
Development and Population of an Elaborate Formal Ontology for
Clinical Practice Knowledge Representation
David Mendes
1
, Irene Pimenta Rodrigues
1
and Carlos Fernandes Baeta
2
1
Departamento de Informática, Universidade de Évora, 7004-516 Évora, Portugal
2
Departmento de Medicina, Hospital José Maria Grande, Portalegre, Portugal
Keywords:
OGCP, OGMS, CPR, Ontological Realism, SOAP, Clinical Practice Knowledge, OWL.
Abstract:
We introduce the Ontology for General Clinical Practice (OGCP) for better knowledge representation support
in the Clinical Practice domain. We followed the established OBO Foundry principles to leverage the onto-
logical relations that might be present in the ontology axioms we harvest from clinical reports text segments.
In accordance to the Ontological Realism principles we expect the reasoning inferred from the ontological
relations to render more acceptable consequences then logical relations alone. We enhance the Ontology for
General Medical Science (OGMS) with the Computer-Based Patient Record Ontology (CPR) structure and
propose knowledge base creation/enhancing automatically extracting from clinical reports written in the, well
known to the medical community, SOAP format. Reasoning over the resulting (OGCP) knowledge base with
novel parallel algorithms that appeared recently in literature is presented. We finally propose Controlled
Natural Language justifications of the inferred knowledge intending to achieve wider acceptance among clin-
icians.
1 MOTIVATION AND RESEARCH
QUESTIONS
Originally our research intention was the develop-
ment of personal CDS
1
tools to help the healthcare
professionals in scarce resource countries like most
in Africa and Asia. After evaluating the State-of-the-
Art presented ahead we found that relevant work is
yet to be done in the KR
2
area regarding the Clinical
Practice domain. We believe that some developments
that have been achieved recently motivate us to incor-
porate our expertise in NLP
3
into effective ontology
population. Our main intention is to be able to auto-
matically produce clinical practice knowledge bases
extracting from healthcare reports text.
Research Questions. Ontologies in the sub-domain
of Clinical Medicine
4
are lacking some thorough
study. These can be stated as current problems for the
effectiveness of using them as knowledge support for
1
Clinical Decision Support
2
Knowledge Representation
3
Natural Language Processing
4
The study of disease by direct examination of the living
patient
clinical reasoning. Problems found in current ontolo-
gies and enumerated in literature (Hoehndorf et al.,
2011) that lead to reasoning hurdles are:
• Lack of adequate modularization to achieve
the minimum amount of implicit differentiation
among primitive concepts.
• Inadequate clear separation of digital entities
from the reality they represent.
• Inability to avoid the knowledge acquisition bot-
tleneck (Wong et al., 2012) in order to speed start
any automatic enrichment.
In our work we try to overcome the different is-
sues identified by the several experts in (Brochhausen
et al., 2011). In order to maximize the reasoning capa-
bilities based in our extended OGMS(OGMS, 2010)
ontology, different considerations in the referred work
by Brochhausen et al. were taken into good ac-
count. We complemented the OGMS ontology with
the CPR into what we call the OGCP that is intended
to be a more supportive structure for representation of
clinical practice while, at the same time, embodies a
formal medical theory of disease and healthcare.
286
Mendes D., Rodrigues I. and Fernandes Baeta C..
Development and Population of an Elaborate Formal Ontology for Clinical Practice Knowledge Representation.
DOI: 10.5220/0004548602860292
In Proceedings of the International Conference on Knowledge Engineering and Ontology Development (KEOD-2013), pages 286-292
ISBN: 978-989-8565-81-5
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

2 STATE OF THE ART
Our previous work (Mendes and Rodrigues, 2012b),
where an exhaustive state of the art is presented, is
focusing mainly over the CPR ontology (W3C, 2009)
but we are now targeting an extended OGMS because
it is more promising as suitable for representation
of a disease theory and model enhancing the corre-
sponding reasoning capabilities. We base our work
in (Ogbuji, 2011) for what matters about the foun-
dational principles of structuring meaningful knowl-
edge representation as a framework for clinical rea-
soning. We consider the above mentioned (Smith and
Ceusters, 2010) for Ontological Realism approach.
We used the excellent recent review by Wong (Wong
et al., 2012) for updated state of the art problems in
knowledge acquisition from text. We explore the re-
cent achievements in controlled natural language gen-
eration presented in (Kaljurand, 2010) with the dis-
tributed processing possibilities suggested in (Kaza-
kov et al., 2011) for consequence based axiom infer-
ring introduced in (Simancik et al., 2011).
3 APPROACH
We illustrate the relations between open questions
and the current line of work to illustrate the used ap-
proach:
Ontological Realism and Relations. The method-
ology to avoid mistakes that cannot be detected by
logical formalisms alone is the formal use of Onto-
logical Realism. We highlight the reasoning power
that formal ontological relations provide to a carefully
crafted ontology given the higher semantic level that
these relations comprise (Smith and Ceusters, 2010).
The formalization of Ontological Relations has been
advocated for many years and it succeeded in the
development of "relations that obtain between enti-
ties in reality, independently of our ways of gaining
knowledge about such entities" (Smith et al., 2005).
OGCP as Suitable Support for Clinical Practice
Knowledge. It is an ontology of entities involved
in a clinical encounter. OGCP includes very general
terms that are used across medical disciplines, includ-
ing: ’disease’, ’disorder’, ’disease course’, ’diagno-
sis’, ’patient’, and ’healthcare provider’. OGCP uses
the Basic Formal Ontology (BFO) (BFO, 2012) as an
upper-level ontology. OGCP provides a formal theory
of disease and treatment. This theory is implemented
using OWL-DL and is available in OWL.
SNOMED CT as the Primary Terminology Aggre-
gation. Our effort will take advantage of the breadth
of coverage of SNOMED CT in our domain of inter-
est(Smith and Brochhausen, 2010).
It has an underlying description logic (EL family).
EL family has shown to be suitable for medical ter-
minology processing and subsequently, E LH R + is
the performance target of many modern classifiers in-
cluding those based in consequence driven reasoning
capable of classifying SNOMED CT in practical and
acceptable processing times with recent proposed ex-
tension for concurrent processing (Simancik et al.,
2011) that benefits of current advances in BigData
cluster processing.
OGCP abiding to OBO Foundry. The upper-level
ontologies that support OGCP are introduced in what
regards the ontological relations that can and shall be
used: BFO (IFOMIS, 2004) is strictly focused on the
task of providing a genuine upper ontology which can
be used in support of domain ontologies developed for
scientific research within the framework of the OBO
Foundry; FMA; RO(RO, 2012) and AIAO.
Clinical Ontology Fine Tuning. Starting from the
ontology alignment in the following figure.
Figure 1: Ontology Alignment.
We made an effort of trimming and pruning of
the OGMS and CPR complementing in accordance
to our team of cardiologists to better accommodate
their needs expressed in the reports we sampled. That
included some "gardening" to include: SO the Symp-
tom Ontology, VSO the Vital Signs Ontology and oth-
ers all of them accord to OBO Foundry principles. In
order to align the clinical concepts in the various on-
tologies present, an effort was needed to amalgamate
them according to a sound theory of disease and that’s
why we incorporate the DO that was expressly built
with this purpose in mind (Schriml et al., 2012). The
DevelopmentandPopulationofanElaborateFormalOntologyforClinicalPracticeKnowledgeRepresentation
287

Disease Ontology is a community driven, open source
ontology that is designed to link disparate datasets
through disease concepts. It’s provided a computable
structure of inheritable, environmental and infectious
origins of human disease to facilitate the connection
of genetic data, clinical data, and symptoms through
the lens of human disease (Wiki-DO, 2012). The DO
semantically integrates disease and medical vocabu-
laries through extensive cross mapping and integra-
tion of MeSH, ICD, NCI Thesaurus, SNOMED CT
and OMIM (OMIM, 2012) disease-specific terms and
identifiers. It represents a comprehensive knowledge
base of 8043 inherited, developmental and acquired
human diseases.
Ontology Learning From Text. The problem of
acquiring the knowledge necessary for ontology pop-
ulation known as the "Knowledge Acquisition Bottle-
neck" is a challenging (Wong et al., 2012) issue that
remains one of the main barriers for automated acqui-
sition and we tried to circumvent it by using a progres-
sive tutored learning approach. We start from semi-
structured text and use the semi-automated translation
tasks to generate a controlled domain specific vocab-
ulary on which further acquisition tasks build upon
(Mendes and Rodrigues, 2012b) minimizing ambi-
guity and redundancy for better reasoning capabili-
ties. When instantiating individuals (populate) formal
heavyweight ontologies like the OGCP we do not nor-
mally intend to enrich the ontology but instead turn
them from theoretical models of the domain into rea-
soning able knowledge bases.
4 RESEARCH METHODOLOGY
As reviewed in (Wong et al., 2012) the state-of-the-
Art for acquisition from Clinical Text has enjoyed
strong developments in recent years. We are diving
into extraction from free text present in most inter-
faces used by clinicians. So far we are elaborating in
Cardiovascular related healthcare.
4.1 Text Ontological Annotation
To convert the source texts (clinical note, release re-
port, exam report, or others) the process is a trans-
forming sequence that involves several sequential
steps. This transformation renders ultimately an
OGCP instance. These tasks can be done manually or
automated. Those steps workflow can be configured
declaratively using the software architecture shown in
section 5.1. There are steps involved that consist of:
Figure 2: SOAP Report Sample.
• PDF to raw text or to structured (XML) convert-
ing for adequate documents cleansing. For in-
stance the graphical presentation of Vital Signs
that are originally rendered in the respective report
has to be deleted from the document for easier
terms processing and the tables with values must
be structured accordingly for the annotators to be-
have properly. Initially there is a proof of con-
cept that involves manually cleaning the original
reports
• Manual translation (that is indispensable for the
translator tutoring as shown in 4.2) with the
precise clinicians validation of their jargon ade-
quately translated into English,
• Annotation, either manually using the Web inter-
face of any of the services that we introduce in 5.2,
or automatically through the Web Services avail-
able
• Filtering the concepts from the annotated text to
insert in OGCP instances
Given the array of available Web Services that can se-
mantically annotate bio-medical concepts in English
that are presented ahead in section 5.2, we chose to
use an evolutionary approach for use of the BioPortal
annotator (Noy et al., 2009). We mean by evolution-
ary approach the fact that we first use the annotator af-
ter manual pre-processing and then a more automatic
workflow.
4.2 Using Automated Translation for
Concept Unification
We can take advantage of the fact that we have to
translate from jargon to English to customize the
Google translator toolkit
5
with our own Translation
5
https://translate.google.com/toolkit
KEOD2013-InternationalConferenceonKnowledgeEngineeringandOntologyDevelopment
288
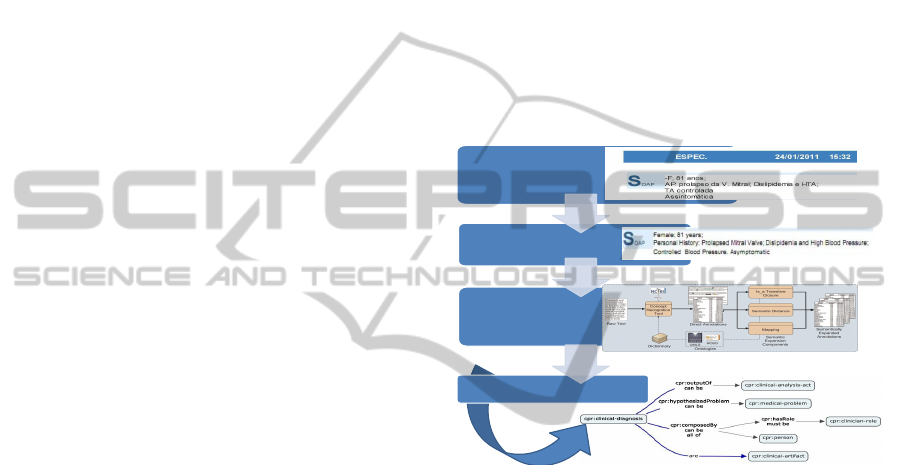
Memories and Glossaries. Let us introduce some
demonstrative examples taken from the sample doc-
ument gently provided by Dr. Carlos Baeta and prop-
erly de-identified presented in the figure "SOAP Re-
port Sample" above.
We will, in the process of using the Google toolkit,
create Translation Memories with the identified per-
sonal acronyms like:
• AP (Antecedentes Pessoais) into Personal History
• HTA (Hiper Tensão Arterial) into High Blood
Pressure
• FA (Fibrilhação Auricular) into Atrial Fibrilation
• V. Mitral (Válvula Mitral) into Mitral Valve
Some which are acronyms that can be given the suit-
able translated concept like:
• ECG (Electro Cardio Grama) into Electro Cardio
Gram
or those that are even English acronyms:
• INR (International Normalized Ratio) into Inter-
national Normalized Ratio
Included in this sample are notorious some more com-
plex problems that are not related to the translation it-
self but with some other problems like the time span-
ning of concepts like “1 comp/dia” which is ade-
quately translated to “1 tablet per day” using the de-
fined Translation Memory but has to be posteriorly
exactly characterized as time delimited occurring pro-
cess.
4.3 SOAP Report
This report depicts a clinical encounter in a semi-
structured way. As seen previously in the figure in
this section we find sections that can be associated
with
Symptoms, the subjective section S where we extract
directly to ogcp:symptom-recording.
Signs, the objective section O that are
ogcp:sign-recording that we take as gen-
erator for ogcp:clinical-findings.
Actions, the analysis section A which are the
ogcp:clinical-investigation-act whose outputs
can be ogcp:clinical-artifact to investigate
things that can be ogcp:isConsequenceOf
any of ogcp:physiological-process or
ogcp:pathological-process
and finally
Plan, the plan section P where the therapeutic acts
can be extracted with all the timing, posology and
prescriptions registered in a particular clinical en-
counter.
We find then that if a sufficient amount of clin-
ical reports are fed into the knowledge base it will
ultimately build a sound picture of a clinical practice.
For the inferred axioms to be believable by the com-
munity and thus usable as a Clinical Practice Support-
ing Tool that generated knowledge has to be clearly,
although basically, explained to the user.
4.4 The Complete Acquisition
Workflow Picture
Text cleansing
•Lexical, Syntactic and Morphological tagging
•Acronym identification through TM development
Accurate translation
Raw text convert
Expanded Semantic annotation through
BioPortal
Export into TXT, CSV or XML
GRDDL XSLT
OGCP instance creation
Figure 3: Acquisition Flowchart.
The flowchart that depicts graphically the acqui-
sition from the source texts in Portuguese to the cre-
ation of the appropriate OGCP instance is shown in
figure "Acquisition Flowchart"
5 RESULTS
5.1 Software Implementation
We have presented the full conception of an archi-
tecture in (Mendes and Rodrigues, 2012a). We are
proposing an extensible Enterprise Architecture based
in a ESB which we call CP-ESP (Clinical Practice -
Enterprise Service Bus). This is a common rail where
messaging can flow using a subscription model that
enables the communication to be detached from any
two particular services but instead be available on-
request by one and served by another in a loosely
coupled way. The ESB can then intervene in mes-
sage exchange and overwrite standard rules for ser-
vice execution. The case of an intervention here is
DevelopmentandPopulationofanElaborateFormalOntologyforClinicalPracticeKnowledgeRepresentation
289

the ability to filter and redirect invocations to the
appropriate NLP task processors depending on the
source being labeled with the status of the load it
carries. The REST philosophy is suggested in our
proposal as the best way of implementing a Service
Oriented Architecture that serves as the communica-
tion underlying structure of our system. REST end-
points are available for the generality of our needs.
The available Web Services can render responses in
highly-structured forms like JSON or in any of the
standardized mime types that can be handled by the
filtering and enqueuing capabilities of any config-
urable available ESB like those based in Apache Ser-
viceMix (http://servicemix.apache.org/home.html) or
Mule (http://www.mulesoft.org/) for instance. They
can be configured to compose a complete pipeline
very easily:
Figure 4: Instance Translation and Creation.
In the picture is shown the possibility of defining
services (daemons) that monitor the presence of new
reports and appropriately apply the needed transfor-
mations according to their status and content until a
translated document is delivered to the adequate end-
point for annotation. All of this can even be done with
due care about scalability, availability and all prob-
lems associated with a modern state-of-the-art soft-
ware architecture as presented in (Mendes and Ro-
drigues, 2012a).
In the picture is shown the possibility of defin-
ing services (daemons) that monitor the presence
of new reports and appropriately apply the needed
transformations according to their status and con-
tent until a translated document is delivered to the
adequate end-point for annotation. All of this can
even be done with due care about scalability, avail-
ability and all problems associated with a modern
state-of-the-art software architecture as presented in
(Mendes and Rodrigues, 2012a) Building over the
suggested infrastructure the systems are rather com-
posed as opposed to monolithically built and so man-
ifest high capabilities of plug-and-play configuration
allowing for interchangeable providers (as Web Ser-
vices), Reference Ontologies (Feeders), and target
ontologies. Having the foundations available with
the right weapons provided one has to take a prac-
tical approach to the development of a target system
using, in our case, the Java best-practices for prag-
matic development that include a number of Patterns
as in JEE (Java Enterprise Edition) or the pragmatic
approaches developed in such successful projects as
Spring (http://www.springsource.com/).
5.2 OGCP-ESB
We use, through BioPortal and ODIE, algorithms for
Named Entity Recognition, Co-reference resolution,
concept discovery, discourse reasoning and attribute
value extraction. A local version gives the possibility
of developing extensions to the algorithms provided
in the base offering allowing, for instance, targeting
different languages in the NLP tasks. The Web Ser-
vices provided by BioPortal or ODIE can be locally
extended and refined for different sources and are pro-
vided as one of the project deliverables.
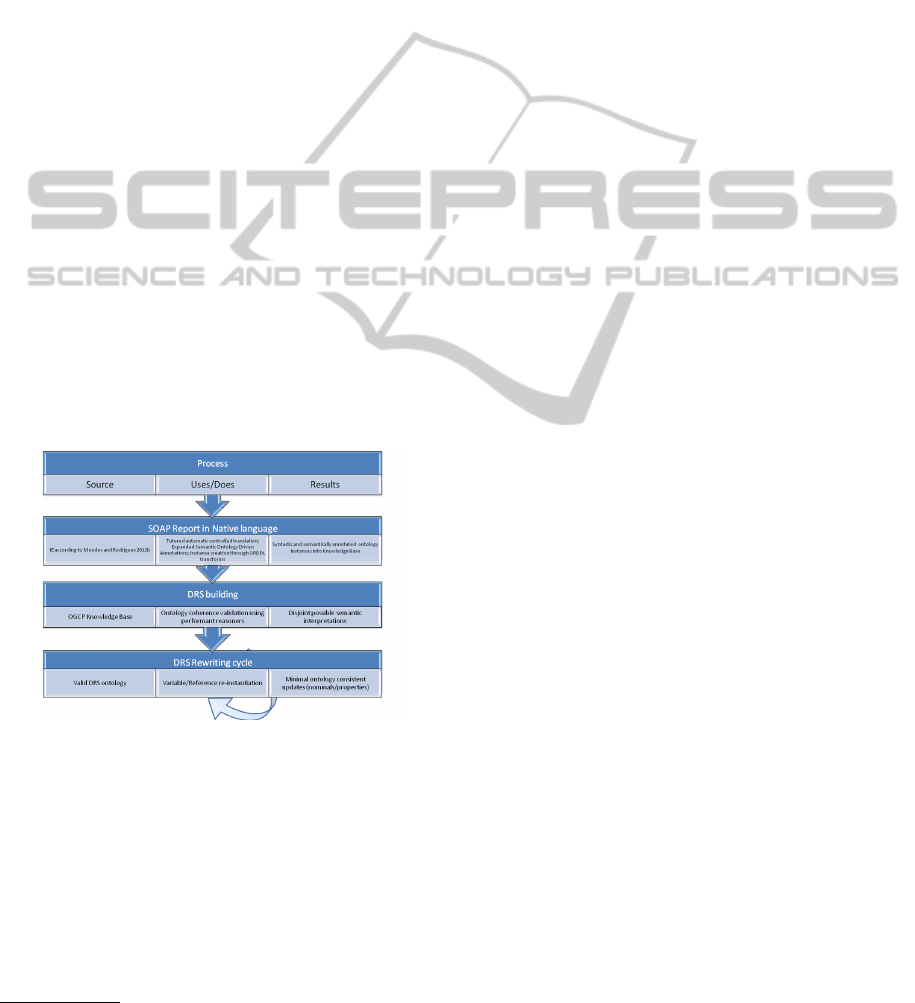
5.3 NLP Pragmatics and Discourse
Controller
The text for any particular encounter (actually for any
Clinical Episode) may be collected in the form suit-
able for processing into the Ontology framework us-
ing some NLP pragmatics. Populating the OGCP
the “Clinical Picture” is completed and thus our KB
is available for validation and further logical infer-
encing. The semantic representation is done us-
ing pragmatic interpretation as defined in our fellow
researcher at CENTRIA Dora Melo’s article (Melo
et al., 2012). The enrichment process must always
maintain the entailments provided by the base (gold-
standard) ontologies and so can never lead to incon-
sistency. We use a round-trip, debug and repair, build-
ing method to populate/enhance the OGCP then. For
any new instance the validation is performed and new
possible inferred facts generated if consistency is yet
valid. These new facts are candidates for NLP justifi-
cations generation. The main objective of the system
is to provide accurate answers to questions posed by
users and, in our proposal these answers are clinically
valid because the generation method guarantees that.
QA is, however, only one of the interesting features
of our work that is enhanced by the adequate justi-
fication to be evidently useful for practitioners. To
develop justifications from DL
6
arguments inferred
from consequence based reasoners (Kazakov, 2009;
6
Description Logic
KEOD2013-InternationalConferenceonKnowledgeEngineeringandOntologyDevelopment
290
Kazakov et al., 2011) we based our work in (Bail
et al., 2011) to study and compare the justificatory
structure to those present in the NCBO BioPortal ad-
dressed in the mentioned article. The results so far
are in the realm of ’ontology verbalization’, the gen-
erated explanations are still in a controlled natural
language (CNL) fashion. The obtained results seem
to be adequate enough for the users to find them be-
lievable and thus the justifications stand in our con-
trolled clinical setting. We use the verbalization tool-
ing (Kaljurand, 2010) to present the justifications in
an acceptable manner. The foundational techniques
were introduced in (Kaljurand and Fuchs, 2007). For
the verbalization to function properly all the restric-
tions of content are guaranteed in the process of on-
tology (Knowledge base) enrichment from SOAP re-
ports. For instance, all names are English words and
individuals are singular proper names (preferably cap-
italized) named classes are denoted by singular count-
able nouns and (object) properties by transitive verbs
in their lemma form (i.e. infinitive form) (Kalju-
rand and Fuchs, 2007). The decision of what inferred
knowledge is then presented with its justifications to
the user is a task handled by the DC
7
using the de-
veloped pragmatics introduced in the above referred
article (Melo et al., 2012). In our proposed methodol-
ogy we make use os the DC to align the most relevant
clinical terms into a acceptable CNL document and
the process may be graphically presented as:
Figure 5: Discourse Controller Flow.
6 CONCLUSIONS
We propose an OGMS extension using the adequate
ontological realism approaches and incorporating the
CPR and its upper level ontologies as framework for
an EL reasoning workhorse. We present our efforts
for knowledge base population from semi-structured
clinical text reports and discuss the underlying prob-
7
Discourse Controller
lem of automatic instance creation from them into the
proposed knowledge representation structure. Cur-
rently, after having passed an internal process of
validating the proposed framework (Ontology struc-
ture+Population mechanism) we are assessing its ac-
ceptance in a wider regional level by exposing a group
of related cardiologists to the works done so far and
receiving their feedback in a formal and traceable
manner. We are developing a knowledge represen-
tation infrastructure enabling the usage of highly op-
timized distributed consequence based reasoners that
are referred in literature only in 2011. With these very
recent developments it’s finally possible to validate
the enormous knowledge bases that are created by au-
tomatically populating the proposed ontology OGCP
that relies on extensive, and very solid, foundations
like SNOMED-CT and FMA among others. Logi-
cal inferencing and clinical facts entailment that is
possible through this capability is an interesting con-
tribution to the application of Artificial Intelligence
to healthcare. We introduce clinical decision sup-
port systems (CDSS) that are based on such a break-
through technique. We further argue that it is impera-
tive, for the broad acceptance of these tooling by the
medical community, that their inferences are justified
using controlled natural language and adequate termi-
nology.
7 FUTURE WORK
We intend to deliver OGCP in the NCBO BioPor-
tal as soon as it reaches a minimum of usability as
KR tool for cardiology which we intend to happen
later this year. We are currently in the evaluation pro-
cess mentioned above and, depending on the level of
usability/acceptance, will evolve to different clinical
specialties to demonstrate its flexibility. Shall all the
efforts prove to be worthy we will try to extend it
to wider levels following a community development
process based in some OSS (Open Source Software)
repository like Google Code for example. It will all
be summed up in the PhD thesis of the first author to
be presented late 2013.
ACKNOWLEDGEMENTS
We acknowledge IIFA - Instituto de Investigação e
Formação Avançada of Universidade de Évora for the
Bento de Jesus Caraça scholarship that is awarded to
the first author and CENTRIA Center for Research in
Artificial Intelligence of Faculdade de Ciências e Tec-
DevelopmentandPopulationofanElaborateFormalOntologyforClinicalPracticeKnowledgeRepresentation
291

nologia of Universidade Nova de Lisboa for its
continuous financial support of our work.
REFERENCES
Bail, S., Horridge, M., Parsia, B., and Sattler, U. (2011).
The justificatory structure of the ncbo bioportal on-
tologies. In Aroyo, L., Welty, C., Alani, H., Taylor, J.,
Bernstein, A., Kagal, L., Noy, N. F., and Blomqvist,
E., editors, International Semantic Web Conference
(1), volume 7031 of Lecture Notes in Computer Sci-
ence, page 67Ã
´
câ
´
C
ˇ
nâ
˘
AIJ82. Springer.
BFO (2012). Basic formal ontology 2.0.
Brochhausen, M., Burgun, A., Ceusters, W., Hasman, A.,
Leong, T., Musen, M., Oliveira, J., Peleg, M., Rector,
A., Schulz, S., et al. (2011). Discussion of" biomedi-
cal ontologies: Toward scientific debate". Methods of
information in medicine, 50(3):217.
Hoehndorf, R., Dumontier, M., Oellrich, A., Rebholz-
Schuhmann, D., Schofield, P., and Gkoutos, G.
(2011). Interoperability between biomedical ontolo-
gies through relation expansion, upper-level ontolo-
gies and automatic reasoning. PloS one, 6(7):e22006.
IFOMIS (2004). Basic formal ontology.
Kaljurand, K. (2010). Owl verbalizer: making machine-
readable knowledge also human-readable. Available
Online: https://code.google.com/p/owlverbalizer/.
Kaljurand, K. and Fuchs, N. E. (2007). Verbalizing
owl in attempto controlled english. Proceedings of
OWLED07.
Kazakov, Y. (2009). Consequence-Driven Reasoning for
Horn SHIQ Ontologies. In Boutilier, C., editor, IJCAI,
pages 2040–2045. IJCAI Distinguished Paper Award
Winner.
Kazakov, Y., Krötzsch, M., and Simancík, F. (2011). Con-
current classification of el ontologies. In Proceedings
of the 10th international conference on The seman-
tic web - Volume Part I, ISWC’11, pages 305–320,
Berlin, Heidelberg. Springer-Verlag.
Melo, D., Rodrigues, I., and Nogueira, V. (2012). Work
out the semantic web search: The cooperative way.
Advances in Artificial Intelligence, 2012.
Mendes, D. and Rodrigues, I. P. (2012a). A Semantic
Web pragmatic approach to develop Clinical Ontolo-
gies, and thus Semantic Interoperability, based in HL7
v2.xml messaging. In Information Systems and Tech-
nologies for Enhancing Health and Social Care. IGI
Global.
Mendes, D. and Rodrigues, I. P. (2012b). Advances to se-
mantic interoperability through cpr ontology extract-
ing from soap framework reports. electronic Journal
of Health Informatics.
Noy, N. F., Shah, N. H., Whetzel, P. L., Dai, B., Dorf, M.,
Griffith, N., Jonquet, C., Rubin, D. L., Storey, M.-A.,
Chute, C. G., and Musen, M. a. (2009). BioPortal:
ontologies and integrated data resources at the click
of a mouse. Nucleic acids research, 37(Web Server
issue):W170–3.
Ogbuji, C. (2011). A Framework Ontology for Computer-
Based Patient Record Systems. In Proceedings of the
ICBO: International Conference on Biomedical On-
tology, pages 217–223, Buffalo, NY, USA.
OGMS (2010). Ontology for general medical science.
OMIM (2012). Omim, online mendelian inheritance in
man. Available Online: http://www.ncbi.nlm.nih.gov/
omim.
RO, O. F. (2012). Relations ontology.
Schriml, L., Arze, C., Nadendla, S., Chang, Y., Mazaitis,
M., Felix, V., Feng, G., and Kibbe, W. (2012). Dis-
ease ontology: a backbone for disease semantic inte-
gration. Nucleic Acids Research, 40(D1):D940–D946.
Simancik, F., Kazakov, Y., and Horrocks, I. (2011).
Consequence-Based Reasoning beyond Horn Ontolo-
gies. In Walsh, T., editor, IJCAI, pages 1093–1098.
IJCAI/AAAI.
Smith, B. and Brochhausen, M. (2010). Putting Biomedical
Ontologies to Work. Methods Inf Med, 49.
Smith, B. and Ceusters, W. (2010). Ontological realism:
A methodology for coordinated evolution of scientific
ontologies. Applied ontology, 5(3-4):139–188.
Smith, B., Ceusters, W., Klagges, B., KÃ˝uhler, J., Kumar,
A., Lomax, J., Mungall, C., Neuhaus, F., Rector, A. L.,
and Rosse, C. (2005). Relations in biomedical ontolo-
gies. Genome Biol, 6(5):R46.
W3C (2009). Computer-based patient record ontology.
http://code.google.com/p/cprontology. http://code.
google.com/p/cprontology.
Wiki-DO (2012). Disease ontology wiki page. Avail-
able Online: http://do-wiki.nubic.northwestern.edu/
do-wiki/index.php/Main_Page.
Wong, W., Liu, W., and Bennamoun, M. (2012). Ontology
learning from text: A look back and into the future.
ACM Comput. Surv., 44(4):20:1–20:36.
KEOD2013-InternationalConferenceonKnowledgeEngineeringandOntologyDevelopment
292
