
Technical Trends and Challenges in Mobile Health
A Systematic Review of Recent Available Literature
Daniel Antonio Callegari, Luis Carlos Jersak and Adriana Cássia da Costa
FACIN - Faculdade de Informática, Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, RS, Brazil
Keywords: Mobile, Health, Systematic Review, Trends, Challenges.
Abstract: This paper presents the state of the art from the available literature on mobile health care. The study was
performed by means of a systematic review, a way of assessing and interpreting all available research on a
particular topic in a given area, using a reliable and rigorous method. From an initial amount of 1,482
papers, we extracted and analysed data via a full reading of 40 (2.69%) of the papers that matched our
selection criteria. Our analysis since 2010 show current development in 10 application areas and present on-
going trends and technical challenges on the subject. The application areas include patient monitoring,
infrastructure, software architecture, modelling, framework, security, notifications, multimedia, mobile
cloud computing, and literature reviews on the topic. The most relevant challenges include the low battery
life of devices, multiplatform development, data transmission and security. Our study consolidates recent
findings in the field and serves as a resourceful guide for future research planning and development.
1 INTRODUCTION
Today, one area that deserves attention in mobile
technology is health care. In a broader sense, health
care has experienced changes in treatment, exam
manipulation and also on the development of studies
in remote regions. The World Health Organization
(2011) defines Mobile Health as the medical practice
with support of mobile devices, such as cell phones,
patient monitoring devices, PDAs and other wireless
devices, including the use of cell phones’ functions
like audio, messages, Bluetooth and other services.
The present work focuses on identifying the state
of the art on mobile health in terms of application
areas, pointing out current trends and challenges.
This research is performed by means of a systematic
review on the more recent available literature. A
total of 1,482 papers from January 2010 to January
2013 were analysed and 2.69% of the sample
matched our research criteria – see (Biolchini et al.,
2005). Our findings are intended as a resourceful
guide for future research planning and development
on the area. The systematic review follows the
protocol proposed by Kitchenham (2004). In the
following sections, we assume that the reader is
familiar with such research method. Due to space
reasons, we only present the most relevant aspects in
this paper. Other details can be found in
(Jersak et. al., 2013).
2 EARLY CLASSIFICATION
OF STUDIES
Since each of the selected papers follow a different
research methodology, we first grouped them in 10
different methodologies according to the
classification presented in (Oates, 2006). The
methodology that had the majority of the papers was
“design and creation”, containing 21 of the 40
papers (52.5%). Seven papers were classified as
“experiments”, five papers as “proof of concept”,
three as “literature review”, two as “case-study”, one
as “survey”, and one as “ethnography”.
Most of the papers (26 in 40; i.e. 65%) used
prototypes to test the solutions. Among those
studies, half of them (13) focused on patient
monitoring (Fernandes et al., 2011; Catarinucci et
al., 2012; Chi et al., 2010; Heslop et al., 2010;
Ivanov et al., 2010; Lara et al., 2012; Pandey et al.,
2012; Masse et al., 2010; Pigadas et al., 2011; Siebra
et al., 2011; Soomro and Schmitt, 2011; Al-Taee et
al., 2011; O’Brien et al., 2010).
Works focusing on vital signs such as blood
pressure and heart rate were also frequent, as well as
studies about daily life monitoring and transmission
519
Antonio Callegari D., Carlos Jersak L. and Cássia da Costa A..
Technical Trends and Challenges in Mobile Health - A Systematic Review of Recent Available Literature.
DOI: 10.5220/0004563405190525
In Proceedings of the 15th International Conference on Enterprise Information Systems (ICEIS-2013), pages 519-525
ISBN: 978-989-8565-60-0
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)
of such data (see section 3). It is worth noting that
monitoring applications very often require specific
hardware to collect the patient’s data, such as
sensors for an ECG (electrocardiography) or blood
pressure measurement (see section 3.1).
3 MOBILE HEALTH
APPLICATION AREAS
This section presents our findings regarding
mHealth solutions in the identified areas.
3.1 Patient Monitoring
Several of the analysed studies focus on solutions
for monitoring bio-signals. Monitoring is usually
done using external sensors. These sensors usually
communicate with the mobile device via Wi-Fi or
short-ranged protocols such as Bluetooth. We found
that in most cases the mobile device acts as a
gateway that gathers raw data from the sensors and
then forwards it to a separate system that will
process it and return data ready for visualization by
doctors or the patient himself.
As a first example, Masse et al. (2010) use a
smartphone as a gateway to collect bio-signal data
from sensors and further present it to the doctor or
patient. Other studies (Pigadas et al., 2011; Lara et
al., 2012; Warren et al., 2011) and (Al-Taee et al.,
2011) propose monitoring systems in which the
sensor data is gathered by the smartphone and then
sent to a remote server for processing and storage.
Similarly, the study from Pandey et al. (2012)
presents a system in which the mobile device
collects data and sends it for processing in the cloud.
The mobile device can also retrieve data from the
cloud and present it to the doctor or patient.
Likewise, Fernandes et al. (2011) propose a solution
where data gathered from external sensors by the
mobile device is forwarded via a ZigBee link to a
computer that acts as a ZigBee-to-Wi-Fi gateway.
This computer also processes the data and then
sends it to a remote server where it is stored and can
be accessed using mobile devices or the web.
Blumrosen et al. (2011) present a solution that
gathers sensor data via a ZigBee network using the
smartphone at first as a gateway. The data is sent via
MMS (Multimedia Messaging Service) to an e-mail
box at a remote server for analysis and processing.
The data is then sent back to the smartphone so the
patient can visualize it.
At times hardware evolve so quickly that it is
hard to keep up-to-date knowledge in this regard. In
Ivanov et al.’s work (2010) an example of a
monitoring application is presented and tested in 11
different smartphones and PDAs. The objective was
to check and compare the performance of each
device for health care applications. The study from
Pereira et al. (2011) shows a solution implemented
in 4 different operating systems (Android, Symbian,
iOS and Windows Mobile). This solution
communicates with the sensors via Bluetooth and is
capable of plotting graphs to better show the
patients’ vital signs.
By the analysis of the studies under the patient
monitoring category, we found that 12 proposals use
some sort of sensor to gather the patient’s vital
signs. It is important to note that the sensors built-in
to the mobile devices are typically insufficient to
cover the needs of this area.
The solutions presented in Masse et al. (2010)
and in Chi et al. (2010) have even developed
prototypes for those types of sensors. The sensors
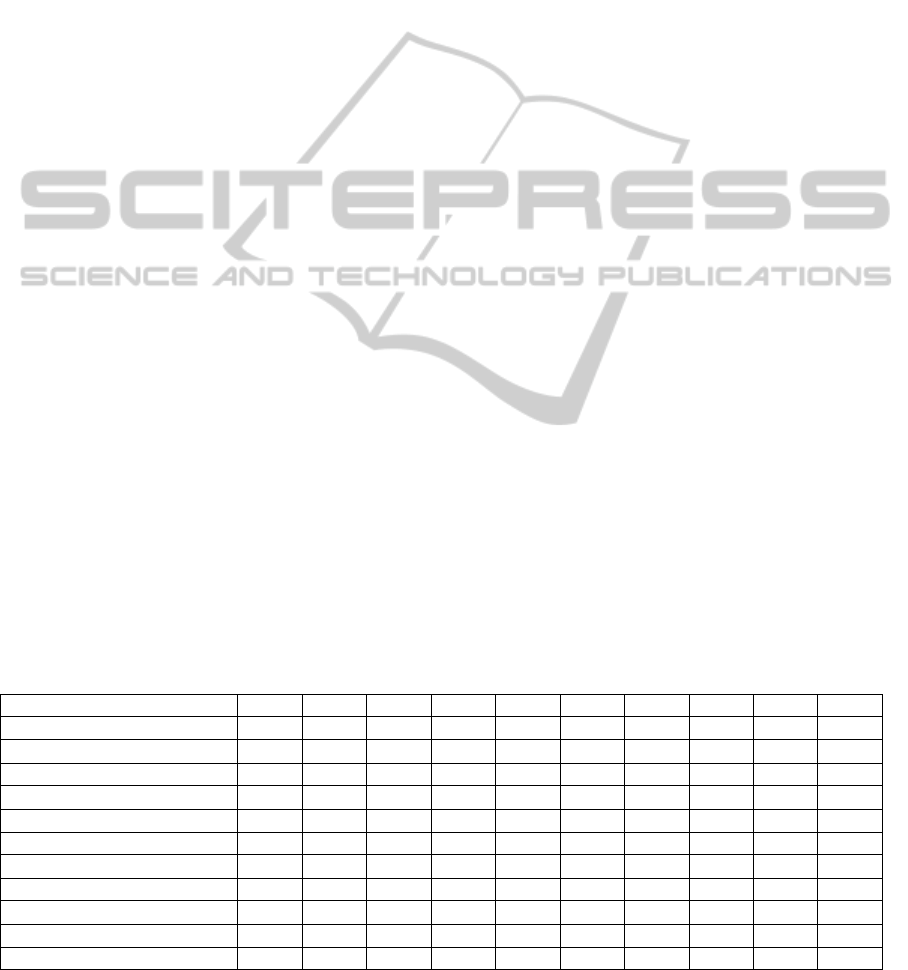
Table 1: The use of sensors in each proposal.
Source / Sensor ECG EEG BP Temp RR HR Accel* GPS* Lum* Gyr*
Fernandes et al., 2011
X
X
X
Altini et al., 2010
X
X
Blumrosen et al., 2011***
X
Catarinucci et al., 2012***
X
X
Chi et al., 2010
X X
Lara et al., 2012
X
X
X
X
X
O’Brien et al., 2010***
X
X
Pandey et al., 2012
X
Masse et al., 2010
X
X**
Pereira et al., 2011***
X
Pigadas et al., 2011
X
X X
* Mobile devices’ native (built-in) sensors; ** In this case, the accelerometer is encapsulated in an external sensor; *** The number of sensors is small
because this is only a demonstration of the application’s features. In the case of real use, more sensors can be involved.
ICEIS2013-15thInternationalConferenceonEnterpriseInformationSystems
520

found in the studies were: Electrocardiogram (ECG);
Electroencephalogram (EEG); Blood Pressure (BP);
Skin Temperature (Temp); Respiratory Rate (RR);
Heart Rate (HR); Accelerometer (Accel); GPS;
Luminosity Sensor (Lum); Gyroscope (Gyr). We
observe from Table 1 that most of the sensors used
in those solutions are not built-in to the mobile
devices.
From the 11 studies that do use sensors, only 3
did not use an external sensor. From those 3 studies,
the solution shown in Pigadas et al. (2011) only
keeps track of the patient’s location and corporal
position, while in the works of Blumrosen et al.
(2011) and O'Brien et al. (2010) the sensors are only
used as a proof of concept for the proposed solutions
of the respective studies, as those solutions focus on
communication or data processing. Thus, it is
important to note that applications that keep track of
vital signs will typicaly have to depend on external
sensors, as the available technology for mobile
devices is not capable or reliable enough for
measuring such important data.
3.2 Hardware Infrastructure
In mobile health applications, the low battery life of
devices is a frequent complaint. In Heslop et al.
(2010), for instance, the authors mention the benefits
of tablets, such as the ease of use and good screen
resolution that favours the visualization of certain
exams, e.g. radiology images, but report an average
battery life of only 2.5 hours. Smaller devices such
as mobile phones contain even less battery capacity.
In fact, despite technology advances, we found that
in several cases batteries do not last long enough to
cover an entire work day in such circumstances –
e.g. Siebra et al. (2011), Warren et al. (2011),
Pandey et al. (2012), Lagerspetz and Tarkoma
(2011), Alamri (2012). The remote processing of
data is a growing trend as we shall see later in
section 3.10.
3.3 Software Architecture
A mobile network architecture for clinical use is
proposed in (Rahbar, 2010). The health care unit
receives the patient's location and sends help from
the nearest location.
The study presented in (Siebra et al., 2011)
focuses on monitoring systems that use SMS and
agents which analyze information and make
decisions. Also, it tries to address energy
consumption and emergency alerts. Patient data is
sent from the sensors to the smartphone via
Bluetooth. Heart rate and blood pressure sensors
were used for testing the solution.
Several studies on architectures were found,
including solutions for monitoring specific areas
such as (Blobel, 2011) and many address cloud
computing solutions (section 3.10).
3.4 Modelling
Only one paper was classified under the modeling
area (Gomes et al., 2012). It presents a modeling of
their proposal for an mHealth software product line,
leaving the implementation in a real environment for
future work. A drawback of this kind of approach is
that we can only estimate how the solution's
behavior would be. In other words, real world
situations would be more suitable for testing and
analysis.
3.5 Software Development
Frameworks
Ahmed and Ahamad (2012) propose a framework
for mHealth data security on Android systems. It is
possible to define which data will be monitored by
the framework by configuring some parameters.
When an application running on the patient’s
smartphone tries to transfer monitored data to an
unknown destination, the user is prompted if she
really wants to complete the operation.
The work by Lin et al. (2010) proposes a
framework to facilitate the development of
applications which communicate with external
sensors. Authors claim that the framework simplifies
the programming of sensors using what they call
senselets – blocks that run in between the sensors
and the application; they are platform independent
and they abstract sensor calls. In the prototype, the
authors manage to, in some cases, obtain a decrease
of over 75% on the initial source code lines required
for a solution (e.g. from 72 to 17 lines in the case of
a fall detector application).
As noted before, mobile devices present a special
issue regarding battery life. Warren et al. (2011)
present a service oriented framework for monitoring
applications that implements context-aware
characteristics. As an example of this feature, the
framework may change the current connection type
for one that uses less battery (e.g. Wi-Fi to
Bluetooth) when available.
In their study, Constantinescu and colleagues
(2012) propose a framework for medical multimedia
data. A daemon of the framework is attached to
mHealth applications, collecting the multimedia data
TechnicalTrendsandChallengesinMobileHealth-ASystematicReviewofRecentAvailableLiterature
521

and adapting them to be viewed using different
methods (web browser, mobile devices, etc.). Also,
the daemons may communicate to each other,
creating a data cloud that is transparent to the user.
3.6 Security
Security is an obligatory issue in health solutions.
For example, Ahmed and Ahamad (2012) propose a
framework to force security policies in mHealth
applications for Android devices. This is done using
a system that marks sensitive data. When this data is
requested for another application or for transmission,
the framework uses pre-established rules to manage
these requests, granting or not access to the data.
In parallel, Mashima and Ahamad (2012)
propose accountability techniques for eHealth data,
with a patient-centric focus. The main concern
assessed in this study is that the patient should know
what is being done with his medical data and be
informed about it. This study tries to reach three
goals: (1) Accountable update: update the patient
about changes made in his medical data stored in a
repository; (2) Accountable usage: inform the
patient when his data is used by an entity; (3)
Protection of honest entities: this happens in the
form of protocols that the entities must follow. This
also makes the patient able to dispute requests from
compromised or dishonest entities.
Another study, presented in (Le et al., 2010),
proposes a cryptography scheme for networks for
mobile devices in mHealth using public keys and
elliptic curve cryptography. The network has special
nodes which are responsible for generating and
distributing the keys. After receiving the key, every
time a device needs to transfer information to
another device in the network, these devices
exchange keys and the connection is encrypted.
Similarly to those two works, Barua and
colleagues (2011) propose a cryptography system
using public keys to control access to patients’ data.
The system is patient-centric, meaning that the
patient decides how his information can be used.
The work by Barnickel et al. (2010) proposes a
cryptography system using the user/password model
to protect patient data. Every time data needs to be
accessed, the user is prompted for his username and
password, and then a session is started.
Along the same lines, Chen et al. (2012) propose
a cloud based security system for sharing patients
data among different institutions. When a record is
accessed by an organization that does not own it,
permission is requested to the owner (except in
emergency cases).
As we can see, privacy and security of medical data
is a very frequent issue in the analysed work. This
concern is due to the fact that, if this data is
intercepted by a malicious party, it may expose
private and personal aspects of the patient’s lives.
Also, another concern goes around frauds involving
medical data, such as false requests of insurance
prizes. We did not get further into those issues here.
3.7 Notifications
We assume notifications simply as the exchange of
information between parties of a health solution. The
work presented in (Du et al., 2011) focuses on a
system in which the user can send emergency alerts
to family members and doctors. The main focus of
the solution lies not on how the patient interacts with
the system but on how the alerts are sent.
Despite the importance of emergency alerts, this
kind of mechanism may not work properly if the
patient is not in conditions to activate the alert.
3.8 Multimedia
The study presented in (Hewage et al., 2011) takes
advantage of the increasing performance of the
mobile devices and networks and proposes a medical
3D video transmission system over 4G networks.
The study simulates 3D video streaming over a 4G
network inside a hospital environment, and makes
both objective and subjective evaluations. The
objective evaluation was made by analyzing the left
and right sides of an image separately. To do the
subjective evaluation, two doctors were invited to
analyze the quality of the video after the
transmission under different packet sizes. Work
from Constantinescu and colleagues (2012) was
already mentioned in section 3.5. No other relevant
papers were found in this specific area.
3.9 Literature Review
The rare studies classified under the Literature
Review category make a compilation of other
studies and highlight some characteristics and
advantages of those studies. One example is
presented in (Liu et al., 2011), where the authors list
the characteristics of iOS devices from a developer's
point of view. Yet in the study of (Kyriacou et al.,
2011) the scope is reduced to specific applications
for emergency situations, including monitoring
systems, multimedia systems and communication
protocols. Their findings corroborate our analysis.
ICEIS2013-15thInternationalConferenceonEnterpriseInformationSystems
522

3.10 Mobile Cloud Computing
A problem closely related to mobile devices in
general is their low autonomy and limited storage.
As the complexity of the data processed by the
applications has increased, the amount of storage
required to persist this data needs to increase too, as
seen in Lagerspetz and Tarkoma’s work (2011).
Also, despite the advances in the energetic
efficiency of the devices' electronic components,
battery duration remains an issue as not many
devices can withstand long work periods without a
recharge. One solution proposed to diminish such
problems is Cloud Computing. Several solutions use
this paradigm to expand the storage capabilities of
mobile devices, to offload processing-intensive (and
therefore, battery-intensive) tasks or simply to ease
the sharing of data among different medical
facilities. In this section we present some works that
use mHealth and cloud computing together.
The study presented by Berndt et al. (2012)
shows a solution for monitoring several health
aspects like bio-signals, fall detection, chronic
diseases, etc. The whole system's infrastructure is
cloud based, using the IaaS - Infrastructure as a
Service model. The cloud is used to increase the
storage of the system, interconnect web based and
mobile based parts of the system, share data among
several medical units and to interact with health care
services and also for security reasons.
Alamri (2012) proposes a medical imaging and
video encoding system. This solution uses cloud
computing to encode the video streams and
automatically process medical images at the correct
rates/sizes for each device. Offloading the process of
encoding to the cloud saves battery and also can
improve the video streaming for devices in a
network with lower bandwidth by identifying the
connection's speed and adjusting the video rate
accordingly.
The work by Hsieh and Hsu (2012) presents a
mobile ECG service where cloud computing is used
to deliver ECG exams to the doctor's mobile device
for quick analysis. The ECG reports are exported in
XML format by the ECG exam equipment
interconnected with the cloud-based system and then
sent with other patient's info, if required, to the
doctor's mobile device for reading. The authors point
that this speeds up the initial care process as the
doctors can analyze the ECG even before the
patient's arrival at the hospital.
4 TRENDS AND CHALLENGES
FOR MOBILE HEALTH
In this section we summarize the identified
challenges found during our literature review.
First, as mentioned earlier, several papers
highlight how battery lifetime is a main concern.
Batteries currently can not withstand a full work day
(e.g. Heslop et al., 2010 among others). Secondly,
multiplatform development is a concern for other
authors such as Fernandes et al. (2011); iOS,
Windows Phone, and Android being the most
common choices. Third, delays in data transmission
and their consequence on patient monitoring is
another current challenge (e.g. Soomro and Schmitt,
2011).
Finally, a common factor listed among the
studies of literature review is the struggle to
implement the project or software architecture in
real environments. For instance, (Gomes et al.,
2012) presents a model for software development in
the healthcare area, but the authors identify the need
to validate the model in real environments. Despite
health care solutions around the world demand for
new technologies, the inherent diverse
environments, security issues, and sometimes
people’s resistance to change remain important
issues to be addressed.
5 RESEARCH SUMMARY
AND FINAL REMARKS
In this systematic review we analyzed state-of-the-
art research related to the Mobile Health subject
area. Four search engines were used to collect
primary and secondary data (see Kitchenham, 2004).
The studies were classified into 10 categories. We
then summarized trends and challenges that we
expect to be addressed by new research on the field.
The key findings are:
1. It remains clear that the mHealth area is in
expansion, mostly due to the advances in mobile
devices technology. Despite the need for external
sensors in several applications, the devices aggregate
some built-in resources which aid in the
development of mHealth applications.
2. Patient monitoring was the most frequent area
in this study. Most of the solutions in this category
use some sort of external sensor to gather the
patient's data and send it to the mobile device. From
the 11 solutions in this category, only 3 did not use
external hardware.
TechnicalTrendsandChallengesinMobileHealth-ASystematicReviewofRecentAvailableLiterature
523

3. Native sensors built in the mobile devices are
insufficient to fulfill the needs of the area. Several
types of communication technologies were found,
Bluetooth being the most used one.
4. Security was the second most frequent
category (8 studies). Placing the patient in the center
of the decision is a very important issue on data
security.
5. The small number of papers in the categories
of infrastructure, modeling, notifications and
multimedia suggests opportunities for further
research.
6. Mobile Cloud Computing appears as an
alternative way to approach battery duration and
storage issues on mobile devices and should also
present opportunities for research, as both Cloud
Computing and mHealth are relatively new
paradigms.
This systematic review consolidates recent
findings in the field and serves as a resourceful
guide for future research planning and development
on the field of mobile heath care. Based on such
findings we now draw the lines for future research in
our group.
The very idea of mobile health involves the
acquisition and the processing of data via mobile
appliances. Nevertheless we have seen that the
batteries on such devices currently do not withstand
too long for some real world mobile health solutions.
Cloud computing appears as an emerging solution
for the remote processing of data. But simply
sending all data to the cloud is inviable because of
security, network and cost issues. There should be a
tradeoff between local and remote processing of
data. Hence, an important issue to mobile health care
solutions relies on developing a way to determine
which sets of information can be processed locally
by the device and which sets of information could be
sent to the cloud for remote processing.
In order to address this tradeoff, we suggest the
development of a model to decide whether some
information is better processed localy or else by the
cloud. The model could comprise a set of variables
(such as data size and type) to tune it for each
application as well as take into account important
network issues, such as latency and cost for both the
infrastructure (computational costs) and the final
users (monetary costs). By monitoring battery
autonomy, application performance, the size and the
nature of the data to be processed and considering
networking issues, one must be able to make this
decision. In a first moment, a static (run-once)
solution could make itself useful for application
developers. Later, a self-learning and more
autonomous solution can be envisioned. Our next
research steps are going in this direction.
We would like to thank the PDTI Program,
financed by Dell Computers of Brazil Ltd. (Law
8.248/91), for sponsoring this research; and our
colleage Sabrina Marczak for reviewing the
manuscript.
REFERENCES
Ahmed, M. and Ahamad, M., 2012. Protecting health
information on mobile devices. In CODASPY '12
Proceedings of the second ACM conference on Data
and Application Security and Privacy.
Al-Taee, M., Jaradat, N., and Ali, D., 2011. Mobile phone-
based health data acquisition system using bluetooth
technology. In AEECT Applied Electrical Engineering
and Computing Technologies.
Alamri, A., 2012. Cloud-based e-health multimedia
framework for heterogeneous network. In ICMEW
Multimedia and Expo Workshops.
Altini, M., Penders, J., and Roebbers, H., 2010. An
android-based body area network gateway for mobile
health applications. In Wireless Health, pp. 188-189.
Barnickel, J., Karahan, H., and Meyer, U., 2010. Security
and privacy for mobile electronic health monitoring
and recording systems. In Proceedings of the
WOWMOM '10 IEEE International Symposium on A
World of Wireless, Mobile and Multimedia Networks.
Barua, M., Liang, X., Lu, R., and Shen, X., 2011. Peace:
An efficient and secure patient-centric access control
scheme for ehealth care system. In INFOCOM
WKSHPS Computer Communications Workshops.
Berndt, R.-D., Takenga, M., Kuehn, S., Preik, P., Sommer,
G., and Berndt, S., 2012. Saas-platform for mobile
health applications. In Systems, Signals and Devices.
Biolchini, J., Mian, P. G., Natali, A. C. C., and Travassos,
G. H., 2005. Sistematic review in software
engineering. Technical Report.
Blobel, B., 2011. Intelligent security and privacy solutions
for enabling personalized telepathology. Diagnostic
Pathology, 6:1–8.
Blumrosen, G., Avisdris, N., Kupfer, R., and Rubinsky,
B., 2011. C-smart: Efficient seamless cellular phone
based patient monitoring system. In Proceedings of
the 2011 WOWMOM IEEE International Symposium
on a World of Wireless, Mobile and Multimedia
Networks.
Catarinucci, L., Colella, R., Esposito, A., Tarricone, L.,
and Zappatore, M., 2012. RFID sensor-tags feeding a
context-aware rule-based healthcare monitoring
system. J. Med. Syst., 36(6):3435–3449.
Chen, Y.-Y., Lu, J.-C., and Jan, J.-K., 2012. A secure
EHR system based on hybrid clouds. Journal of
Medical Systems, 36(5):3375–3384.
Chi, Y. M., Ng, P., Kang, E., Kang, J., Fang, J., and
Cauwenberghs, G., 2010. Wireless non-contact cardiac
and neural monitoring. In WH '10 Wireless Health.
ICEIS2013-15thInternationalConferenceonEnterpriseInformationSystems
524

Constantinescu, L., Kim, J., and Feng, D. D., 2012.
Sparkmed: A framework for dynamic integration of
multimedia medical data into distributed m-health
systems. Trans. Info. Tech. Biomed., 16(1):40–52.
Du, Y., Chen, Y., Wang, D., Liu, J., and Lu, Y., 2011. An
Android-based emergency alarm and healthcare
management system. In 2011 International
Symposium on IT in Medicine and Education.
Fernandes, B., Afonso, J., and Simoes, R., 2011. Vital
signs monitoring and management using mobile
devices. In (CISTI) Information Systems and
Technologies.
Gomes, A. T. A., Ziviani, A., Correa, B. S. P. M.,
Teixeira, I. M., and Moreira, V. M., 2012. Splice: a
software product line for healthcare. In Proceedings
of the 2
nd
ACM SIGHIT International Health
Informatics Symposium.
Heslop, L., Weeding, S., Dawson, L., Fisher, J., and
Howard, A., 2010. Implementation issues for mobile-
wireless infrastructure and mobile health care
computing devices for a hospital ward setting. In
Journal of Medical Systems, 34:509–518.
Hewage, C. T. E. R., Martini, M. G., and Khan, N.,2011.
3d medical video transmission over 4g networks. In
Proceedings of the 4th International Symposium on
Applied Sciences in Biomedical and Communication
Technologies.
Hsieh, J.-c. and Hsu, M.-W., 2012. A cloud computing
based 12-lead ECG telemedicine service. BMC
Medical Informatics and Decision Making, 12(1):77.
Ivanov, I., Gueorguiev, V., Bodurski, V., and Trifonov,
V., 2010. Telemedicine and smart phones as medical
peripheral devices (computational approaches). In
Developments in E-systems Engineering (DESE).
Jersak, L. C., Costa, A. C., Callegari, D. A., 2013. A
systematic review on mobile health care. PUCRS
Tecnical Report TR 073. Available at:
http://www3.pucrs.br/portal/page/portal/facinppg/ppgc
c/ppgccRelatoriosTecnicos.
Kitchenham, B., 2004. Procedures for performing
systematic reviews. Joint Technical Report. Keele
University Technical Report.
Kyriacou, E., Constantinides, P., Pattichis, C., Pattichis,
M., and Panayides, A., 2011. Emergency health care
information systems. In Engineering in Medicine and
Biology Society, EMBC.
Lagerspetz, E. and Tarkoma, S., 2011. Mobile search and
the cloud: The benefits of offloading. In Pervasive
Computing and Communications Workshops.
Lara, O. D., Perez, A. J., Labrador, M. A., and Posada, J.
D., 2012. Centinela: A human activity recognition
system based on acceleration and vital sign data.
Pervasive and Mobile Computing, 8(5):717 – 729.
Le, X. H., Sankar, R., Khalid, M., and Lee, S., 2010.
Public key cryptography-based security scheme for
wireless sensor networks in healthcare.In Proceedings
of the 4th International Conference on Uniquitous
Information Management and Communication,
ICUIMC '10.
Lin, F. X., Rahmati, A., and Zhong, L., 2010. Dandelion:
a framework for transparently programming phone-
centered wireless body sensor applications for health.
In Wireless Health 2010, WH '10.
Liu, C., Zhu, Q., Holroyd, K. A., and Seng, E. K., 2011.
Status and trends of mobile-health applications for iOS
devices: A developer's perspective. In Journal of
Systems and Software, 84(11):2022–2033.
Mashima, D. and Ahamad, M., 2012. Enhancing
accountability of electronic health record usage via
patient-centric monitoring. In Proceedings of the 2nd
ACM SIGHIT International Health Informatics
Symposium, IHI '12.
Masse, F., Penders, J., Serteyn, A., van Bussel, M., and
Arends, J., 2010. Miniaturized wireless ecg-monitor
for real-time detection of epileptic seizures. In
Wireless Health 2010, WH '10, pages 111–117, New
York, NY, USA. ACM.
Oates, B. J. B., 2006. Researching information systems
and computing. SAGE Ed.
O'Brien, H., Van de Ven, P., Nelson, J., and Bourke, A.,
2010. Smart phone interfaces to wireless health
sensors. In International Conference on e-Health
Networking Applications and Services (Healthcom).
Pandey, S., Voorsluys, W., Niu, S., Khandoker, A., and
Buyya, R., 2012. An autonomic cloud environment for
hosting ecg data analysis services. In Future
Generation Computer Systems, 28(1):147 – 154.
Pereira, O., Caldeira, J., and Rodrigues, J., 2011. Body
sensor network mobile solutions for biofeedback
monitoring. In Mobile Networks and Applications,
16:713–732.
Pigadas, V., Doukas, C., Plagianakos, V. P., and
Maglogiannis, I., 2011. Enabling constant monitoring
of chronic patient using Android smart phones. In
Proceedings of the 4th International Conference on
Pervasive Technologies Related to Assistive
Environments, PETRA '11.
Rahbar, A., 2010. An E-ambulatory healthcare system
using mobile network. In Proceedings of Seventh
international conference on information technology.
pp 1269-1273.
Siebra, C., Lino, N., Silva, M., and Siebra, H., 2011. An
embedded mobile deductive system for low cost health
monitoring support. In International Symposium on
Computer-Based Medical Systems (CBMS).
Soomro, A. and Schmitt, R., 2011. A framework for
mobile healthcare applications over heterogeneous
networks. In International Conference on e-Health
Networking Applications and Services (Healthcom).
Warren, I., Weerasinghe, T., Maddison, R., and Wang, Y.,
2011. Odintelehealth: A mobile service platform for
telehealth. In The 2nd International Conference on
Ambient Systems, Networks and Technologies.
World Health Organization, 2011. Global observatory for
ehealth series: mHealth: new horizons for health
through mobile technologies. Vol 3. 111 pp.
TechnicalTrendsandChallengesinMobileHealth-ASystematicReviewofRecentAvailableLiterature
525
