
Towards Adapting Scientific Workflow Systems to Healthcare Planning
Bruno S. C. M. Vilar, Claudia Bauzer Medeiros and Andr
´
e Santanch
`
e
IC - UNICAMP, 13083-852, Campinas, SP, Brazil
Keywords:
Scientific Workflows, Task Network Models and Nursing.
Abstract:
Healthcare and research environments have common characteristics and needs, such as managing people and
resources, planning and conducting distributed activities, event-sensitive and monitoring processes. There are
several examples in which Workflow Management Systems can aid healthcare management, systematizing,
logging and automating activities. In this work we propose a context-driven approach to produce health
workflows, which goes beyond an adaptation of workflows tasks to afford health procedures – as proposed
in related work – departing from the rationale born from health professionals and materialized in CIG. This
paper presents our proposal to support nursing processes through customization of workflows tools using as a
starting point a comparative study of systems with respect to features required by healthcare professionals.
1 INTRODUCTION
Healthcare facilities involve the management and co-
ordination of healthcare providers, patients, and re-
sources. There is a need for automated ways to mon-
itor and integrate the flow of exams, nursing proce-
dures and resources.
A common approach adopted to model health-
care processes are Computer-Interpretable Guide-
lines (CIGs), which implement guidelines in active
computer-based decision support systems, able to
monitor actions and observations of care providers
and to provide guideline-based advice at the point
of care (de Clercq and Kaiser, 2008). CIG can be
modelled as Task-network Model (TNM), which “de-
composes guidelines into networks of tasks unfolding
over time” (Ye et al., 2009). A TNM can be seen
as a hierarchical directed graph that specifies a flow
of activities. Its enactment is often supported by ar-
tificial intelligence planning environments, in which
a TNM is specified using some adaptation of a goal-
based planning language.
Our key argument in this paper is that CIG sys-
tems, born in the healthcare context, embed the usual
rationale applied in this context, tailored to the dy-
namic healthcare environment. Workflows, on the
other hand, are robust tools, broadly tested and refined
by the community for many domains. They are being
increasingly adopted in hospitals – e.g., (Ria
˜
no et al.,
2012) – to support task automation, but are based on
standard (business) workflow environments.
Healthcare activities involve a dynamic scenario, in
which professionals have to constantly interact with
the tools, to register patient information, intervention
plans, and desired outcomes, creating the need for
flexible workflow management.
As Panzarasa and Stefanelli (Panzarasa and Ste-
fanelli, 2006) highlight, “a critical challenge for any
Workflow Management Systems (WfMS), in a real
clinical setting, is its capability to respond effectively
when exceptions occur. An exception can be defined
as any deviation from the normal flow of activities,
and it can arise from changes in resource availability,
task requirements or task priority, and anomalous, but
expected, effects of delivered care.”
In fact, the generic modeling approach adopted
by workflows, contrasts with the domain-specific for-
malisms (e.g., TNM) applied to model clinical prac-
tice guidelines. These formalisms are derived from
the practical clinical activities and embed their ratio-
nale and approach to plan and manage activities.
There are research on adding flexibility to WfMS
in a healthcare scenario, such as (Dang et al., 2008),
(Mikolajczak and Shenoy, 2010), and (Schick et al.,
2012). There are, however, additional requirements
to be fulfilled so that a WfMS can provide an ade-
quate environment for practical clinic usage, such as
preserve the systematization and work organization of
clinicians, provide the traceability of actions, allow
remote and collaborative work, among others.
Our solution to overcome these problems is based
on two aspects: first, to adopt scientific workflow
75
S. C. M. Vilar B., Bauzer Medeiros C. and Santanchè A..
Towards Adapting Scientific Workflow Systems to Healthcare Planning.
DOI: 10.5220/0004242600750084
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2013), pages 75-84
ISBN: 978-989-8565-37-2
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

systems
1
; second, to extend these systems with fa-
cilities for dynamic self-adaptation based on context.
Our context-driven approach is a glue that enables to
“think” workflows using a healthcare perspective.
Scientific workflow systems are normally adopted
in research environments, to manage research ac-
tivities, specification and execution of experiments.
Given their event-driven characteristics, openness,
flexibility, support to distributed collaborative work,
and ability to handle exceptions, they are more suit-
able to health environments than business workflows.
This paper justifies this claim through analysis
on the requirements of WfMS, created for scientific
and business contexts, comparing their features with
CIGs, applied to the healthcare domain. Our second
ingredient – context-driven self-adaptation – is de-
rived from the approach of planning and monitoring
healthcare activities, as observed in TNM specifica-
tions.
The contributions of this paper are: (i) an outline
of the architecture proposed with a case study (Sec-
tion 4); (ii) a detailed analysis of the factors that led
us this proposal, and comparative tables (Sections 2
and 3).
2 RELATED WORK
2.1 Context
One of the aspects to be covered in this work is adap-
tation of workflows to a context. Defining the term
“context” in an accurate or complete way is not a
simple task: in the literature, it varies according to
the perspective of who uses the term, and where it is
used. (Millard et al., 2004) say that “it is very difficult
to take into consideration all the contextual factors in
one information retrieval system, so that researchers
often define the context as certain factors (location for
example)”.
(Dey, 2000) presents a generic definition of con-
text, from a Computing perspective: “any informa-
tion that can be used to characterize the situation of
an entity. An entity is a person, place, or object that is
considered relevant to the interaction between a user
and an application, including the user and application
themselves”. (Strang et al., 2003) define the term as:
“the set of all information characterizing the entities
relevant for a specific task in their relevant aspects”.
The definitions of (Bolchini et al., 2007), (Dey,
2000) and (Strang et al., 2003) are generic with re-
1
As opposed to the business workflow systems adopted
in hospitals.
spect to the application. However, researchers more
commonly require tailoring a concept to their needs,
e.g., as in (Asfari et al., 2010). For them, “context
describes the user current task, its changes over time
and its states, i.e. we take into account the task which
the user is undertaking when the information retrieval
process occurs”. (Turner, 1999), concerned with In-
telligent Agents, defines context as “a distinguished
(e.g., named) collection of possible world features
that has predictive worth to the agent”. To (Ban-
dara et al., 2009), it is “any static or dynamic client-
, provider- or service-related information, which en-
ables or enhances efficient communications among
clients, providers and services”.
The variation of the use of “context” in different
fields and purposes results in diverse denominations.
Table 1 summarizes our survey of the usages of the
term. The table shows for each paper the applica-
tion area, the domain of use and the representation
of “context”. This study also showed that diverse
kinds of information can be used to specify “context”,
such as: those that identify a user’s characteristics
and preferences; or the location of an event and infor-
mation about it, such as history, climatic conditions,
legislation, service characteristics, domain, platform
and others. This information is collected in differ-
ent ways: sensors, logs of users’ actions in systems,
forms and others.
In spite of a wide space of variables to identify a
context – eg. domain, service, location, identity, and
device –, some can be highlighted. To (Dey, 2000), lo-
cation, identity, time, and activity are the most impor-
tant context variables to characterize the situation of
an entity. According to the author, these kinds of con-
texts not only can answer questions such as “Who”,
“What”, “When” and “Where”, but also they can act
as indexes to other contextual information sources.
For instance, in all mobility and location-based stud-
ies, the most important variables are space (coordi-
nates) and time.
2.2 Scientific Workflows
A workflow is the sequence of steps that are necessary
to achieve a specific goal (Barthelmess, 1996). It al-
lows to systematize a task in activities that, from their
respective input resources, generate a certain result.
Each activity can be composite or atomic. Workflows
can be designed from an abstract specification that is
refined gradually until it reaches an execution level –
a concrete workflow (Medeiros et al., 2005). An ab-
stract specification helps to understand how workflow
tasks are carried out, identify problematic spots (e.g.,
bottlenecks), and analyze changes that can be carried
HEALTHINF2013-InternationalConferenceonHealthInformatics
76
Table 1: Characteristics of work using the notion of context.
Work Computing-related Aspects Application Do-
main
Context Representation in a Com-
puter
(Dey, 2000) Context-Aware Computing Generic -
(Millard et al., 2004) Context-Aware Environments Pervasive Com-
puting
Multiple Ontologies (OWL)
(Bolchini et al., 2007) Evaluation Framework - Con-
text Models
Generic Generic: analyze and suggest mod-
els
(Bandara et al., 2009) Web Services Composition Business Ontology (OWL - light)
(Kholladi and Doan, 2010) Information Retrieval Generic Relational DB
(Asfari et al., 2010) Information Retrieval Generic Tasks represented as UML State Di-
agram. Terms associated to ontolo-
gies (WordNET e ODP)
(Carmagnola et al., 2005) Adaptive Hypermedia Generic/Validation:
Tourism
Multi-ontology matrix and SWRL
rules
(Lundberg, 2007) and
(Lundberg and Rune, 2009)
Distributed Environment In-
formation Sharing
Emergency
Service Centres
Inference rules mapped on Work-
flows Simulates: state and conse-
quence
(Bardram and Hansen,
2010)
Computer-Supported Cooper-
ative Work
Hospital Clini-
cians
Not specified
(Strang et al., 2003) Middleware Generic Ontology (represented in: OWL,
DAML+OIL and F-Logic)
(Cho et al., 2010) Workflows Agriculture RDF: restrictions. uWLD: context
aware workflows language.
(Turner, 1999) Intelligent Agents Medical Diagno-
sis
C-Schemas (”frame-like”)
out in designing the workflow. Executable (or con-
crete) activities are those associated with some tool or
service that processes or aids the obtention of results
that serve as input to other activities.
Workflow management, coordination of processes
and other functionalities are the responsibility of
WfMSs. These systems orchestrate algorithms and
computational processes, combining parallel and dis-
tributed processing, databases, artificial intelligence,
among others, building a repository for experimenta-
tion through simulation (Deelman et al., 2009).
WfMSs allow processes to be organized in differ-
ent ways to meet requirements and processing needs.
The main characteristic of a WfMS is process au-
tomation, involving the combination of activities per-
formed by people and computers (Hollingsworth and
Others, 1993). The role of these systems, however, is
not limited only to the automation, but also allows to
obtain process information in different levels of de-
tail, besides systematically capturing provenance in-
formation of produced data (Scheidegger et al., 2008).
In this paper, scientific workflows are adapted to
healthcare. A scientific workflow can represent the
process chaining that transforms data aiming at an ex-
perimentation by simulation(Ogasawara et al., 2008).
These systems “enable researchers to collaboratively
design, manage, and obtain results that involve hun-
dreds of thousands of steps, access terabytes of data,
and generate similar amounts of intermediate and fi-
nal data products” (Deelman and Chervenak, 2008).
Thus, scientists can focus on their research and not
on computation management (Deelman et al., 2009).
2.3 Computer-interpretable Guidelines
“Clinical guidelines can be viewed as generic
skeletal-plan schemata that represent clinical proce-
dural knowledge and that are instantiated and refined
dynamically by care providers over significant time
periods” (Shahar et al., 1998). There are also special-
ized versions of the guidelines, e.g., Nursing Clinical
Guidelines, which provide evidence-based instruc-
tions/recommendations about how to handle specific
patient care issues (Din et al., 2010).
Even though the guidelines represent clinicians’
background about suggested ways to deal with health
issues, (Fox et al., 2009) highlight that the clinicians’
judgment may conflict with the general guidelines,
so the treatment may differ from the one originally
stated. This may occur because the guidelines are
generic, and thus may not consider new knowledge
about the treatment, or patient allergy to the medicine,
etc.
To automate the process of guideline applica-
tion, as well as avoid errors and improve the pro-
cess, there is the study and development of Computer-
Interpretable Guidelines (CIGs). There are several
rich studies to provide support for clinicians, such as
TowardsAdaptingScientificWorkflowSystemstoHealthcarePlanning
77

Clinical Decision Support Systems (El-Fakdi et al.,
2012), Care Flow (Mikolajczak and Shenoy, 2010),
Task Network Model (Ye et al., 2009), Clinical Path-
way Management System (Ye et al., 2009), and
Healthcare Information Management System (Dang
et al., 2008). To be effective, “these tools need to be
simple to use, easily available, and work with differ-
ent information systems in changing environments”
(Leong et al., 2007). For those characteristics, there is
a need to: i) Preserve methodology and systematiza-
tion already applied by clinicians; ii) Provide flexibil-
ity to adapt the guideline instance to the situation; iii)
Dispose of open and extensible environment to add
resources and better suit the solution to the problem.
Our work tries to comply with those requirements
combining features from WfMS and CIG systems.
Section 3 analyses characteristics from both systems.
3 COMPARING WFMS AND CIG
SYSTEMS
Ideally, automated systems to support healthcare ac-
tivities must comply with a variety of software re-
quirements. They must be flexible, extensible by
plug-ins, support different kinds of activities (ser-
vices, languages, etc.), allow annotation of tasks, reg-
ister provenance, provide access by a remote client,
and support changes according to context variables.
Also, they must maintain the nature of work of clin-
icians, be flexible to changes, responding to new in-
formation about patients. We analyzed different tools
designed to automate and monitor activities with re-
spect to these properties, as a necessary step to under-
stand deficiencies and advantages of such tools. We
present the results of this study in this section.
We separated the analyzed features in two groups,
infrastructure and organization, respectively pre-
sented on Tables 2 and 3. On Table 2, features are
focused on resources that allow flexibility to extend
the tool, including its openness and extensibility by
plug-ins, possibility to annotate (describe) basic com-
ponents, share and reuse resources, schedule activi-
ties and provide some level of security. We use ’+’ to
indicate compliance, ’±’ a partial or limited compli-
ance, and ’-’ the lack of it. On Table 3 we analyzed
the following: the basic component (building block)
of the system, how it can be associated to other com-
ponents, and which resources can be used to define a
component. The table also contains a description of
flexibility to change the flow of execution and which
contextual information is associated to components.
Column “resources to define a component” gives an
idea of a system’s flexibility to create/execute work-
flows on CIGs so let us now explain these systems.
Trident (Barga et al., 2008) is a scientific WfMS
that provides workflow provenance, schedule, and
monitoring. However, there is a lack of extensibil-
ity features, especially to deal with external resources
as a workflow task. To add a task it is necessary to ex-
tend a specific Microsoft .NET class or use external
tools to import webservices.
VisTrails (Howe et al., 2008) has resources for
visualization and creation of workflows by analogy,
useful to provide easy use for non-IT specialists.
Also, there is an exemplification mechanism that al-
low faster identification of the purpose of a task,
which benefits workflow creation to achieve the goal.
There is a versioning tree that allows to view changes
made to workflows, which would be interesting to an-
alyze different interventions applied to patients. The
tool has limitations regarding the use of subworkflows
and support to share and retrieve workflows, reducing
its suitability on collaborative environment.
Kepler (Altintas et al., 2004) can execute tasks se-
quentially, paralleled, iteratively, etc. The WfMS sup-
ports a wide diversity of options to implement tasks,
including webservices, R and XSTL. It is possible to
register provenance information and to semantically
annotate components, using URN (Uniform Resource
Name), which is interesting to make links between se-
mantically described clinical guidelines. The limita-
tions found are the lack of a client-server architecture.
Taverna (Hull et al., 2006) does not have an in-
tuitive interface, but is easy to extend and supports
annotations, provenance and sub-workflows. Also,
it allows a diverse use of resources to implement
tasks, such as webservices, Java API and spread-
sheets. Tasks can be organized hierarchically using
sub-workflows.
ASBRU (Seyfang et al., 2002), part of Asgaard
(Yuval Shahar and Johnson, 1998), allows the de-
sign and execution of tasks. The basic component of
the work (a plan) can have different attributes and be
composed by subplans, forming a hierarchy. Atomic
units of plans are actions, which represent a specific
tasks under a plan, and have the flexibility to be as-
sociated to a user interaction, external program or de-
vice. The work deals with context and provides flex-
ibility to change and adapt to situations. It is done
associating a set of attributes that are used to per-
form reasoning, trigger plans, change states and al-
ter measure values. Such attributes are: preferences
(constraints, e.g., strategy, utility and resources), in-
tentions (goals), conditions (rules that govern state
transition) and effects (known effects that plan argu-
ments have over measurable parameters). From the
infrastructure point of view of ASBRU and Asgaard
HEALTHINF2013-InternationalConferenceonHealthInformatics
78

do not provide a flexible way to extend using plug-ins
or modular components from third party developers,
and do not implement security policies.
(Mikolajczak and Shenoy, 2010) developed Care-
flow System, a WfMS developed for healthcare, us-
ing case handling technique to add the necessary flex-
ibility inherent to the problem. The workflow can be
executed in a flexible way because tasks are oriented
to data and can be executed by different users. Each
task has the flexibility to be executed, skipped or re-
executed. As result of the case handling flexibility
usage, the complexity to deal with context variables
is transferred to users, who need to know about the
case to deal appropriately with the task. To avoid the
inadequate handling of tasks, there is an access con-
trol mechanism that associate users and tasks to roles.
The system is developed over the YAWL WfMS, thus
ensuring its important infrastructure features, such as
reuse and share of workflows, flexibility to extend,
client-service architecture, and flexibility to use exter-
nal resources as tasks and support for subworkflows.
CPO (Ye et al., 2009) was developed focusing on
healthcare applications. However, as the authors re-
mark, their approach is different from those based on
TNMs (e.g., ASBRU). “The tasks in clinical path-
ways are not decisions and actions recommended to
clinicians, but the interventions to be performed by a
multidisciplinary team by using healthcare resources,
which contains not only clinicians but other health-
care professionals within one or more organizations.”
As result, CPO is more similar to a traditional WfMS,
with tasks that can be composed by subtasks, as work-
flows and subworkflows.
Perikles (Schick et al., 2012), also extends YAWL
to increase the flexibility of a traditional WfMS, and
makes it more suitable for healthcare applications. To
this purpose, the work adds resources to control and
plan tasks. Each task is specified under the HL7 stan-
dard, and may specify which tasks must be executed
before or after another one, guiding users under activ-
ity planing.
ClinicSpace (Souza and Augustin, 2010) uses
(Yamin et al., 2005) middleware to provide a tool to
support collaboration and management of resources.
The work is developed for pervasive and context-
sensitive computing, interacting with sensors, devices
and users. One of the main features is the recommen-
dation of tasks based on task execution log.
The research analyzed can be classified in four
main groups: scientific WfMSs ((Hull et al.,
2006),(Howe et al., 2008), (Barga et al., 2008), and
(Altintas et al., 2004)); business WfMSs ((Schick
et al., 2012)); CIGs ((Seyfang et al., 2002), (Ye et al.,
2009), and (Souza and Augustin, 2010)); hybrid ap-
proaches that extend or use WfMS to create a health-
care application.
Analysed WfMSs are extensible and, mostly,
comply with open standards to connect with services;
they support the management of provenance and an-
notation and can handle long transactions. The main
workflow standards and/or tools have big libraries of
shared workflows and support routines. Additionally,
they allow the use of abstract activities, which can be
associated to different resources, such as tools, docu-
ments or algorithms – provided as source code or ser-
vice. Moreover, they commonly provide a more com-
plete execution infrastructure with support to client-
server architectures and allow the reuse of already ex-
isting resources. However, they lack support for dy-
namic self-adaptation, and do not provide support to
context changes.
CIGs are essentially activity graphs and may ac-
cept the use of external resources. CIG execution sys-
tems are focused on guiding healthcare profession-
als through recommended actions and register, in a
database, data from executed tasks or events. They
are usually hierarchical (e.g., TNM approach) and
embed the practices and usages of health guidelines.
Moreover, they support definition of sets of conditions
which tailor the actions to perform for each situation.
In fact, such sets are nothing more than contexts for
CIG execution.
An important characteristic found on CIGs is the
approach to support the methodology and the pattern
of work of healthcare professionals. It is essential to
reduce the resistance that professionals may have to
the use of a new tool, as well as reduce the learning
curve to use it.
There is, also, initiatives that combine CIG and
WfMS: (Dang et al., 2008), (Mikolajczak and Shenoy,
2010), and (Schick et al., 2012). Those tools are able
to extend the properties of WfMSs, specializing its
features to be used in healthcare domain. The result
is the possibility to use the WfMS features we char-
acterized as infrastructure, and the improvement of
the tool to allow better usage for healthcare profes-
sionals. Some of the properties of WfMSs and CIGs,
however, can be lost while processing a workflow or
a guideline. (Mikolajczak and Shenoy, 2010), for ex-
ample, add flexibility to workflows, but transfer to the
user the responsibility to deal with context adapta-
tions. (Schick et al., 2012) limits the use of external
tools to those compliant with HL7 standards.
This comparative study guided our model of con-
text, to extend scientific WfMSs. Figure 1 summa-
rizes our perception as result of the comparative anal-
ysis presented in CIG systems. At the top, we show
an abstract representation of the CIG approach to or-
TowardsAdaptingScientificWorkflowSystemstoHealthcarePlanning
79
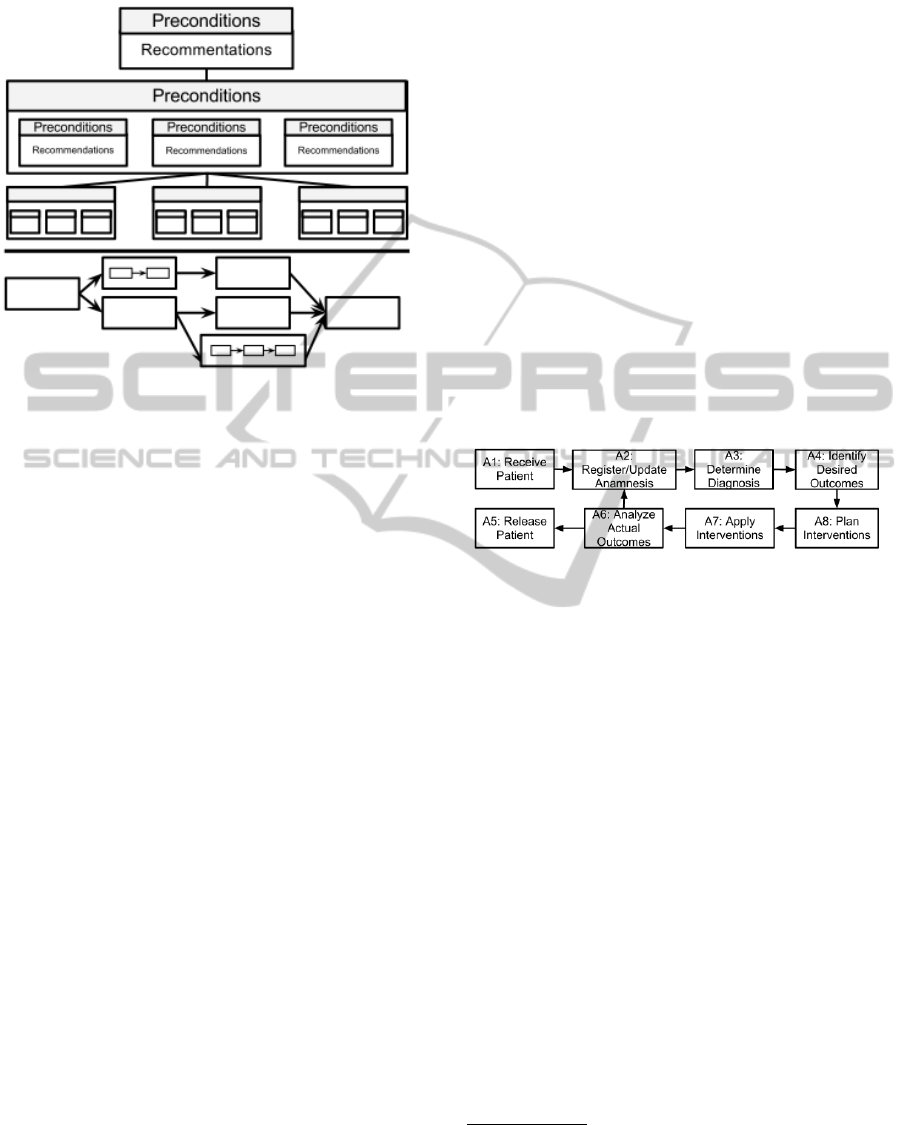
ganize and handle tasks, as observed in CIG systems.
Figure 1: Organization of CIG and Workflow approaches as
well as our proposed model.
Each box represents a plan whose execution is de-
termined by the fulfilment of conditions, evaluated ac-
cording to the state of variables, which we classify
here as context variables. By context we mean, for
example, the patient condition or the outcomes of a
procedure. As illustrated in the figure, each plan can
be decomposed in sub-plans, which in turn also have
conditions defined by context variables – contextual
conditions. We contrast this approach to the workflow
approach illustrated at the bottom of Figure 1. Work-
flows are organized as a flow of tasks, whose connec-
tions are depicted by arrows. Even tough workflows
can decompose their tasks in sub-workflows, different
from CIG systems, this composition is a reuse strat-
egy and will not guide the workflow execution accord-
ing contextual variables. This observation motivated
our work of applying this CIG hierarchical decompo-
sition, based on contextual variables, to workflows;
resulting in our context-driven workflow mechanism,
detailed in the next section.
This will be discussed further, using our real case
study as a basis for nursing activities.
4 CHARACTERIZATION OF THE
SCENARIO AND PROPOSAL
Our case study involves the PROCENF system (Peres
et al., 2009) and nursing professionals from the hos-
pitals from University of Campinas and University
of S
˜
ao Paulo
2
. Given this scenario, as well as the
work described in (Doenges and Moorhouse, 2008),
we identified that a patient’s admission and monitor-
ing process in a hospital can be expressed, in a gen-
eral way, by the abstract workflow presented in Figure
2. This workflow reflects the patterns of the anal-
ysed CIGs, which are synthesized in table 3. The
figure uses vocabulary from NANDA – North Amer-
ican Nursing Diagnosis Association – (Intl., 2012),
NIC – Nursing interventions classification – (Sigsby
and Campbell, 1995), and NOC – Nursing outcomes
classification – (CNC, 2012). As can be seen, the
workflow includes an iterative step in which a patient
passes through anamnesis interrogation, an assess-
ment phase. Then, there is the analysis of registered
data to diagnose the problem and to identify expected
outcomes (prognosis). Intervention planning and ap-
plication phases occur to achieve an outcome. Out-
come analysis consists in the analysis of intervention
results, followed by updates to anamnesis records. If
the treatment achieves expected outcomes, the patient
can be released. Otherwise, a new iteration occurs.
Figure 2: High level Workflow for healthcare treatment.
Health plans are characterized by progressively
refinement by health professionals according to the
context in which they are executed. While several
“standard” procedures exist for a multitude of situa-
tions, each procedure is related to a given situation,
or context, e.g., illness to be treated, patient anam-
nesis, and so on. However, depending on how a pa-
tient responds to interventions, a plan may change
drastically. Thus, the execution of a sequence of
tasks within a procedure is usually undertaken hier-
archically: global procedures are defined in a high
level manner, and undergo top-down refinement ac-
cording to a given situation. Thus dynamics of this
context-driven construction presents a marked con-
trast to other domains in which workflows or plans
are conceived
If each procedure is defined as a workflow, this
involves at least two aspects: (i) The execution of a
given workflow may be suddenly interrupted to yield
control to a different workflow dynamically defined
by context and the original workflow may not even
be ever resumed; (ii) Every workflow task subsumes
2
The hospital complex of the University of Camp-
inas alone receives about 500,000 appointments, with over
43,000 internments and 34,000 surgical interventions per
year.
HEALTHINF2013-InternationalConferenceonHealthInformatics
80
Table 2: Infrastructure characteristics of flow organized systems.
Work
Open Source
Flexibility
Annotation
Client-Server
Schedule
Provenance
Reuse/Share
Security
Trident (Barga
et al., 2008)
+ - - + + Who executed, How
long was execution,
Associated data
Non integrated MyEx-
periment
User access and
priviledge control
and workflow roles
VisTrails (Howe
et al., 2008)
+ + + + - Who executed; Where;
How long; etc. Flex-
ible framework to ex-
tend features.
DB share; Synchro-
nization; Versioning
made by external
resources, e.g. SVN.
-
Taverna (Hull
et al., 2006)
+ + + + - Open Provenance
Model: Executed ser-
vice;Execution date;
Parameters used.
MyExperiment Inte-
grated
Secure services and
user credentials
Kepler (Altintas
et al., 2004)
+ + + - - Records provenance
information
KAR files can be reused
and shared. There is a
central KAR repository.
-
ClinicSpace
(Souza and
Augustin, 2010)
- - - + - Records provenance
information
Allows the reuse of reg-
istered tasks
Limits the user ac-
cess to tasks
ASBRU (Seyfang
et al., 2002)
- - + - + Temporal View pro-
vides events history.
Import, export, and du-
plicate plans
-
CPO (Ye et al.,
2009)
- - - + + - Model created as ontol-
ogy to be reused
-
Perikles (Schick
et al., 2012)
extending YAWL
? ? ± + + Logging mechanism
from YAWL
Provides reuse ±
Careflow (Miko-
lajczak and
Shenoy, 2010)
extending YAWL
+ + + + + Logging mechanism
from YAWL
Provides reuse Limits user’s ac-
tions by roles and
authorization.
(Dang et al.,
2008)
- - + + + Logging mechanism
from BPEL Server
Provides reuse Protects processes
and encrypts com-
munication
subworkflows that are chosen according to context.
The dynamic change of tasks implies on another
important aspect to be treated: traceability. Not only
does traceability play a major role, in the sense that
all action and actors must be recorded, but requires a
new dimension – one must also keep track of dynamic
configurations (how, when, and by whom). It is fun-
damental to provide a history of steps performed, to
allow to learn with experience from other profession-
als and to recognize which steps were decisive to the
achieved outcomes. Because of this, provenance is an
important feature that must be supported.
The analysis presented in the previous section
stresses the importance of guiding the workflow ex-
ecution by means of contextual variables, as observed
in CIG systems. Our proposed architecture is able ex-
tend a workflow engine to afford equivalent properties
of a hierarchical decomposition based on contextual
variables, as we will further detail.
Figure 3 shows the top level abstraction workflow
to be executed, as portrayed in Figure 2. CRec is a dy-
namic data structure that records context variables at
each instant. CEng is a context adaptation engine, an
extension of a workflow engine, which monitors the
context (CRec) and dynamically adapts workflow exe-
cution. The part shaded in gray represents the abstract
activities yet to be executed under control of CAEng.
The other abstract activities have already been refined
and dashed line outlines the step executed under grad-
ual refinement and execution.
Figure 3 illustrates two consecutive steps of a
workflow execution carried by an engine, designed
to support our context-based workflow customization
and to allow to the user to interrupt or change the ex-
ecution of an activity at any moment. In each step
of the execution the CAEng monitors the running ac-
tivity to capture context changes, updating the CRec
(operation indicated by a dashed line). Whenever
TowardsAdaptingScientificWorkflowSystemstoHealthcarePlanning
81
Table 3: Basic component (BC) characteristics of flow organized systems.
Work Type BC Resources to Combine
Components
Flow Flexibility BC Organiza-
tion
Modelling of
Context
Trident (Barga
et al., 2008)
WfMS Activity Modified .NET classes;
WebServices imported
using external tool.
- Sub-workflows -
VisTrails (Howe
et al., 2008)
WfMS Activity WebServices;Python
Packages
- Does not make
clear that a
workflow can
be used as
activity.
-
Taverna (Hull
et al., 2006)
WfMS Activity WSDL/RESTful ser-
vices, BioMart, BioMoby,
SoapLab, Java APIs, R,
Beanshell, Spreadsheets,
Plugins to extend support.
- Sub-workflows -
Kepler (Altintas
et al., 2004)
WfMS Activity WSDL/RESTful services,
R, MatLab, Spreadsheets,
command-line applica-
tions, XPath and XSLT;
- Sub-workflows -
ClinicSpace
(Souza and
Augustin, 2010)
CIG +
middle-
ware
Clinical
Task
Limited to previously inte-
grated tasks
Invoke tasks un-
der certain condi-
tions
Tasks and sub-
tasks
Users, loca-
tion, time and
resources.
ASBRU (Sey-
fang et al.,
2002)
CIG Plans User interaction and exter-
nal tools and devices
Relationships
and conditions
change execution
flow
Hierarchy Conditions for
plan activation
CPO (Ye et al.,
2009)
CIG Activity Specification of interven-
tions with associated val-
ues
? Subprocess
similar to
subworkflows
?
Perikles (Schick
et al., 2012) ex-
tending YAWL
CIG Task Service with HL7 compli-
ant interfaces
? Subworkflows ?
Careflow
(Mikolajczak
and Shenoy,
2010) extending
YAWL
Case
Han-
dling +
WfMS
Task External applications, Java
classes and webservices
Users can ex-
ecute, redo, or
skip task and
change data at
any time.
Tasks, Sub-
Tasks and
Workflows
Each task con-
sider the entire
case. Part of the
context is han-
dled by user
(Dang et al.,
2008)
Ont. KB
+ BPEL
server
Tasks Web Service Dynamic work-
flow composition
and execution
Hierarchy Yes
an activity finishes its execution, CAEng verify the
new CRec state in order to apply modifications in
the workflow (operation indicated by a gray area) if
necessary. When the workflow starts, it has a start-
ing CRec containing a set of basic context variables
(see Figure 3 (i)), e.g., environment (e.g., type of
medical facility), user, etc. The
Register/Update
Anamnesis
is the main activity responsible for updat-
ing the CRec. Thus, the system can provide flexibility
to change the flow of the execution, without force user
to adapt the content to context.
5 CONCLUSIONS
The addition of dynamic self-adaptation capability to
scientific WfMSs can provide several advantages to
healthcare activities. Benefits include automation and
monitoring, and distributed execution of activities and
the basis to support traceability of tasks and adapta-
tions. Our work identified three important aspects that
need to be considered: (i) Each task subsumes sub-
workflows that are conducted/invoked dynamically
according to a context; (ii) Tasks can be interrupted
or changed, adding flexibility to the way that health
activities are performed under a WfMS; (iii) Trace-
ability must be provided to record changes performed,
as well as to allow the improvement of activities by of
analysis the historic data.
Those three aspects allow: to extend a WfMS cre-
ating a tool that maintains the hierarchical nature of
clinical guidelines, to adapt the flow to the context and
to analyse whether performed tasks can be trusted or
HEALTHINF2013-InternationalConferenceonHealthInformatics
82
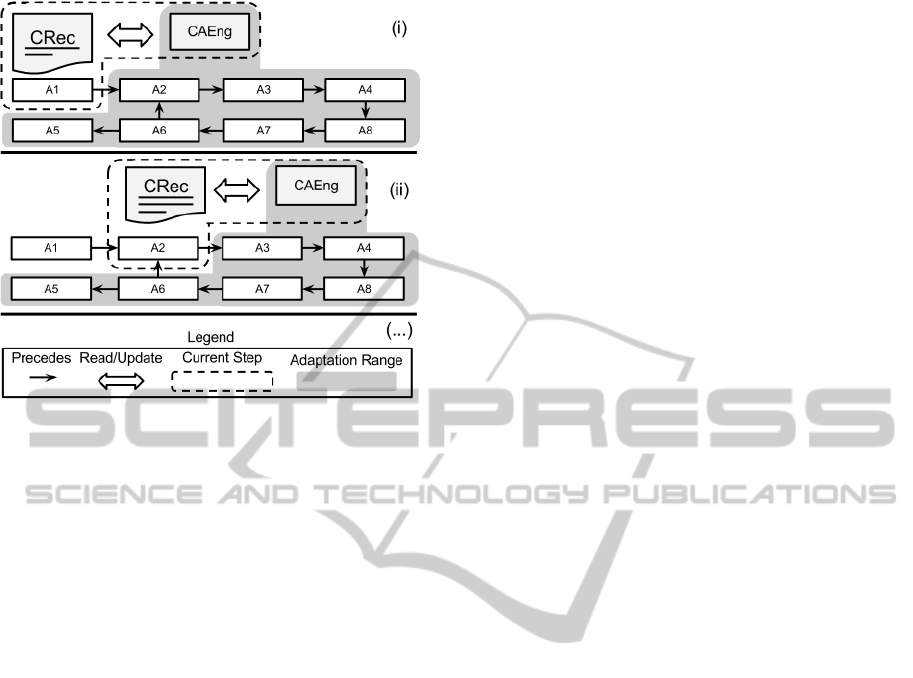
Figure 3: Adaptation of the flow of a workflow.
not. Also, the use of nursing standards contributes to
better adaptation to healthcare workflows.
Future work includes the analysis and definition of
context variables that will be used, resulting on a meta
model and its instantiation. After this step, our model
will be implemented in a scientific WfMS, which will
be compared to the traditional approach, providing
more evidences about advantages and disadvantages
of the approaches.
ACKNOWLEDGEMENTS
Work partially financed by FAPESP (grant
2011/17196-0), the Microsoft Research FAPESP
Virtual Institute (NavScales project), CNPq
(grant 143483/2011-0, MuZOO Project and
PRONEX-FAPESP), INCT in Web Science (CNPq
557.128/2009-9) and CAPES, as well as individ-
ual grants from CNPq. We also thank healthcare
providers from University of Campinas and Univer-
sity of S
˜
ao Paulo, who provide us support in this
research.
REFERENCES
Altintas, I., Berkley, C., Jaeger, E., Jones, M., Ludascher,
B., and Mock, S. (2004). Kepler: an extensible system
for design and execution of scientific workflows. In
Proc. of 16th Intl. Conf. on Scientific and Statistical
Database Management, 2004., pages 423–424. Ieee.
Asfari, O., Doan, B., Bourda, Y., and Sansonnet, J. (2010).
A Context-based Model for Web Query Reformula-
tion. limsi.fr.
Bandara, K., Wang, M., and Pahl, C. (2009). Dynamic Inte-
gration of Context Model Constraints in Web Service
Processes. In Software Engineering. ACTA Press.
Bardram, J. E. and Hansen, T. R. (2010). Context-Based
Workplace Awareness. Computer Supported Cooper-
ative Work (CSCW), 19(2):105–138.
Barga, R., Jackson, J., Araujo, N., Guo, D., Gautam, N.,
Grochow, K., and Lazowska, E. (2008). Trident: Sci-
entific workflow workbench for oceanography. In Ser-
vices - Part I, 2008. IEEE Congress on, pages 465–
466.
Barthelmess, P. (1996). Sistemas de workflow: An
´
alise da
´
area e proposta de modelo. Master’s thesis, Instituto
de Computac¸
˜
ao - Unicamp.
Bolchini, C., Curino, C. A., Quintarelli, E., Schreiber, F. A.,
and Tanca, L. (2007). A data-oriented survey of con-
text models. SIGMOD Rec., 36:19–26.
Carmagnola, F., Cena, F., Gena, C., and Torre, I. (2005). A
semantic framework for adaptive web-based systems.
In Proc. of SWAP, pages 1613–0073. Citeseer.
Cho, Y., Moon, J., and Yoe, H. (2010). LNCS 6018 - A
Context-Aware Service Model Based on Workflows
for u-Agriculture. Technology, pages 258–268.
CNC (2012). Cnc - overview: Nursing outcomes classifica-
tion (noc).
Dang, J., Hedayati, A., Hampel, K., and Toklu, C. (2008).
An ontological knowledge framework for adaptive
medical workflow. Journal of biomedical informatics,
41(5):829–36.
de Clercq, P. and Kaiser, K. (2008). Computer-interpretable
guideline formalisms. Studies in health technology,
pages 22–43.
Deelman, E. and Chervenak, A. (2008). Data Manage-
ment Challenges of Data-Intensive Scientific Work-
flows. 2008 Eighth IEEE Intl. Symposium on Cluster
Computing and the Grid (CCGRID), pages 687–692.
Deelman, E., Gannon, D., Shields, M., and Taylor, I.
(2009). Workflows and e-Science: An overview of
workflow system features and capabilities. Future
Generation Computer Systems, 25(5):528–540.
Dey, A. K. (2000). Providing architectural support for
building context-aware applications. PhD thesis,
Georgia Tech, Atlanta, GA, USA. AAI9994400.
Din, M. A., Abidi, S. S. R., and Jafarpour, B. (2010). On-
tology based modeling and execution of Nursing Care
Plans and Practice Guidelines. Studies in health tech-
nology and informatics, 160(Pt 2):1104–8.
Doenges, M. and Moorhouse, M. (2008). Application of
nursing process and nursing diagnosis: an interactive
text for diagnostic reasoning. G - Reference, Informa-
tion and Interdisciplinary Subjects Series. F.A. Davis.
El-Fakdi, A., Mel
´
endez, J., and Petite, R. (2012). A pro-
posal of a workflow-based cbr for interventional cdss
- application to transcatheter aortic valve implantation
(tavi). In HEALTHINF, pages 201–206.
Fox, J., Patkar, V., Chronakis, I., and Begent, R. (2009).
From practice guidelines to clinical decision support:
closing the loop. Journal of the Royal Society of
Medicine, 102(11):464–73.
TowardsAdaptingScientificWorkflowSystemstoHealthcarePlanning
83

Hollingsworth, D. and Others (1993). Workflow manage-
ment coalition: The workflow reference model. Work-
flow Management Coalition, (1):1–55.
Howe, B., Lawson, P., Bellinger, R., Freire, J., Ander-
son, E., Santos, E., Scheidegger, C., Baptista, A., and
Silva”, C. (2008). End-to-end escience: Integrating
workflow, query, visualization, and provenance at an
ocean observatory. In Proc. of the 2008 Fourth IEEE
Intl. Conf. on eScience”, pages 127–134.
Hull, D., Wolstencroft, K., Stevens, R., Goble, C., Pocock,
M. R., Li, P., and Oinn, T. (2006). Taverna: a tool for
building and running workflows of services. Nucleic
acids research, 34(-):W729–32.
Intl., N. (2012). Nursing Diagnoses: Definitions and Clas-
sification 2012-14 (NANDA Intl. Nursing Diagnosis).
Wiley.
Kholladi, M. and Doan, B. (2010). PRESY: A Context
Based Query Reformulation Tool for Information Re-
trieval on the Web. Annals of Physics, 54(4):258.
Leong, T. Y., Kaiser, K., and Miksch, S. (2007). Free and
open source enabling technologies for patient-centric,
guideline-based clinical decision support: a survey.
Yearbook of medical informatics, (April):74–86.
Lundberg, J. (2007). Principles of workflow support in life
critical situations. Licentiate thesis, School of Engi-
neering, Blekinge Institute of Technology.
Lundberg, J. and Rune, G. (2009). Robust approach towards
context dependant information sharing in distributed
environments. ICEIS09, Milan, Italy.
Medeiros, C. B., Prez-Alcazar, J., Digiampietri, L., Jr., G.
Z. P., Santanch, A., da Silva Torres, R., Madeira, E.,
and Bacarin, E. (2005). Woodss and the web: An-
notating and reusing scientific workflows. SIGMOD
Record, 34(3):18–23.
Mikolajczak, B. and Shenoy, M. (2010). Flexibility through
case handling in careflow systems: A case study of
cutaneous melanoma. In Health Care Management
(WHCM), 2010 IEEE Workshop on, pages 1 –6.
Millard, I. C., Roure, D. D., and Shadbolt, N. (2004). The
use of ontologies in contextually aware environments.
In Indulska, J. and Roure, D. D., editors, Proc. of First
Intl. Workshop on Advanced Context Modelling, Rea-
soning And Management, pages 42–47, Nottingham,
UK.
Ogasawara, E., Murta, L., Werner, C., and Mattoso, M.
(2008). Linhas de Experimento: Reutilizac¸
˜
ao e
Ger
ˆ
encia de Configurac¸
˜
ao em Workflows Cient
´
ıficos.
In 2 E-Science Workshop co-locado ao SBBD/SBES,
pages 31–40.
Panzarasa, S. and Stefanelli, M. (2006). Workflow manage-
ment systems for guideline implementation. Neuro-
logical sciences : official journal of the Italian Neu-
rological Society and of the Italian Society of Clinical
Neurophysiology, 27 Suppl 3:S245–9.
Peres, H. H. C., Cruz, D. D. A. L. M. D., Lima, A. F. C.,
Gaidzinski, R. R., Ortiz, D. C. F., Trindade, M. M. E.,
Tsukamoto, R., and Conceic¸
˜
ao, N. B. (2009). Desen-
volvimento de Sistema Eletr
ˆ
onico de Documentac¸
˜
ao
Cl
´
ınica de Enfermagem estruturado em diagn
´
osticos,
resultados e intervenc¸
˜
oes. Revista da Escola de En-
fermagem da USP, 43(spe2):1149–1155.
Ria
˜
no, D., Real, F., L
´
opez-Vallverd
´
u, J. A., Campana, F.,
Ercolani, S., Mecocci, P., Annicchiarico, R., and Cal-
tagirone, C. (2012). An ontology-based personaliza-
tion of health-care knowledge to support clinical deci-
sions for chronically ill patients. Journal of biomedi-
cal informatics.
Scheidegger, C. E., Vo, H. T., Koop, D., Freire, J., and Silva,
C. T. (2008). Querying and re-using workflows with
VsTrails. Proc. of the 2008 ACM SIGMOD intl. conf.
on Management of data - SIGMOD ’08, page 1251.
Schick, S., Meyer, H., Bandt, M., and Heuer, A. (2012). En-
abling yawl to handle dynamic operating room man-
agement. In Daniel, F., Barkaoui, K., and Dustdar,
S., editors, Business Process Management Workshops
(2), volume 100 of Lecture Notes in Business Infor-
mation Processing, pages 249–260. Springer.
Seyfang, A., Miksch, S., and Marcos, M. (2002). Com-
bining diagnosis and treatment using ASBRU. Intl.
journal of medical informatics, 68(1-3):49–57.
Shahar, Y., Miksch, S., and Johnson, P. (1998). The asgaard
project: a task-specific framework for the application
and critiquing of time-oriented clinical guidelines. Ar-
tificial Intelligence in Medicine, 14(1?2):29 – 51.
Sigsby, L. M. and Campbell, D. W. (1995). Nursing in-
terventions classification: A content analysis of nurs-
ing activities in public schools. Journal of Community
Health Nursing, 12(4):229–237.
Souza, M. V. B. and Augustin, I. (2010). Infer
ˆ
encia de
Atividades Cl
´
ınicas a partir de Propriedades do Con-
texto. Interface, pages 1717–1726.
Strang, T., Linnhoff-popien, C., and Frank, K. (2003).
CoOL: A Context Ontology Language to Enable Con-
textual Interoperability. Ifip Intl. Federation For Infor-
mation Processing, pages 236–247.
Turner, R. (1999). A model of explicit context represen-
tation and use for intelligent agents. Modeling and
Using Context, pages 831–831.
Yamin, A., Augustin, I., da Silva, L. C., Real, R. A., Filho,
A. E. S., and Geyer, C. F. R. (2005). Exehda: adap-
tive middleware for building a pervasive grid environ-
ment. In Proc. of the 2005 conf. on Self-Organization
and Autonomic Informatics (I), pages 203–219, Ams-
terdam, The Netherlands. IOS Press.
Ye, Y., Jiang, Z., Diao, X., Yang, D., and Du, G. (2009). An
ontology-based hierarchical semantic modeling ap-
proach to clinical pathway workflows. Comput. Biol.
Med., 39(8):722–732.
Yuval Shahar, S. M. and Johnson, P. (1998). The Asgaard
project: a task-specific framework for the application
and critiquing of time-oriented clinical guidelines. Ar-
tificial intelligence in medicine, 14(1-2):29–51.
HEALTHINF2013-InternationalConferenceonHealthInformatics
84
