
Additional Pulmonary Blood Flow in the Cavopulmonary
Anastomosis by Means of a Modified Blalock-Taussig Shunt
Is It a Beneficial Clinical Option?
Giuseppe D’Avenio
1
, Antonio Amodeo
2
and Mauro Grigioni
1
1
Technology and Health, Istituto Superiore di Sanità, Rome, Italy
2
Pediatric Hospital “Bambino Gesù”, Rome, Italy
Keywords: Cardiac Surgery, Congenital Heart Disease, Mathematical Modelling.
Abstract: Since many years, patients with functionally single ventricles are subjected to surgical operations, meant to
create a more favourable haemodynamics. The bidirectional cavopulmonary anastomosis (BCPA) is one of
such operations, and is principally meant to prepare a future total cavopulmonary anastomosis, i.e., the
direct connection of the two vene cavae to the pulmonary arteries. Since the circulation ensuing from a
BCPA is basically composed of two circuits in parallel, the upper and the lower circulation, the latter being
external to the lung perfusion, there is a potential problem of low oxygen saturation. It has been proposed
that an additional pulmonary blood flow, such as that imparted by a modified Blalock-Taussig shunt could
be beneficial as for the oxygen saturation. In the present study, this hypothesis is verified by means of a
lumped parameter model, considering different degrees of shunting. The results support the view that an
additional source of blood flow can have a beneficial effect on the pediatric patient operated on with a
BCPA. Future comparison of numerical results with actual clinical data will allow to evaluate the predictive
capabilities of the model.
1 INTRODUCTION
Since many years, patients with functionally single
ventricles are operated on with one (or more, in
various stages at different patient’s ages) of a series
of surgical operations. In fact, these patients present
congenital hindrances to the normal circulation,
undermining the physiological circulation and tissue
oxygenation. The bidirectional cavopulmonary
anastomosis (BCPA) is one of the operations dealing
with the treatment of such patients, and is principally
meant to prepare a future total cavopulmonary
anastomosis, i.e., the connection with the two vene
cavae connected directly to the pulmonary arteries.
This connection is particularly important in the
treatment of hypoplastic left heart syndrome
(HLHS), when the functional right ventricle must be
gradually prepared to bear the load associated to the
circulation (Goldberg and Gomez, 2003).
Since the circulation ensuing from a BCPA is
basically composed of two circuits in parallel, the
upper and the lower circulation, the latter being
external to the lung perfusion, there is a potential
problem of low oxygen saturation: the lower
circulation is only oxygenated by the mixing with
the blood from the pulmonary veins, in the right
atrium (RA), hence the blood in the inferior part of
the systemic circulation can be hypooxygenated,
especially during exercise conditions. It has been
proposed that an additional pulmonary blood flow,
such as that imparted by a modified Blalock-Taussig
shunt could be beneficial as for the oxygen
saturation (Caspi et al., 2003). This hypothesis needs
to be put to test in clearly controllable conditions,
such as those provided by a mathematical model of
the circulation. In the present study, the beneficial
role of an additional pulmonary blood flow is tested
by means of a lumped parameter model, which is a
generalization of that proposed by (Santamore et al.,
1998).
The effects of various degrees of shunting are
discussed, in order to evaluate whether such an
operation actually constitutes an advantage over the
traditional BCPA. The model of the operation has
not yet been validated with a point-to-point
comparison with clinical data, but the clinical
reports available in the literature allow at least a
qualitative assessment of the model.
392
D’Avenio G., Amodeo A. and Grigioni M..
Additional Pulmonary Blood Flow in the Cavopulmonary Anastomosis by Means of a Modified Blalock-Taussig Shunt - Is It a Beneficial Clinical Option?.
DOI: 10.5220/0004328003920395
In Proceedings of the International Conference on Bio-inspired Systems and Signal Processing (BIOSIGNALS-2013), pages 392-395
ISBN: 978-989-8565-36-5
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)
2 MATERIALS AND METHODS
With reference to the modelling of the BCPA
proposed by Santamore et al., suitable modifications
can be provided to account for the presence of an
additional contribution to the pulmonary flow, such
as that imparted by a Blalock-Taussig shunt. Fig. 1
presents an instance of this operation, meant to
increase pulmonary blood flow by surgical means.
Figure 1: The modified Blalock-Taussig shunt is meant to
enhance the pulmonary flow, by deriving a fraction of the
blood from the subclavian artery to the pulmonary arteries
(figure downloaded from http://upload.wikimedia.org/
wikipedia/commons/thumb/6/63/Blalock_shuntWiki.jpg/2
20px-Blalock_shuntWiki.jpg).
For the total oxygen consumption
2
O
V
, it can be
stated that
2222
1
OsOsOO
VkkVkVkV
(1a)
k being the fraction of the whole body oxygen
consumption relative to used by the upper body,
while
s
k is the fraction of the same quantity which
can be attributed to the part of the circulatory system
constituted by the shunt. Eq. (1a) states that the
oxygen consumption in the lower body is
2
1
Os
Vkk
. It is natural to assume that 0
s
k ,
so that
222
1
OOO
VkVkV
(1b)
The rate of oxygen supply in the inferior (IVC) and
susperior vena cava (SVC) is given by Eqs. 2 and 3,
respectively:
IVCOIVCOIVCOa
QCVkQC
222
,,
1
(2)
SVCOSVCOSVCOa
QCVkQC
222
,,
(3)
These formulas relate the oxygen content in the
aorta,
2
,Oa
C
, and the rate of oxygen consumption in
the whole body,
2
O
V
, to the oxygen content in the
lower and upper body circulation,
2
,OIVC
C
and
2
,OSVC
C respectively.
Since the pulmonary flow is given in this case by
two contributions, the following formula applies:
shuntSVCP
QQQ
(4)
where
shunt
Q is the flow rate across the shunt
connecting the aorta and the PAs.
In the usual BCPA, i.e., without additional
sources of pulmonary blood flow, the mass
conservation in Eq. (4) is simplified as
SVCP
QQ .
The balance of oxygen content in the pulmonary
circulation leads to
POPV
LOshuntOshuntSVCOSVC
QC
VQCQC
2
222
,
,,,
(4b)
The combined cardiac output can be expressed as
SVCIVC
QQCO
(5)
In a steady state, the oxygen provided by the lungs is
equal to that consumed in the body, i.e.,
22
, OLO
VV
(6)
From Eq. (4b), after substitution of the term
SVCOSVC
QC
2
,
with the left-hand side of Eq. 3,
POPV
LOshuntOshuntOSVCOa
QC
VQCVkQC
2
2222
,
,,,
Since
22
,, OaOshunt
CC
, this equation can be
rewritten as
shuntSVCOPV
OshuntSVCOa
QQC
VkQQC
2
22
,
,
1
(7)
In the derivation, use has been made of Eq. (6).
Since (rearranging Eq. 5)
shuntSVC
QQ
shuntIVC
QQCO
, from Eq. (7) we can write the
following expression, useful to derive the oxygen
delivery to the arterial system:
IVCOPVIVCOaO
shuntOPVshuntOa
QCQCVk
QCOCQCOC
222
22
,,
,,
1
(8)
Dividing Eq. (7) by
shuntSVC
QQ
and multiplying
it by
IVC
Q , we derive the formula:
AdditionalPulmonaryBloodFlowintheCavopulmonaryAnastomosisbyMeansofaModifiedBlalock-TaussigShunt-Is
ItaBeneficialClinicalOption?
393
shuntSVC
IVC
O
IVCOPVOa
QQ
Q
Vk
QCC
2
22
1
,,
(9)
This expression for
IVCOPVOa
QCC
22
,,
can be
substituted at the right-hand side of Eq. (8), to give
the result
shuntSVC
IVC
OO
shuntOPVshuntOa
QQ
Q
VkVk
QCOCQCOC
22
22
11
,,
shuntSVC
IVC
O
shuntOPV
QQ
Q
Vk
QCOC
11
2
2
,
and finally
shuntOa
QCOC
2
,
(10)
x
x
VkQCOC
OshuntOPV
1
1
22
,
where the position
IVCshuntSVC
QQQx / has
been made.
Eq. (10) is a generalization of the formula
provided by (Santamore et al. 1998) for the case of a
BCPA without additional source of pulmonary flow.
Of course, the two formulas coincide for
0
shunt
Q .
In order to evaluate the effect of the systemic-to-
pulmonary shunt, we assume in the following that
COQ
shunt
, hence different degrees of shunting
will be considered, by means of
, the fraction of
the CO which is driven into the systemic-to-
pulmonary shunt. From Eq. 10, the value of systemic
oxygen delivery (
COC
Oa
2
,
) can be immediately
derived. Furthermore, with some additional
derivations, the value of oxygen saturation, both
globally and regionally (in the lower and upper
circulation) can be calculated, similarly to the
approach in (Santamore et al., 1998).
3 RESULTS
The results of the simulation indicate that there is an
overall improvement in blood oxygen saturation
level, either globally or at the regional (IVC or SVC)
level, as a function of the parameter
.
It must be underlined that the values for the
SVC/IVC ratio in the figures hereby reported are in
the physiological range (
IVCSVC
QQ / comprised
between 35/65 and 65/35), as in (Salim et al., 1995).
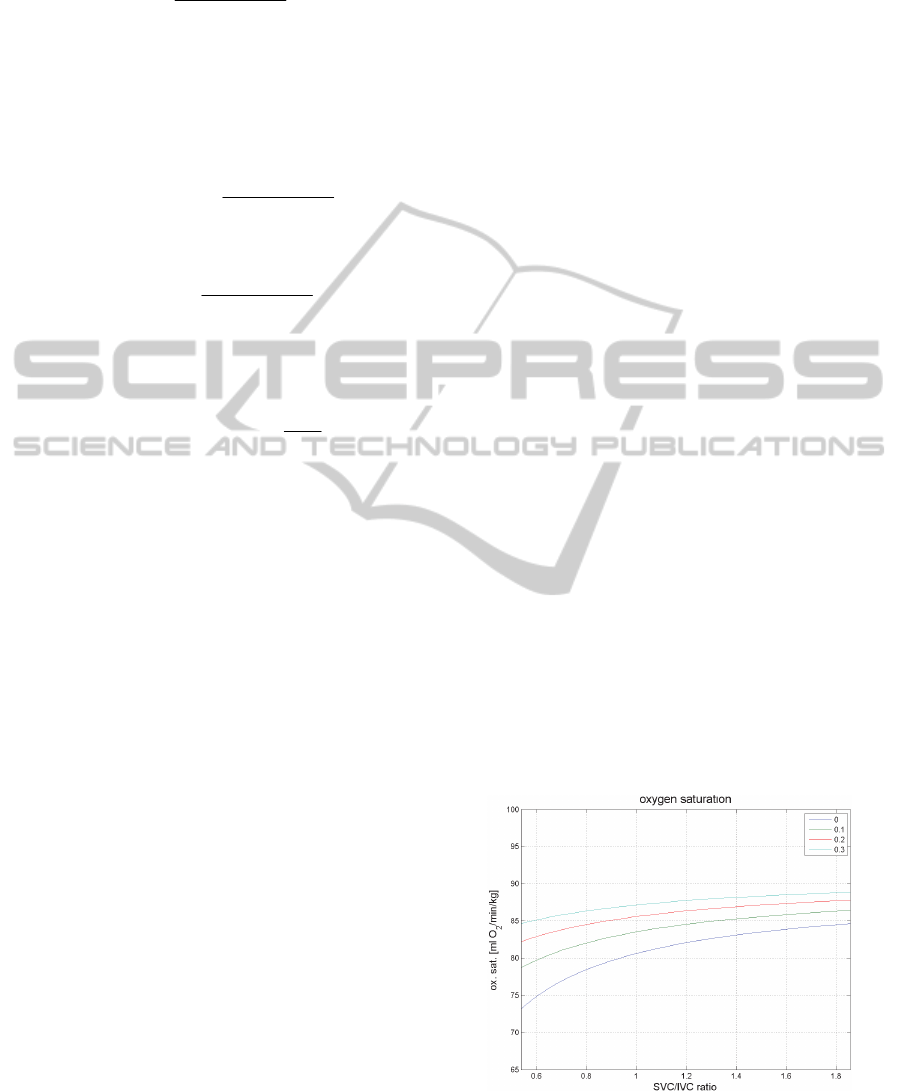
In particular, Fig. 2 reports the global blood
oxygen saturation level, which increases with
IVCSVC
QQ / , for every value of the shunt parameter
. This is expected, since higher SVC flows entail
a higher pulmonary perfusion, as per Eq. 4. It is
evident that increasing
, at a given value of the
ratio
IVCSVC
QQ / , improves the blood oxygen
saturation level, especially at the lower
IVCSVC
QQ /
values. Such values can be considered relevant
especially for exercise conditions, when the lower
body requires a higher oxygen increase than the
upper body.
Also for the regional blood oxygen saturation
level the presence of additional blood flow is
beneficial. Fig. 3 shows how the IVC oxygen
saturation varies as a function of Q
IVC
/Q
SVC
and
;
similarly for the SVC oxygen saturation in Fig. 4. A
marked improvement is observed, especially for the
minimum physiological value of Q
IVC
/Q
SVC
in Fig.
3, allowing the oxygen saturation in the lower
circulation to reach over 70% (for
=0.3), from 60%
in absence of additional pulmonary flow.
A lesser effect, albeit clearly positive, is given by
the presence of the shunt in the oxygen saturation in
the upper circulation (Fig. 4).
It should be considered that, in the study, the
flow through the shunt was not calculated in the total
CO, which was instead calculated as the sum of the
caval flows, Q
IVC
+ Q
SVC
. Thus, for increasing values
of
the work exerted by the heart is higher, at the
same CO level, since it must provide also the flow in
the shunt. This should be clearly considered together
with the advantages in terms of blood oxygenation,
during surgery planning.
Figure 2: Oxygen saturation vs. SVC/IVC ratio, as a
function of the parameter
which characterizes the
systemic-to-pulmonary shunt.
BIOSIGNALS2013-InternationalConferenceonBio-inspiredSystemsandSignalProcessing
394
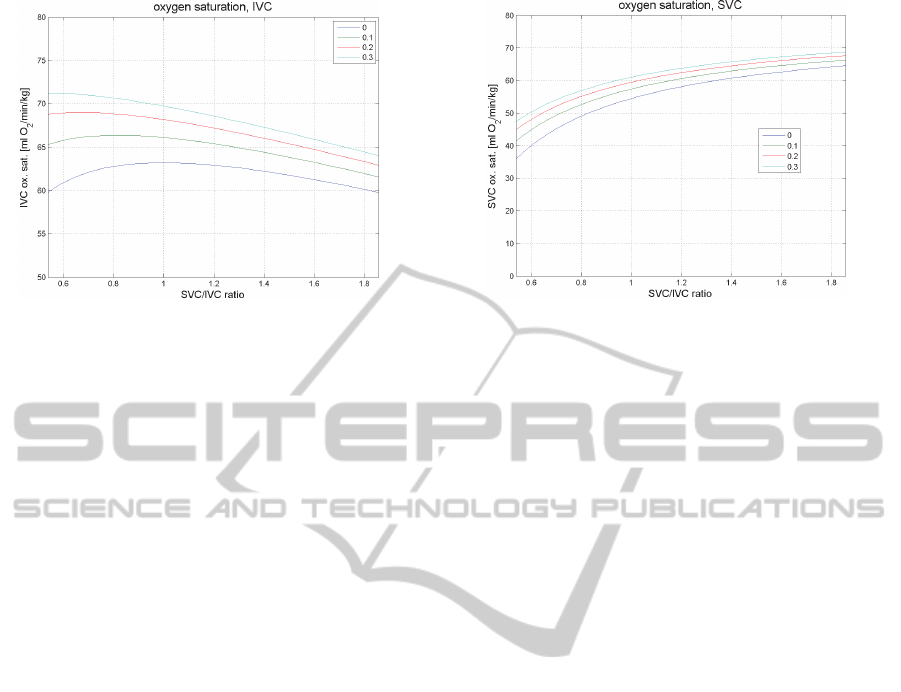
Figure 3: IVC oxygen saturation vs. SVC/IVC ratio.
In the model, we did not take explicitly into
account the contribution of the lungs’ vascular bed
to the observed effects. Actually such a role impacts
on the pulmonary resistance, and therefore on
P
Q ,
so that it is implicitly considered. Nevertheless, a
more accurate description of the pulmonary
circulation could improve the predictive capabilities
of the model, given the importance of lung
physiology and development in univentricular
patients.
4 CONCLUSIONS
The mathematical modelling of the circulation after
BCPA and an additional source of pulmonary blood
flow, such as the modified Blalock-Taussig shunt,
demonstrated clear advantages of this surgical
option, with respect to the simple BCPA, in terms of
systemic blood oxygen saturation, especially in the
lower circulation. The results are substantially in
accordance with recent reports (van Slooten et al.,
2012) of a retrospective study with a remarkable
sample size (82 patients), which confirmed the
advantage of additional pulmonary blood flow in
BCPA patients.
In the future, we intend to apply this
mathematical model, with the necessary
modifications, to optimize the management of the
pediatric patients with a single functional ventricle,
from birth to the final surgical stage, the TCPC, i.e.,
total cavopulmonary connection (Giannico et al.,
2006). We look forward to evaluating the predictive
capabilities of this model by comparing the results
with actual clinical data: this step will indicate
whether further refinements of the model are
necessary.
Figure 4: SVC oxygen saturation vs. SVC/IVC ratio.
REFERENCES
Caspi J., Pettitt T. W., Ferguson T. B. Jr., Stopa A. R.,
Sandhu S. K., 2003. Ann Thorac Surg. 76(6):1917-21.
Giannico S., Hammad F., Amodeo A., Michielon G.,
Drago F., Turchetta A., Di Donato R., Sanders S. P.,
(2006). Clinical outcome of 193 extracardiac Fontan
patients: the first 15 years. J Am Coll Cardiol.
47(10):2065-73.
Goldberg C. S., Gomez C. A., 2003. Semin Neonatol.
8(6):461-8.
Salim, M. A., Case C. L., Sade R. M., Watson D. C.,
Alpert B. S., and DiSessa T. G., 1995.
Pulmonary/systemic flow ratio in children after
cavopulmonary anastomosis. J. Am. Coll. Cardiol. 25:
735–738.
Santamore W. P., Barnea O., Riordan C. J., Ross M. P.,
Austin E. H., 1998. Theoretical optimization of
pulmonary-to-systemic flow ratio after a bidirectional
cavopulmonary anastomosis. Am J Physiol. 274(2 Pt
2):H694-700.
van Slooten Y. J., Elzenga N. J., Waterbolk T. W., van
Melle J. P., Berger R. M. F., Ebels T., 2012, The
Effect of Additional Pulmonary Blood Flow on
Timing of the Total Cavopulmonary Connection, Ann
Thorac Surg., 93(6):2028-2033.
AdditionalPulmonaryBloodFlowintheCavopulmonaryAnastomosisbyMeansofaModifiedBlalock-TaussigShunt-Is
ItaBeneficialClinicalOption?
395
