
Designing Collaboratively Crisis Scenarios for Serious Games
Nour El Mawas and Jean-pierre Cahier
ICD/Tech-CICO, Université de Technologie de Troyes, Troyes, France
Keywords: Emergency Crisis Management, Serious Games, Crisis Training, Discussion Forum, Participative Design.
Abstract: Numerous studies have explored the using of serious games as methodological tools for improving crisis
management. Training in the Emergency Medical Services (EMS) field requires a combination of
approaches and techniques to acquire medical skills with unanticipated events and to develop the capability
to cooperate and coordinate individual emergency activities towards a collective effort. Crisis management
is a special type of collaborative situations that why we propose a participative and knowledge-intensive
serious game, as a collaborative e-learning tool for training (EMS). We believe that emergencies doctors
learn best through real life experiences and serious games have the ability to simulate situations that are
impossible to generate in a real-life exercise due to high cost, safety and complex environment related to
situations. However, our approach takes into account the presence of different actors in crisis situation like
police and firefighters and the high volume of (medical as well as non-medical) expert knowledge.
1 INTRODUCTION
Today, the term serious game is becoming more and
more popular. There are many definitions of the
concept. According to (Sawyer, 2007), serious
games are “any meaningful use of computerized
game/game industry resources whose chief mission
is not entertainment”. According to (Corti, 2006)
game-based learning/serious games “is all about
leveraging the power of computer games to captivate
and engage end-users for a specific purpose, such as
to develop new knowledge and skills”. Nowadays,
serious games are in many knowledge fields,
including defence, crisis management, learning,
health, and other areas. According to (Navarro et al.,
2010), serious game is an emerging technology for
specialized training, taking advantage of 3D games
in order to improve the realistic experience of users.
Constructivism theory (Tobias et al., 2009)
argues that humans generate knowledge and learning
from an interaction between their experiences and
their ideas. Serious games offer a constructivist way
of learning where the people gain knowledge and
experience while interacting with the game. It’s
difficult to predict how a person will react in an
emergency crisis due to many factors involved in
decision making.
Decision making in highly dynamic, complex
situations is difficult. The literature on complex
problem solving and natural decision making
provides interesting insights into human error
tendencies and has pointed to numerous traps and
pitfalls we are likely to stumble into (Dörner et al.,
1994); (Frensch et al., 1995); (Dörner, 1996); (Klein,
1997); (Strohschneider et al., 1999). If we translate
“complex problem solving” into “management of
crises and emergencies” (Danielsson et al., 1997), it
has become quite obvious that training and
education are mandatory. After all, emergencies and
crises are among those situations where deficient
problem solving is dangerous and can become
extremely costly on different dimensions. The
widespread adoption of computer games for
entertainment purposes, the continuous decrease of
hardware cost and the success in military
simulations made gaming technologies attractive to
some “serious” industries such as medicine,
architecture, education, city planning, and
government applications (Smith, 2007). Through the
use of serious games, doctors and nurses can gain
the benefits of learning and how to cope up with an
emergency situation without being exposed to the
dangers of real world emergencies. In this way, it’s
possible to observe how they adapt to new situations
and apply the knowledge they have gained to come
up with solutions to new problems.
Emergency crisis situations are complex
collaborative situations, personnel from different
domains (doctors, nurses, police, and firefighters)
381
El Mawas N. and Cahier J..
Designing Collaboratively Crisis Scenarios for Serious Games.
DOI: 10.5220/0004548303810388
In Proceedings of the International Conference on Knowledge Discovery and Information Retrieval and the International Conference on Knowledge
Management and Information Sharing (KMIS-2013), pages 381-388
ISBN: 978-989-8565-75-4
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

often must work together. The emergency
management is based on “staff work” that focuses
on planning, coordinating, and monitoring operative
procedures (Helmreich et al., 1999); (Helmreich et
al., 1993); (Orasanu et al., 1996). Communication
and coordination is very important between
emergency management teams (Schaafstal et al.,
2001). Information presented to the participants of
the collaborative staff has to be simple enough to
support cooperation between people from different
organizations but at the same time be rich enough
for an individual from a specific organization to
facilitate his decision making. The aim of training is
not to teach teams new task knowledge or skills.
Instead teams need strategies that enable them to
better manage the increases in coordination and
information overhead that result from increases in
workload and stress (Entin et al., 1999).
Our goal is an attempt to co-develop a learning
environment that equips persons working in
emergency medical services with the knowledge and
skills necessary to act as members of such a staff
and deal with rare crises and emergencies.
The rest of this paper is organized as follows.
From some readings, the section II defines features
of a crisis management. The section III proposes a
preliminary overview on the use of serious game in
emergency health care. The section IV details our
scientific positioning and defines our approach of
serious games "participative and intensive in
knowledge" and our technical architecture, with our
developed ARGILE forum intended to illustrate the
key concepts. The section V summarizes the
conclusions of this paper and presents its
perspectives.
2 FEATURES OF A CRISIS
MANAGEMENT
Among the five Activities inventoried by Johnson
(Johnson, 2000) for disasters and emergency
management – planning, mitigation, preparedness,
response and recovery – serious game can be
principally useful in the preparedness Activity.
Crisis management is complex and we do not aim at
its complete characterization, but rather outline
general issues for designing serious games useful for
preparedness. Let’s use a simplified example to help
us in this task. The worked example is real; it’s the
result of interviews we conducted with trainers at the
mobile Emergency Medical Service (EMS) in the
(middle town -150 00 inhabitants) hospital
participating in our project.
During a winter Sunday, a tank truck
transporting potentially toxic material has an
accident with a van (see figure 1) on a national
highway 25km from the EMS basis. If this toxic
material gets in contact with air, it causes a major air
contamination. The situation requires the
coordinated intervention of multiple units:
firefighters trying to avoid contamination; medical
units taking cares of victims and police trying to
avoid traffic problems. So, we are dealing with a
complex problem, and we have different solutions
with associated costs and risks.
Figure 1: Crash between a tank truck and a van (image
proposed to the learner in the serious game).
The interference between predictable and
unpredictable events, the impossibility to only apply
predefined procedures, characterizes such a crisis. In
our example, accidents involving vehicles
transporting toxic material are a well-known
problem for which protocols of action are defined.
However, nobody can predict when/where this will
happen and the context, like type of transported
material, weather conditions, victims’ number or
population in the area. Toxic risk can happen in
combination with other factors (meteorology,
organizational problems…). During a crisis, the
main problem is divided into many sub-problems,
e.g. securing the area, taking care of the victims,
putting population in safe conditions, avoiding
contamination, contacting the main hospital to
accommodate victims and so on. Once the main
problem is divided into sub-problems, action has to
be planned. Each unit might define plans for sub-
problem they have to handle, but with the need to
coordinate the effort. Plans have to conform to
approved protocols of action. Action leading to an
optimal result locally is not always leading to the
intended global result. For example, "divert the
traffic in one direction might reduce congestion in
KMIS2013-InternationalConferenceonKnowledgeManagementandInformationSharing
382

one area, but create problems to emergency vehicles
parked in another road" says a doctor at the EMS of
the hospital. Members in a crisis management team
need to communicate to coordinate their action. For
example, if firefighters are the first to be present in
the area, when emergency doctor arrives, he must
contact directly the commander of rescue operation
(CRO) to know more about the accident. Also, the
time is very important for decision making in our
example: the tank truck can start spilling out toxic
material and contaminate the air if the emergency
team is not able to act quickly; or an injured
situation may become worse if he doesn’t receive
first aid quickly. Crises are related to specific social
and physical contexts that influence their
management. If our example is happening in a
highly populated area with schools or university
nearby, we are submitted to different requirements
than if the accident happens in an isolated area. As
we can see crisis management is a task that can rise
in complexity very quickly. Emergencies are made
up of both predictable and unpredictable elements.
Crisis management works exactly anticipating the
former in order to minimize the damage (Palen et al.,
2007). One of the ways to anticipate unpredictable
events is building predictive models or scenarios and
uses them for training. Managing unexpected
elements requires instead to learn not only how to
behave during the crisis, but also the importance of
passing the right information, in the right amount, at
the right time, from the right place, to the right
person (Sagun et al., 2008).
3 RELATED WORK
In this section, we consider previous work
concerning serious games for medical emergency
domain. Virtual training environments have been
developed for traditional emergency services
(Jenvald et al., 2004) (Metello et al., 2008), for
triage training (Dumay, 1995) (Jarvis et al., 2009)
and many industry specific applications (Mallett et
al., 2007).
A few knowledge-based systems have been
proposed for information and resources management
in crises: for example, R-CAST-MED (Zhu et al.,
2007) is a system that uses an intelligent agent
architecture built on Recognition-Primed Decision-
making (RPD) and Shared Mental Models (SMMs)
to manage information sharing among
geographically-dispersed teams to improve
collaboration and coordination in mass casualty
incidents, and iRevive (Gaynor et al., 2005) is a
robust pre-hospital patient care application that
includes wireless sensors to handle coordination
among ambulance teams, local site management and
a distributed collection of hospitals.
Other knowledge-based systems focus on triage
in EMS: for example, Mobile Emergency Triage
MET (Michalowski et al., 2003) is an m-health
application that supports emergency triage of
various types of acute pain at the point of care. The
system is designed for use in the Emergency
Department (ED) of a hospital and to aid physicians
in disposition decisions. While Automated Triage
Management ATM is a decision support model that
assists healthcare practitioners to find patients’ chief
complaints (Guterman et al., 1993). (Gertner et al.,
1998) proposed instead the TraumaTIQ knowledge-
based system to support physicians in trauma
management. Their approach is based on evaluating
rather than recommending plans: the system aims at
recognizing what plan the physician is following,
evaluating it and providing a user-focused critique to
the course of actions chosen by the physician if
possible problems have been detected. Comments
presented by the system are sorted by order of
importance and topic.
BioHazard/Hot Zone (Wilen-Daugenti, 2007)
was generally created to teach college students
introductory college biology and environmental
science. It has evolved into a game to help
emergency first responders deal with toxic spills in
public locations. Players race against the clock to
save civilians. The game involves scanning and
assessing the situation quickly, teaming; and
understanding chemicals, viruses, and symptoms.
Individuals also learn how unpredictable behaviors
can be in high-stress emergency situations. The aim
of the game is to help emergency first responders
prepare for potentially catastrophic situations.
Play2Train (Boulos et al., 2009) is a virtual
training space in Second Life designed to support
Strategic National Stockpile (SNS), Simple Triage
Rapid Transportation (START), Risk
Communication and Incident Command System
(ICS) Training. Play2Train provides opportunities
for training through interactive role playing and is
the foundation for the emergency preparedness
educational machinima. It helps first responders,
first receivers and other health care professionals
prepare for disasters. According to Dr Ramloll,
Play2Train could eventually replace physical
dioramas, commonly used by emergency services
personnel when they train for disasters, in a way that
holds the interest of participants longer than the
current training approaches.
DesigningCollaborativelyCrisisScenariosforSeriousGames
383

Another interactive training game, called Zero Hour
(Hom, 2009) was developed through a collaboration
between the Chicago Health Department, the U.S.
Centers for Disease Control and Prevention and the
University of Illinois. It simulates a mass anthrax
attack, requiring participants to make critical
operational decisions, respond to questions from
simulated departments with competing needs, and
field simulated phone calls with requests for added
equipment. The game is designed to mirror real-
world complexity.
Texas A&M University-Corpus Christi develops
Pulse!! (McDonald, 2011) which is an important
serious game in the area of healthcare. “Pulse!!” is
used to train medical professionals on how to handle
health emergency situations. The main “purpose” of
this game is not to broadcast a message but to
improve the player’s cognitive and/or motor skills
for precise tasks or applications. EMSAVE,
"Emergency Medical Services for the disAbled"
(Vidani, 2010) Virtual Environment is a virtual
reality system for training in emergency medical
procedures concerning disabled persons. It allows
users to experience emergency situations involving
disabled persons. The simulations take place in a
freely explorable virtual environment. The user can
choose what actions to perform among a set of
possibilities that depends on the difficulty level.
Relevant effects of user's actions on the patient (e.g.,
change in complexion) are simulated by the system.
(Sharma et al., 2012) proposed a collaborative
virtual environment to study aircraft evacuation for
training and education with two types of agents: user
controlled agents and computer controlled agents.
The idea is to have multiple users enter the virtual
aircraft environment as avatars. These avatars would
be able to interact with each other and make
decisions such as following the directions by the
leader and avoid bumping into other agents. There
are also computer controlled agent, present in the
environment which are programmed and act as
obstacles to the user controlled agents.
In our work, we refer to serious games for
training emergency medical services for many
reasons. First of all, the use of serious game ensures
in the preparedness phase a more extensive control
in complex and knowledge-intensive situations. It is
difficult to control variable like wind direction, rain,
snow, the position of large good vehicles and the
consecutive occurrence of multiple events in real life
simulation. The control and the combination of these
different variables are very important to generate
different scenarios for pedagogical aims. Serious
gaming environments can be simultaneously
complex and controllable and computerized
standardization makes serious gaming experiments
also repeatable. Control and repetition offer great
opportunities for training. In addition, serious games
have the ability to simulate situations that are
impossible to generate in a real-life exercise due to
high cost, safety and complex environment related to
situations (Corti, 2006) (Squire et al., 2003).
Although virtual reality isn’t real, fire shown in
virtual environments can have more resemblance
with real fire or smoke than the means used to
imitate fire and smoke during many real-live
exercises (Jenvald et al., 2004).
In our work, we are interested in serious games
for training experts in EMS. This domain is based on
complex knowledge and interdisciplinarity that is
why experts must be the game designers. In
addition, scenarios in this context depend on many
factors (like weather, victims type, hour where the
accident happens ...) and if we use a classic
approach of serious game, we could treat only some
scenarios due to the high cost. We need a new
approch wich covers a large number of scenrios and
which allows to experts to add easily a new scene,
item and knowledge in the game whithout the need
of IT specialists.
4 A PARTICIPATIVE
ARCHITECTURE ADRESSING
CRISIS MANAGEMENT E-
TRAINING CONSTRAINTS
In this section, we justify and present our detailed
approaches of the co-design system and the learners’
forum before explaining our technical infrastructure.
4.1 Co-designing the Serious Game
Elements with the A.R.G.I.L.E
System: Why and How?
First we propose in the A.R.G.I.L.E system
(Architecture for Representations, Games,
Interactions, and Learning among Experts) a
participative approach to associate EMS experts into
an efficient writing of crisis scenes scenario.
Developing Serious Game sequences for numerous
cases (including cases at a very low probability) is
necessary, but very expansive with traditional game
editors (El Mawas et al., 2012). It is easy with
traditional methods to formalize well established
prescribed procedures, but a characteristic of a crisis
is precisely that prescribed procedures often are not
KMIS2013-InternationalConferenceonKnowledgeManagementandInformationSharing
384
sufficient, and have to be completed by experience.
To involve experienced EMS people in the scenario
design is a good means to capitalize Knowledge and
transmit it to novices. Actions that are almost easy
for experimented emergency doctors might be
extremely challenging for newcomers, both
technically and in terms of emotional response
(especially if the crisis is rarely to happen). That’s
why experts have to be active in the co-design
process we propose.
Figure 2: Participative architecture.
Our challenge is to transfer the accumulated
knowledge flowing from concrete experiences, well-
documented and discussed by trainers in EMS (in
other words, reliable data), to a training model in
which actors will be actively engaged. These
knowledge are neither stabilized nor unanimous, but
on the contrary dynamics and in continuous
evolution. The actor does not make his decisions
according to pre-established recipes. He mobilizes
all his intelligence, to proceed by trial and error, to
communicate with his peers and to discover
continuously the suitable solutions in complex
situations proposed to him.
The innovation in our approach is the co-
conception of rules and certain objects of the game
by the trainers of the domain. We make the
hypothesis, that rules, knowledge and objects of the
game can be written, commented, discussed easily
and modified by trainers in EMS, with the help of
the researchers (cf. Figures 2,3), but without to
delegate the design to IT specialists and specialized
software editors. We also wont to verify the
hypothesis of a better quality of the knowledge for
crisis management “on the field”, if co-designed by
this way.
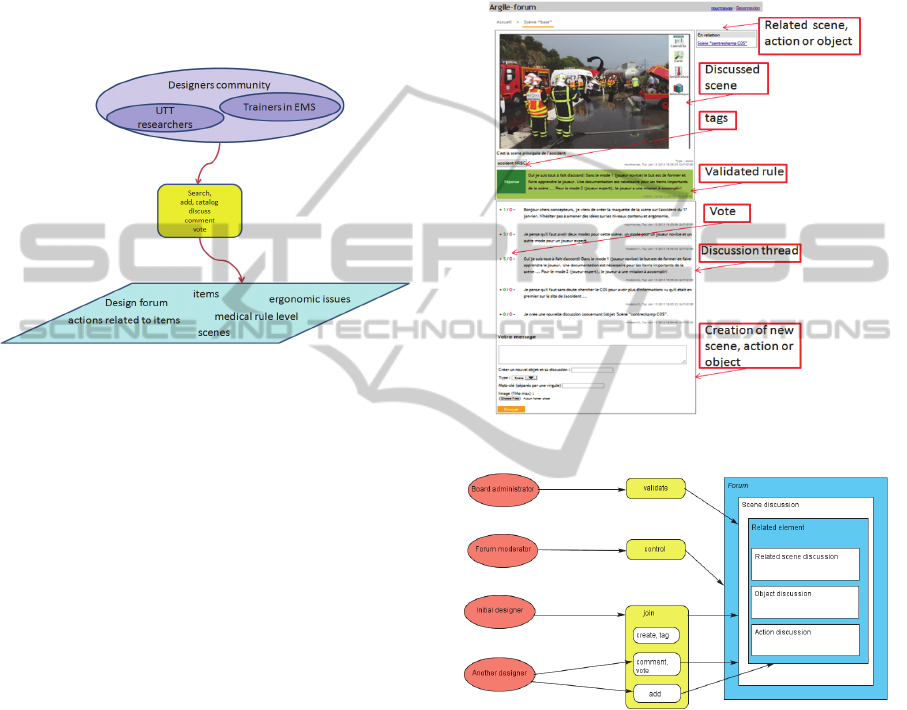
A SeeMe diagram (Herrmann et al., 2000) is
used for the roles, the activities and the entities
presentation (see figure 4). We distinguish several
roles in this model: the initial designer, the other
designers, the board administrator and the forum
moderator. To note that designers have on the forum
a discussion thread for every scene object or action
related to an item in the scene. Every time that an
initial designer creates a scene/object/action
discussion, designers are notified to participate in
the discussion.
Figure 3: Discussion forum.
Figure 4: Model of designers’ activity (SeeMe diagram).
The proposed architecture offers to the designers a
Web-based working system which articulates:
- A specification system directed to teamwork
susceptible to associate skills of experimented
emergency doctors and nurses
- A navigation system in the game objects (this
point is particularly crucial in the applications of
knowledge-intensive in game, which contain
numerous objects and rules),
- A discussion forum type: crisis management
games rules depend on places, seasons, physical
and social context and many other factors. That
is why for a designer who builds objects and
DesigningCollaborativelyCrisisScenariosforSeriousGames
385

rules of a scene, it is important to have a design
forum for the discussion between peers.
All designers are invited to join the “design forum”
to discuss new scenes, actions and objects before
implementing them in the game. Figure 3 shows an
example of a designer who creates a scene
discussion (“Crash between a van and a truck”),
uploads the correspondent mock-up, tags the created
scene (accident NRBC: Nuclear, Radiological,
Biological or Chemical). He invites other designers
to discuss different elements, add an action/ object
related to this scene or add a sub-scene that shows
various cameras angles and may complicate or
change the situation. Another designer comments
that adding a scene where we can see the CRO is
important; due to his active role in crisis situation.
All designers can vote for any comment/rule. The
board administrator validates a rule after discussion
and it will appear on green background. In crisis
situations, knowledge is in continuous evolution, so
rules that are validated now may be invalidated later.
Through the forum, we can have successive versions
of a rule and traces of rules amelioration.
Hospital emergency trainers involved in the
project don’t prefer that the won/lost points system
appears to learners in the game. “The won/lost
points system is important for us, as trainers, at the
debriefing phase. We prefer that it will be hidden to
learners because it will influence on them” says a
doctor at the hospital EMS. We are in the context of
interactive pedagogy, so trainer watches
players/learners where they are playing and can add
in real time new items or messages or sounds to
complex the situation and to teach specific
knowledge.
4.2 Knowledge in EMS
In EMS, knowledge is in procedural or declarative
forms. Anderson (Anderson, 1993) underlines that
knowledge starts with declarative actions, the
conscious and control; and this control paves the
way for procedural processes. Moreover, he argues
that declarative knowledge forms the basis of
knowledge transfers. Procedural knowledge is about
how to think (Heyworth, 1999). It is linked with the
performance change in knowledge, skills and tasks
(LeFevre et al., 2006). It is the knowledge that
explains how to perform an action within the
framework of clear procedures.
In other words, Declarative knowledge is
knowledge about something and procedural
knowledge is knowledge of how to do something.
For example, declarative knowledge enables a
doctor in EMS to describe the rule "victims’
evacuation" in crisis situation. Procedural
knowledge enables him to apply the evacuation in
real crisis. We use the expression “advanced doctor”
for a doctor with minimum 5 years of experience in
emergency service and “beginner doctor” for a
doctor with unless than 5 years of experience.
The aim of the scene presented in figure 1 is to
train doctors how to deal in rare crises like NRBC
accident. We believe that our training tool must not
contain the same knowledge for advanced and
beginner doctors. That’s why we have the game with
2 modes (see figure 5) depending on knowledge
level of player. In mode 1, players are beginner
doctors in EMS so the knowledge implemented in
the game are declarative knowledge. The player can
click on any scene item to have documentation about
it. For example he can click on the CRO to know
who he is, what his background is and what his role
is in an accident.
In mode 2, players are advanced doctors so they
have already the declarative knowledge through
their experiences. The knowledge implemented in
the game is procedural knowledge. The number of
clickable items in mode 2 is reduced in comparison
to mode 1. For the same item CRO, player in mode 2
will hear a voicemail message about the situation
and then a question appears. He must complete
missing fields about the 5 important topics in the
CRO message. In general, we use pedagogical tools
in mode 2 like multiple choices or Yes/No quiz,
action on an item…
Figure 5: 2 Modes of the game depending on doctor’s
level.
5 CONCLUSIONS AND
PERSPECTIVES
In this paper, we proposed for Crisis Management
KMIS2013-InternationalConferenceonKnowledgeManagementandInformationSharing
386

(in the preparedness stage) a new approach of
participative and knowledge-intensive serious games
where scenarios are designed collaboratively. We
proposed, with the A.R.G.I.L.E architecture
functional and technical solution elements, by
indicating on some examples why this solution is the
most suitable to these games service. This reflection
comes along with a work plan for the architecture
implementation which allows us to validate
gradually certain underlying hypotheses in our
proposal.
Our first objective is to validate the practicability
of the co-design approach of the participative and
knowledge-intensive serious game. We would like to
verify that the proposed co-design method allows a
better precision for described knowledge elements,
especially for common ground EMS non-procedural
crisis management “on the field” knowledge. We
presently are already implying EMS-trainers as co-
designers, so they define scenes, create and modify
them continuously, according to the proposed rapid
prototyping and co-building method.
Now, we are developing, in our discussion
forum, a space for learners to discuss
scene/object/actions once they play. We think that
these discussions will thread as resource to play
better and to exchange hints and tips. In an
experiment envisaged in September 2013, we are
interested in the player's learning and his/her
progress through the discussion forum and not only
through the game itself. For that purpose, the
learning will be estimated by placing the players in
two configurations, without and with the discussion
forum, and the results will be compared to evaluate
our hypothesis: by using the discussion forum, we
have a better learning.
REFERENCES
Sawyer, B., (2007). The "Serious Games" Landscape.
Presented at the Instructional & Research Technology
Symposium for Arts, Humanities and Social Sciences,
Camden, USA.
Corti, K., (2006). Games-based Learning; a serious
business application. PIXELearning Limited.
Navarro A., Pradilla J., Madrinan P., Univ Icesi C., (2010)
Work in progress serious 3d game for mobile
networks planning, In FIE 2010 Frontiers in
Education Conference, 2010 IEEE.
S. Tobias, T. M. Duffy, Constructivist instruction: Success
or failure? New York: Taylor & Francis, 2009.
Dörner, D. Schaub, H., (1994). Errors in planning and
decision-making and the nature of human information
processing. Applied Psychology: An International
Review, 43, 433-453.
Frensch, P., & Funke, J. (Eds.) (1995). Complex problem
solving: The European perspective. Hillsdale, NJ:
Lawrence Erlbaum.
Dörner, D., (1996). The logic of failure. New York: Holt.
Klein, G., (1997). The current status of the naturalistic
decision-making framework. In R. Flin, E. Salas,M.
Strub, & L. Martin (Eds.), Decision-making under
stress: Emerging themes and applications (pp. 11-28).
Aldershot, UK: Ashgate.
Strohschneider, S., & Güss, D., (1999). The fate of the
Moros: A cross-cultural exploration in strategies in
complex and dynamic decision-making. International
Journal of Psychology, 34, 235-252.
Danielsson,M. & Ohlsson, K., (1997).Models of decision-
making in emergencymanagement. InD. Harris (Ed.),
Engineering psychology and cognitive ergonomics:
Vol. 2. Job design and product design (pp. 39-45).
Aldershot, UK: Ashgate.
Smith, R. (2007) Game Impact Theory: Five Forces That
Are Driving the Adoption of Game Technologies
within Multiple Established Industries. Games and
Society Yearbook.
Helmreich, R. L., Merritt, A. C. & Wilhelm, J. A., (1999)
The evolution of crew resource management training
in commercial aviation. International Journal of
Aviation Psychology, 9, 19-32.
Helmreich, R. L., & Foushee, H. C., (1993) Why crew
resource management? Empirical and theoretical bases
of human factors training in aviation. In E. L. Wiener,
B. G. Kanki, & R. L. Helmreich (Eds.), Cockpit
resource management (pp. 3-45). San Diego, CA:
Academic Press.
Orasanu, J. M. & Backer, P., (1996). Stress and military
performance. In J. E. Driskell & E. Salas (Eds), Stress
and human performance. Series in applied psychology
(pp. 89-125). Hillsdale, NJ: Lawrence Erlbaum.
Schaafstal, A.M., Johnston, J. H., & Oser, R. L. (2001).
Training teams for emergency management.
Computers in Human Behavior, 17, 615-626.
Entin, E. E. & Serfaty, D., (1999). Adaptive team
coordination. Human Factors, 41, 312-325.
Johnson R., GIS technology for disasters and emergency,
ESRI White Paper, May 2000.
Palen, L. and S. B. Liu, (2007) Citizen communications in
crisis: anticipating a future of ict-supported public
participation. ACM Conference on Human Factors in
Computing Systems CHI 2007 Proceedings:
Emergency Action 28 April-3 May 2007, San Jose,
California: 728-736.
Sagun, A., Bouchlaghem, D., and Anumba, J.C. (2008) A
Scenario-based Study on Information Flow and
Collaboration Patterns in Disaster Management,
Disasters (33:2), August 2008, pp. 214-238.
Jenvald, J. and Morin, M., (2004) Simulation-Supported
Live Training for Emergency Response in Hazardous
Environments, Simulation Gaming 35, 3, 363-377.
Metello, M. G., Casanova, M. A. and Carvalho, M. T. M.,
(2008) Using Serious Game Techniques to Simulate
Emergency Situations, Proceedings of the X Brazilian
DesigningCollaborativelyCrisisScenariosforSeriousGames
387

Symposium on GeoInformatics, Rio de Janeiro, Brazil.
Dumay, A. C. M., (1995) Triage simulation in a virtual
environment. in: Interactive Technology and the New
Paradigm for Healthcare. Satava, R. M., Morgan, K.,
Sieburg, H. B., Mattheus, R. andChristensen, J. P.
Amsterdam, IOS Press.
Jarvis, S. and de Freitas, S., (2009) Evaluation of an
Immersive Learning Programme to Support
TriageTraining, Proceedings of the 2009 Conference
in Games and Virtual Worlds for Serious
Applications,Coventry, UK, IEEE Computer Society.
Mallett, L. and Unger, R., (2007) Virtual reality in mine
training, Society for Mining, Metallurgy, and
Exploration, Inc 2, 1-4.
Zhu, S., Abraham, J., Paul, S. A., Reddy, M., Yen, J.,
Pfaff, M., Deflitch, C., (2007) R-CAST-MED:
applying intelligent agents to support emergency
medical decision-making teams. In: Proceedings of the
11th Conference on Artificial intelligence in Medicine
(AIME 2007). LNCS 4594, July 2007, Springer-
Verlag, Berlin, pp. 24–33.
Gaynor, M., Seltzer, M., Moulton, S., Freedman, J., (2005)
A dynamic, data-driven, decision support system for
emergency medical services. In: Proceedings of the
International Conference on Computational Science,
LNCS 3515, May 2005, Springer-Verlag, Berlin, pp.
703–711.
Michalowski, W., Rubin, S., Slowinski, R.,Wilk, S.,
(2003) Mobile clinical support system for pediatric
emergencies. Decis. Support Syst. 36(2), 161–176.
Guterman, J. J., Mankovich, N. J., Hiller, J., (1993)
Assessing the effectiveness of a computer-based
decision support system for emergency department
triage. In: Proceedings of the 15th Annual
International Conference of the IEEE Engineering in
Medicine and Biology Society, 1993, IEEE Press,
Hong Kong, pp.592–593.
Gertner, A. S., Webber, B. L., (1998) TraumaTIQ: online
decision support for trauma management. IEEE Intell.
Syst. 13(1), 32–39.
Wilen-Daugenti Tracey: “The 21st Century Learning
Environment: Next-generation Strategies for Higher
Education,” Cisco IBSG, November 2007.
Boulos M., Ramloll R., Jones R. and Toth-Cohen S.,
(2009) Web 3D for Public, Environmental and
Occupational Health: Early Examples from Second
Life® , International Journal of Environmental
Research and Public Health, ISSN 1660-4601.
Hom K., (2009). Video Game Gives First Responders
Advance Look at Emergencies, the Washington Post.
McDonald Claudia L. (2011) Pulse!! Technical Report
Fifth Award: Pulse!! The Virtual Clinical Learning
Lab, August 2011: http://www.dtic.mil/cgi-
bin/GetTRDoc?AD=ADA549718.
Vidani A., Chittaro L., Carchietti E., (March 2010)
Assessing nurses’ acceptance of a serious game for
emergency medical services. pp 101–108.
Sharma S., Otunba S.: Collaborative virtual environment
to study aircraft evacuation for training and education.
In: Proceedings of CTS 2012: 569-574.
Squire, K. & Jenkins, H., (2003) Harnessing the power of
games in education. Insight, 3(1), 5-33.
EL Mawas, Nour; Cahier, Jean-Pierre; Bénel, Aurélien,
(2012) Serious games for expertise training: Rules in
questions, Proceedings of 17th International
Conference on Computer Games (CGAMES),
Louisville, KY.
Herrmann, Th., Hoffmann, M., Loser, K.-U., Moysich, K.,
(2000): Semistructured models are surprisingly useful
for user-centered design. In: Dieng, R.; Giboin, A.,
Karsenty, L., De Michelis, G. (Hrsg.): Designing
cooperative systems. Amsterdam: IOC press. pp 159 -
174.
Anderson, J. R., (1993). Rules of the mind, Hillsdale, NJ:
Lawrence Erlbaum Associates Inc.
Heyworth, R. M., (1999). Procedural and conceptual
knowledge of expert and novice students for the
solving of a basic problem in chemistry, International
Journal of Science Education, 21(2), 195-211.
LeFevre, J. A., Smith-Chant, B. L., Fast, L., Skwarchuk,
S. L., Sargla, E., Arnup, J. S., Penner-Wilger,
M.,Binsanz, J and Kamawar, D., (2006). What counts
as knowing? The development of conceptual and
procedural knowledge of counting from kindergarten
through Grade 2, Journal of Experimental Child
Psychology, 93(4), 285-303.
KMIS2013-InternationalConferenceonKnowledgeManagementandInformationSharing
388
