
Vibration Diagnostic Probe for Discogenic Pain Due to a Fissure in an
Annulus Fibrosus
Jae-Cheon Kim
1
, Giseok Kang
1
, Hyoung-Ihl Kim
1,2
and Jong-Hyun Lee
1,2
1
Department of Medical System Engineering, Gwangju Institute of Science and Technology, Gwangju, Republic of Korea
2
School of Mechatronics, Gwangju Institute of Science and Technology, Gwangju, Republic of Korea
Keywords: Discography, Vibration Probe, Low Back Pain, Discogenic Pain, Pain Stimulation, Intervertebral Disc,
Annular Fissure, Disc Degeneration, Internal Disc Derangement, Linear Motor.
Abstract: Discogenic pain is the most common cause of chronic low back pain, accounting for 39% of causes. One
possible diagnostic method to determine the cause of discogenic pain is provocative discography. However,
this method is not available to patients with severe fissures due to degenerative disc disease. In this paper,
we present a diagnostic probe in which plastic optical fiber (POF), which is located in a hole in the flexible
tube of the probe, can be steered to the vicinity of fissures in the annulus fibrosus. Then, a linear motor
placed inside the grip generates a minute axial vibration of the POF tip, which irritates the tiny pain nerves
located near fissures. The intensity of the pain thus generated is used as a guideline to determine the level of
discogenic disease. The frequency and amplitude of the vibration discography ranged from 2.5 Hz to 5.7 Hz
and 1.5 mm to 3.4 mm, respectively. The applicability of the designed probe was successfully confirmed by
testing the modified intradiscal microprobe in an ex vivo animal experiment.
1 INTRODUCTION
The intervertebral disc (or disk) is the core structure
of the vertebral column located between vertebral
bodies, lending stability of the body. In the center of
the disc lies a jelly-like structure, the nucleus
pulposus, which is composed of collagen fibers and
mucopolysaccharides. The nucleus pulposus is
surrounded by strong, thick layers of the annulus
which confines the nucleus pulposus in the center of
the disc. On one hand, discs play a key role in
absorbing the axial pressure load delivered from the
trunk and head during movement of the body. On
the other hand, discs are a common source of
chronic low back pain.
The pathological process of a disc usually starts
from the tearing of the annulus. As the lesion
deteriorates, the tears enlarge and coalesce until they
form a fissure in the annulus (internal disc
derangement: IDD), or annulus ruptures at the site of
herniation of disc materials (disc herniation).
Subsequently, low back pain is generally known to
be produced by the secretion of inflammatory
cytokines around the fissure in IDD and by
mechanical compression of the nerve root in disc
herniation (Burke et al., 2002). Although disc
herniation has been well known to the public for
some time, our understanding of the etiology of
chronic back pain has changed during the last two
decades. Major studies on chronic low back pain
have shown that discogenic pain caused by IDD is
estimated to range from 26 % to 39 %, whereas pain
cause by disc herniation ranges from 2.8 % to 3.5 %
(Schwarzer et al., 1995). Recent advances in high-
resolution diagnostic imaging techniques, such as
computed tomography (CT) and magnetic resonance
imaging (MRI), facilitate the diagnosis of disc
herniation. However, even modern imaging methods
are not sufficient to discern the internal disc
derangement.
Modern discography is a pain-provocative test
which can reproduce each patient’s unique pain.
Despite controversy regarding the accuracy and
specificity of discography, it is recognized as the
only method of proving the diagnostic standard for
discogenic pain. Discography is known to provoke
pain by pressing onto nerve structures around the
fissures through the injection of contrast media (Shin
et al., 2009). However, intradiscal pressure cannot
be increased to provoke pains because severely
degenerated discs cannot entrap contrast medium
inside the discs (Kim et al., 2009); (Adams et al.,
159
Kim J., Kang G., Kim H. and Lee J..
Vibration Diagnostic Probe for Discogenic Pain Due to a Fissure in an Annulus Fibrosus.
DOI: 10.5220/0004242201590162
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2013), pages 159-162
ISBN: 978-989-8565-34-1
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)
1986). Therefore, discography has practical
limitations in patients with severely degenerated
discs.
Meanwhile, vibration diagnostic method of
discogenic pain was studied by stimulating lumbar
spinous process (the bony part of the spine) from
skin surface (Yrjama et al., 1994). The method,
however, also couldn’t diagnose patients with total
annular rupture because they felt no pain during the
bony vibration provocation.
In this paper, to overcome the weakness of
conventional discography, we propose a novel
intradiscal microprobe that delivers direct
mechanical stimuli on the nerve endings around the
fissure. The microprobe, capable of steering and
vibrating, was realized for clinical trials, and its
applicability was confirmed by ex vivo animal
experiment.
2 CONFIGURATION
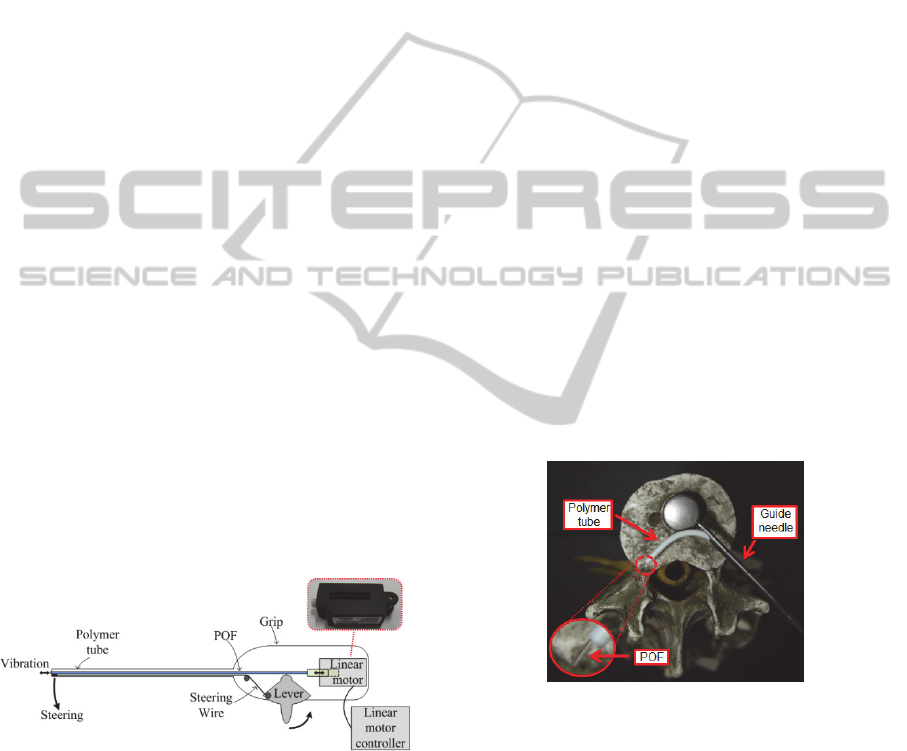
Fig. 1 shows the configuration of the proposed
intradiscal microprobe used to diagnose discogenic
pain. The intradiscal microprobe is composed of a
polymer tube, a plastic optical fiber (POF), a
steering lever, a steering wire, a grip, a linear motor
and a motor controller. The polymer tube has two
holes for insertion of the steering wire and the POF.
The steering wire is inserted into one hole of the
polymer tube, and then each end of the wire is fixed
to the tip of the polymer tube and the lever. Thus,
the lever bend the polymer tube in a counter
clockwise direction as the lever is driven manually.
Figure 1: Diagram of the proposed intradiscal microprobe
capable of steering and vibrational stimulus. The device is
composed of a polymer tube, a plastic optical fiber (POF),
a steering lever, a steering wire, a grip, a linear motor and
a motor controller. The steering lever enables the tip of the
polymer tube to be navigated within an annulus fibrosus.
The linear motor and motor controller are used to generate
axial vibration of the POF tip.
Meanwhile, the POF is inserted into the other
hole of polymer tube and then connected with the
moving part of the linear motor, which is located in
the grip of the microprobe. Also, the linear motor is
linked to the motor controller which enables the
reciprocation of the linear motor. Reciprocation
leads to axial vibration of the POF tip which
facilitates stimulation of the nerve endings around
the fissure.
3 OPERATION PRINCIPLE
Fig. 2 shows how the POF, which is placed in the
polymer tube of the intradiscal microprobe,
approaches the annulus fibrosus. First, the polymer
tube is introduced through a guide needle into the
nucleus pulposus (jelly-like substance inside the
disc). After that, the POF is steered to the vicinity of
the fissure in the annulus fibrosus as the lever is
pulled slowly. As shown in the inset of fig. 2, one
end of the POF comes out from the polymer tube,
facilitating navigation toward the fissure. The other
end of the POF is connected to the movable part of
the linear motor. The movable part moves back and
forth to produce the alternating motion of the
protruding POF tip which delivers a vibrational
stimulus to nerve structures near the fissures. The
frequency and amplitude of the vibrational stimulus
can be changed according to two input variables of
the linear motor. The variables are velocity and span,
which can be regulated by the motor controller.
Figure 2: Photograph of the polymer tube steered towards
the outer disc above a life-size human spine model. The
inset is a magnified view of the protruding POF tip. A
round metal plate is a fixture used to fasten the spine.
The vibration of the POF tip directly irritating
the nerve endings will cause pain, the intensity of
which is applicable as an effective indicator for the
diagnosis of discogenic pain. In addition, unlike
conventional discography, the proposed method is
valid even for patients with severely degenerated
discs where the nucleus pulposus has escaped from
the annulus fibrosus.
BIODEVICES2013-InternationalConferenceonBiomedicalElectronicsandDevices
160
4 FABRICATION
The intradiscal microprobe was fabricated by
modification of commercial steerable catheter for
drug injection. First, considering the size of the
human intervertebral disc, the polymer tube length
was designed to protrude 30 mm from the guide
needle. Next, the linear motor (PoteNit, LSA-3024)
was fixed inside the grip of the microprobe, and was
electrically coupled to the motor controller outside
of the grip. After that, one end of the wire (dia. 250
μm) was inserted into the smaller hole (dia. 300 μm)
of the polymer tube (dia. 2000 μm, and was fixed at
the tip of polymer tube. The other end was joined to
the lever. Then, the moving part of the linear motor
was connected with one end of the POF (dia. 500
μm). Finally, the fabrication of the microprobe was
completed by the insertion of a POF into the larger
hole (dia. 2000 μm) of the polymer tube.
Fig. 3 shows the process of steering the polymer
tube tip that is inserted into the guide needle. The
steering angle of the tube tip was about 10° when the
steering lever was in the middle of the operating
range as shown in fig. 3a. As the lever was fully
pulled back, the tube tip became more bent in a
counter clockwise direction as shown in figs. 3b and
3c. Meanwhile, the POF tip protruded further
outwards as the steering angle of the tube increased,
as shown in the insets of figs. 3a, 3b, and 3c.
Consequently, the protruding POF tip could reach to
the fissures more easily and more efficiently.
Figure 3: The steering process of the polymer tube tip of
the fabricated intradiscal microprobe: (a) initial state, (b)
the lever in the middle, and (c) the lever fully pulled. The
steering angle of the tube tip ranges from 10° to 90°. The
insets show that the POF tip protrudes from the polymer
tube with bending of the polymer tube. The protruding
length ranges from 0 mm to 2 mm.
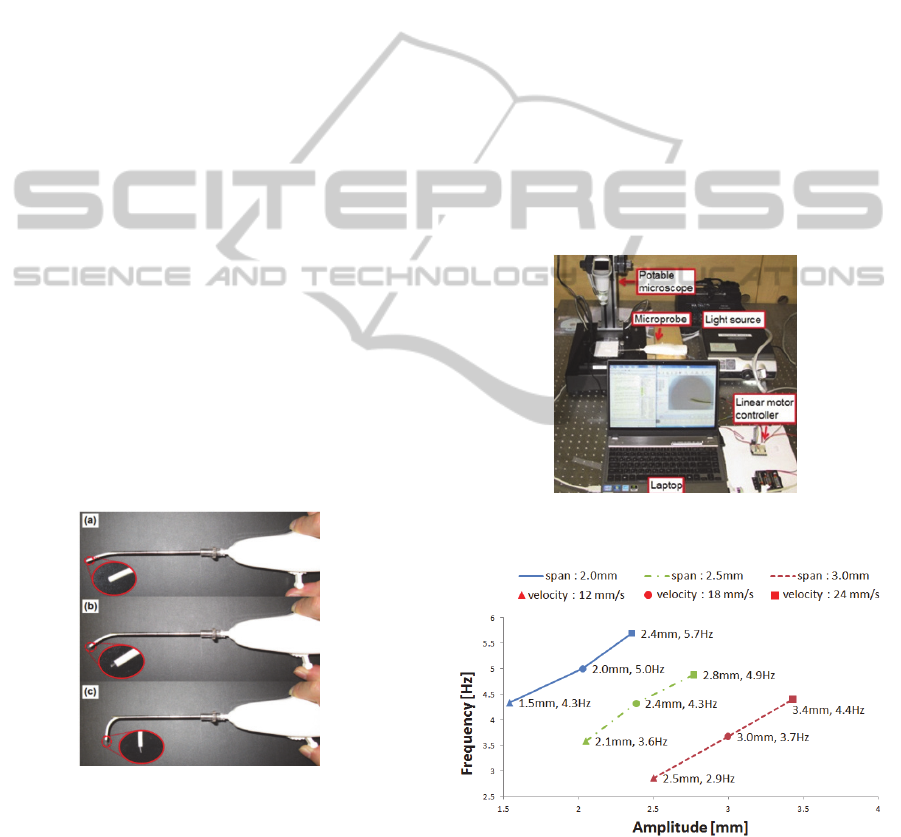
5 EXPERIMANTAL RESULTS
Fig. 4 shows the experiment set-up to evaluate the
performance of the intradiscal microprobe. The axial
reciprocation of the POF tip was expressed as a sine
wave on an oscilloscope by using a micro-
vibrometer (Nihon Kagaku Eng. MLD-211D) which
was set to a horizontal scale of 50 ms/div and a
vertical scale of 160μm/div. The sine waves were
recorded while the velocity and span, which are
input variables of the device, were increased from 12
mm/s to 24 mm/s in increments of 6 mm/s and 2 mm
to 3 mm increments of 0.5 mm, respectively. The
frequency and amplitude of the sine wave were
converted to those of the axial reciprocation of the
POF tip using the scale. The minimum values of the
measured frequency and amplitude were 2.5 Hz and
1.5 mm, respectively, and the corresponding
maximum values were 5.7 Hz and 3.4 mm,
respectively (fig. 5).
Figure 4: Photograph of the experiment set-up to evaluate
the intradical microprobe for vibration discography.
Figure 5: Measured vibration characteristics of the
intradical microprobe.
The maximum frequency obtained with currently
available micro-motor was 5.7 Hz which is smaller
than 42 Hz to 50 Hz of the bony vibrator device
(Yrjama et al., 1994). The vibration frequency of the
VibrationDiagnosticProbeforDiscogenicPainDuetoaFissureinanAnnulusFibrosus
161

present intradiscal microprobe is thought to be high
enough to provoke pains because the method
directly irritates the nerve ending, not the bone.
In addition, the preliminary experiment to
evaluate the ex vivo steering performance of the
intradiscal microprobe was implemented using C-
arm x-ray imaging. The experiment was carried out
in a pig spinal cord, instead of the nucleus pulposus,
because an x-ray image of the polymer tube would
not be visible due to the opaque vertebrae located at
top and bottom sides of the nucleus pulposus.
Considering that the mechanical properties of the
jelly-like spinal cord are similar to those of the
nucleus pulposus, this preliminary experiment is
thought to be able to provide meaningful data for
subsequent ex vivo experiment.
Prior to the ex vivo experiment, we conducted a
steering test of the polymer tube in air to compare
with the steering performance in the ex vivo spinal
cord. The protruding length of the polymer tube,
from the guide needle, was decreased to 13 mm,
because the diameter of the pig spinal cord prepared
for the experiment was only 15 mm. The maximum
steering angle of the 13 mm length of the protruding
tube in air was measured to be 42°, which is about
half that of the 30 mm protruding tube. The
reduction in the steering angle is attributed to the
shortening of the protruding tube length, which is
easily predictable.
Fig. 6 is an ex vivo x-ray image (C-arm) which
shows that the polymer tube was successfully guided
to the outer rim of the pig spinal cord. The
maximum steering angle in the spinal cord was
measured as 40°, which is in good agreement to that
in air. This indicates that there is a negligible
difference in the steering angle in air and that in the
spinal cord. Even in a case of the tube protruding 30
mm, we can infer that the steering angle and
amplitude in clinical trials will be almost the same as
the results obtained from experiments in air.
Figure 6: The C-arm picture of the polymer tube steered
towards the outer rim of the pig spinal cord.
In a further study, we will carry out an in vitro
vibration experiment using a model that has
mechanical properties similar to those of the nucleus
pulposus before clinical trials. Also, a high-
performance linear motor will be used to achieve a
wider range of vibration frequency and amplitude.
ACKNOWLEDGEMENTS
This research was supported by a grant from the
Institute of Medical System Engineering (iMSE) of
the Gwangju Institute of Science and Technology
(GIST), Republic of Korea.
REFERENCES
Yrjama, M. and Vanharanta, H., 1994, Bony Vibration
Stimulation: a New, Non-Invasive Method for
Examining Intradiscal Pain. European Spin Journal,
3:233-235.
Burke, J. G., Watson, R. W. G., McCormack, D., Dowling,
F. E., Walsh, M. G. and Fitzpatrick, J. M., 2002.
Intervertebral Discs Which Cause Low Back Pain
Secrete High Levels of Proinflammatory Mediators.
Journal of Bone and Join Surgery, Vol.84-B:196-201.
Schwarzer, A. C., Aprill, C. N., Derby, R., Fortin, J., Kine,
G. and Bogduk, N., 1995. The Prevalence and Clinical
Features of Internal Disc Disruption in Patients With
Chronic Low Back Pain. Spine, Vol.20:1878-1883.
Shin, D., Kim, H., Jung, J., Shin, D. and Lee, J., 2006,
Diagnostic Relevance of Pressure-Controlled
Discography, Journal of Korean Neurosurgical
Society, 21(5):911-916.
Kim, H., Shin, D., Kim, H., Yoo, E., Shin, D. and Lee, J.,
2009, Clinical and Radiological Findings of
Discogenic Low Back Pain Confirmed by Automated
Pressure-Controlled Discography. Journal of Korean
Neurosurgical Society, 46(4):333-339.
Adams, M. A., Dolan, P. and Hutton, W. C., 1986, The
Stages of Disc Degeneration as Revealed by
Discograms. Journal of Bone and Joint Surgery,
Vol.68-B:36-41.
BIODEVICES2013-InternationalConferenceonBiomedicalElectronicsandDevices
162
