
Using Knowledge Management Tools and Techniques to Increase the
Rate of Attendance at Breast Screening
Rajeev K. Bali
1
, Jacqueline Binnersley
1
, Vikraman Baskaran
2
and M. Chris Gibbons
3
1
BIOCORE Applied Research Group, Coventry University, Puma Way, Coventry, U.K.
2
College of Continuing and Professional Studies, Mercer University, Atlanta, U.S.A.
3
Johns Hopkins Urban Health Institute, John Hopkins University, Baltimore, U.S.A.
Keywords: Knowledge Management, Breast Screening, Barriers to Attendance.
Abstract: Breast screening is an important method of detecting cancer early, with around a third of breast cancers now
diagnosed through screening. Previous research has demonstrated that there are many contributors to health
inequalities, with poor access to good health services chief among them: there are significant disparities in
the use of health services linked to income, ethnicity and education. Empirical data was analysed from a
breast screening service (n=159,405) using advanced data mining techniques, as well as being collected
from service users by way of two focus groups conducted before and after the use of a detailed
questionnaire (n=102). The results were used to make recommendations of interventions to reduce the rate
of non-attendance.
1 INTRODUCTION
Breast cancer is the most common cancer in women,
with over 40,000 being diagnosed each year in the
UK (Cancer Research UK, 2005). Screening is an
effective way to detect cancer early, with around a
third of breast cancers being diagnosed in this way.
There is currently a screening program catering to
almost two million women in the UK (Cancer
Research UK, 2005), which screens all eligible
women every three years. The information published
by the UK Government Statistical Service has
shown that for the ten years since 1995, the uptake
has remained constant at around 75%.
Previous research has shown that non-attendance
is associated with having to travel long distances to a
screening centre (Baskaran, 2008), with a woman’s
economic background and a lack of family support
(Katz et al., 2000). According to Bekker et al.
(1999), non-attendance can be attributed to
disinterest, negative attitudes, beliefs, medical
problems and fear of X-rays. These factors could be
addressed by educating people about the importance
of screening and tackling some of the socio-cultural
and personal barriers to attendance (Cassandra,
2006). Baskaran (2008) was able to predict breast
screening attendance using factors such as age,
previous attendance, postal area, past cancer history,
history of a false positive result and a representation
of socio-economic status called the Townsend score
(Townsend et al., 1988).
Semi-permanent factors such as ethnicity, age,
marital status, income, education and long term
conditions may affect whether women attend
screening (Katz et al., 2000). These may be more
difficult to address than temporary factors such as
employment, personal apprehensions, beliefs,
knowledge and access to screening facilities (Sin
and Leger 1999, Bekker et al., 1999). It has been
found that using mobile screening units rather than
expecting women to travel long distances can
improve attendance rates (Day et al., 1989).
Interventions with educational materials have
limited effectiveness but when used in conjunction
with primary care initiatives they can help women to
make informed decisions about screening (Jepson et
al., 2000). Primary care can address some of the
temporary factors, such as personal apprehensions,
beliefs and knowledge (Fox et al., 1991; Bekker et
al., 1999). Bankhead et al. (2001) found letter based
interventions by primary care to be effective and
Atri et al. (1997) found a telephone intervention to
be effective.
Baskaran (2008) used the techniques and tools of
knowledge management to identify women with
344
K. Bali R., Binnersley J., Baskaran V. and Chris Gibbons M..
Using Knowledge Management Tools and Techniques to Increase the Rate of Attendance at Breast Screening.
DOI: 10.5220/0004544503440350
In Proceedings of the International Conference on Knowledge Discovery and Information Retrieval and the International Conference on Knowledge
Management and Information Sharing (KMIS-2013), pages 344-350
ISBN: 978-989-8565-75-4
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)
characteristics associated with non-attendance at
breast screening. Knowledge management is an
approach that is concerned with the creation and
sharing of knowledge, with the aim of improving the
efficiency and effectiveness of organisations (Bali et
al., 2009). Early detection has a huge impact on
reducing cancer related deaths (Baskaran, 2008) and
therefore, the primary concern is to reduce non-
attendance (Bankhead et al., 2001).
2 AIMS AND OBJECTIVES
The current project aimed to use the tools and
techniques of knowledge management to identify
women who face barriers to breast screening
attendance and to suggest effective ways of
overcoming these. The objectives were to:
Show that screening non-attendance can be
attributed to demographic factors and
screening history
Understand the reasons why some women
fail to participate in the program
Examine inequalities and disparities in
relation to accessing screening
Recommend interventions to reduce the
impact of the barriers and increase the rate
of attendance at breast screening
3 METHODS
Stage One: (Quantitative) Analysis of
Screening Records
The Warwickshire, Solihull and Coventry Breast
Screening Service is part of the National Breast
Screening Program and invites around 55,000
women to participate each year. Data mining
techniques were used to analyse a large number of
the records of service users.
Stage one of the current study used two distinct
approaches. The first approach focused on predicting
non-attendees and the second approach used results
generated at the end of the screening episodes to
identify those women who had failed to attend.
The first approach used an artificial intelligence
algorithm (which embedded knowledge
management activity) to predict non-attendance. It
employed Neural Network algorithms and included
a Service Orientated Architecture to deliver the
knowledge. This work combined the existing
National Breast Screening Computer System
software into a single platform and created a
prototype software component based on Open
Source technologies. The prototype software was
automated to produce the pre-processed data and
eventually normalise the data for artificial
intelligence (neural network) assimilation. These
activities were performed sequentially.
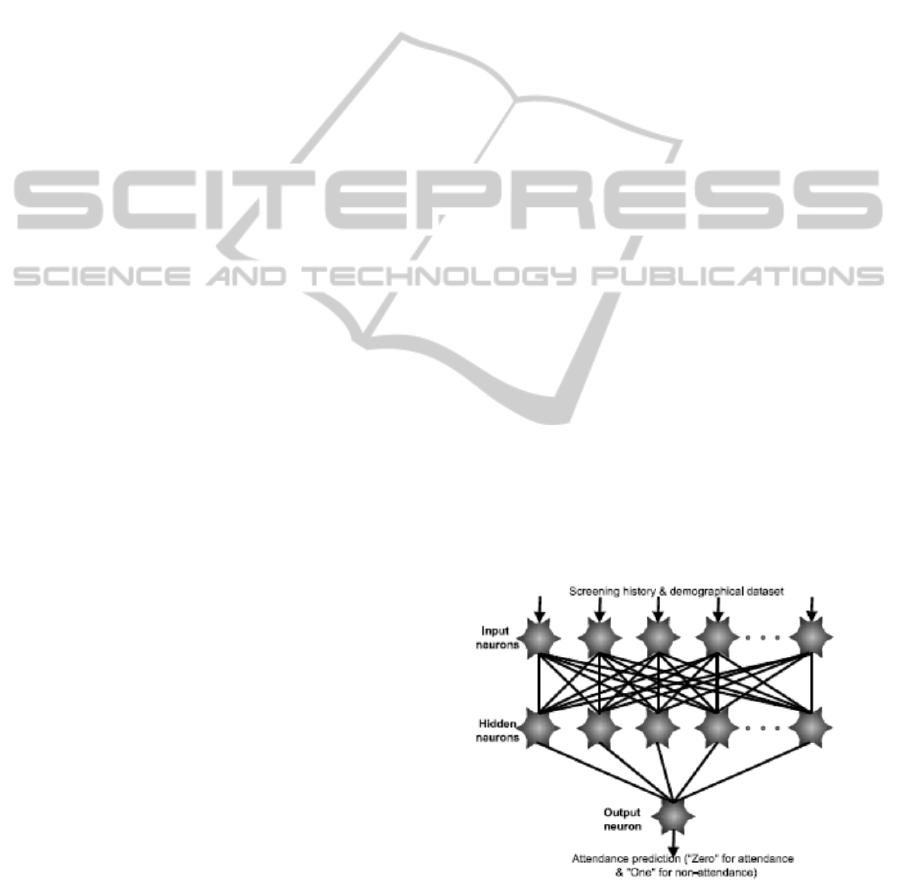
The Java Based Attendance prediction by
Artificial Intelligence for Breast Screening model
was simulated on the Open Source technology
platform. It used historical screening data and
demographic information from the National Breast
Screening database as predicting factors. This was
converted to a flat file and formed the dataset that
was presented to the input neurons. The output
neuron remained at ‘zero’ when a woman was
predicted to attend screening and showed ‘one’ for a
non-attendee (see Figure one). Earlier research had
confirmed that one hidden layer would suffice to
map any multivariate type of input domain to the
output domain. During the training stage, the error
function was fed back through the network from the
output neuron. The knowledge capture was
implemented using the architecture shown in figure
one.
The user (via the GUI interface) pointed the
neural networks to the location of the historical data
(in the flat file) to train the network. Once the
training was completed, the net was pointed to the
normalised data so that prediction could be initiated.
Any errors during the pre-processing, training and
the actual prediction activities were stored in
individual log files which could be viewed at a later
point in time.
Figure 1: Knowledge creation captured within artificial
intelligence neural networks.
The GUI gave the option to the user to initiate
the Simple Object Access Protocol (SOAP)
message. The message body was instantiated with
UsingKnowledgeManagementToolsandTechniquestoIncreasetheRateofAttendanceatBreastScreening
345

reference to an eXtensible Markup Language (XML)
schema definition designed on the Health Level 7
version 3 standards. The message was called upon
by the software to generate the SOAP envelope and
attached the XML message to the SOAP body with a
digital signature (for security). The Java-based web
services technology provided encryption to make the
message completely secure. The message was
transmitted via web services to the general
practitioner’s mailbox server.
Once the doctor’s server connected with the
mailbox it downloaded the messages and
automatically updated the womens’ records with the
likelihood of non-attendance. Meanwhile the breast
screening service continued its routine process of
inviting women by dispatching an appointed letter
(with details of the screening date and time). General
practitioners were now aware of those women who
are likely to miss breast screening appointments. If
those women visit the doctor for other services the
doctor can initiate an opportunistic intervention,
thereby increasing the likeliness of improving
screening uptake.
The second approach relied on knowledge
generated through a bespoke software program
written to capture non-attendees from results
generated by the National Breast Screening
Software. The prototype
framework incorporated the artificial intelligence
model for creating a list of predicted non-attending
women. The screening service produced the results
of the screening activity and used a report template
to export the batch list. The user (via GUI) pointed
to the location of the flat file to segregate the non-
attendees. Once segregation was complete, a new
message was generated using the same procedure as
before and it was sent to the respective general
practitioners. This updated the women’s medical
records with their non-attendance. The prototype
combined the demographic data pertaining to the
non-attending women and sent this information to
the General Practitioner as a messaging package.
The package triggered the generation of an
electronic message based on the Health Level 7
version 3 standards and utilised Service Orientated
Architecture as the message delivering technology.
The system has been designed in a way that will
enable it to be integrated into the UK health system.
Both approaches relied on the ability of the general
practitioner to intervene once women had been
identified as having characteristics that had been
shown to be associated with non-attendance.
Stage one of the project used quantitative
techniques to establish that non-attendance can be
predicted. The results can be shared with healthcare
providers in order to target interventions at women
who have characteristics associated with non-
attendance and overcome some of the barriers that
they face.
As the data collected in stage one was
impersonal (in addition to being anonymised),
personalised (human) components such as personal
apprehension, ethnicity-based influences, age-based
factors, personal economic circumstances and socio-
cultural factors also needed to be considered. To
address these “softer” issues and in order to
triangulate the results (from a qualitative
perspective), the use of focus groups was a natural
evolution of this study. In order to explore these
aspects further, two focus groups were carried out
(which straddled a detailed questionnaire).
Stage Two: (Qualitative) First Focus
Group
The information from the analysis of the records was
used to form a list of topics for discussion in the first
focus group, the aim of which was to identify
barriers to breast screening attendance. Participants
for the focus groups and questionnaire were clients
of Age UK, an organisation that aims to improve the
lives of older people (Age UK, 2013). Data from the
focus groups was analysed using thematic analysis
as described by Aronson (1994).
Stage Three: (Quantitative)
Questionnaire
The results of the initial focus group were compared
to the literature review and used to form a
questionnaire, using a technique described by Hoppe
et al. (1995) and Lankshear (1993). The aim of the
survey was to find out whether the views expressed
by the small number of people in the focus group
were shared by a larger and more representative
sample.
Stage Four: (Qualitative) Final Focus
Group
A second focus group discussed ways of tackling the
barriers to screening that had been identified.
KMIS2013-InternationalConferenceonKnowledgeManagementandInformationSharing
346

4 RESULTS
Stage One: Analysis of Screening
Records
Data mining techniques were used to analyse records
from the local breast screening service. The valid
records constituted 86% (n=159,405) of the
extracted dataset. From 2002, women in the age
range 65-70 had an uptake of 70%. The efficiency of
the program can be mapped to attendance and the
number of non-attendees has been increasing so that
it has now reached half a million. Simple projection
of this data suggests that nearly 4,000 cancer
incidences would have been missed due to non-
attendance. A literature review identified factors that
have been shown to be associated with non-
attendance and for this reason analysis of the records
focused on key fields like Townsend Deprivation
Score, postcode and distance that women travelled
to a screening appointment.
Stage one of the current study produced bespoke
software developed within an open source
environment that was able to use demographic data
to identify individuals who were likely to face
barriers to attendance. Sharing this knowledge with
primary care enabled health professionals to deliver
interventions that helped the women make informed
decisions about whether to attend screening.
Stage Two: First Focus Group
Six participants took part in the first focus group.
They were five women and one man, with ages
ranging from 45-87 years. They all stated that their
ethnicity was English or British and they were either
retired or a housewife. Participants were asked why
they thought some women did not attend breast
screening and a variety of possible reasons were
discussed. Three main themes were identified and
the results will be presented under headings related
to these.
Communication Problems
The theme of communication problems incorporated
sub-themes of people not understanding English,
people being hard of hearing and people not
understanding medical terms.
The group thought interpreters and/ or
representatives from the patient’s community should
be available to support people who do not
understand English. It was also suggested that in
order to tackle all the forms of communication
problems, health professionals should avoid using
jargon and check that they have been understood.
Transport Problems
Public transport was thought to be unreliable,
journeys often took a long time and participants
were reluctant to ask other people for lifts. One
participant had used hospital transport and thought it
would be helpful to raise awareness of this service.
Reasons Associated with Beliefs and
Attitudes
Three sub-themes were identified: embarrassment,
anxiety and not realising the importance of
screening. The group thought that older people were
more likely to be embarrassed about having to
undress for examinations than younger people and
people with a cultural background that emphasised
female modesty might find screening examinations
particularly difficult.
It was clear that there was no single reason for
the anxiety that many women experience in relation
to screening. Two participants who had not yet been
invited to attend screening were anxious because
other people had told them that the procedure was
painful. Other group members had first-hand
experience of painful breast examinations and this
made them reluctant to return. One woman had
extensive scarring on her chest that made screening
unbearable. It was suggested that professionals
should acknowledge that the procedure could be
uncomfortable and offer ultrasound scans where
appropriate. The anxiety about receiving a positive
result was also discussed and it was also suggested
that some people might be unaware of the value of
screening.
Stage Three: Questionnaire
147 questionnaires were given out and 102 were
completed, giving a response rate of 69%. 93
women and 9 men completed the questionnaire and
their average age was 65. Although the majority (69)
stated their ethnicity to be White British, 16% were
from an Asian Background and 12% were from a
Black background. People from an Asian
background make up 12% of Coventry’s population
and people from a Black background make up 3%
(Coventry Link, 2012). These are the largest
minority groups in Coventry and were well
represented in the survey. The pie chart (see figure
two) shows the ethnic origins of the survey
participants. Four Irish people took part in the
UsingKnowledgeManagementToolsandTechniquestoIncreasetheRateofAttendanceatBreastScreening
347
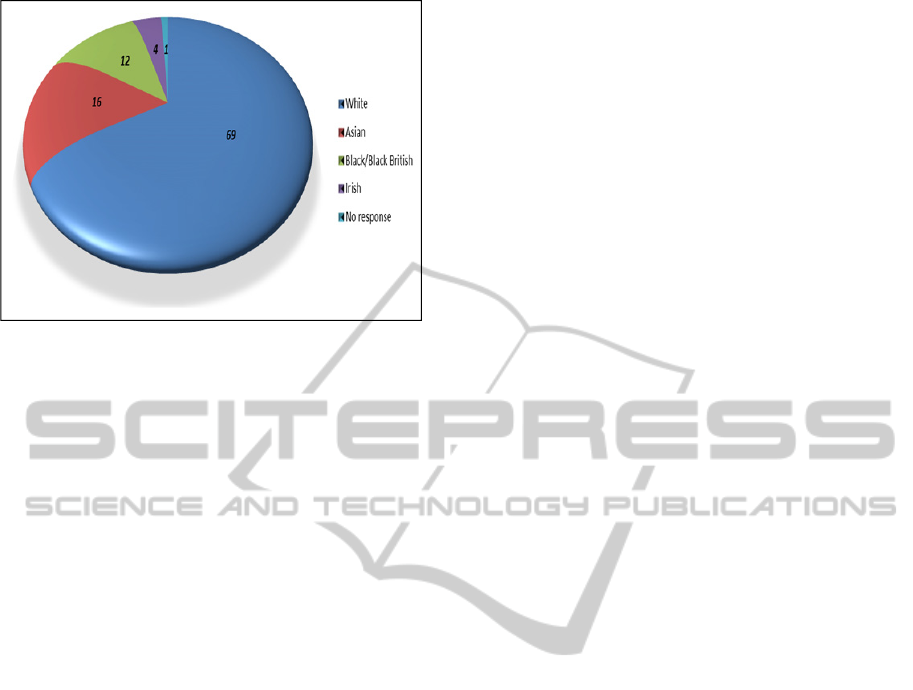
Figure 2: Pie chart comparing the ethnic origins of the
participants in the questionnaire survey.
survey and one participant did not answer the
question about ethnic origin.
75% of the participants had been invited to
attend screening and only four had not done so.
Their reasons for non-attendance were: the
appointment being at an inconvenient time, being
afraid of X-rays, not wanting to get a cancer
diagnosis and being put off by adverse publicity
about over-diagnosis.
78% of the participants thought problems with
communication might be a reason for non-
attendance. They suggested having more
interpreters, providing the information in different
languages, strengthening links with local
communities and improving the communication
skills of professionals.
56% of the participants thought that difficulties
getting transport would affect attendance. Solutions
included having more mobile units and holding
screening at locations convenient for users of public
transport.
11% of the participants thought that embarrassment
might put women off attending screening. They
thought creating links with local communities and
reassuring women that screening is carried out by
female professionals would help.
Anxiety about the procedure or the possibility of
receiving bad news was the most common reason
that participants gave for non-attendance, with
exactly 50% of the participants mentioning anxiety.
Eleven of the participants said that having more
information about the procedure would be useful.
The use of television to educate people about what
happens and providing a helpline where women can
ask for more information were suggested. Two
participants thought the recent bad publicity about
over-diagnosis might make some women reluctant to
attend and three participants thought that some
women might not appreciate the importance of
screening.
It was clear from both the focus group and
questionnaire results that anxiety was not a single
factor but included concerns about the procedure
(including ignorance about what was involved and
concerns that the procedure would be painful) and
anxiety about receiving a cancer diagnosis.
Educating people about the procedure was suggested
as a way to reduce anxiety. It was also suggested
that the service should balance recent negative
publicity about over-diagnosis with positive stories
of how early diagnosis and treatment can enable
cancer to be treated while it is still at an early stage.
The results from the questionnaire and the focus
group informed the discussion that took place in the
final focus group, the purpose of which was to
suggest ways in which the barriers to screening
could be overcome.
Stage Four: Final Focus Group
Five participants took part in the group. They were
all women and their ages ranged from 54-77.
Communication Problems
One of the group suggested having more interpreters
available and another pointed out that people often
have cultural barriers to overcome in addition to
language barriers. Suggestions of how these could
be tackled included promoting screening at women’s
groups and encouraging community elders to
support the program.
It was noted that it is not always obvious if
people have difficulty hearing. Health professionals
should be aware that this might be the case and
check that they have been understood. Several group
members had experienced being unable to
understand the terms used by professionals and
thought it would help if familiar language was used.
Transport Problems
Although providing transport was suggested, this
was thought to be expensive and ensuring that
screening is carried out in locations convenient for
public transport was suggested as a more realistic
solution. It was also thought to be important to offer
appointments at a range of times, including
evenings, to make these convenient for the service
users.
KMIS2013-InternationalConferenceonKnowledgeManagementandInformationSharing
348

Beliefs and Attitudes
Participants thought that creating links with
communities would help women to feel comfortable
about attending screening. Two participants thought
it was important for screening to be carried out by
female professionals and for potential clients to be
made aware of this. It was suggested that women
should be encouraged to ask professionals about
screening so they get accurate information and
reassurance. One participant who had been
successfully treated for breast cancer as a result of
this being picked up at screening thought women
who had similar experiences would be good at
persuading others of the importance of screening.
5 LIMITATIONS
A local sample of participants was used in the study
and it is not clear how far the results can be
generalised to other areas of the country. Although
care was taken to ensure that the participants were
representative of the local population of older adults,
there are ways in which people who attend Age UK
meetings may differ from those who fail to attend
breast screening. Those who attend the meetings are
able to arrange transport to do so and it can be
assumed that they will also be able to arrange
transport to attend screening. People attending
activities organised by Age UK are also interested in
their health and in socialising. These characteristics
may not be shared by people who fail to attend
screening. It is clear that ethnicity and family
support are factors affecting attendance. Women
who do not speak English, rarely socialise outside
their community and have family responsibilities
that make it difficult for them to attend appointments
may also be unlikely to be involved with the type of
activities offered by Age UK.
6 RECOMMENDATIONS FOR
PRACTICE
It is clear from the results that the barriers to breast
screening attendance are varied and include social
influences like family support and psychological
factors such as anxiety. It is likely that women who
do not attend screening face a combination of
barriers. Contemporary approaches like knowledge
management offer a means by which intelligence
about individuals can be shared between primary
care and the breast screening service, in order to
identify women who may face barriers to
attendance. Targeted interventions, such as
providing information in their own language can
then be deployed.
The main barriers to breast screening attendance
that were identified during the study included those
associated with communication. Problems getting
transport to appointments was also a barrier but the
most common reason for non-attendance was
thought to be anxiety. This ranged from concern that
the procedure would be painful to being afraid of
receiving bad news. In common with a recent local
study (Coventry Link, 2012), many participants
thought that there was a lack of knowledge about
screening and that educating people about its
importance and what is involved would increase
attendance rates. The results of the current study
suggest that attendance could be improved by:
Providing invitations and information about
screening in simple language and in
different languages where appropriate
Having interpreters and community
representatives available to support women
at appointments
Ensuring screening is carried out at
locations that are easy for women to get to
by public transport
Creating links with local communities,
educating people about screening and
encouraging them to talk to professionals
about their concerns
Publicising stories of women who have
been successfully treated for breast cancer
as a result of being diagnosed early
It will be important to evaluate the effect of these
initiatives on attendance rates.
7 CONCLUSIONS
Baskaran (2008) identified individual characteristics,
such as age, ethnicity and socio-economic status that
were associated with breast screening non-
attendance. This study demonstrated that such
characteristics could be used to predict non-
attendance and provide health professionals with the
opportunity to carry out interventions, such as
ensuring information is provided in a language that
will be understood by potential participants.
The current study identified additional barriers to
attendance that were concerned with
UsingKnowledgeManagementToolsandTechniquestoIncreasetheRateofAttendanceatBreastScreening
349

communication, transport, beliefs and attitudes. The
results were similar to another local study (Coventry
Link 2012) which considered barriers faced by
people from ethnic minority backgrounds when
trying to access screening services. Both studies
identified communication problems, transport
problems and attitudes as barriers to attendance. The
recommendations that were formed from the results
of the current study provide suggestions of
interventions that would be expected to increase
screening attendance rates.
Future work should include evaluating the effect
of the suggested interventions on the attendance rate.
Research should also be carried out in other areas of
the country to see how far the results can be
generalised.
REFERENCES
Age UK (2013) [online] Available from
<http://www.ageuk.org.uk/> [3rd March 2013].
Aronson, J. (1994) “A pragmatic view of thematic
analysis.” The Qualitative Report 2 (1) [online]
Available from <http://www.nova.edu/ssss/QR
/Backissues/QR2-1/aronson.html> [28 March 2010].
Atri, J., Falshaw, M., Gregg, R., Robson, J. Omar, R.Z.
and Dixon, S. (1997) “Improving uptake of breast
screening in multiethnic populations in a randomised
controlled trial using practice reception staff to contact
non-attenders.” BMJ 315, 1356-9.
Bali, R.K., Wickramasinghe, N. and Lehaney, B. (2009)
Knowledge Management Primer, Routledge: USA.
Bankhead, C., Austoker, J., Sharp, D., Peters, T.,
Richards, S.H., Hobbs, R., Brown, J., Wilson, S.,
Roberts, L., Redman., Tydeman, C., Formby, J. (2001)
“ A practice based randomised controlled trial of two
simple interventions aimed to increase uptake of breast
cancer screening.” Journal of Medical Screening 8, (2)
91-98.
Baskaran, V. (2008) Implementation of a breast cancer
screening prediction algorithm: a knowledge
management approach, PhD thesis. Coventry
University.
Bekker, H., Morrison, L., and Marteau, T.M. (1999)
“Breast Screening: GP’s beliefs, attitudes and
practices.” New York: Basic Books.
Cancer Research UK (2005) CancerStats Incidence-UK
[online] Available from www.cancerresearchuk
.org/aboutcancer/statistics/statsmisc/pdfs/cancerstats_I
ncidence_apr05.pdf, [August 2005].
Cassandra, E. S. (2006) “Breast cancer screening: cultural
beliefs and diverse populations.” Health and social
work 31, (1) 36-43.
Coventry Link (2012) Accessing Cancer Screening
Services for People from ethnic minority communities
in Coventry, Coventry Link.
Day, N.E., Williams, D.D.R., Khaw, K.T. (1989) “Breast
cancer screening programmes: the development of a
monitoring and evaluation system.” British Journal of
Cancer 59, 954-8.
Fox, S., Murata, P. and Stein, J. (1991) “The impact of
physician compliance on screening mammography for
older women.” Arch. Internal Medicine 151, 50-56.
Hoppe, M. J., Wells, E. A., Morrison, D. M., Gilmore, M.
R., and Wilsdon, A. (1995) “Using Focus Groups to
Discuss Sensitive Topics With Children.” Evaluation
Review 19 (1), 102-14.
Jepson, r., Clegg, A., Forbes, C., Lewis, R., Sowden, A.
and Kleijnen, J. (2000) “The determinants of screening
uptake and interventions for increasing uptake: a
systematic review.” Health Technology Assess 4, (14)
Katz, S.J., Zemencuk, J.K., Hofer, T.P. (2000) “Breast
cancer screening in the United States and Canada,
1994: Socioeconomic Gradients Persist.” American
Journal of Public Health, 90, (5) 799-803.
Katz, S.J., Zemencuk, J.K., Hofer, T.P. (2000) “Breast
cancer screening in the United States and Canada,
1994: Socioeconomic Gradients Persist.” American
Journal of Public Health, 90, (5) 799-803.
Lankshear, A. J. (1993) “The Use of Focus Groups in a
Study of Attitudes to Student Nurse Assessment.”
Journal of Advanced Nursing 18, 1986-89.
Sin, J.P. and Leger, A.S. (1999) “Interventions to increase
breast screening uptake, do they make any
difference?” Journal of Medical Screening 6, (1) 170-
181.
Townsend P, Phillimore P, Beattie A. (1988) Health and
Deprivation: Inequality and the North Croom Helm:
London.
KMIS2013-InternationalConferenceonKnowledgeManagementandInformationSharing
350
