
Assessment of 3D Scanners for Modeling Pectus Carinatum
Corrective Bar
António H. J. Moreira
1,2
, João Gomes Fonseca
2
, Pedro L. Rodrigues
1,2
, Jaime C. Fonseca
1,5
,
A. C. M. Pinho
6
, Jorge Correia-Pinto
2
, Nuno F. Rodrigues
3,4
and João L. Vilaça
1,2,3
1
Centro ALGORITMI, School of Engineering, University of Minho, Guimarães, Portugal
2
ICVS/3B’s - PT Government Associate Laboratory, Braga/Guimarães, Portugal
3
DIGARC, Polytechnic Institute of Cávado and Ave, Barcelos, Portugal
4
HASLab / INESC TEC –University of Minho, Braga, Portugal
5
DEI, Industrial Electronics Department, University of Minho, Guimarães, Portugal
6
DEM, Mechanical Department, University of Minho, Guimarães, Portugal
Keywords: 3D Scanner, Kinect, FastSCAN, Pectus Carinatum, Surface Mesh, 3D Reconstruction.
Abstract: Pectus Carinatum (PC) is a chest deformity consisting on the anterior protrusion of the sternum and
adjacent costal cartilages. Non-operative corrections, such as the orthotic compression brace, require
previous information of the patient chest surface, to improve the overall brace fit. This paper focuses on the
validation of the Kinect scanner for the modelling of an orthotic compression brace for the correction of
Pectus Carinatum. To this extent, a phantom chest wall surface was acquired using two scanner systems –
Kinect and Polhemus FastSCAN – and compared through CT. The results show a RMS error of 3.25mm
between the CT data and the surface mesh from the Kinect sensor and 1.5mm from the FastSCAN sensor.
1 INTRODUCTION
Pectus Carinatum (PC) is a chest deformity
characterised by the anterior projection of the
sternum and adjacent costal cartilages. The
deformity is caused by a disproportionate growth of
the costal cartilages, compared to the thoracic
skeleton, resulting in a protrusion with symmetric or
asymmetric overgrowth (Golladay ES., 2003).
Nowadays, several authors propose non-
operative corrections, such as the body cast or the
orthotic compression brace (OCB) (Frey et al.,
2006).
Due to the symmetric or asymmetric nature of
the deformity, some studies report better outcomes
with a custom-fitted OCB (Egan et al., 2000).
Currently, this procedure is performed using
rough measurements, which may lead to future
adjustments in OCB design; or CT-scan with
radiation dosage; or, in few cases, precision 3D
scanners which are costly (Philippe et al., 2007).
In this paper our primary focus is the validation
of the Kinect sensor as a handheld scanner for
modelling Pectus Carinatum OCB. To this extent, it
is compared and discussed the differences between
the 3D scans and errors that affect the OCB
modelling from a software using Kinect
(ReconstructMe), the mesh from an available
handheld scanner (Polhemus FastSCAN) and the
mesh from the CT-Scan as reference.
The paper proceeds with the description of the
acquisition procedure and reliability assessment for
a phantom model, and also the measurements for the
OCB modelling. In Section 3, the errors obtained
from different scans and OCB measurements are
presented. The paper concludes with some
observations and future improvements in Section 4.
2 METHODS
2.1 3D Scanning
2.1.1 FastSCAN
The Polhemus FastSCAN™ Cobra is a handheld
scanner which uses a camera and a laser to
triangulate a 3D stripe. An electromagnetic tracking
system is used to track the scanner wand location in
the 3D space.
Resolution along the laser line depends on wand-
object range, typically 0.5mm at 200mm range and it
122
H. J. Moreira A., Gomes Fonseca J., L. Rodrigues P., C. Fonseca J., C. M. Pinho A., Correia-Pinto J., F. Rodrigues N. and L. Vilaça J..
Assessment of 3D Scanners for Modeling Pectus Carinatum Corrective Bar.
DOI: 10.5220/0004300901220125
In Proceedings of the International Conference on Computer Vision Theory and Applications (VISAPP-2013), pages 122-125
ISBN: 978-989-8565-48-8
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

can reach resolutions as low as 0.1mm. The distance
between transmitter (small ranger) and wand is
limited to a radius of 310mm, so a good accuracy is
achieved (0.75mm) within a 600mm sphere centered
on the reference source (Polhemus, 2012).
2.1.2 3D Kinect (Reconstructme Software)
Kinect is a device composed by one Infra-Red (IR)
projector, one IR camera and one RGB camera. The
IR projector and IR camera are used to triangulate
the points in space, and to estimate the depth by
measuring the disparities captured by the IR camera
(Smisek et al., 2011); (Khoshelham and Elberink,
2012).
The operating range of the sensor is between 0.4
meters to 5 meters. At the range of 2 meters, one
level of disparity corresponds to 1 cm. Thus, to
increase the depth resolution for acquisitions with
Kinect, the acquisition range is limited to 0.4 meters
up to 1.2 meters. According to Khoshelham et. al.,
the standard deviations of depth resolution at 1.5
meters can be as high as 0.5 cm.
The software ReconstructMe (Non-commercial
version 405), developed by PROFACTOR GmbH,
was used to build the surface meshes.
(ReconstructMe, 2012). Essentially, ReconstructMe
uses depth acquisitions to represent 3D points,
which characterize a 3D scene.
2.2 Reliability Assessment
In order to access and validate the differences
between scanners capability to scan the human chest
wall, a phantom (Training Model “ABDFAN” -
Kyoto Kagaku Co., Ltd) was used in this analysis.
The usage of Kinect is then evaluated for OCB
measures by assessing its similarity with FastSCAN
and CT-Scan results.
The surface mesh reconstructed from the CT-
data is used as the ground-truth in this study. The
volume resolution is 512×512×241 with voxel
dimensions of 0.684×0.684×1mm, the 241 axial
slices were acquired with the HiSpeed CT/e™ (GE
Medical Systems).
The surface contours from the segmented slices
are used to reconstruct the final mesh, see Figure 1.
Figure 1: Surface mesh from CT-scan.
Two different setups were performed:
- Movement - the scanner moves around a static
object;
- Static - the scanner is fixed and the object moves
in front of it.
To improve the static mode, the object is fixed in
a support which allows 360 degrees rotation. For
each mode and scanner, 10 meshes were acquired.
2.2.1 Repeatability
The FastSCAN scanner is operator dependent, since
the mesh precision depends of the distance between
the wand and the reference. Occlusion is another
problem which brings the necessity of extra sweeps.
Therefore, to overcome these limitations, some post-
processing was applied to the meshes. First, the
sweeps were slightly registered to decrease the
distances between them. Then, smooth and decimate
operators were applied to the merged meshes
The repeatability was also studied in Kinect
based on ReconstructMe software with default
settings.
To analyse the repeatability, the CloudCompare
software running the ICP algorithm was used to
align the meshes. Two hundred thousand sampling
points were used. Then, the registration was
validated by Root-Mean-Square (RMS) error
between meshes. The distance between meshes was
computed assigning each point of the compared
mesh to the nearest-neighbour point in the reference
mesh.
Four different setups were defined and, for each,
10 meshes were acquired. To compute the
repeatability, the described process was applied to
all meshes. To reduce the influence of the
registration in error measurements, due to different
number of vertexes per mesh, the comparisons were
made through the combination of all meshes, using
all of them as reference. In each setup 90
comparisons were computed.
2.2.2 Accuracy
This subsection describes how the meshes accuracy
was accessed. Accuracy represents the distance
between the corresponding points of the surface
mesh acquired from the scanner and the ground-truth
surface mesh.
Here, they were applied the same steps of the
repeatability, however, for this case, the acquired
meshes were compared with ground-truth mesh built
from the CT-scan. The accuracy is measured and
compared in the four setups, resulting in a total of 40
comparisons.
Assessmentof3DScannersforModelingPectusCarinatumCorrectiveBar
123
2.3 OCB Modelling
Usually, the OCB is modelled by taking
measurements from CT-Scan or, if there is no
available patient CT-Scan, measured manually in the
patient. In the CT-data, one slice is chosen at the
point of greatest protrusion. The measurements for
modelling the OCB are the transverse diameter of
the thorax (Figure 2 – A), the right and left
hemithorax distance (Figure 2 – B and C) and the
thorax perimeter. The curvature of the anterior and
posterior elements of the OCB (Figure 2 – D
a
and
D
p
) are modelled following the lateral tangential
curvature of the chest.
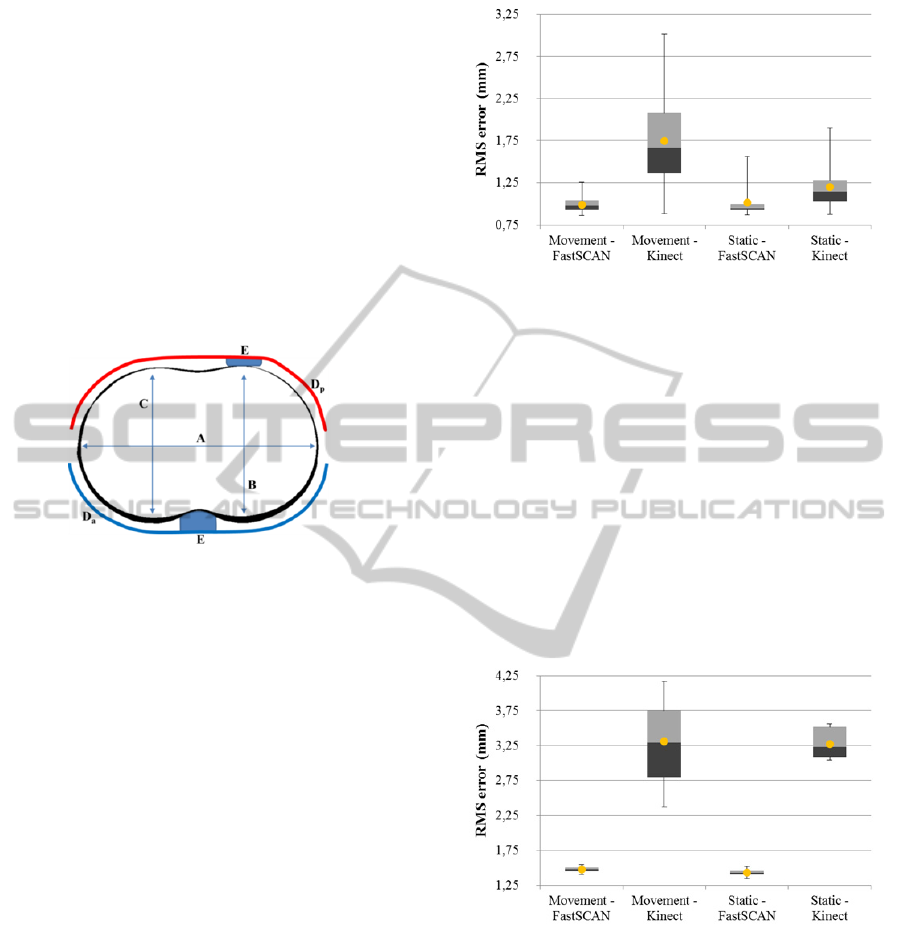
Figure 2: Measurements for modelling the OCB: A –
transverse diameter of the thorax; B and C –
anteroposterior distance of the right and left hemithorax.
D
a
and D
p
– anterior and posterior elements of the OCB, E
– Contact pillow/support.
To realise if the OCB modelling can be achieved
using 3D scanners, the defined measurements were
computed in both scan meshes and compare to the
CT-Scan mesh in the greatest protrusion point.
3 RESULTS AND DISCUSSION
For each scan preformed with the Kinect, the
phantom was turned around 360º, at least 3 times, to
minimize random noise.
When the mean and standard deviation were
computed, the outliers were eliminated using
99.73% (3σ
) of the total data for each mesh
comparison.
3.1 Repeatability
The results reveal that the Kinect acquisition based
on ReconstructMe has higher errors for both modes.
The RMS errors, obtained from registration, are
reported in Figure 3.
As the differences are not substantial, it is possible
to mention that FastSCAN performs repeatable
Figure 3: Repeatability - Boxplot results of the RMS error
for the four setups. Mean value is represented by the
yellow dot.
acquisitions in both modes. Using Kinect, the results
reveal that repeatability is higher when the sensor
stays static and the object moves. When the Kinect
is used as a handheld scanner (movement mode), the
influence of the operator is verified - on average
higher than 0.5mm.
3.2 Accuracy
The accuracy results are presented in Figure 4,
revealing that FastSCAN is more accurate than
Kinect.
Figure 4: Accuracy - Boxplot results of the RMS error for
the four setups for. Mean value is represented by the
yellow dot.
On average, the accuracy differences between
scanners are higher than 1.8mm in RMS error.
Although, when comparing acquisition modes
(movement and static), these do not greatly
influence the resulting meshes in either scanners.
3.3 Corrective Bar Similarity
Thorax perimeter, transverse diameter, left and right
hemithorax distances are reported in table 1. This
VISAPP2013-InternationalConferenceonComputerVisionTheoryandApplications
124
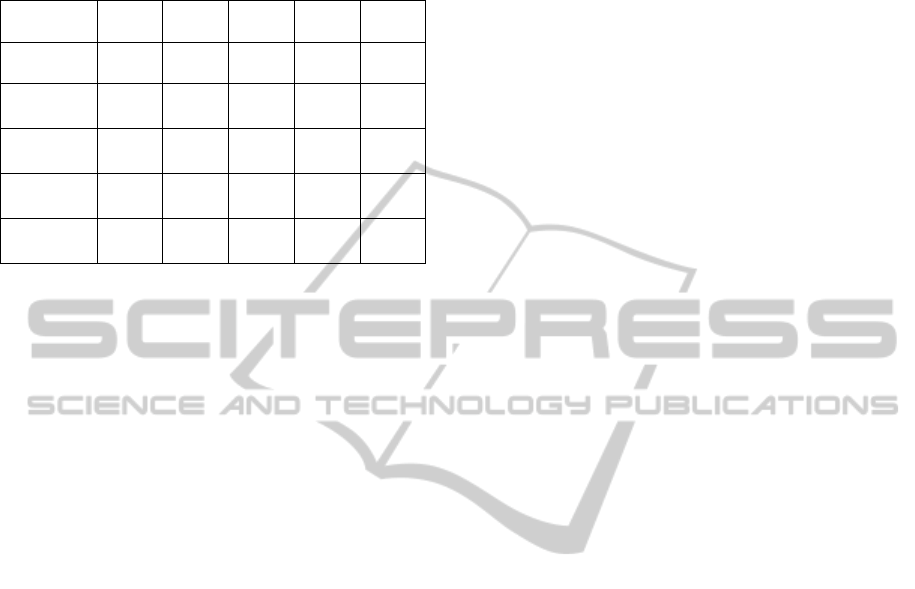
table describes the mean values of the 10 meshes of
each setup.
Table 1: OCB thorax mean distances, in millimetres.
Setup TP TTD
Left
HTD
Right
HTD
%
CT (Ref) 858,02 338,38 218,06 216,69
Kinect
(MM)
842,30
±6,28
332,29
±1,72
211,16
±1,49
211,03
±3,87
97,65
±0,93
Kinect
(SM)
855,60
±7,07
∆
328,38
±0,96
206,00
±1,74
216,10
±0,85
∆
97,74
±0,57
FastSCAN
(MM)
865,85
±2,78
339,77
±0,49
∆
217,93
±1,02
∆
218,88
±0,54
□
100,57
±0,30
FastSCAN
(SM)
853,35
±3,54
□
334,45
±0,71
□
215,63
±0,95
□
213,21
±0,61
98,89
±0,33
TP – thorax perimeter; TTD - thorax transverse distance; HTD –
Hemithorax distance; % - percentage of similarity with CT-data;
SM – static mode; MM – movement mode. ∆ - best result; □ –
second best result.
The best performance was achieved using the
FastSCAN in MM setup (see Table 1 - %). Also, the
overall best results are achieved with FastSCAN
scanner in both modes, MM and SM.
Observing the difference of similarity in Kinect
(~2.5%), this can result in mean error between 5mm
and 16mm, affecting the OCB modelling. In the
FastSCAN case, with difference of similarity lower
than 1.2%, the worst mean error is 7.8mm.
4 CONCLUSIONS
FastSCAN has revealed to be the most accurate and
precise scanner. Kinect, with ReconstructMe
software, has proved to be a well capable system for
the acquisition of 3D objects, demonstrating a RMS
accuracy error up to 3mm, higher than FastSCAN
(~1.5mm), when compared to ground-truth. Also, it
shows less level of detail than FastSCAN.
Since Kinect is a static acquisition system, it
shows more variability when used as a handheld.
Unlike it, FastSCAN remains stable in both motion
setups, SM and MM.
One major drawback of FastSCAN system is its
cost when compared to Kinect.
Future improvements in Kinect registration and
depth field sensor can expand the usage of this
scanner as a low-cost handheld device allowing for
fast and precise remote scans for custom-fitted OCB
modelling.
ACKNOWLEDGEMENTS
The authors acknowledge to Foundation for Science
and Technology (FCT) - Portugal for the fellowships
with the references: UMINHO/BI/95/2012;
SFRH/BD/68270/2010; SFRH/BD/74276/2010 and
SFRH/BPD/46851/2008. This work was also
supported by FCT R&D project PTDC/SAU-
BEB/103368/2008.
REFERENCES
Golladay, E. S., 2003. Pectus carinatum and other
deformities of the chestwall. In Ziegler, M. M.,
Azizkhan, R. G., Weber, T. R. Operative pediatric
surgery. New York (NY) McGraw-Hill, p. 269-77.
Frey, A. S., Garcia, V. F., Brown, R,L,, Inge, T. H.,
Ryckman, F.C., Cohen, A. P., Durrett, G., Azizkhan,
R. G., 2006. Nonoperative management of pectus
carinatum. In J Pediatr Surg, 41, p. 40-5.
Egan, J. C., DuBois, J. J., Morphy, M., et al., 2000.
Compressive orthotics in the treatment of asymmetric
pectus carinatum: a preliminary report with an
objective radiographic marker. In J Pediatr Surg, 35,
p. 1183-6.
Philippe Poncet, Dragan Kravarusic, Tessa Richart,
Rhiannon Evison, Janet L. Ronsky, Ali Alassiri, David
Sigalet, Clinical impact of optical imaging with 3-D
reconstruction of torso topography in common anterior
chest wall anomalies, Journal of Pediatric Surgery,
Volume 42, Issue 5, May 2007, 898-903.
Smisek, J., Jancosek, M., Pajdla T., 2011. 3D with Kinect.
In IEEE International Conference on Computer Vision
Workshops, p.1154-60.
Khoshelham, K., Elberink, S. O., 2012. Accuracy and
Resolution of Kinect Depth Data for Indoor Mapping
Applications. In Sensors, 12, p. 1437-54.
Polhemus, 2012. http://www.polhemus.com/ (accessed
August 2012).
ReconstructMe, 2012. http://reconstructme.net/ (accessed
August 2012).
Assessmentof3DScannersforModelingPectusCarinatumCorrectiveBar
125
