
Integrating User-centred Design in an Early Stage of Mobile Medical
Application Prototyping
A Case Study on Data Acquistion in Health Organisations
Bernhard Peischl
1
, Michaela Ferk
2
and Andreas Holzinger
3
1
Softnet Austria, Inffeldgasse 16b/II, 8010 Graz, Austria
2
FERK Systems GmbH, Raiffeisenstrasse 46, 8010 Graz, Austria
3
Medical University Graz, Auenbruggerplatz 2/V, 8036 Graz, Austria
Keywords: ICF, ICD, User-centred Design, Data Acquisition in Healthcare, Usability Engineering in SMEs.
Abstract: This paper reports on collaborative work with an SME, developing a system for data acquisition in health
care organisations, providing mobile data support. We briefly introduce the ICF and the ICD classification
scheme from the WHO as a foundation for our mobile application. A two-staged usability evaluation in a
very early stage of development allows us to integrate user-centred design in the mobile application
development process. Our procedure comprises interviews and usability tests with a limited number of users
and thus can even be performed within a resource-constrained setting as it is typically found in smaller
software development teams. We discuss the consolidated results of the usability tests quantitatively and
qualitatively. From these results we deduce recommendations (and open issues) concerning the user
interface design of the mobile application.
1 INTRODUCTION
For almost 40 years, experiences have shown that
software engineering methods (e.g. the waterfall
model, V model and recently agile methods such as
Scrum) often result in poor user experience
(Holzinger and Slany, 2006). One of the reasons for
this is that requirement specifications (in particular
regarding the user interface and interaction design)
often do not reflect the real needs of the users.
Over the past decades, work in usability
engineering has shown that one of the best ways to
evaluate the quality of a user interface is to carefully
watch users interacting with the user interface
(Norman and Draper, 1986); however, this alone is
not enough, also the context and the environment is
of importance and we can speak of a total workplace
usability (Holzinger and Leitner, 2005). Depending
on the concrete development process and stage of
development this can be done with the application
(if already in place) or a mock-up in the form of a
paper prototype (Snyder, 2003).
Numerous projects have also shown that
substantial resources are needed for an adequate
interaction design and usability engineering
However, in practice software projects always
struggle with limited resources. Thus, today’s
challenge is to use fast, cheap and still efficient
usability engineering that can be used iteratively
throughout the development process (Hussain et al.,
2009).
This particularly holds for the development of
mobile business applications that typically do not
only have to fulfil high usability requirements but
also business-critical requirements. Moreover, the
sector specific contextual knowledge will influence
how user interface designs are perceived and
interpreted. Consequently, it is of uttermost
importance to integrate human-centred design into
the software development process as early as
possible (Holzinger et al., 2005).
In this paper we report on the design and
development of a mobile application for data
acquisition within healthcare organisations.
Typically, such an application is used by the nursing
staff, physiotherapists and other medical
professionals.
The application requires some basic knowledge
of standards such as the ICF (International
Classification of Functioning, Disability and Health,
WHO2) and the ICD classification (International
185
Peischl B., Ferk M. and Holzinger A..
Integrating User-centred Design in an Early Stage of Mobile Medical Application Prototyping - A Case Study on Data Acquistion in Health Organisations.
DOI: 10.5220/0004493901850195
In Proceedings of the 4th International Conference on Data Communication Networking, 10th International Conference on e-Business and 4th
International Conference on Optical Communication Systems (ICE-B-2013), pages 185-195
ISBN: 978-989-8565-72-3
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

Classification of Diseases, WHO1). This
prerequisite has to be taken into account when
addressing usability engineering methods from the
very beginning.
In this article we briefly provide an introduction
to the ICF and the ICD classification and outline
some surrounding success factors for mobile
business applications in general. In Section 4 we
focus on the user-centred design of our application.
We briefly explain the research questions, outline
the design of our usability tests and their execution
and describe the specific tasks our test users had to
fulfil. Afterwards we summarize the (1) results
quantitatively and briefly show the (2) outcome of
our qualitative evaluation. As a concrete outcome
for the next iteration within the software
development cycle we come up with
recommendations even before a single line of code
has been written. Our procedure is fast, cheap in
terms of resources and can be repeated at any point
in the development lifecycle. Notably this procedure
helped to discover usability flaws in a very early
stage of mobile application development.
2 ICF / ICD CLASSIFICATION
Our goal is to develop a software system, including
an application running on mobile devices that
supports acquisition and documentation of the health
state of a patient. Therefore we make use of the ICF
and the ICD standards (WHO1, 2012); (WHO2,
2012). Internationally endorsed classifications like
ICF and ICD facilitate the storage, retrieval,
analysis, and interpretation of data. For example,
this allows one for comparison of data within
populations over time as well as the compilation of
nationally or regionally consistent data.
ICF is a comprehensive classification of the
health state of a person. “Comprehensive” in this
sense means that the health state of a person is not
exclusively assessed by relying on physical
functions or disorders but also by taking into
account the possibility of an active lifestyle and
factors regarding the environment of the patient. The
ICF consists of several components (a hierarchical
structure grouped into physical functions, activities,
means of participation, environmental factors,
factors regarding the person itself), where each
component is assigned a set of ICF codes. The
assessment for each ICF code is done with the help
of a five-valued scale. The value increases with
increasing limitation of the patient. Details regarding
the assessment are explained in the ICF application
and training tools (WHO3).
The ICD is a classification system of medical
diagnoses. Within the ICD each medical diagnosis is
assigned to a three or four digit code. ICD also
supports hierarchies in terms of chapters, groups and
categories. In general the relevance of ICF codes
depends on ICD diagnoses. Therefore ICF-CoreSets
have been developed. ICF-CoreSets contain ICF
codes that are of particular relevance for groups of
ICD diagnoses.
3 SUCCESS FACTORS
The development of mobile applications for
professional usage in the healthcare field challenges
mobile software development in various ways.
First, there is the question of the platform being
supported. As the current landscape for mobile
operating systems is rather heterogeneous we need
to trade off advantages and drawbacks particularly
for the healthcare sector.
Second, and in contrast to the mainstream
consumer market, mobile business applications must
fulfil business critical requirements like a certain
degree of quality of service and requirements with
respect to security and privacy. The communication
of the mobile device and the data synchronisation
mechanism has to be robust and reliable independent
from place, time or usage context.
Third, as the application being developed is
highly interactive, the acceptance among the staff
members is crucial (Holzinger et al., 2011). This
success factor becomes even more crucial, as the
exposure to occupational stress in health care
organisations typically is extremely high. Unclear
user requirements pose a further challenge in
developing a user-centred and useful application. In
the following we particularly address this aspect.
4 USER-CENTRED DESIGN
Today it is well-known that usability engineering
methods have a huge impact on the perceived
quality of a software product or a software service.
However, in practice high costs and stringent time
planning prevent the use of these expensive methods
(Boivie et al., 2003), (Cooke and Mings, 2005),
(Larusdottir, 2011). In order to address user-centred
design in spite of limited resources, we propose to
integrate usability evaluation in a very early stage of
software design in terms of paper prototypes.
ICE-B2013-InternationalConferenceone-Business
186

Particularly within a fast-paced and innovation
driven setting, under presence of rather fuzzy
requirements, the early feedback of potential users
may considerably improve the quality of the
obtained design and product. Due to this, we
prohibit development efforts that do not match
market and user requirements. Our core element in
integrating usability engineering techniques into the
software development lifecycle is the interview-
guided usage of usability tests in combination with
paper prototypes.
Rubin and Chisnell (Rubin and Chisnell, 2008)
emphasize that the usage of usability engineering
techniques is appropriate as soon as obvious
usability flaws have been removed. Due to this, prior
to conducting usability tests we carried out several
walk-throughs within the small development team.
Further the initial design considered the usability
guidelines for mobile applications according to
Inostroza (Inostroza et al., 2012) as well as the
design guidelines for Android and iOS.
According to Rubin and Chisnell (Rubin and
Chisnell, 2008) we conducted an exploratory and
formative part of the usability evaluation. The
exploratory part of our usability tests aims to clarify
whether or not the assumed user profiles match with
the reality and whether our app provides assistance
in the daily work. In addition to the tests, we
emphasized this aspect by conducting interviews
questioning the state of practice in acquiring health-
related data. The formative part of our usability tests
aims to verify whether our design supports the user
in an optimal way.
4.1 Research Questions
As we relate usability tests with interviews about the
common work practices we decided to classify the
research questions accordingly. The interviews
being performed intend to strengthen the exploratory
component in our evaluation. In the course of the
interview, we reveal typical working procedures in
order to confirm our assumptions on user profiles
and the usage context.
As we interrelate usability test to the everyday
work in data acquisition in health care organisations
we break down our research questions according to
this. The interviews are supposed to strengthen the
explorative part of our evaluation and involve the
following questions:
What are typical working procedures for the
documentation of the health status of a patient in
the course of care and therapy?
To what extent are these procedures standardised?
For example, do you use standardised
questionnaires?
Is ICF used in practice or is the term ICF known at
all?
To what extent are medical doctors involved in the
documentation of a patient’s health status?
After having conducted these interviews in a
very early state of app development, we conducted
the formative component of the evaluation to
evaluate the quality of the user interface design. This
part of the evaluation strived to answer the following
questions:
Does the user benefit from using ICF, that is, does
ICF provide assistance in the working procedures?
Is all the relevant information processed?
Are overall usability and navigation within the app
intuitive?
Which kind of previous knowledge or which kind
of training is required in order to use the app in
everyday work?
This first and very early evaluation of the
usability in the software lifecycle mainly serves the
purpose of providing feedback regarding the
suitability of the user interface design. Taking into
account the lack of resources and the current
practice in software engineering this can be done
even with a small amount of test persons. It is well-
known that the number of test persons has an
economic as well as a qualitative impact. The more
test persons are being considered, the higher the
costs are and the more relevant the results of the
tests are. Thus, the main challenge in the given
context is to reveal as many usability problems as
possible with a small number of test persons.
According to Bastien (Bastien, 2010) the optimal
number of test persons is discussed since the
Nineties. At that time, about four to five test persons
were considered adequate to reveal 80 to 85 per cent
of all usability problems. In the meanwhile more
recent studies recommend a considerably higher
number of test persons (Bastien, 2010).
The number of persons is further determined by
the complexity of the tasks scheduled for the
usability test and is still an open research issue at the
moment. Up to now many successful research works
with practical relevance (Holzinger and Errath,
2007), (Horsky et al., 2010) follow the
recommendation from the Nineties (Short et al.,
1991), (Nielsen, 1994) to conduct usability tests with
four to five persons. According to Rubin (Rubin and
Chisnell, 2008) this number is sufficient to reveal
the majority of the usability problems.
Furthermore, Rubin (Rubin and Chisnell, 2008)
IntegratingUser-centredDesigninanEarlyStageofMobileMedicalApplicationPrototyping-ACaseStudyonData
AcquistioninHealthOrganisations
187

notes that the number of test persons can be smaller,
if the tests are carried out in an iterative manner.
Usability tests that consider the Thinking-Aloud
method can be conducted in an adequate manner
even with three persons per user group (Holzinger,
2005), (Holzinger, 2006), (Holzinger and Brown,
2008). As we used the Thinking-Aloud method,
supported the test in terms of interviews and
performed these tests in an iterative way, we
considered three persons as lower bound for
obtaining meaningful results. This holds for the
relevant user groups of nursing staff and therapists.
Medical doctors are considered as a fringe group, as
they turned out not to be the main users of our
application.
4.2 Test Design and Execution
After conducting the interview regarding the
common practice of collecting health-relevant data
we explained the basic idea of our application and
the concept of ICF. This was followed by a
demonstration of paper prototype tests and an
introduction to the Thinking-Aloud method.
For the usability tests we selected problems that
reflect the most common working procedures in the
daily business. The sequence of the individual tasks
was chosen to represent the typical sequence of tasks
in daily business with an increasing difficulty. After
conducting the usability tests the critical issues
observed during the test have been discussed with
the participants. In the following we briefly
summarize the individual tasks that had to be carried
out:
Task 1: Remembering the concepts of ICF and
ICD in order to establish optimal prerequisites for
the test. Participants were given the design of a
patient sheet(see Figure 2). Based on this design, we
asked the participants to describe the functionalities
behind the individual ICF- and ICD-related buttons.
Task 2: Assigning an ICD diagnoses and the
appropriate ICF-CoreSet to a patient. This test is
intended to establish the relationship between an
ICD diagnoses and an ICF-CoreSet. This
relationship aids in documenting the health state of
the patient at a later stage.
Task 3: Documenting the health status with ICF.
This task deals with the core of our application, the
recording of health-relevant data based on ICF
codes. The participants were asked to evaluate the
code “d450 Gehen”. For this purpose we provided
further information (diagnostic findings of nursing
staff etc.).
Figure 2: Patient sheet.
Task 4: Analysing the health status based on ICF
data. The final task considered the visualisation and
analysis of the ICF recording. First, the participants
were asked to retrieve those ICF codes that have
improved in the recent past (Task 4.1). Second, we
asked the participants to retrieve details about the
evolution of the ICFcode “d450 Gehen” (Task 4.2)
5 RESULTS
AND RECOMMENDATIONS
According to the questions raised in the previous
section, we summarize the results of the interviews
and usability tests. Large parts of the interviews
confirmed our assumptions about the common
working practices of our potential users.
5.1 Consolidated Findings
from the Interviews
Documentation of Health Status in Practice:
Typically the workflow related to the documentation
of the health status is perceived as tedious and
intensive in writing. Both, in health care and therapy
standardised metrics and questionnaires are used
(e.g. Barden index, Barthel index, or Morse-Fall
index). Besides the questionnaires particularly
physiotherapists mentioned the usage of the
“Visuelle Analogskala” (VAS) which is used for
subjective evaluation of pain intensity. The
standardised tools being employed capture a specific
aspect of the health state of a patient. Relevant
additional information is usually captured in the
form of free text. Questionnaires regarding the
ICE-B2013-InternationalConferenceone-Business
188
health state are employed on a regular basis,
however, the period of usage largely varies
depending on the patient. Besides the questionnaires
and the indexes most of the documentation work is
carried out in the form of free text. In care, almost
every action is documented in the form of free text.
Furthermore, the actions carried out by
physiotherapists and the goals of the therapy are
documented using free text.
Separation of Areas of Activity and user
groups: Nursing staff and physiotherapists consider
ICD diagnoses from medical doctors as a starting
point for their work, whereas the medical doctor
emphasised not to use the documentation and
questionnaires of nursing staff and physiotherapists.
This confirms our decision to put the focus of the
usability tests on nursing staff and physiotherapists
rather than on medical doctors.
ICF in Practice: The ICF schema is not used in
practice but is known from time of studying.
Particularly this holds for physiotherapists as the
ICF has been considered an important part of
vocational training. However, none of the
interviewed physiotherapists has used the ICF in
practice.
IT Support: Yet mobile technologies are not
used in daily work by the interviewed persons. In
some cases ward rounds are carried out with a
mobile laptop computer on a creeper. However,
aside of using mobile devices in healthcare, even the
usage of IT in the field of health documentation is
not very common. For example, some of the
interviewed persons mentioned that standardised
questionnaires are not processed automatically but
printed out and handwriting is used to fill out these
forms. Thus, for every patient there is a bulk of
paper to document the state of health and care.
5.2 Consolidated Findings
of the Usability Tests
In the following we provide a summary of the
quantitative results of our tests. However, our main
focus regarding the usability tests is on the
qualitative feedback from our test persons regarding
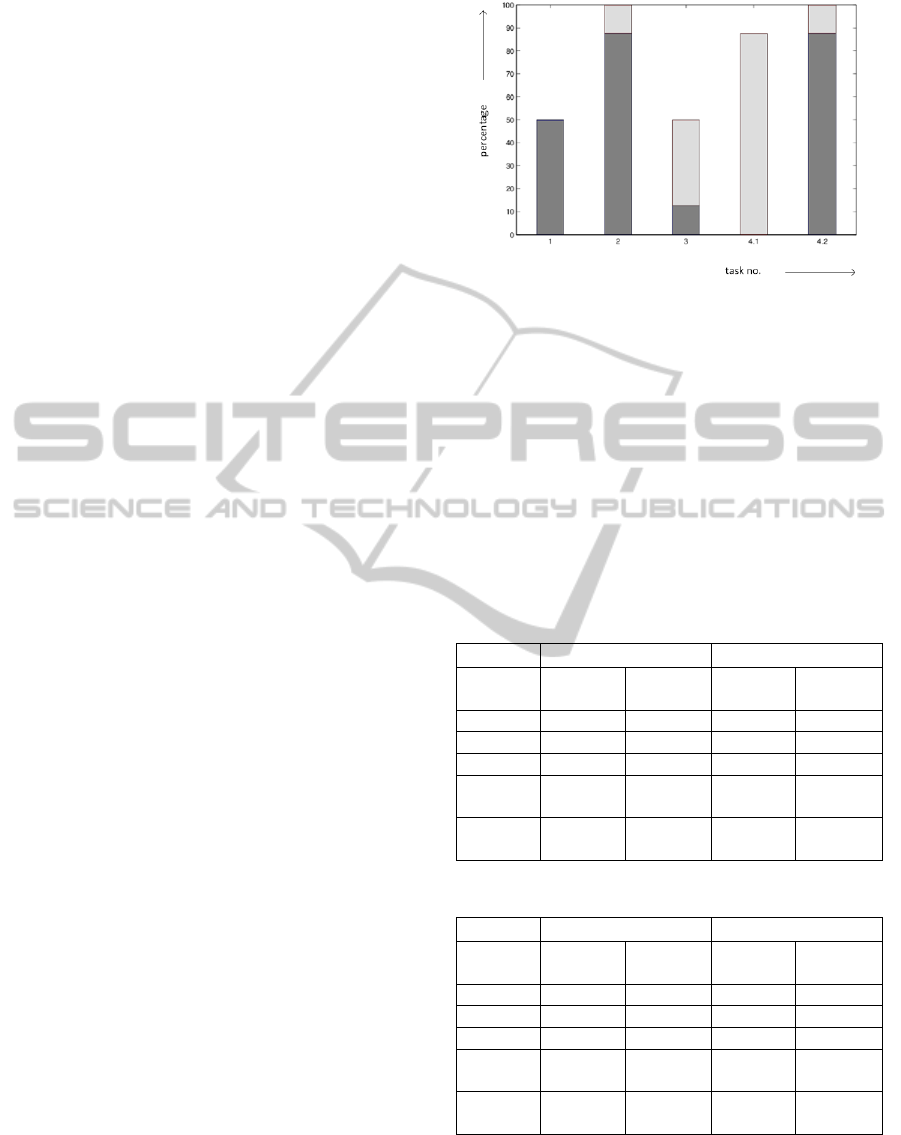
our design concept. Figure 1 outlines the degree of
fulfilment of the tasks discussed in the previous
section (percentage of fulfilled tasks) with (light
shaded) and without (dark shaded) assistance. On
average six out of eight participants were able to
fulfil the given tasks.
Table 1 outlines the comparison according to our
target user groups whereas Table 2 breaks the results
down according to whether a participant is
Figure 1: Percentage of fulfilment of the individual tasks.
experienced in handling a smartphone. Notably, the
results among physiotherapists are considerably
better than among the nursing staff and smartphone
users provided better results than test persons that
have no experience with smartphones at all.
However, it is important to note that all
physiotherapists in our test setting had experience
with smartphones whereas this only holds for about
50 per cent of the nursing staff. This fact has to be
taken into account when interpreting Table 1 and
Table 2.
Table 1: Results grouped by profession.
nursing staff physiotherapist
Task
no.
with.
assist.
without
assist.
with
assist.
without
assist.
Task 1
50 pc. 0 pc. 75 pc. 0 pc.
Task 2
75 pc. 25 pc. 100 pc. 0 pc.
Task 3
25 pc. 25 pc. 75 pc. 0 pc.
Task
4.2
0 pc. 75 pc. 0 pc. 100 pc.
Task
4.1
100 pc. 0 pc. 100 pc. 0 pc.
Table 2: Results grouped by experience of user.
exp. user non-exp. user
Task
no.
with.
assist.
without
assist.
with
assist.
without
assist.
Task 1
75 pc. 0 pc. 0 pc. 0 pc.
Task 2
100 pc. 0 pc. 67 pc. 33 pc.
Task 3
20 pc. 60 pc. 0 pc. 0 pc.
Task
4.2
0 pc. 100 pc. 0 pc. 67 pc.
Task
4.1
100 pc. 0 pc. 67 pc. 33 pc.
For the individual tasks, we obtained the following
qualitative feedback:
Task 1: Figure 2 shows the design of a patient
sheet. The bad results we obtained in this task of our
IntegratingUser-centredDesigninanEarlyStageofMobileMedicalApplicationPrototyping-ACaseStudyonData
AcquistioninHealthOrganisations
189

usability test are mainly due to a term
(“Krankheitsbild” in the German speaking test
environment corresponds to clinical picture or
disease pattern) we used to describe ICF-CoreSets.
Most of the test persons associated this term with the
term “diagnosis” and were not able to associate the
functionality of our application with this specific
term.
Recommendation: Choose a unique and well-
known term that captures the functionality of the app
also for users with a low knowledge of ICF so that
these users are able to associate the right
functionality with the term.
Figure 3: Acquisition of ICD diagnosis (left) ICF
classification (right).
Task 2: Figure 3 outlines the designs for the
acquisition of diagnoses and ICF classifications. All
participants have been able to fulfil this task. At the
very beginning of the design process, the
relationship between acquisition of ICD diagnoses
and ICF-CoreSets in everyday practice was an open
issue. Our interviews revealed that nursing staff and
physiotherapists partially carry out documentation of
a patient’s health status by relying on medical
diagnoses but do not fully rely on these. Therefore
the acquisition of ICF-CoreSets independently of the
medical diagnoses (given an appropriate hint)
appears to be suitable. The good results obtained
from this task emphasize that the user interface
design manages to convey the relationship between
both categories (ICF, ICD) and that navigation
within our application is intuitive.
Task 3: Figure 4 outlines the design of the ICF
acquisition supporting the documentation process.
The rather bad results obtained at this task primarily
result from the fact that around half of the test
persons did not use the supplemental information
regarding the assessment of the ICF codes.
Retrieving this supplemental information has been a
part of the finishing criteria for this task. Without
this finishing criterion the success rate would be 100
per cent. In Figure 4, each value is associated with
concrete criteria that a patient has to fulfil. This
supplemental information can be retrieved by
pressing the central buttons with the numbers.
Figure 4: Dialog for acquisition of the ICF values.
We identified several issues for this problem:
The meaning of the numbers for assessment is
not clear: A part of our test users did not understand
the meaning of the value. Figure 4outlines the value
for the code “d450 Gehen” which is displayed two
times (the green number 1). Although we had
briefed the participant that the assessment is based
on a 5 step scale, they could not associate this value
with the ICF number.
Recommendation: The problem revealed can be
addressed in two different ways. Training on the ICF
codes is a prerequisite for using our application.
Once it is clear to the users, how exactly an ICF
assessment is carried out, the interpretation of the
numbers should be quite obvious. On the other hand,
it might be possible to hide the numbers and use a
colour palette instead. Due to the problems with
colours used in our application (see the following
recommendation) we recommend to use numbers.
However, this issue should be an integral part of the
next iteration.
The relationship between assessment buttons
and the value for the assessment is not obvious:
Several test persons did not recognize the
relationship between the assessment buttons and the
number in the centre. Although our test persons
understood that red, yellow and green buttons denote
ICE-B2013-InternationalConferenceone-Business
190

a degradation of the health state, stable state or an
improvement regarding the health state, the fact that
hitting one of these buttons affected the ICF value in
the centre was not obvious to them. This problem
has already been revealed in the very early walk-
throughs and yielded to the decision to place the ICF
value in the centre of the assessment buttons.
However, the majority of our test persons preferred
positioning the value for the ICF assessment left to
the assessment buttons.
Recommendation: Relying on the obtained
results, the value for the ICF assessment should be
placed left to the assessment buttons. Moreover, a
visual aid, e.g. flashing the number when hitting an
assessment button, should emphasize the
relationship between the assessment buttons and the
value displayed for the ICF code.
Double meaning of colours: This task further
revealed a weakness of our colouring concept.
Several test persons were unsure about the (double)
meaning of our colour concept. On the one hand we
use the colours red, yellow and green for the
assessment buttons to depict degradation of the
health state, stable health state, and improvement of
the state. On the other hand we associated colours to
the ICF values. However, these colours do not
denote the evolvement of the health state but rather a
static assessment. For example, values 0 and 1 are
displayed in green as these values indicate a small
limitation of the patient whereas the values 3 and 4
are displayed in red correspondingly indicating a
severe limitation of the patient.
Recommendation: To solve this issue, set aside
the colouring for the ICF values. The colours green,
yellow and red should solely be used to indicate the
variation (degradation, stable state or improvement)
of ICF values.
Discovering information regarding the ICF
values: Our test persons had problems retrieving the
supplemental information regarding the ICF values.
Often the information for the ICF codes itself or
actions and goal planning (Figure 5) have been
retrieved.
Recommendation: To remove this problem, use
visual means to emphasize that there is some
relevant supplemental information regarding the
ICF values.
Task 4: This task deals with the assessments of
ICF codes. Notably the learning curve is strongly
increasing (see Figure 1) when moving from Task
4.1 to Task 4.2. Whereas none of our test persons
managed to solve Task 4.1 without assistance, 87.5
per cent of our test users were able to perform Task
4.2. This indicates that our user interface enables
simple guidance of the user through the menu and
our test users experienced some learning effect.
Task 4.1: Figure 5 (left) shows the alternation of
certain ICF codes over a certain period of time. In
this figure the current ICF assessment is compared
to 100 acquisitions. Our test persons have not been
able to correctly interpret this alternation. The
following issues have been discovered due to this
test.
Figure 5: ICF trend view (left) and details view on the
ICF-code “d450 Gehen” (right).
Information visualisation: Our test users did not
perceive that the values being displayed refer to a
time period of 100 acquisitions in between.
Intuitively our test users assumed that the current
assessment is compared with the previous
assessment. Our users did not pay attention to the
information that is indicating the longer time period
for acquisition (“100 Erfassungen”). Further, as in
Task 3, the double meaning of colours was
mentioned as a problem.
Recommendation: The time period over which
the trend of the assessment (degradation, constant
state, and improvement) is taking place has to be
emphasized. If possible, also try to reduce the
amount of information displayed to the user to ease
interpreting the data. Use the colours red, yellow
and green consistently but exclusively to depict the
change of health state.
Task 4.2: As mentioned previously the learning
effect from Task 4.1 was vast. Almost no one of our
test users had problems in navigating through the
menu. Figure 5 (right) outlines the detailed view for
the ICF code “d450 Gehen” which lots of our test
persons managed to retrieve without problems.
IntegratingUser-centredDesigninanEarlyStageofMobileMedicalApplicationPrototyping-ACaseStudyonData
AcquistioninHealthOrganisations
191

6 RELATED WORK
The number of health applications and research in
the area of mHealth is growing steadily with lots of
special applications for both the private and
professional sector (Waegemann, 2010), (Zuehlke et
al., 2009), (Phillips et al., 2010).
Applications for the consumer market cover a
variety of fitness and wellness applications, the
management of medication and assistance with self-
diagnosis (Holzinger et al., 2010). Furthermore there
is a variety of mobile health applications for
professional use which ranges from medical
applications to display medical images over
applications of ICD to electronic recording of patient
data.
Software solutions for using ICF are rather rare.
Most of the work regarding ICF deals with the
construction of ICF-CoreSets (DIMDI). In order to
select the relevant ICF codes for patients out of the
thousands ICF codes in general, there is a need for a
standardised set of ICF codes. In general, the set of
relevant ICF codes is related to the ICD diagnoses of
a patient. Therefore there are ICF CoreSets that
cover certain diagnoses or groups of diagnoses. Our
research revealed that there are well-documented
ICF-CoreSets for patients with backache,
osteoporosis, Diabetes mellitus, pain disorder and
depressive disorder (Rensch and Bucher, 2006).
Bender (Bender, 2010) points out that numerous
health organisations experience problems when
applying the ICF classification in practice.
According to (Bender, 2010) the reason for this is
the lack of guidelines for practical application of the
complex ICF classification scheme.
The Rehab-CYCLE software from the RehabNet
AG (DIMDI) to our best knowledge has been the
first ICF-based desktop application for
rehabilitation. This software allows describing the
health status of a patient by using the ICF as well as
the formulation of rehabilitation goals and the
planning of the corresponding activities. This
functionality is supported in terms of an ICF-
browser and ICF-CoreSets for numerous diseases.
As in our case Rehab-CYCLE has been developed in
close collaboration with universities and has been
successfully used from 2004 to 2011 within hospital
facilities in Switzerland and Germany.
In the meanwhile Rehab-CYCLE has been
substituted by the web-enabled application
RehabNET-IPS. As this application can be accessed
via a browser, the access via mobile devices is
possible. However, to our best knowledge there has
been no effort in adapting the application towards
the usage with mobile devices.
Our market research revealed only a single ICF-
based documentation system explicitly supporting
mobile devices, the ICOSys application developed
by Management Partners (ICOSYS, 2012);
(ICOSYS.MOBIL, 2012). The possibility to use the
ICF-classification is embedded within a module
system which is providing functionalities ranging
from the management of resources and patients to
time recordings for employees. ICOsys.mobil runs
on the Windows Mobile operating system. It is an
open issue whether there have been attempts to port
ICOsys.mobil to state of the art platforms like iOS
or Android.
The German company MediFox (MEDIFOX)
offers a mobile software solution on the Windows
Phone platform. However, to our best knowledge
this application does not support the usage of the
ICF classification but offers a spectrum of metrics to
measure the health status of a patient, e.g. the
Braden-Skala. Notably, there is a major difference to
our ICF-based approach: Each of the metrics and
assessments captures a part of the health status in a
highly specialized but isolated manner. Opposed to
this, ICF considers the health status as a whole and
uses a uniform and quantifiable assessment scheme.
However, today it is an open issue whether a
documentation based on the ICF can fully substitute
this spectrum of metrics.
7 CONCLUSIONS
In this article we presented collaborative research
conducted in association with an SME dealing with
the integration of user-centred engineering methods
into mobile application development in a very early
phase of development. The application that has been
designed and developed is part of a larger system
that allows one for acquisition and documentation of
the health state of a person. Our mobile application
is primarily used by nursing staff and
physiotherapists. In this context usability questions
are tied to domain knowledge and practices and thus
this has to be taken into account in particular.
The article gives a brief overview on the
documentation of the health state of a person using
the ICF and the ICD classification scheme according
to the WHO. In our research it turned out that the
scheme is known by physiotherapists but not used in
practice yet. However, our research further revealed
that additional training on the basic ideas of the ICF
and ICD might be necessary in order to establish
acceptance among nursing staff. The authors of
ICE-B2013-InternationalConferenceone-Business
192

(Ziefle et al., 2011) also point out the need for
additional training and thus further support our
findings. Nevertheless, the ICF and the introduction
of mobile devices appears to be beneficial as it
simplifies the prevailing working procedures.
Regarding the mobile application development
for the healthcare domain we identified three success
factors: choosing the appropriate platform, the
fulfilment of business-critical requirements and the
integration of user-centred design into mobile
application development.
In integrating user-centred design into the
software development lifecycle we conducted a two-
staged procedure based on walk-throughs,
interviews and usability tests. Notably this can be
performed in an (1) early stage of development and
with (2) a limited amount of resources and thus is
suitable for smaller development teams and SMEs.
Our procedure is repeatable and revealed design
flaws in the user interface in a very early stage of
development. We briefly summarized quantitative
and qualitative results (with emphasis on the latter
one). From the results we deduced some
recommendations and issues to be investigated in the
next iteration. Finally we summarized related work
on acquisition and documentation of the health state
of a person focusing primarily on products and
studies that use the ICF and ICD classification for
documentation.
ACKNOWLEDGEMENTS
The work presented herein has been partially carried
out at Ferk Systems and has been partially funded by
Ferk Systems and the SME program
“Innovationsscheck” of the Austrian Research
Promotion Agency (FFG, contract no. 840346).
REFERENCES
AMED Dolan, P. Doctors cite ease of use in rapid
adoption of tablet computers, http://www.ama-
assn.org/amednews/2011/04/18/bisc0418.htm (visited
on Dec. 30th 2012).
AND1 Notes on the implementation of encryption in
Android 3.0,
http://source.android.com/tech/encryption/android_cry
pto_implementation.html (visited on 2
nd
July 2012).
APPLE1 Apple Inc,iOS Developer Enterprise Program.
https://developer.apple.com/support/ios/enterprise.htm
l (visited Dec. 30
th
2012).
APPLE2 Apple Inc, Distribute apps to your users,
http://www.apple.com/business/accelerator/deploy/app
-distribution.html (visited Dec. 30
th
2012).
APPLE3 Apple Inc. iOS Security,
http://images.apple.com/ ipad/ business/ docs/ iOS-
Security_May12.pdf (visited on May 2012).
APPLE4 Apple Inc., iOS Security,
http://images.apple.com/ipad/business/docs/iOS-
Security_May12.pdf (visited May 30
th
, 2012).
Bastien, J. M. C, 2010, Usability testing: a review of some
methodological and technicalaspects of the method.
In: International Journal of Medical Informatics79
(2010), Nr. 4, S. e18–e23. – ISSN 1386–5056.
Bender, 2010, D.: Voraussetzungen für die nachhaltige
Anwendung der Internationalen Klassifikation der
Funktionsfähigkeit, Behinderung und Gesundheit
(ICF) in der Rehabilitationspraxis Ergebnisse einer
Analyse im Spannungsfeld von globaler Konzeption
und lokaler Umsetzung. 4. Tectum Verlag, 2010
(Wissenschaftliche Beiträge aus dem Tectum Verlag:
Pädagogik 21). – ISBN 9783828824867.
Bloice, M. ;Simonic, K. ; Kreuzthaler, M. ; Holzinger, A.,
2011, Developmentof an interactive application for
learning medical procedures and clinical decision
making. In: Proceedings of the 7th conference on
Workgroup Human-Computer Interaction and
Usability Engineering of the Austrian Computer
Society: information Quality in e-Health. Berlin,
Heidelberg, Springer-Verlag, 2011, (USAB’11), ISBN
9783642253638, S. 211–224.
Boivie, I. ;Åborg, C. ; Persson, J. ; Löfberg, M., 2003,
Why usability gets lostor usability in in-house
software development. In: Interacting with
Computers15 (2003), Nr. 4, S. 623–639. – ISSN
0953–5438.
Cooke, L. ;Mings, S., 2005, Connecting usability
education and research withindustry needs and
practices. In: Professional Communication, IEEE
Transactions on 48 (2005), Nr. 3, S. 296–312. – ISSN
0361–1434.
CSC Turisco, F. , Garzone, M., 2012, Harnessing the
value of mhealth for your organization, http://
www. csc.com/ health_services/ insights/69713-
harnessing_the_value_of_mhealth_for_your_organizat
ion (visited on Dec. 30
th
, 2012).
DIMDI Deutsches Institut für Medizinische
Dokumentation und Information, www. dimdi.de/
static/de/klassi/icf/icfprojekte.html (visited on Dec.
30th, 2012).
M. Ferk 2013, Konzeption und Entwicklung einer
gelegentlich verbundenen mobile Applikation für die
Datenerfassung in Gesundheitsorganisationen, Master
Thesis, Technische Universität Graz, 2013.
GOOGLE1, Google, Intents and Intent Filters. URL:
http://developer.android.com/guide/components/intent
s-filters.html (visited on 15
th
June 2012).
Holzinger, A. 2005, Usability engineering methods for
software developers.In:Commun. ACM 48 (2005), Nr.
1, S. 71–74. – ISSN 0001–0782.
Holzinger, A. ;Errath, M. 2007, Mobile computer Web-
application design inmedicine: some research based
guidelines. In: Univers. Access Inf. Soc. 6 (2007), Nr.
IntegratingUser-centredDesigninanEarlyStageofMobileMedicalApplicationPrototyping-ACaseStudyonData
AcquistioninHealthOrganisations
193

1, S. 31–41. – ISSN 1615–5289
Holzinger, A. & Brown, S, 2008, Low cost prototyping:
Part 2, or how to apply the thinking-aloud method
efficiently. In: Abuelmaatti, O. & England, D. (eds.)
Proceedings of HCI 2008. Liverpool: John Moores
University (UK): British Computer Society. 217–218.
Holzinger, A. & Leitner, H, 2005, Lessons from Real-Life
Usability Engineering in Hospital: From Software
Usability to Total Workplace Usability. In: Holzinger,
A. & Weidmann, K.-H. (eds.) Empowering Software
Quality: How can Usability Engineering reach these
goals? Vienna: Austrian Computer Society, pp. 153-
160.
Holzinger, A. & Slany, W., 2006, XP + UE -> XU
Praktische Erfahrungen mit eXtremeUsability.
Informatik Spektrum, 29, (2), 91-97.
Holzinger, A, 2006, Thinking-aloud – eine
Königsmethode im Usability Engineering, OCG
Journal, 31, (1), 4-5.
Holzinger, A., Dorner, S., Födinger, M., Valdez, A. C. &
Ziefle, M., 2010, Chances of Increasing Youth Health
Awareness through Mobile Wellness Applications.
Lecture Notes in Computer Science (LNCS 6389).
Berlin, Heidelberg: Springer, pp. 71-81.
Holzinger, A., Geierhofer, R., Ackerl, S. & Searle, G,
2005, CARDIAC@VIEW: The User Centered
Development of a new Medical Image Viewer. In:
Zara, J. &Sloup, J., eds. Central European Multimedia
and Virtual Reality Conference (available in
Eurographics Library), 2005 Prague. Czech Technical
University (CTU), 63-68.
Holzinger, A., Searle, G. & Wernbacher, M., 2011, The
effect of Previous Exposure to Technology (PET) on
Acceptance and its importance in Usability
Engineering. Universal Access in the Information
Society International Journal, 10, (3), 245-260.
Horsky J. ; McColgan, K. ; Pang, J. E. ; Melnikas, A. J. ;
Linder, J.A. ;Schnipper, J. L. ; Middleton, B. et al.
2010, Complementary methods of system
usabilityevaluation: Surveys and observations during
software design and development cycles. In: Journal
of Biomedical Informatics 43 (2010), Nr. 5, S. 782–
790– ISSN 1532–0464.
Hussain, Z., Slany, W. & Holzinger A., 2009, Current
State of Agile User-Centered Design (AUCD): A
Survey. Human-Computer Interaction and Usability
for e-Inclusion. 5th Symposium of the Austrian
Computer Society, USAB 2009, Lecture Notes in
Computer Science (LNCS 5889). Berlin, Heidelberg,
New York: Springer, pp. 416-427.
ICOSYS http://www.icosys.at/icosys/de/philosophie/
index.php (visited on Dec. 30th, 2012).
ICOSYS.MOBIL http://www.icosys.at/icosys/de/news/
news_details.php?id=17 (visited on Dec. 30th, 2012).
IDC1 International Data Corporation, http://www.
idc.com/home.jsp?t=1351618548017 (visited Dec. 30
th
2012).
IDC2 International Data Corporation, International Data
Corporation. Android and iOS Surge to New
SmartphoneOS Record in Second Quarter, According
to IDC, http://www.idc.com/getdoc.jsp?
containerId=prUS23638712 (visited Dec. 30
th
2012).
InostrozaR. ;Rusu, C. ; Roncagliolo, S. ; Jimenez, C.
;Rusu, V., 2012,Usability Heuristics for Touchscreen-
based Mobile Devices. In: InformationTechnology:
New Generations (ITNG), 2012 Ninth International
Conferenceon, 2012, S. 662–667.
JSAES1 JSAES: AES in JavaScript, http://point-at-
infinity.org/jsaes/ (visited on 2
nd
July 2012).
Larusdottir, M. 2011, Usability Evaluation in Software
Development Practice. In:Human-Computer
Interaction – INTERACT 2011 Bd. 6949. Springer
BerlinHeidelberg, 2011. – ISBN 9783642237676, S.
430–433.
Liu, C.; Zhu, Q., Holroyd, K., Seng, E., 2011, Status and
trends of mobilehealthapplications for iOS devices: A
developer’s perspective. In: Journal ofSystems and
Software 84 (2011), Nr. 11, S. 2022–2033. – ISSN
0164–1212.
MAN Manhattan Research, http://manhattanresearch.com/
(visited on December 30th 2012)
MEDIA HTML Media Capture, http://www.developer.
com/ ws/ android/ development-tools/ add-text-to-
speech- and- speech- recognition- toyour- android-
applications.html (visited May 30
th
2012).
MEDIFOX www.medifox.de
Muchow, 2012, Using Keychain to Store Username and
Password, http://mobiledevelopertips.com/core-
services/using-keychainto-store-username-and-
password.html (visited 30
th
May 2012).
Nielsen, J., 1994, Estimating the number of subjects
needed for a thinking aloud test. International Journal
of Human-Computer Studies, 41, (3), 385-397.
Norman, D. A. & Draper, S. 1986. User Centered System
Design, Hillsdale (NY), Erlbaum.
Phillips, G., Felix, L., Galli, L., Patel, V. & Edwards, P.,
2010, The effectiveness of M-health technologies for
improving health and health services: a systematic
review protocol. BMC Research Notes, 3, (1), 250.
M. Pilgrim,The past, present and future of local storage for
web applications, http://diveintohtml5.info/
storage.html (visited 30
th
May 2012).
Rensch, H. ; Bucher, P., 2006, ICF in der Rehabilitation:
Die praktische Anwendung der internationalen
Klassifikation der Funktionsfähigkeit, Behinderung
und Gesundheit im Rehabilitationsalltag. 4. 2006. –
289–291 S.
D. Rousset, Introduction to HTML5 Web Workers: The
JavaScript Multithreading Approach., http://msdn.
microsoft.com/en-us/hh549259.aspx (visited 30
th
Dec.
2012).
Rubin, J. Chisnell, D., 2008, Handbook of Usability
Testing 2, Wiley Publishing, Inc., 2008.
Short, E. J., Evans, S. W., Friebert, S. E. &
Schatschneider, C. W, 1991, Thinking aloud during
problem solving: Facilitation effects. Learning and
Individual Differences, 3, (2), 109-122.
Snyder, C, 2003, Paper Prototyping, San Francisco,
Morgan Kaufmann.
STORAGE http://developer.android.com/guide/topics/
ICE-B2013-InternationalConferenceone-Business
194

data/data-storage.html#filesInternal (visited 2
nd
of July
2012).
Tactio Software International, Global
mHealth Developer Survey,
http://www.tactiosoft.com/files/GlobalmHealthDevelo
perSurvey.pdf, 2010 (visited 30
th
Dec. 2012).
Waegemann, C. P. 2010. mHealth: The Next Generation
of Telemedicine? Telemedicine Journal and E-Health,
16, (1), 23-25.
WHO1, WHO, International Classification of Diseases
(ICD), http://www.who.int/classifications/icd/en/
(visited on 30
th
of Dec2012).
WHO2, WHO, International classification of functioning,
disability and health (ICF), http://www.who.int/
classifications/icf/en/ (visited on 30
th
of Dec 2012).
WHO3, WHO, Towards a Common Language for
Functioning, Disability and Health, http://
www.who.int/classifications/icf/icfapptraining/en/inde
x.html (visited on 30
th
of Dec. 2012).
Ziefle, M., Roecker, C. & Holzinger, 2011, A. Perceived
usefulness of assistive technologies and electronic
services for ambient assisted living. 5th International
Conference on Pervasive Computing Technologies for
Healthcare (PervasiveHealth) 2011, 23-26 May 2011
2011 Dublin. IEEE, 585-592.
Zuehlke, P., Junhua, L., Talaei-Khoei, A. & Ray, P, 2009,
A functional specification for mobile eHealth
(mHealth) systems, 11th International Conference on
e-Health Networking, Applications and Services
(IEEE Healthcom 2009). Sydney, NSW, Australia:
IEEE, 74-78.
IntegratingUser-centredDesigninanEarlyStageofMobileMedicalApplicationPrototyping-ACaseStudyonData
AcquistioninHealthOrganisations
195
