
Log Analysis of Human Computer Interactions Regarding
Break The Glass Accesses to Genetic Reports
Ana Ferreira
1,2
, Pedro Farinha
2
, Cátia Santos-Pereira
2
, Ricardo Correia
2
, Pedro P. Rodrigues
2
,
Altamiro Costa-Pereira
2
and Verónica Orvalho
3
1
SnT, University of Luxembourg, Campus Kirchberg, Luxembourg
2
CINTESIS, Faculty of Medicine, University of Porto, Porto, Portugal
3
IT, Faculty of Science, University of Porto, Porto, Portugal
Keywords: Security Usability, Human Interaction Log Analysis, Electronic Health Records, Access Control Override.
Abstract: Patients’ privacy is critical in healthcare but users of Electronic Health Records (EHR) frequently
circumvent existing security rules to perform their daily work. Users are so-called the weakest link in
security but they are, many times, part of the solution when they are involved in systems’ design. In the
healthcare domain, the focus is to treat patients (many times with scarce technological, time and human
resources) and not to secure their information. Therefore, security must not interfere with this process but be
present, nevertheless. Security usability issues must also be met with interdisciplinary knowledge from
human-computer-interaction, social sciences and psychology. The main goal of this paper is to raise security
and usability awareness with the analysis of users’ interaction logs of a BreakTheGlass (BTG) feature. This
feature is used to restrict access to patient reports to a group of healthcare professionals within an EHR but
also permit access control override in emergency and/or unexpected situations. The analysis of BTG user
interaction logs allows, in a short time span and transparently to the user, revealing security and usability
problems. This log analysis permits a better choice of methodologies to further apply in the investigation
and resolution of the encountered problems.
1 INTRODUCTION
Theoretically, a computer can be made secure if the
three main security characteristics (e.g.
confidentiality, integrity and availability) can be
guaranteed. However, a crucial factor can bring a lot
of entropy to this secure world: humans (Schneier,
2000). Yet, technology that is theoretically secure
and not usable does little to improve information
security because it pushes users away to less secure
platforms. This is very common in healthcare where
users of Electronic Health Records (EHR) frequently
circumvent existing access control rules to perform
their work (Lehoux, 1999), (Cranor, 2005).
In the healthcare domain, the focus is to treat
patients (many times with scarce technological, time
and human resources) and not to secure their
information. Therefore, security must not interfere
with this process but be present, nevertheless.
Ideally, users should be part of the solution and
become more involved in the design of secure and
usable systems (Ferreira, 2010). In fact, this design
can many times raise issues that cannot be met with
existing human computer interaction (HCI)
knowledge and methods (Kainda, 2010), but must
integrate interdisciplinary knowledge such as from
socio-technical systems research, safety critical
systems design and social psychology (Whitten,
1999); (Sasse, 2003).
According to healthcare legislation, both the
North American Health Insurance Portability and
Accountability Act (HIPAA) (Break Glass, 2012)
and the United Kingdom National Health Service
(NHS) documentation (NHS, 2012) specify the need
for Break-The-Glass (BTG) or overriding situations
(break the seal) as described in (Break Glass, 2004).
BTG is required when static access controls are
insufficient and there is the need to override those
controls in emergency and/or unexpected situations.
BTG permits the use of a more flexible and dynamic
access control policy, which can be adapted to the
users’ needs at the point of care.
In terms of BTG auditing, an email alert (or
another type of alert such an SMS or a phone call)
46
Ferreira A., Farinha P., Santos-Pereira C., Correia R., P. Rodrigues P., Costa-Pereira A. and Orvalho V..
Log Analysis of Human Computer Interactions Regarding Break The Glass Accesses to Genetic Reports.
DOI: 10.5220/0004419200460053
In Proceedings of the 15th International Conference on Enterprise Information Systems (ICEIS-2013), pages 46-53
ISBN: 978-989-8565-61-7
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

can be sent to a responsible party when the glass is
broken (e.g. when a user overrides access control
permissions) and this party or another entity can
further investigate whether this access was justified
(Ferreira, 2006).
The BTG users’ interaction logs can provide
regular monitoring and auditing functions (which are
rarely used unless a serious breach needs
investigation) but can also gather a rich amount of
information concerning both security and usability
behaviours (Iglesias, 2012).
The main goal of this paper is to raise security
usability awareness by identifying some security
and/or usability problems regarding human-
computer interaction behaviour, with the analysis of
users’ interaction logs of a BTG feature in
healthcare. The identified problems can then be
further explored and mitigated with the most
appropriate methodologies.
This paper is organised as follows: the next
section presents background information; Section 3
describes the use-case scenario where this research
has been applied, together with the methods used for
log acquisition and analysis; Section 4 presents the
obtained results while Section 5 discusses and
analyses those results; Section 6 presents some
future work and Section 7 concludes the paper.
2 BACKGROUND
2.1 Security Usability
An information system is usable when its users can
perform the tasks they need in a fast and easy
manner and routinely/automatically apply correct
protection mechanisms (Saltzer, 1975). This points
out that: (1) usability focuses on users; (2) people
use products to be productive; (3) users are busy
people trying to accomplish tasks; and (4) users
decide when a product is easy to use (Redish, 1999).
With this in mind, there seems to be an implicit
assumption that technologies that are widely used
are, by definition, usable. However, examples such
as passwords and email security show that
technologies that worked well enough when
introduced can evolve into usability disasters with
extended use (Sasse, 2003).
Different approaches need to be applied
regarding not only, authentication mechanisms
(Kuo, 2006); (Brostoff, 2000) email encryption
(Whitten, 1999), access control (Ferreira, 2011a),
security tools and privacy (ZIshuang, 2005), but also
issues that are aimed at achieving users’ goals,
which may not be directly related with security, but
have an element of security in them (Cranor, 2005).
Security usability’s main goal is then to improve
the usability of information system’s security
features or even other features not directly related
with security. In the later scenario, this must be done
without compromising system’s security.
2.2 Log Analysis
Non-repudiation is also a very important security
goal (Harris, 2012) and so auditability measures are
commonly put into place usually for when
something goes wrong and a thorough investigation
is needed. Most of the times, the only way to do this
is to recur to the registration of all activities
performed within a system. This log of activities
includes all accesses and interactions that programs,
processes, and most importantly, users have with
that system.
So besides its most common usages, logs can
integrate a wide and rich set of interaction data
whose analysis can be used for other purposes rather
than auditing. Users’ interaction logs can help
improving data quality and integrity by allowing, for
instance, the detection of healthcare information
errors and inconsistencies (Cruz-Correia, 2011).
Although logs may need pre-processing to allow a
useful analysis they can be very valuable to study
user modelling, improve activity analysis,
monitoring and security (Xhafa, 2012). There are
also cases where logs can be used to provide a better
knowledge of users’ behaviour with the main goal to
assist them in performing their tasks (Iglesias, 2012),
(Shun-Hua, 2010), as well as identify usability
problems (Palanque, 2011).
3 USE-CASE & METHODS
3.1 Legislation Compliance
Many healthcare institutions developed their
healthcare processes and subsequent healthcare
information systems. Legislation is usually generic
and abstract enough to allow this type of diversity.
However, this also allows for systems’ heterogeneity
and, commonly, difficult communication and
integration (Cruz-Correia, 2007).
On the other hand, there is also specific
legislation available which focus on special parts of
healthcare data protection that needs compliance.
This is the case of the Portuguese law for genetic
healthcare related information that defines how
LogAnalysisofHumanComputerInteractionsRegardingBreakTheGlassAccessestoGeneticReports
47

genetic information must be protected and how and
what healthcare professionals are authorized to
access it during the course of their work
(Assembleia, 2005). The law states that only a pre-
defined group of healthcare professionals, whose
speciality is directly related with genetics’ study and
treatment, can access data containing this type of
information. Section 3.2 describes how this law was
enforced using the BTG feature.
3.2 Healthcare Scenario
In May 2003, the Department of Biostatistics and
Medical Informatics (currently CIDES -
Departamento de Ciências da Informação e da
Decisão em Saúde) at Porto Faculty of Medicine
implemented a Virtual Electronic Patient Record
(VEPR) (Cruz-Correia, 2005) at the São João
Hospital Center, which is the second biggest hospital
in Portugal, where more than 5300 patients are
attended every day. This VEPR is a subset of an
EHR and integrates clinical reports from 14 hospital
departments, Diagnosis Related Groups and hospital
administrative databases. Around 452 healthcare
professionals access the system on a daily basis
(there is a total of 2300 active users) and visualize
1525 reports in 1674 daily sessions (there are more
than 9.000.000 stored patient reports but usually
around 3.000.000 are available for access).
The authentication mechanisms used for this
VEPR are login and password and the authorisation
platform is based on the RBAC (Role-Based Access
Control) standard (Ferraiolo, 2001). Once the user
authenticates successfully to the system his/her
access control profile is selected and activated in a
transparent way. This profile includes permissions
and resources that can be accessed by that user and
associated role(s). A web based platform (webcare)
was developed to administer the access control
policy for all VEPR users (Farinha, 2010).
The described VEPR integrates reports which
contain patients’ genetic information. In order to
comply with the legislation described in Section 3.1,
only a predefined group of healthcare professionals
has direct access to this type of patient reports. The
Hospital’s Ethical Commission and the board of
directors have defined the group of authorised users.
However, if needed, other healthcare professionals
can access these reports if they perform BTG by
overriding the stated access control policy and abide
to its subsequent conditions and/or consequences.
BTG was implemented to control policy override
and block immediate access to the reports that
contain genetic information to unauthorised users.
When the users try to access a genetic report and do
not belong to the authorization group, a popup
window appears, alerting them of the BTG
procedure, the legislation it enforces and possible
consequences.
The user needs to decide if the reason to perform
BTG is strong enough to still perform this access.
He/she is obliged to select a reason to execute BTG.
Two of the reasons are fixed and are: [reason R1 - “I
belong or should belong to the authorised group”]
and [reason R2 - “I have urgency to see this report
even though I have no permission, at this moment, to
do it”]. A third option is also available where the
users can [reason R3 - write his/her own
reason/justification].
3.3 Log Acquisition and Analysis
For the presented VEPR (Section 3.2) users’ log
interactions are registered within a separate instance
of a relational database system solely for this
purpose. All records are stored in a structured
manner in database tables where is easier and faster
to search and retrieve them.
Users’ interaction logs have been collected since
November 2004 but the data analyzed within this
paper were collected from November 2007 until
December 2012. Genetic reports started to be
identified on collection in November 2007 so data
are presented according to these figures. May 2009
was the date when the BTG feature started to be
used. The log analysis focused on the comparison of
the period before and after using BTG features and
verifies if these specific access control mechanisms
can reveal how users interact and/or change behavior
over long periods of time. As a means to easily and
quickly reveal usability and security problems, the
analysis presented in this study is mainly about
summarizing the main user interaction behaviour. So
analysis is made regarding data frequencies from
search queries applied directly to the audit log
database. It is possible to make deeper analysis using
several data mining tools (Iglesias, 2012) to find
more complex behavioural patterns but this is not
the main purpose of this research.
The search queries that were applied to the audit
database for this study included: (1) the total number
of identified genetic reports; (2) the total number of
accesses to genetic reports by all users (authorised
and unauthorised) before and after BTG
implementation; (3) how many users performed
BTG and how many gave up once warned about its
consequences; (4) the reasons chosen to perform
BTG and the most common inserted reason R3; (5)
ICEIS2013-15thInternationalConferenceonEnterpriseInformationSystems
48
if there was any suspicious individual behaviour
amongst the users who most perform BTG and also
give up doing it; (6) and if there was a specific time
of the year where usage patterns were very different
from other periods of time.
Results are presented in Section 4 and their
subsequent discussion is introduced in Section 5.
4 RESULTS
Before the implementation of the
BTG feature (November 2007 – April 2009), 2875
genetic reports were stored within the database. A
total of 7774 genetic reports were available
afterwards (May 2009 - December 2012).
Table 1 compares the accesses to genetic reports
from authorised and unauthorised users, before and
after the BTG implementation. Before BTG, all
accesses (n=842) by unauthorised users to genetic
reports were successful. After the BTG
implementation and from the unauthorised users’
attempts (n=5608), 3071 (55%) BTG accesses were
successful while 2537 (45%) were unsuccessful as
users gave up performing BTG after being warned
(waivers). From these waivers, 2366 (93%) closed
the browser while 171 (7%) preferred to select the “I
don’t want to see this report” button.
Table 1: Frequencies (percentages) of attempts (total of
7176) to access genetic reports from authorized (n=726)
and unauthorised users (n=6450), before and after the
Break The Glass (BTG) implementation and use.
AttemptsbeforeBTG
(Nov2007–Apr2009)
(n=1001)
AttemptsafterBTG
(May2009‐Dec2012)
(n=6175)
successful
accesses
n(%)
successfu
laccesses
n(%)
unsuccessful
accesses
n(%)
Authorised
users
159(16) 567(9) 0(0)
Unauthorise
dusers
842(84)
3071
(50)
2537*
(41)
* From the 2537 unsuccessful accesses, which correspond to 45%
of the total of 5608 access attempts from unauthorised users after
BTG use, 171 (7%) of these users pressed the button “I don’t
want to see this report” while 2366 (93%) closed the browser.
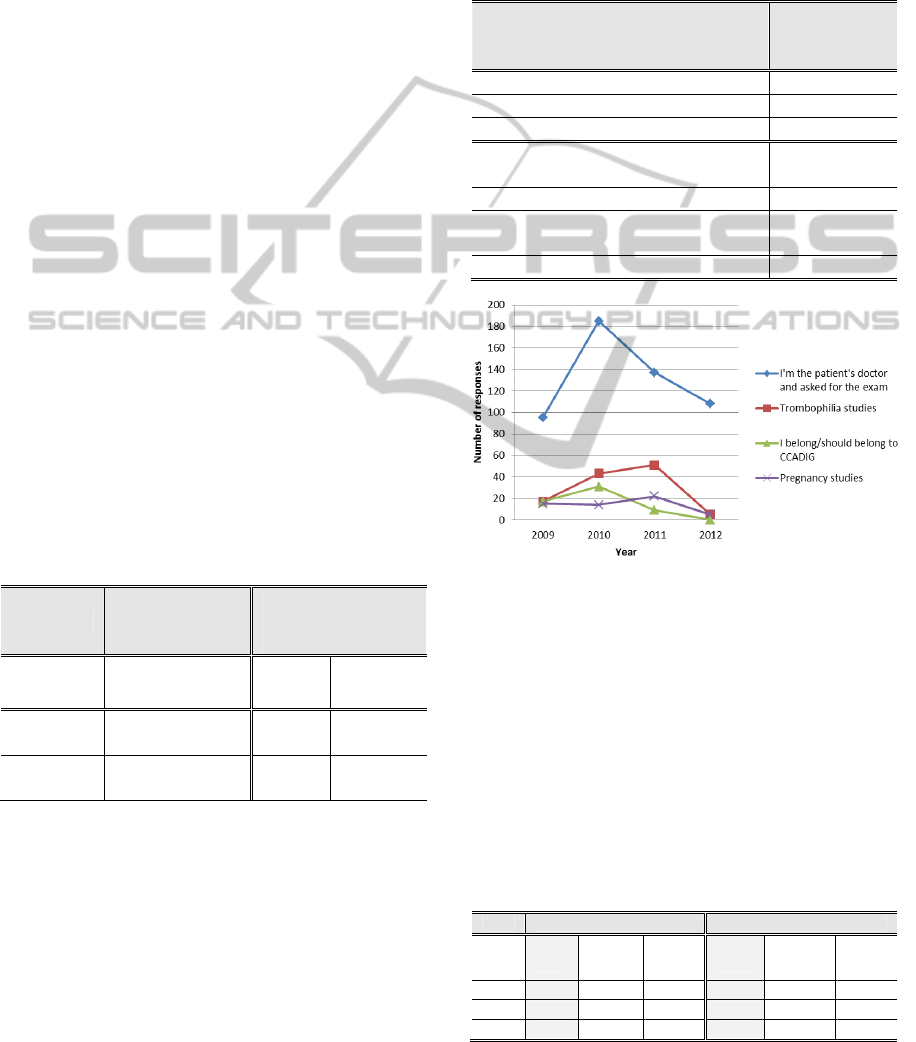
For the three reasons that could be selected by
the users who performed a BTG access, Table 2
presents the total number of selections that were
made, together with the four most common reasons
that the users inserted before “breaking the glass”.
Figure 1 presents the yearly distribution of these
four reasons.
Moreover, there were also 6 empty answers (the
users are obliged to insert a reason) and one user that
refers that the system is wrong.
Table 2: Frequencies (percentages) of pre-selected (R1
and R2) and stated reasons (R3a to R3d) chosen
by unauthorised users who performed BTG within their
3071 accesses to genetic reports.
Typeofpre‐selectedorstatedreasons
Totalnumber
ofselections
n(%)
R1–Ibelongtotheauthorisedgroup
834
(27)
R2–Ihaveurgencytoseethisreport
1229
(40)
R3–Iwriteanotherjustification:
1008
(33)
R3a‐“I’mthepatient’sdoctorand
requestedtheexam”
525
(52)
R3b‐“Thrombophiliastudies”
116
(12)
R3c‐“Ibelongtotheauthorised
group”
57
(6)
R3d‐“Pregnancy/infertilitystudies”
56
(6)
Figure 1: Four most common reasons introduced by the
users to justify their BTG accesses (yearly distribution).
Focusing now on individual accesses, the top
three BTG users were identified. Table 3 compares
the total of BTG accesses and waivers to patient
genetic reports regarding these three users. This
comparison is performed between two moments in
time: 2009-2010 and 2011-2012.
Table 3: Frequencies (percentages) of BTG accesses
and waivers (unsuccessful accesses) regarding the total
number of attempts to access genetic reports by the three
unauthorised users who mostly performed BTG (u_A,
u_B, u_C), in two consecutive periods.
During2009and2010 During2011and2012
Total
n
BTG
accesses
n(%)
Waivers
n(%)
Total
n
BTG
accesses
n(%)
Waivers
n(%)
u_A 81 47(58) 34(42) 155 90(58) 65(42)
u_B 134 67(50) 67(50) 125 64(51) 61(49)
u_C 95 73(77) 22(23) 72 53(74) 19(26)
LogAnalysisofHumanComputerInteractionsRegardingBreakTheGlassAccessestoGeneticReports
49
Table 4 presents in more detail the number and
types of reasons selected by the three users that
performed most BTG accesses.
Table 4: Number and types of reasons selected by the
three unauthorised users who most performed BTG (u_A,
u_B, u_C).
During2009and2010 During2011and2012
R1 R2 R3 R1 R2 R3
u_A 1 45 1 0 89 1
u_B 67 0 0 64 0 0
u_C 1 0 72 1 0 52
Users u_A and u_B hardly selected reason R3 to
justify their BTG accesses. User u_A mainly selects
reason R2 and chooses reason R3 to justify only two
accesses (i.e., 1 trombophilia study and 1 I asked the
patient’s exam). This user also mistakenly inserts
reason R2 together with reason R3 at one time, and
again gives “thrombophilia study” as the
justification. User u_B only selects reason R1. User
u_C mainly selects reason R3 to justify the BTG
accesses and writes “I asked the patient’s exam” 124
times in total. This user also mistakenly inserts two
times the reason R1 with that same justification in
reason R3.
5 DISCUSSION
This section discusses the results presented in
Section 4 and gives some recommendations on what
security and usability issues need further
investigation, and what are the most appropriate
methodologies to better understand and resolve
those issues.
Regarding Table 1, before implementing the
BTG features, 84% of all accesses were
unauthorised, but successful accesses.
After BTG implementation, from all the access
attempts and with 3 times more patient genetic
reports available, 55% of those attempts from
unauthorised users were successful and used BTG,
with the most varied reasons presented in Table 2.
Still, in total, 45% of unauthorised accesses (that
would not normally be detected) were prevented,
after BTG implementation. However, 91% of all
access attempts were made from unauthorized users,
so only 1 in every 9 attempts is made from
authorised users.
During the course of 4 years there has been an
increase of almost 200% of access attempts. Before
BTG features there were around 55 access attempts
per month (in this case all successful) while after
BTG features this number increased to 144 access
attempts per month (71 from unauthorised users).
Further investigation with qualitative studies such as
focus groups is needed to make sure daily processes
match the users’ daily needs regarding data access.
Why the number of unauthorised access attempts has
increased so much? Do unauthorised users need to
access genetic reports this often? If so, why? (the
legislation may not match real healthcare processes).
If not, better monitoring and feedback needs to be
made to avoid most unauthorised accesses.
Also important to note from Table 1 is the fact
that, in percentage, accesses from the authorised
group were reduced to half. Does this mean that
users belonging to the authorised group need to be
re-checked? Maybe some users have already left the
hospital and some unauthorised users should belong
to the authorised group instead. Either way, the
access control policy to genetic reports needs to be
reviewed and updated. In order to do this, the
responsible parties and board of direction, as well as
the Hospital Ethical Committee need to be
consulted.
Finally, from users who give up performing BTG
and are warned of the consequences, only 7% select
the provided button. The other 93% simply closed
the window. Further investigation needs to be done
to find out why users do not select the “I don’t want
to see this report” button. Do they think is a mistake
and close the window to restart the browser? More
specific individual user log analysis can be done to
exploit this question (Table 3 gives evidence that
some users can do that). If users do not need to see
the requested genetic report, do they think that just
by closing the window their access attempt is not
registered as if it would be by actively pressing a
button? Again, focus groups can be performed to
better understanding the later question.
Analysing now the results regarding the three
reasons that users choose to perform BTG (Table 2),
the most selected reason is the one that states that
they have urgency to see the report (40
%). This in itself does not say much. There can be
many different types of urgencies and some more
“urgent” than others. The text which appears on the
BTG warning interface may need revision and the
reasons to perform BTG need to be clarified.
Further, open interviews can be applied to the users
to better understand what types and degrees of
urgencies can commonly appear. Maybe one
suggestion could be to have only one reason where
users could introduce their justification and no other
options as, for example, even with a fixed option
reason R1 – “I belong or should belong to the
ICEIS2013-15thInternationalConferenceonEnterpriseInformationSystems
50

authorised group” available (with 27% of
selections), users still use reason R3 to state that
they belong to the authorised group (6%).
For the previous suggestion, there are also some
issues to be further explored. The most common
BTG justification inserted by the users include the
fact that they are the healthcare professionals
treating the patient and asked for that exam (52%)
or that they requested it in order to perform studies
relating to specific medical specialities (i.e.,
thrombophilia and pregnancy studies) (18%).
All these issues can be related to how the access
control policy is defined. Firstly, there is not yet the
possibility for the patient to define or control what
healthcare professionals can/should access which
parts of his/her medical record, as stated within the
European legislation. This is an issue outside the
scope of this research but which needs to be urgently
addressed in a near future as also interferes with
healthcare access control policy definition (Santos-
Pereira, 2012). Secondly, focus groups need to be
performed with the users to find out if the most
common inserted reasons are/can be justified. If they
are, the access control policy needs to be reviewed
and updated by the responsible parties.
Within the mentioned focus group study, another
issue must be raised. Why have the reasons inserted
decreased so much during 2012? In this year, the
BTG accesses by users that selected reason R3 have
decreased almost 60% when compared with the two
previous years. Are users performing BTG only
when they really need now? Do they select mainly
the other two fixed reasons? Or have they access to
this type of information from other means (i.e., other
applications, paper documents), bypassing this way
BTG features so that their accesses are not so closely
monitored and registered? Has the background
justification process become more active or
effective? Is there any technical problem with the
BTG features? Are they working as expected? To
help answering these questions, qualitative
observation and focus group studies should be
performed with the users, as well as meeting with
responsible parties to analyse the BTG background
justification (is it being done? How? When? By
Whom?). Quantitative users’ interaction log
analysis, together with testing and validating the
technical aspects of the interface, must also be
performed.
One more issue that can be directly related with
the interface and technical implementation is the fact
that there were at least two situations detected where
a user was able to perform BTG without having to
insert a reason to justify it. Maybe the user just filled
the space provided with space characters, if this is
allowed. It should be compulsory to select or insert a
non-empty reason to perform BTG. Technical
measures need to be corrected so that empty answers
are avoided.
Focusing now on the analysis of BTG accesses
from individual users (Table 3), further investigation
is required to understand why these users need to
perform BTG more often than the others. In more
detail, user u_A has increased by almost 100% his
BTG accesses and attempts in the last two years
(2011 and 2012). The other two users (u_B, u_C)
have slightly decreased their BTG accesses but still
remain high. Further research needs to be made to
confirm if these users are just maliciously or
negligently accessing the genetic reports or if they
should be part of the authorised group and access
control policy needs, once more, reviewing and
updating.
Individual users’ interaction logs seem to reflect
what was also identified by the generic analysis of
those same logs. It is also possible to identify in
Table 3 that the users who most perform BTG also
give up doing it a very high number of times. So
maybe the issue of trying several times before
actually succeeding when they see there is no other
option but to press the “I want to see this report”
button, may be happening. Observation studies and
more detailed analysis of interaction logs can be
performed to confirm this.
Finally, regarding Table 4 results, the most
common reasons to perform BTG which were
inserted mostly by user u_A are in tune with the
ones presented in Table 2. Also, the three identified
users tend to choose the same reason every time they
try to access a genetic report. Their behaviour
regarding BTG does not change over 4 years of use.
However, separately, they choose very different
reasons to justify BTG accesses. Furthermore, these
users choose a few times both a fixed reason (R1 or
R2) with reason R3
to describe a BTG access. This
must be corrected in the interface. Users must only
be able to select one reason at a time.
In summary, and as a preliminary analysis of the
obtained results, several technical, usability, security
and even social issues were raised for further
investigation. In order to fasten this investigation,
each study to be performed should include the
biggest number of issues to study. For example, if
focus groups are employed, all the issues raised here
that require this type of method can be explored at
the same time. Is it also important to state that these
studies should not be used to control or survey users’
actions to further punish them. The main goal is to
LogAnalysisofHumanComputerInteractionsRegardingBreakTheGlassAccessestoGeneticReports
51

improve BTG’s HCI, security, usability and its
usefulness, and allow users to perform their daily
tasks in a safe/efficient manner.
However, a very important question remains:
why were some users accessing genetic reports
before BTG implementation, if they did not access
those reports so often once BTG features were
available? It may not be easy to find out why this
was happening with the proposed research methods
but maybe by correcting some of the other problems
raised in the discussion, this type of unauthorised
accesses can be avoided in the future.
6 FUTURE WORK
Future work includes further investigation of the
previously identified security usability issues, but
also the analysis of other issues that arose during this
research, including if there are (recommendations on
what type of studies could be used to further explore
these issues are in square brackets): (a) accesses
made simultaneously by the same login at different
locations with different sessions [quantitative log
analysis]; (b) many waiting sessions or automatic
session locks [quantitative log analysis]; (c) any
suspicious behavior relating with the number of
times a user authenticates daily [quantitative log
analysis & qualitative observations]; (d) any
suspicious behavior relating with how many times a
computer is used and for how many different people
on a daily basis [qualitative observations &
interviews]; (e) any common authentication errors,
mostly login or password problems [quantitative log
analysis & qualitative interviews].
Other usability issues that also be analysed
include if: (a) there could be any suspicious behavior
relating with password sharing [quantitative log
analysis] (Ferreira, 2011b); (b) there are any
common paths to search for information inside the
system [quantitative log analysis & qualitative
observations]; (c) there are many backward flows
within the searches performed by the users
[quantitative log analysis].
7 CONCLUSIONS
Users’ interaction logs can be a helpful tool to
studying user-system interaction but other
exploratory studies are needed to focus on user-user
interaction, in which context the user is interacting
with the system and which characteristics and
individual knowledge the user has and uses to
perform those interactions (Xhafa, 2012).
This paper presented an analysis of users’
interaction logs in order to study HCI security and
usability issues. Logs generate a great amount of
data that can be useful as to unveil both those issues.
Users’ interaction log analysis can be used not only
in healthcare to analyse users’ behaviour regarding
BTG accesses but also in other scenarios where
confidentiality is very important (i.e., home banking,
online shopping, etc). However, logs are not enough
to change unsecure, erroneous or even malicious
users’ behaviour. Other methods and techniques
need to be used to further explore how this
can/should be done.
Finally, as much as users’ interaction logs can be
a promising tool to be used to study and improve
HCI and security usability problems, bad quality
logs (many times they do not even exist), will
certainly not be helpful in pursuing these tasks and
so it is recommended that logs should be taken more
seriously and be adequately and securely
implemented and maintained.
ACKNOWLEDGEMENTS
This work was supported by the Portuguese FCT,
through the research project “Optimizing
Information Systems for healthcare: improving
Graphical User Interface and Storage Management
through Machine Learning techniques on user logs
data” [PTDC/EIA-EIA/099920/2008].
REFERENCES
Assembleia da República, 2005. Lei n. 12/2005 de 26 de
Janeiro. DIÁRIO DA REPÚBLICA — I SÉRIE-A.
Break-glass, 2004. An approach to granting emergency
access to healthcare systems. White paper, Joint –
NEMA/COCIR/JIRA Security and Privacy Committee
(SPC).
Break Glass, 2012. Granting Emergency Access to
Critical ePHI Systems – HIPAA Security. Accessed at:
http://hipaa.yale.edu/security/breakglass.html.
Accessed on the 13th December 2012.
Brostoff, S., Sasse, A., 2000. Are passfaces more usable
than password? A field trial investigation. People and
Computers XIV-Usability of else. Proceedings of HCI
2000. S. McDonald Springer, 405-424.
Cranor & Garfinkel, 2005. Security and usability:
designing secure systems that people can use.
O’Reilly.
Cruz-Correia, R., Lapão, L., Rodrigues, P., 2011.
ICEIS2013-15thInternationalConferenceonEnterpriseInformationSystems
52

Traceability of patient records usage: barriers and
opportunities for improving user interface design and
data management. Studies in Health Technologies and
Informatics, vol. 169, pp. 275-279.
Cruz-Correia, R., Vieira-Marques, P., Costa, P., Ferreira,
A., Oliveira-Palhares, E., Araújo, F., Costa-Pereira,
A., 2005. Integration of Hospital data using Agent
Technologies – a case study. AICommunications
special issue of ECAI, 18(3):191-200.
Cruz-Correia, R., Vieira-Marques, P., Ferreira, A.,
Almeida, F., Wyatt, J., Costa-Pereira, A., 2007.
Reviewing the integration of patient data: how systems
are evolving in practice to meet patient needs. BMC
Medical Informatics and Decision Making, 7(14).
Farinha, P., Cruz-Correia, R., Antunes, L., Almeida, F.,
Ferreira, A., 2010. From legislation to practice: a case
study of break the glass in healthcare. Proceedings of
the International Conference on Health Informatics,
114-120.
Ferraiolo, D., Sandhu, R., Gavrila, S., Kuhn, R.,
Chandramouli, R., 2001. Proposed NIST Standard for
Role-based Access Control. ACM Transactions on
Information and systems security, 4(3): 224-274.
Ferreira, A., Antunes, L., Chadwick, D., Cruz-Correia, R.,
2010. Grounding Information Security in Healthcare.
International Journal of Medical Informatics, 79(4):
268-283.
Ferreira, A., Correia-Cruz, R., Antunes, L., 2011a.
Usability of authentication and access control: a case
study in healthcare. IEEE International Carnahan
Conference on Security Technology, 1-7.
Ferreira, A., Cruz-Correia, R., Chadwick, D., Santos, H.,
Gomes, R., Reis, D., Antunes, L., 2011b. Password
sharing and how to reduce it. Certification and
Security in Health-Related Web Applications:
Concepts and Solutions, 243-263.
Ferreira, A., Cruz-Correia, R., Antunes, L., Farinha, P.,
Oliveira-Palhares, E., Chadwick, D. W., Costa-Pereira,
A., 2006. How to break access control in a controlled
manner? Proceedings of the 19th IEEE Symposium on
Computer-Based Medical Systems, 847-851.
Harris, S., 2012. CISSP All-in-one Exam Guide. McGraw-
Hill Osborne Media. 6
th
Edition.
Iglesias, J., Angelov, P., Ledezma, A., Sanchis, A., 2012.
Creating evolving user behavior profiles
automatically. IEEE Trasactions on Knowledge and
data engineering, 24(5): 854-867.
Kainda, R., Flechais, I., Roscoe, A.W., 2010. Security and
usability: analysis and evaluation. International
conference on Availability, Reliability and Security,
275 – 282.
Kuo, C., Romanosky, S., Cranor, L., 2006. Human
Selection of Mnemonic Phrase-Based Passwords.
Symposium on usable privacy and security (SOUPS),
67-78.
Lehoux, P., Sicotte, C., Denis, J., 1999. Assessment of a
computerized medical record system: disclosing
scripts of use. Evaluation and Program Planning, 22(
4): 439-53.
NHS care records service, 2012. NHS Connecting for
Health. Sealing Overview. Accessed at:
http://www.connectingforhealth.nhs.uk/elearning/scr/s
cr2008b/modules/scr07_sealing/t1/scr07t1p1.htm.
Accessed on the 13th December 2012.
Palanque, P., Barboni, E., Martinie, C., Navare, D.,
Winckler, M., 2011. Proceedings of the 3rd ACM
SIGCHI symposium on Engineering interactive
computing systems, 21-30.
Redish, J., Dumas, J., 1999. A Practical Guide to Usability
Testing. Intellect Ltd.
Saltzer, J., Schroeder, M., 1975. The protection of
Information in Computer Systems. Proceedings of the
IEEE, 63(9): 1278-1308.
Santos-Pereira, Cátia., Augusto, Alexandre., Correia,
Manuel., Ferreira, Ana., Cruz-Correia, Ricardo., 2012.
A Mobile Based Authorization Mechanism for Patient
Managed Role Based Access Control. Information
Technology in Bio and Medical Informatics. Lecture
Notes in Computer Science, 7451: 54-68.
Sasse A., 2003. Computer Security: Anatomy of a
Usability Disaster and a Plan for Recovery.
Proceedings of CHI2003 Workshop on Human-
Computer Interaction and Security Systems.
Schneier, B., 2000. Secrets and Lies: digital security in a
networked world. 1st ed.: John Wiley &Sons
Shun-Hua, T., Miao, C., Guo-Hai, Y., 2010. User behavior
mining on large scale web log data. International
Conference on Apperceiving Computing and
Intelligence Analysis, 60-63.
Whitten, A., Tygar, J., 1999. Why Johnny can’t encrypt: a
usability evaluation of PGP 5.0. Proceedings of 8th
USENIX Security Symposium, 169-183.
Xhafa, F., Ruiz, J., Caballe, S., Spaho, E., Barolli, L.,
Miho, R., 2012. Massive Processing of Activity Logs
of a Virtual Campus. Third International Conference
on Emerging Intelligent Data and Web Technologies,
104-110.
ZIshuang, Ye., Smith, S., 2005. Trusted Paths for
Browsers. ACM transactions in information systems
security, 8(2): 153-186.
LogAnalysisofHumanComputerInteractionsRegardingBreakTheGlassAccessestoGeneticReports
53
