
ECG Biometrics: Principles and Applications
Hugo Silva
1
, Andr
´
e Lourenc¸o
1,2
, Filipe Canento
1
, Ana Fred
1
and Nuno Raposo
3
1
Instituto de Telecomunicac¸
˜
oes, IST-UTL, Lisbon, Portugal
2
DEETC, ISEL-IPL, Lisbon, Portugal
3
Escola Superior de Sa
´
ude, Cruz Vermelha Portuguesa, Lisbon, Portugal
Keywords:
Electrocardiography, Identity Recognition, Biometrics, Biosignal Processing.
Abstract:
Electrocardiographic (ECG) signals have several properties that can greatly complement the existing, and more
established biometric modalities. Some of the most prominent properties are the fact that the signals can be
continuously acquired using minimally intrusive setups, are not prone to produce latent patterns, and provide
intrinsic liveliness detection, opening new opportunities within the area of biometric systems development.
The potential impact of this technique extends to a broad variety of application domains, ranging from the
entertainment industry, to digital transactions. In this paper, we present a framework for ECG biometrics,
with focus on some of the latest developments and future trends in the field, covering multiple aspects of
the problem with the aim of a real-world deployment. Our results so far, further reinforce the feasibility and
interest of the method in a multibiometrics approach.
1 INTRODUCTION
Biometrics is an increasingly growing multibillion
dollar market; a recent report by Global Industry An-
alysts, Inc. (Global Industry Analysts, 2011), esti-
mates that by 2017 revenues will grow above $16 bil-
lion USD.
User recognition techniques, either in an authen-
tication or identification framework, are generally
classified according to their operating principle (Jain
et al., 2011), namely: a) What the person knows (e.g.
passwords); b) What the person has (e.g. identity
card); c) What the person appears to be (e.g. face);
and d) What the person does (e.g. voice). The later
two methods are generally framed in the area of bio-
metric recognition which, in the current state-of-the-
art, includes different types of physical (e.g. finger-
print or iris) and behavioral traits (e.g. signature or
keystroke dynamics), among others.
Despite the fact that biometric systems are highly
advantageous for user recognition, as they provide in-
formation which is more directly related to intrinsic
characteristics of the individual, most of the traits cur-
rently in use today are only practical for momentary,
single validation recognition operations, within a rea-
sonably large time frame. For example, techniques
that rely on the fingerprint and/or hand geometry, re-
quire the user to place or pass the finger and/or hand
in a specific way through a physical reader; tech-
niques that rely on the iris, require the user to stand in
a specific physical space, and to have the eye in line
of sight with the reader; these and other constraints
ultimately limit the scope of application.
The unique properties of ECG signals, are particu-
larly interesting in a multibiometrics approach, either
as a security enhancement layer in hard biometrics
systems, or as a standalone soft biometrics for low
security and low user throughput applications. More
importantly, as it can be continuously measured, it
enables a new class of applications benefitting from
the continuous biometric perspective. In this paper
we present a framework for ECG biometrics, cover-
ing the essential building blocks; experimental results
have been performed, which further reinforce the in-
terest of the ECG-based methods both in an identifi-
cation and authentication approach.
The remainder of the paper is organized as fol-
lows. Sections 2 and 3, present a brief overview of the
state-of-the-art and base principles of Electrocardio-
graphy (ECG). The proposed approach is described
throughout Sections 4, 5, and 6, where the sensor
design, signal processing, and biometric recognition
steps are presented. Experimental results are summa-
rized in Section7, and finally we highlight discussion
topics and outline the main conclusions in Sections 8
and 9.
215
Silva H., Lourenço A., Canento F., Fred A. and Raposo N..
ECG Biometrics: Principles and Applications.
DOI: 10.5220/0004243202150220
In Proceedings of the International Conference on Bio-inspired Systems and Signal Processing (BIOSIGNALS-2013), pages 215-220
ISBN: 978-989-8565-36-5
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)
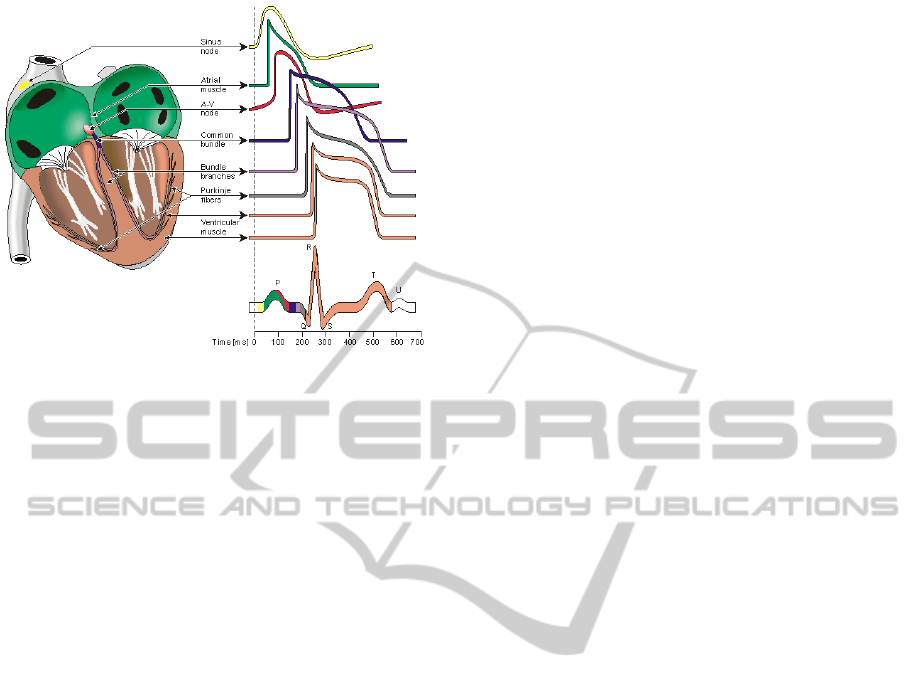
Figure 1: Waveforms of each specialized cells found in the
heart (Malmivuo and Plonsey, 1995).
2 STATE-OF-THE-ART
Recent work has been devoted to the characterization
of ECG features for human identification, and exper-
imental results have highlighted their discriminating
capacity. Still, studies have focused on the offline pro-
cessing of clinical-grade ECG in an on-the-person ap-
proach, with multiple measurement leads. Biel et al.
(Biel et al., 2001) were precursors in the field; in their
initial work a 12-lead setup was used, and with 10
fiducial features the authors reported 100% accuracy
in identification for a population of 20 subjects.
Shen et al. (Shen et al., 2002) experimented on
a group of 20 subjects from the MIT/BIH database
(Goldberger, A. et al., 2000); they achieved 100% ac-
curacy using a combination of template matching and
neural networks. Other experiments were performed
by (Israel et al., 2005) on data from 29 subjects; sig-
nals were collected at the chest and neck, and 12 la-
tency and amplitude features were used. Using LDA,
individual waveforms are classified and mapped to the
identity of the subject by majority voting, leading to
100% identification rates.
Research to date has mostly neglected the speci-
ficities of real-world application scenarios and accept-
ability by the potential end users, which pose sev-
eral constraints and research questions. In the work
by (Silva et al., 2007), the authors have concluded
that a single lead setup suffices; using a V
2
chest
placement, an identification accuracy of 100% was
achieved. Later, a palmar placement has been shown
to perform accurately in the work by (Lourenc¸o et al.,
2011), where for a group of 16 users, even with con-
siderably noisier signals, recognition rates of 94.3%
for identification and an Equal Error Rate (EER) of
10.1% are still achieved.
3 PRINCIPLES OF ECG
To accomplish its function, which is basically to
pump blood to the pulmonary and systemic circula-
tion, the heart generates electrical current, by the con-
traction of its muscle cells. Some of these are special-
ized; the conduction system. These cells have the ca-
pability of self-stimulation, which generates the car-
diac rhythm, usually a regular sequence of heart beats.
The electrical conduction system of the heart is
composed by the sinoatrial node (SA node) that nor-
mally initiates the cardiac cycle, the atrioventricular
node (AV node), the internodal atrial pathways, which
connect the two and regulate the passage of the car-
diac impulse from the atria to the ventricles, and the
bundle of His and corresponding branches, which in
turn are terminated by the Purkinje fibers (Chung,
2000; Malmivuo and Plonsey, 1995). This system
enables the electrical triggering impulses generated
at the SA node, to be propagated from the wall of
the right atrium (where the SA node is located), to
the deeper tissues of the ventricular muscles (through
where the Purkinje fibers are spread).
The ultimate result of this overall bioelectrical ac-
tion is the heartbeat. Figure 1 depicts the contribu-
tion of each specialized group of cells to the heartbeat
waveform (Malmivuo and Plonsey, 1995). The de-
polarization of the atria generates an ECG wave (P
wave), followed by the QRS complex, which repre-
sents the ventricular contraction. The end of the car-
diac cycle is the cell repolarization phase, which ap-
pears as another deflection, the T wave; in some cases,
the a second deflection may appear, the U wave.
When measured non-invasively, the ECG records
the combined contribution of each component of the
electrical conduction system, as propagated to the
body surface, and which is expressed as the typical
P-QRS-T complexes; this effect alone favors the ex-
istence of subject-dependent information, due to the
size, shape, and position of the heart within the chest
cavity, which varies amongst individuals. However,
other factors such as tissue conductivity, genetic sin-
gularities, congenital disorders, and heart conditions,
constitute additional information sources.
Figure 2 illustrates the ECG while at rest, from
two different subjects without any reported heart con-
dition. The plotted individual waveforms y
i
were nor-
malized to the mean wave ¯x computed from the orig-
inal segmented heartbeat waveforms x
i
(eq. 2) and
clipped for better visual understanding. Both subjects
BIOSIGNALS2013-InternationalConferenceonBio-inspiredSystemsandSignalProcessing
216
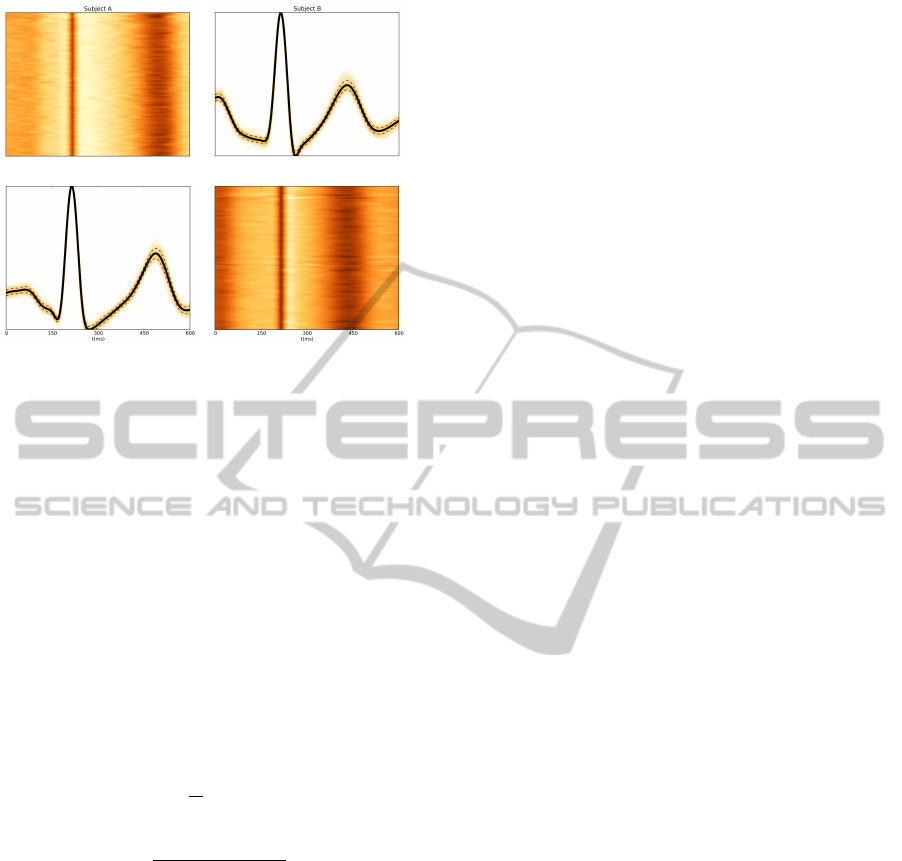
(a) (b)
(c) (d)
Figure 2: Electrocardiographic recordings from two differ-
ent subjects while at rest, where the time series were pro-
cessed to extract one hundred individual heartbeat wave-
forms, which were then clipped and scaled to fit to the
same XX and YY axis limits for better comparison. Fig-
ures 2(b) and 2(c) depict the individual waves overlapped,
with a solid line representing the mean wave, and a dashed
line representing the standard deviation. Figures 2(a) and
2(d) depict a color-map plot, where each line corresponds
to an individual heartbeat wave form, and each column rep-
resents the amplitude value of a sample; in the color-map,
the signal was smoothed around the R peak to enhance the
color intensities in the remaining signal.
exhibit morphologically distinct waveforms, with a
low intersubject variability; the intensity map of the
segmented heartbeat waveforms, showing their tem-
poral evolution, further enhances the differences.
¯x =
1
N
N
∑
i=1
x
i
(1)
y
i
=
x
i
− min( ¯x)
max( ¯x) − min( ¯x)
(2)
Amongst other singularities, in these two cases,
the P-Q and S-T curves and latency are significantly
distinct; the relative amplitude P-T also varies be-
tween subjects. Comparing the ECG of Subject A and
B, we observe for example that the bundle branches
and Purkinje fibers have a lower activation amplitude
in Subject B, or that the AV node recovery time is
lower in Subject A.
The fact that there are subject dependent features
in the ECG, enhances its applicability for user recog-
nition. Furthermore, the ECG has unique properties
when looked at in a multibiometrics approach; in par-
ticular, it is: a) universally available in live subjects;
b) measurable non-intrusively using suitable devices;
c) acceptable due to the latest advances in the sens-
ing technologies; d) not easily circumvented through
latent patterns.
4 SENSOR DESIGN
Conventional clinical-grade ECGs are acquired using
12 or more leads mounted on the chest and limbs, us-
ing conductive paste or gel to lower the electrode/skin
impedance. Part of our work has focused on extend-
ing the state-of-the-art, improving current methods by
developing a sensor for signal acquisition at the hand
palms or fingers. We focused on minimizing the num-
ber of electrical contact points with the subject’s body,
eliminating the need for any gel or conductive paste
in the interface with the skin, and devising a non-
intrusive sensor design for wearable devices and end-
user applications.
A pseudo V
1
bipolar sensor with virtual ground
and dry electrodes was created, consisting of: a) a
differential amplifier with gain 10, input impedance
> 1MΩ, and 110dB CMRR; b) two passive analog
filtering steps composed by a [0.05;100]Hz band pass
filter, and a notch filter to cut off the 50Hz power
line interference; and c) a second amplification stage
with gain 100 to obtain higher resolution from the col-
lected signal. The sensor has only two contact points
with the subject, and works with standard pre-gelled,
dry Ag/AgCl, or conductive textile electrodes.
Experimental results have shown that this setup
provides an adequate signal quality and biometric per-
formance, even when compared with a more tradi-
tional chest setup (Silva et al., 2011; Lourenc¸o et al.,
2011). In the overall, we follow a novel off-the-
person approach, thus making the usability and intru-
siveness comparable to the one found in other bio-
metric traits (e.g. fingerprint). Figure 3 shows the
prototype sensor, which can be used as a standalone
module, or integrated into everyday objects.
5 SIGNAL PROCESSING
5.1 Filtering
As measured at the body surface, ECG signals are af-
fected by multiple noise sources such as motion arti-
facts, and power line or electromyographic noise; this
aspect is event more challenging in the proposed off-
the-person approach, where the impedance between
the electrode and the skin is significantly higher due
to the lack of gel. We designed a digital zero-phase
forward and reverse Butterworth band pass filter with
1 − 30Hz cutoff frequencies, to limit the bandwidth
ECGBiometrics:PrinciplesandApplications
217

(a) Standalone module. (b) Computer panel.
(c) Video game controller. (d) Mobile device.
Figure 3: Sensor integration possibilities of the proposed
approach.
of the raw data. Note that whereas for clinical appli-
cations, a larger passing band is required to preserve
additional fiducia, for biometrics we can optimize the
filtering taking into account the recognition accuracy.
5.2 Segmentation
Our classifier is based on template matching, using
the informative content of the heartbeat waveforms,
and as such, a compatible real-time segmentation al-
gorithm is adopted. We build on the work by (En-
gelse and Zeelenberg, 1979) for offline QRS detec-
tion, and propose a combination strategy that uses
adaptive thresholds estimated along the acquisition
process, according to the methodology and estimation
scheme described in (Christov, 2004; Christov and
Stoyanov, 2002). A comprehensive description of our
proposed approach and comparison between offline
and real-time approaches can be found in (Lourenc¸o
et al., 2012), where the proposed real-time approach
has shown to be competitive. On the ECG biometric
point of view, these algorithms represent an important
contribution towards the real-world deployment.
6 BIOMETRIC RECOGNITION
6.1 Feature Extraction
All segmented heartbeat waveforms are aligned by
their R-peak, and clipped taking into account the typ-
ical physiological latencies between the P-R and R-
T complexes, which are approximately 200 and 400
milliseconds respectively (Chung, 2000). In this pa-
per, the feature vector for each heartbeat waveform
i, consists of a vector x
i
with the waveform ampli-
tude values, which corresponds to 600ms of collected
signal. During the enrollment stage, the patterns x
i
are stored in the database of known users, whereas
in the recognition stage, it is the pattern which will
be checked against the database. Depending on the
latency requirements of the application, we can also
use an average of m feature vectors, which is prone to
further improve the recognition rates.
6.2 Classification
We use an instance-based learning, template matching
approach, through a 1-NN classifier, by computing
the similarity between the feature vectors x
u
extracted
in the recognition phase, and the ones extracted and
stored on the enrollment phase, x
i
. The decision on a
genuine/impostor (authentication task), is determined
by verifying if the Euclidean distance D(x
u
, x
i
), is
below an acceptance threshold, computed from the
database of enrolled users. For identification, the
dissimilarities between the observed pattern x
u
and
the templates from all enrolled users are computed,
and the user identity ˆw
u
is estimated as the class w
i
corresponding to the pattern x
i
with lower distance
D(x
u
, x
i
), that is, ˆw
u
= w
i
: i = argmin
i
(D(x
u
, x
i
)).
7 EXPERIMENTAL EVALUATION
Tests were performed on 32 healthy individuals (25
males) with 31.1±9.46 years, using the proposed sen-
sor setup. Subjects were asked to rest their left/right
hands over the sensor leads, and data was acquired
during a period of approximately 1m30s, during
which the experiment supervisor explained the pur-
pose of the study. Raw signals were processed ac-
cording to the proposed approach, separated into a
training set with 30% of the total collected patterns,
and a test set with the remaining 70% of the patterns.
We evaluated the user recognition potential of
ECG signals collected at the hand palms using di-
rectly the individual heartbeat waveforms directly,
and also the mean waves computed from a variable
number, m, of waveforms. The template matching
technique is extremely lightweight in terms of real-
time processing, and the mean waves reduce the pat-
tern variability, which is particularly suitable in a real-
time framework.
BIOSIGNALS2013-InternationalConferenceonBio-inspiredSystemsandSignalProcessing
218
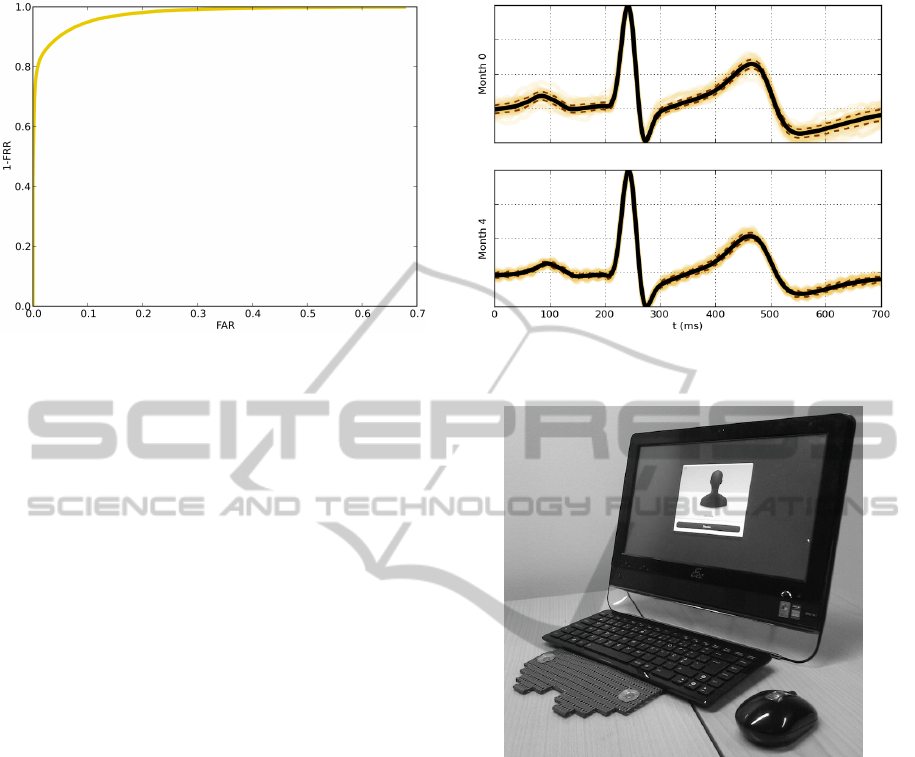
Figure 4: ROC curve for the m = 5 best case scenario; m de-
notes the number of waves used to compute the mean wave.
Table 1 shows the Equal Error Rate (EER) for au-
thentication and Identification Error (EID) varying the
number of patterns m used on the computation of the
mean waves. When individual heartbeat waveforms
are used, a mean EER of 9.39% ± 0.19 is obtained
in authentication, which decreases to 2.75% ± 0.29
when averages of 5 waveforms are used; for identifi-
cation, a mean EID of 17.62% ± 0.59 is obtained us-
ing individual heartbeat wave forms, which decreases
to 5.61% ± 0.94, when averages of 5 waveforms are
used. The 1 and 5 heartbeats cases correspond, re-
spectively, to 1s and 5s of acquired signals. The
Receiver Operating Characteristics (ROC) curve for
the m = 5 best case scenario, is presented in Figure 4.
Our results hold comparable performance when
matched to other modalities; even when compared to
previous ECG based approaches. Table 2, summa-
rizes the user recognition results typically found in
the literature for other biosignal based modalities (see
(Gamboa, 2008) and references therein). Although
the traditional V
2
ECG lead approaches achieve higher
accuracy levels, our results, besides holding compa-
rable results, also provide a good compromise be-
tween performance and acceptability. Our experi-
mental setup provides usability levels similar to those
found in the most widespread modalities, and can be
easily integrated into everyday use devices without
impacting on the users normal activities, potentiating
its use in a continuous biometrics framework.
8 DISCUSSION
Experimental evaluation with real-world data, has re-
vealed an EER of 2.75% ±0.29 in authentication and
5.61% ± 0.94 EID in identification within a group of
32 subjects. Our system can be further optimized de-
Figure 5: Example of signals collected on two different mo-
ments in time (approximately 4 months appart).
Figure 6: Experimental hardware and software prototype.
pending on the application scenarios. In our previous
paper (Silva et al., 2012), a variation of the proposed
approach was used to evaluate the applicability of our
method to in-vehicle driver recognition. An impor-
tant aspect within ECG biometric systems, which has
been marginally covered in the state-of-the-art is the
stability of the signals over time. Preliminary results
from our work have shown that, in similar acquisi-
tion conditions, the heartbeat waveforms retain a great
part of their informative content over time. Figure 5,
shows an example of two heartbeat waveforms col-
lected with a 4 months interval in one test subject; the
waves are normalized by the maximum and minimum
value for easier comparison, and as we can observe,
both show a high morphological resemblance.
ECGBiometrics:PrinciplesandApplications
219

Table 1: EER and EID for the proposed approach over 30 runs where exclusive training and test sets were randomly selected.
m 1 2 3 4 5
EER 9.39% ±0.19 6.05% ±0.36 4.55% ±0.41 3.13% ±0.41 2.75% ±0.29
EID 17.62% ±0.59 11.94% ±0.96 8.71% ±0.85 6.72% ±0.82 5.61% ±0.94
Table 2: EER for other behavioral biometric approaches.
Method Key Stroke Mouse Voice Gait Eye Gaze EEG ECG V
2
EER ∼ 4% ∼ 10% ∼ 10% ∼ 5% ∼ 5% ∼ 10% ∼ 5%
9 CONCLUSIONS
In this paper we have presented an overview of the
base principles and applications of ECG biometrics.
If we analyze the ECG in a multibiometrics perspec-
tive, it sets an important ground for novel biomet-
ric applications, especially those related to continu-
ous user recognition. Results so far are encouraging,
which have led us to create an initial prototype sys-
tem (Figure 6). Immediate applications of our tech-
nology include scenarios of low security and low user
throughput, such as recognition in mobile phones,
laptop computers, cable TV interfaces, and user-tuned
in-game experience. If combined with other modali-
ties, there are several use cases where the ECG stands
as an important add-on. For example high security
applications, we can envision scenarios where user
recognition is periodically performed using a hard
biometrics such as the fingerprint, ECG data is col-
lected simultaneously with the fingerprint to extract
a heartbeat waveform template, and after the initial
identity validation using the hard biometric modality,
the ECG continues to enable the validation of the user.
ACKNOWLEDGEMENTS
This work was funded by Fundac¸
˜
ao para a
Ci
ˆ
encia e Tecnologia (FCT) under the grants
SFRH/BD/65248/2009 and SFRH/PROTEC/49512/
2009, and by the Instituto de Telecomunicac¸
˜
oes un-
der the grant ”Android Biometric System”.
REFERENCES
Biel, L., Petterson, O., Phillipson, L., and Wide, P. (2001).
ECG analysis: A new approach in human identifica-
tion. IEEE Transactions on Instrumentation and Mea-
surement, 50(3):808–812.
Christov, I. I. (2004). Real time electrocardiogram QRS
detection using combined adaptive threshold. Biomed
Eng Online, 3(1).
Christov, I. I. and Stoyanov (2002). Steep slope method
for real time QRS detection. Electrotechniques and
Electronics, pages 13–17.
Chung, E. K. (2000). Pocketguide to ECG Diagnosis.
Blackwell Publishing Professional.
Engelse, W. A. H. and Zeelenberg, C. (1979). A single scan
algorithm for QRS-detection and feature extraction.
Comp. in Cardiology, 6:37–42.
Gamboa, H. (2008). Multi-Modal Behavioural Biometrics
Based on HCI and Electrophysiology. PhD thesis,
IST-UTL.
Global Industry Analysts, I. (2011). Biometrics - a global
strategic business report. T. Rep. GIA, Inc.
Goldberger, A. et al. (2000). PhysioBank, physiotoolkit,
and physionet: Comp. of a new research res. for com-
plex physiologic signals.
Israel, S., Irvine, J., Cheng, A., Wiederhold, M., and
Wiederhold, B. (2005). ECG to identify individuals.
Pattern Recognition, 38(1):133–142.
Jain, A. K., Ross, A. A., and Nandakumar, K. (2011). In-
troduction to Biometrics. Springer.
Lourenc¸o, A., Silva, H., and Fred, A. (2011). Unveiling
the biometric potential of Finger-Based ECG signals.
Comp. Intell. and Neuroscience, 2011.
Lourenc¸o, A., Silva, H., Leite, P., Lourenc¸o, R., and Fred,
A. (2012). Real time electrocardiogram segmenta-
tion for finger based ECG biometric. In BIOSIGNALS
2012, pages 49–54.
Malmivuo, J. and Plonsey, R. (1995). Bioelectromagnetism:
Principles and Applications of Bioelectric and Bio-
magnetic Fields. Oxford Press.
Shen, T. W., Tompkins, W. J., and Hu, Y. H. (2002). One-
lead ECG for identity verification. In Proc. of the
IEEE EMBS ’02 Conference.
Silva, H., Gamboa, H., and Fred, A. (2007). Applicability
of lead v2 ECG measurements in biometrics. In Proc.
of the Med-e-Tel Forum.
Silva, H., Lourenc¸o, A., and Fred, A. (2012). In-vehicle
driver recognition based on hand ECG signals. In
Proc. of the IUI ’12 Conf., IUI ’12.
Silva, H., Lourenc¸o, A., Lourenc¸o, R., Leite, P., Coutinho,
D., and Fred, A. (2011). Study and eval. of a sin-
gle differential sensor design based on electro-textile
electrodes for ECG biometrics applications. In Proc.
of the IEEE Sensors Conf.
BIOSIGNALS2013-InternationalConferenceonBio-inspiredSystemsandSignalProcessing
220
