/10-2298).
REFERENCES
Besio, W., Aakula, R., Koka, K., and Dai, W., 2006.
Development of a tri-polar concentric ring electrode
for acquiring accurate Laplacian body surface
potentials. Ann.Biomed.Eng 34 426-435
Besio W., and Chen T., 2007. Tripolar Laplacian
electrocardiogram and moment of activation
isochronal mapping. Physiol, Meas. 28 515-529.
Bradshaw, L. A., Richards, W. O., and Wikswo, J. P., Jr.,
2001. Volume conductor effects on the spatial
resolution of magnetic fields and electric potentials
from gastrointestinal electrical activity. Med. Biol.
Eng. Comput. 39 35-43
Chang S. J., Cho E. T., Heo G. S., Park, C. G., Kim M.
W., Chang I. Y., Shin M. K., Cha, K. H., Yeum, C. H.,
Jun, J. Y., 2006. Fasting and postprandial small
intestinal slow waves non-invasively measured in
subjects with total gastrectomy. Gastroenterology
247-252.
Chen, J. D., Schirmer, B. D. and Mccallum, R. W., 1993.
Measurement of Electrical-Activity of the Human
Small-Intestine Using Surface Electrodes. IEEE Trans.
Biomed. Eng. 40 6 598-602.
Fleckenstein P. and Oigaard A., 1978. Electrical spike
activity in the human small intestine. A multiple
electrode study of fasting diurnal variations.
Am.J.Dig.Dis. 23: 776-780.
Garcia-Casado J., Martinez-de-Juan J. L., Ponce J. L.,
2006. Adaptive filtering of ECG interference on
surface EEnGs based on signal averaging. Physiol
Meas. 27: 509-527.
Hjorth, B., 1975. An on-line transformation of EEG scalp
potentials into orthogonal source derivations
Electroencephalogr. Clin. Neurophysiol. 39 526-530
Koka, K. and Besio, W. G., 2007. Improvement of spatial
selectivity and decrease of mutual information of tri-
polar concentric ring electrodes. J.Neurosci. Methods
165 216-222.
Li, G., Wang, Y., Jiang, W., Wang, L. L., Lu, C-Y S., and
Besio, W. G., 2005. Active Laplacian Electrode for the
Data-acquisition System of EHG. Journal of Physics:
Conference Series, 13, 330-335.
Lu, C. C. and Tarjan, P. P. 1999. An ultra-high common-
mode rejection ratio (CMRR) AC instrumentation
amplifier for laplacian electrocardiographic
measurement. Biomed. Instrum. Technol. 33 76-83.
Perrin, F., Pernier, J., Bertrand, O., Giard, M. H., and
Echallier, J. F. 1987. Mapping of scalp potentials by
surface spline interpolation. Electroencephalogr. Clin.
Neurophysiol. 66 75-81.
Prats-Boluda, G., Garcia-Casado, J., Martinez-de-Juan, J.
L., and Ponce J. L. 2007. Identification of the slow
wave component of the electroenterogram from
Laplacian abdominal surface recordings in humans.
Physol. Meas 28 1115-1133.
Prats-Boluda, G., Garcia-Casado, J., Martinez-de-Juan, J.
L., and Ye-Lin, Y. 2011. Active concentric ring
electrode for non-invasive detection of intestinal
myoelectric signals. Med.Eng Phys. 33 446-455.
BIODEVICES2013-InternationalConferenceonBiomedicalElectronicsandDevices
26

Prats-Boluda, G., Ye-Lin, Y., Ibañez, J., Garcia-Breijo, E.,
Garcia-Casado, J., 2012. Active flexible concentric
ring electrode for non invasive surface bioelectrical
recordings. Meas. Sci. Technol, (to be published).
Quigley, E. M. 1996. Gastric and small intestinal motility
in health and disease. Gastroenterol. Clin.North Am.,
25 113–145.
Soundararajan, V. and Besio, W. 2005. Simulated
Comparison of Disc and Concentric Electrode Maps
During Atrial Arrhythmias. International Journal of
Bioelectromagnetism 7 217-220.
Weisbrodt, N. W. 1987. Motility of the Small Intestine. in
Physiology of the Gastrointestinal Tract, 2nd ed. vol.
1, L. R. Johnson, Ed. New York: Raven Press, , pp.
631–663.
Wu, D., Tsai, H. C., and He, B. 1999. On the estimation of
the Laplacian electrocardiogram during ventricular
activation. Ann.Biomed.Eng 27 731-745.
FlexibleArrayofActiveConcentricRingElectrodesforSurfaceBioelectricalRecordings-ApplicationtoNon-invasive
RecordingsofEEnG
27
