
Decision Making for Patients with Asymptomatic Severe Aortic
Stenosis
The Case for Preemptive Aortic Valve Replacement Surgery
Tulvio S. Durand
BSEE, Villanova University, Math/Science Teaching Credentials, University of California,
San Diego, Resident of Anza, CA, U.S.A.
Keywords: Asymptomatic, Aortic Stenosis, Aortic Valve Replacement, Decision Making.
Abstract: Aortic stenosis disease typically progresses from mild to severe as patients age beyond 50, during which
time patients are generally asymptomatic and their quality of life will remain similar to that of the general
population. Most patients with Asymptomatic Severe Aortic Stenosis (ASAS) will develop one or more
symptoms of angina, dyspnea, or syncope within five years. As there is no medicinal cure for the disease,
these newly symptomatic patients will require Aortic Valve Replacement (AVR) surgery soon after onset of
symptoms because without it 75% of them will die within three years from the first symptoms onset. The
proper treatment of ASAS patients before they become symptomatic is subject to debate. The American
College of Cardiology and American Heart Association (ACC/AHA) recommend “watchful waiting” for the
onset of symptoms after which they recommend AVR surgery. Review of results of studies based on
recently improved surgical outcomes indicate that preemptive AVR surgery before onset of symptoms
produces vastly improved survivability compared to the watchful-waiting protocol. ACC/AHA guidelines
for treatment of severe aortic stenosis accordingly should be modified to reflect this new reality by
recommending early AVR surgery in place of watchful waiting for most all ASAS patients.
1 INTRODUCTION
The proper treatment of Asymptomatic Severe
Aortic Stenosis (ASAS) patients during the
asymptomatic period is controversial. Though the
cardiologist knows from testing that AVR surgery
will soon be needed, the patient is reluctant to have
surgery because he does not experience symptoms.
The cardiologist is also reluctant to recommend
surgery because of the operative mortality risk
which until recently was substantial. Consequently
the American College of Cardiology and American
Heart Association (ACC/AHA) recommend (in
Bonow, R., Carabello, B., et al. 2006) “watchful
waiting” for the onset of symptoms before
considering Aortic Valve Replacement (AVR). But
if onset of symptoms is not quickly recognized and
acted upon the patient is subject to sudden death, as
is explained in the Section 2 discussion that follows.
Cardiology researchers have been seeking an
indicator or combination of indicators that can
reliably signal when onset of symptoms is imminent
so that early AVR surgery in such patients may be
warranted, especially when very low surgical
mortality risk is expected. Operative mortality risk
in a high volume AVR surgical theater with highly
experienced surgeons is now typically 1% to 2% for
isolated AVR surgery and 3% to 5% for more
complex AVR surgery as reported in Egrie et al.,
(2010) and Stanford SHC (2013). Complex AVR as
used herein involves one or more of: repair and/or
replacement of multiple heart valves, coronary
bypass, or debridement of a heavily calcified aortic
valve, in addition to AVR.
Review of event-free survival data from one
large study presented and discussed in Section 3
indicates astoundingly large 43% mortality is
experienced with those ASAS patients during the
watchful-waiting period of five years. With such
large attrition, the question that comes to mind is
how many of those ASAS patients who died during
watchful waiting would have survived had all them
been given, and all accepted, the option of having
early AVR surgery in today’s expected low
operative mortality risk for this surgical procedure?
49
S. Durand T..
Decision Making for Patients with Asymptomatic Severe Aortic Stenosis - The Case for Preemptive Aortic Valve Replacement Surgery.
DOI: 10.5220/0004615000490056
In Proceedings of the International Congress on Cardiovascular Technologies (CARDIOTECHNIX-2013), pages 49-56
ISBN: 978-989-8565-78-5
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)
Accordingly, the watchful-waiting data from this
and other studies is reanalyzed in Section 3 to yield
predicted survival percentages for both 2% and 5%
operative mortality risk for AVR surgery. Predicted
survival from early AVR surgery is shown to be
vastly superior to survival from watchful waiting.
Moreover, the data from a recent study is very
significant and unique because it directly compares
actual AVR surgery survival to watchful waiting
survival of ASAS patients. The AVR surgery
subgroup of patients experienced significantly
superior survival compared to the subgroup of
patients in watchful waiting. Finally, in two separate
studies of elderly patients, long term survival of
ASAS patients is compared between those who had
AVR surgery with those who were in watchful
waiting and did not have AVR surgery. The long
term survival of patients who underwent AVR
surgery was again vastly superior in both studies.
Moreover their long term survival was also
significantly superior to the survival of the referent
general population when matched for age and
gender.
These results make a strong case for changing
the recommended treatment protocol for ASAS
patients. In other words, the time has come for the
ACC/AHA to reconsider their position on the
treatment of asymptomatic patients with severe or
extremely severe aortic stenosis and recommend
early AVR surgery for most all such patients.
Exceptions might include patients with significant
comorbidities like cancer.
It should be noted throughout this paper that
advocacy for AVR surgery treatment of ASAS
patients applies equally to asymptomatic patients
who have very severe or extremely severe aortic
stenosis. Asymptomatic severe aortic stenosis
(ASAS) and asymptomatic extremely severe aortic
stenosis are defined in Table 1, Section 2.
Asymptomatic very severe aortic stenosis
designation and criteria for its designation may vary
by author. This topic is expanded when treating such
data and is further discussed in Section 3.
2 DISCUSSION
The American College of Cardiology and American
Heart Association (ACC/AHA) have jointly issued
severity-grading criteria of aortic stenosis as well as
provided guidelines for aortic valve replacement
(Bonow, 2006). A succinct restatement of
ACC/AHA’s severity grading of aortic stenosis is
shown in Table 1, and summary restatement of its
guidelines for asymptomatic patients are excerpted
and restated below Table 1. Note also that Table 1
and AVR guidelines are the result of combining
separate data in Bonow et al., (2006 pp. 97, 101, 107
and 120).
Table 1: ACC/AHA grading of aortic stenosis.
EXTREMELY
SEVERE
SEVERE MODERATE MILD
Jet velocity
(m/s)
>5.0 >4.0 3.0-4.0 <3.0
Mean aortic
gradient (mm
Hg)
>60 >40 25-40 <25
Aortic valve
area (cm
2
)
<0.6 <1.0 1.0-1.5 >1.5
Indexed*
aortic valve
area (cm
2
/m
2
)
- <0.6 - -
*indexed to patient’s body surface area
The corresponding ACC/AHA guidelines
from
Bonow et al., (2006) regarding advisability of AVR
in asymptomatic aortic stenosis patients are as
follows:
1. AVR may be considered for asymptomatic
patients with severe aortic stenosis and any of the
following:
- An abnormal response to exercise.
- A high likelihood of rapid progression of aortic
stenosis disease.
- When surgery might be delayed at the time of
symptom onset.
2. AVR may also be considered for asymptomatic
patients with extremely severe aortic stenosis and
when the patient’s expected operative mortality
is 1.0% or less.
The protocol expressed in these guidelines for
treatment of ASAS patients is commonly referred to
in the literature as watchful waiting, in which the
patient is medicinally treated and periodically
monitored or tested for the onset of symptoms. It is
important to note that these ACA/AHA guidelines
from Bonow et al., (2006) are based on older pre
2000 valve-prosthesis technology and AVR surgical
outcomes that have since greatly improved. For
example ACA/AHA guidelines in Bonow et al (2006
p. 108) quotes the average perioperative mortality
values thusly: “3% to 4% for isolated AVR, 8.8%
mortality for AVR in patients over age 65 which can
also reach 13% mortality in low-volume AVR
centers”. These mortality percentages have been at
least halved in recent practice as can be seen, for
example, in Egrie et al., (2010) and Stanford (2013)
CARDIOTECHNIX2013-InternationalCongressonCardiovascularTechnologies
50
and in the two studies of AVR in the elderly patients
reported in Section 3.3. Moreover ACA/AHA
properly anticipated this progress where they state in
Bonow et al (2006 p. 109) “… as improved valve
substitutes are developed and methods of valve
replacement become safer, the risk-benefit balance
may change to favor earlier intervention in aortic
stenosis”. It appears that the time for favoring and
recommending earlier AVR intervention has arrived.
2.1 The Problem with
Watchful-waiting Protocol
The big problem with watchful-waiting protocol as
deduced from data presented and discussed below is
that a significant percentage of ASAS patients
routinely die from the underlying aortic stenosis
disease during watchful waiting that would have
survived if they had they had undergone early AVR
surgery before the onset of symptoms. The same
logic applies to asymptomatic patients with extreme
aortic stenosis, as they should be recommended for
immediate AVR surgery, asymptomatic or not.
Supporting this position are the results from four
studies described in Section 3 that compare survival
rates from watchful waiting to predicted and actual
results of early AVR. But before delving into the
results of the studies it is important to note that
survivability is reduced from three causes: aortic
stenosis disease, normal aging effects, and mortality
risk associated with AVR surgery. An overview of
survivability versus age and the impact of onset of
aortic stenosis symptoms on survivability are each
illustrated in Figure 1.
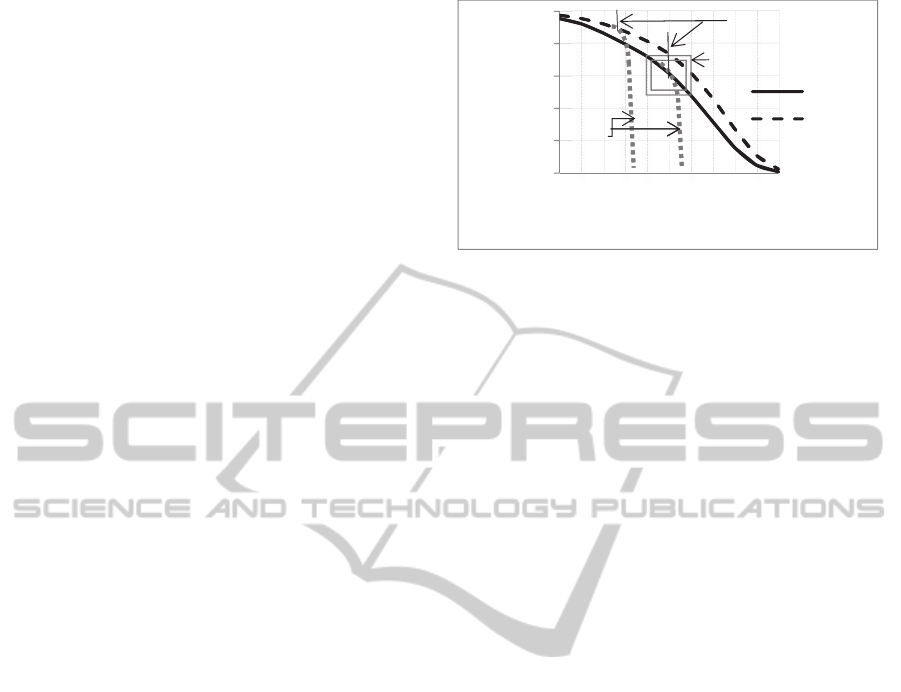
Gender-specific survivor curves of the general
population based on 2007 U.S life expectancy data
obtained from the Life Expectancy Calculator
(2013) are depicted in Figure 1. For example, 91.2%
females aged 60 are survived to the present from
the100% of that group when born. The
corresponding percentage survivors for males aged
60 is 85.2%. The studies of Carabello (2012), Shah
(2012), and others agree that ASAS patients have
approximately equal life expectancy as the general
population during the time they remain
asymptomatic. After onset of symptoms the life
expectancy of symptomatic patients with aortic
stenosis nosedives as is illustrated by the two dotted
“no-surgery” lines, with the result that three quarters
of those patients die within three years if they do not
undergo AVR surgery, according to Carabello
(2012) and Shah (2012).
Figure 1: General Population Average Survival versus
Age and Illustrated Effect of Symptoms Onset on Survival
without AVR Surgery. (The “No Surgery” data was
adapted from Shah (2012, Fig.1A, p. 2).
2.2 “Watchful Waiting” Makes the
ASAS Patient a Ticking Time
Bomb
The onset of symptoms has to be detected early and
reported quickly to the monitoring cardiologist. The
penalty for not promptly undergoing AVR surgery
after first onset of symptoms is the loss of 2%
survivability for every month of delay according to
Carabello (2012). Realize that the latter penalty for a
one-month delay equates or exceeds to the 30-day
mortality risk of 1% to 2% for isolated AVR
surgery, the latter is based on operative mortality
risk data of Egrie et al., (2010) and others. Early
detection and prompt reporting of the onset of
symptoms is not only vitally important, it is also
difficult to achieve outside the clinically controlled
environment of hospital or health clinic for various
reasons, including those reasons described in 2.2.1 -
2.2.4.
2.2.1 Onset of Symptoms is often Masked
Recalling that ASAS patients enjoy the same quality
of life as the general population while they are
asymptomatic, there is a natural tendency for them
to deny the existence and seriousness of symptoms
once they do occur. Bonow (2006, p. 103) adds “It
is important to emphasize that symptoms may be
subtle and often are not elicited by the physician in
taking a routine clinical history”.
2.2.2 Sedentary and Low-aerobic Demand
Sports and Routine Yard Work do not
Produce Symptoms
A physically inactive ASAS patient will frequently
not recognize the onset of symptoms because of lack
0
20
40
60
80
100
40 60 70 80 90 100
%SURVIVORS
AGE
Male
Female
No
Surgery
Symptoms
Onset
Fig. 2
DecisionMakingforPatientswithAsymptomaticSevereAorticStenosis-TheCaseforPreemptiveAorticValve
ReplacementSurgery
51

of the type of exercise that would unequivocally
bring on the symptom; example activities that don’t
produce symptoms are card playing, watching TV,
and watering the roses. Also, golfing from a golf cart
is generally not sufficiently aerobic to bring about
symptoms of progressing aortic stenosis disease.
2.2.3 Advancing Age and Medications often
Produce Similar Symptoms
Dyspnea symptoms of extreme shortness of breath,
tiredness and feelings of exhaustion following
exercise are often and incorrectly attributed to
advancing age. Angina can sometimes be confused
with expected muscular soreness from repetitive
types of yard work. Syncope can be confused with
expected side effects of medications being taken for
hypertension and other health problems.
2.2.4 Physical Intensity and Performance
Level in Sports and Work are often
Lowered in the Face of
Symptom-related Declining
Capabilities
A tennis player, for example, will often opt to make
the games and points shorter when he becomes
extremely tired and may play less often to mask a
loss of vigor from what the player thinks are simply
the vagaries of advancing age. This same adaptive
behavior can also mask the real onset of symptoms
of aortic stenosis disease.
Clearly there is a need for educating all aortic
stenosis patients on what to watch for and to
immediately report suspected onset of symptoms.
“Valve Clinics” should be established at hospitals
where aortic stenosis patients can be educated and
more closely monitored during watchful waiting.
Exercise stress tests should be periodically
employed for all ASAS patients in clinical settings
to see if they produce symptoms. The stress test is
often intentionally avoided by cardiologists for fear,
mostly unsupported, that it can bring on heart
failure, and is of itself yet another reason that
symptoms are sometimes not recognized early
enough to keep mortality rates low. Suffice it to say
that watchful waiting for onset of symptoms is a
dangerous protocol for ASAS patients. It will be
shown herein that a much safer alternative to
watchful waiting is early AVR surgery. But it is to
be expected that watchful-waiting protocol will not
be abandoned anytime soon, so care must be
exercised to make it work as well as possible.
2.3 The AVR Surgery Option
There are two categories of AVR cardiac surgery
considered herein: Isolated AVR surgery and more
involved or what is referred in this paper as complex
AVR surgery. Isolated AVR surgery involves the
removal and replacement of the aortic valve only
and is usually performed using minimally invasive
surgery techniques. The 30-day expected mortality
risk from Isolated AVR is 1% to 2% as
demonstrated in Egrie (2010), Stanford (2013),
Kang (2010) and Varadajaran (2006), and depends
on the experience of the surgical team and AVR
surgery volume of the hospital; the more
conservative 2% is used herein in survivability
calculations for Isolated AVR surgery. Complex
AVR surgery can involve surgical repair and/or
replacement of multiple heart valves, coronary
bypass, debridement of a heavily calcified aortic
valve, and a host of other cardiovascular surgical
procedures in addition to AVR. The 30-day expected
mortality from complex AVR is 3% to 5%
also as
demonstrated in Egrie et al., (2010) and Stanford
(2013) depending on the experience of surgical team
and AVR volume of the hospital; the more
conservative 5% is used in survivability calculations
herein. As a point of interest, Isolated AVRs
constituted about one-half of the 2532 total AVRs
performed by one surgical group during the 11 year
period 1998-2008 as reported in Egrie (2010, p. 16).
Survivability from the Isolated AVR surgery
option with 30-day 2% mortality risk is illustrated in
Figure 2.
Note that all calculations that follow are
based on male life expectancy only, which is the
more conservative choice since male life expectancy
is shorter.
A portion of the General Population Survivors
(solid black line) is replicated from the small
rectangular area in Figure 1 spanning the ages 74.5
years to 76.5 years. That line shows the expected
decline of the male general population survivors
from aging factors alone based on Life Expectancy
Calculator (2013). At age 75, for example, 61.6% of
all males are survived, and at age 76 the male
survivors reduces to 59.2% in nearly linear fashion.
Assume, for the following discussion, that a
group of 100 ASAS male patients all aged 75 opt to
have Isolated AVR surgery for which the expected
30-day operative mortality risk is 2%. Those
patients’ 2% mortality risk is comprised of 1.67%
mortality risk from surgery (line pointed down) and
0.33% mortality risk from normal aging effects on
the general population during the 30-day
postoperative period (shown by very short line
CARDIOTECHNIX2013-InternationalCongressonCardiovascularTechnologies
52

segment parallel to the general population aging
line). Of the initial 100 ASAS patients, two of them
do not survive AVR surgery (dotted arrow facing
down towards 0%). The remaining 98 are all
survivors (arrow pointed up), and they rejoin the
general population group in life expectancy (parallel
lines shown for clarity only). Importantly, the AVR
surgery survivors can expect at least the same, and
possibly greater life expectancy compared to that of
the general population as is reported in the two AVR
survival studies in Section 3.3.
The more complex AVR surgery with 30-day
mortality risk of 5% is similarly represented by
Figure 2, except the mortality dip would be 3%
larger. But the 95% surgery survivors are also
expected to attain equal or better life expectancy
compared to the general population as is discussed
in Section 3.
2.4 The ASAS Patient Asks: Which is
Less Risky, Watchful Waiting or
Early AVR Surgery?
At a minimum, the informed views of the patient
should be considered along with those of the
cardiologist and cardiothoracic surgeon.
Accordingly, the ASAS patient should be informed
that he has two options: (1) watchful waiting for
symptoms, after which his/her survival percentage
decreases by 2% per month
according to Carabello
(2012), or (2) Isolated AVR surgery for which there
is a 30-day mortality risk of 2%. Also the patient
should be informed it is not unreasonable to expect
that it could take up to three months or so from
actual symptoms onset (as opposed to delayed
recognition of symptoms onset) to the time of being
wheeled into the operating room for AVR surgery,
so that option (1) could incur up to three times more
mortality risk compared to option (2).
It should also be noted that the Isolated AVR
operative mortality risk 2% could equate to only a
fraction of the yearly mortality risk from aging. For
example the general-population male on his 75
th
birthday has a 4% probability of dying before age
76. Isolated AVR surgery adds only 1.67% mortality
risk which is equivalent to 6 months’ (or 4.7%) loss
in life expectancy. However, to a 40 year male the
2% operative mortality risk equates to about 6.72
years (or 18%) loss of life expectancy, and is
therefore a decision that should not be taken lightly.
Isolated AVR operative mortality risk of < 1%
remains a highly desirable goal especially for
younger, < 55-year patients.
3 STUDIES COMPARING
WATCHFUL WAITING TO
AVR SURGERY
The principal source of survival data from watchful-
waiting protocol treatment of asymptomatic patients
with aortic stenosis disease comes from eight studies
that are aggregated in Bonow et al., (2006, p.104).
Of those only the Pellikka et al., (2005) study is
examined herein because of its being the largest,
comprising over ½ of the total patients, all of whom
were asymptomatic with severe aortic stenosis
disease, and it alone provides results in sufficient
detail relating to the issue of relative efficacy of
watchful waiting protocol compared to early AVR
surgery.
3.1 Pellikka et al., (2005) Watchful
Waiting Study
622 ASAS patients, average age 72 years, Vmax ≥
4.0 m/s, were followed up for a period of five years.
The patients were reevaluated at intervals of six
months or one year and they were told to report
promptly for reevaluation at onset of symptoms.
Those with verified symptoms were recommended
for AVR surgery. A summary of results pertinent to
the present study is shown in Figure 3. Of particular
interest is that by the end of the five-year study
period 265 (43%) patients died and 357 (57%)
patients survived; also of the 352 patients who did
undergo AVR surgery 86 (24%) died.
If at the beginning of the study all 622 patients
had available to them and all opted for AVR, with
either the 2% operative risk for Isolated AVR
surgery or the 5% operative mortality risk associated
with complex AVR (defined in Section 2.3), their
predicted 5-year survival rates would have been 81%
and 78% respectively. These are both markedly
superior to the 57% survival rate actually
experienced. Far fewer patients would have died:
118 for Isolated AVR and 134 for complex AVR,
fatality numbers that are about one-half the 265 total
deaths experienced. Yet, these results are not too
surprising when considering that the results of the
Pellikka (2005) retrospective study represent 24
year-old (1984-1995) AVR surgical and valve
prosthesis technologies. Also as noted above, the
mortality rate for those who elected to undergo AVR
surgery was an abysmally large 24%. It is not
surprising then that, as shown in Figure 3, 90
patients (30%) opted not to have AVR surgery even
after their having developed deadly symptoms.
DecisionMakingforPatientswithAsymptomaticSevereAorticStenosis-TheCaseforPreemptiveAorticValve
ReplacementSurgery
53
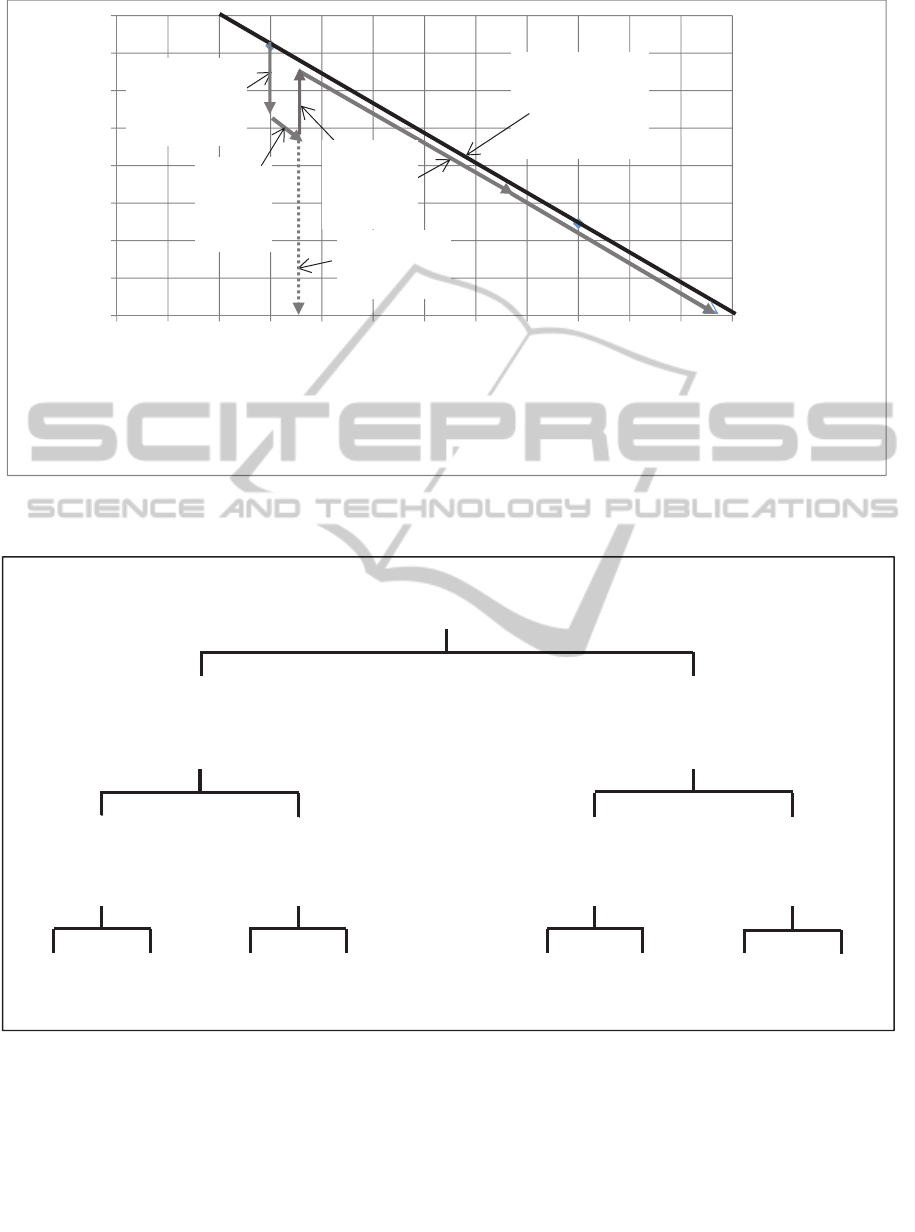
Figure 2: Illustration of Isolated AVR Surgical Option with 30-Day 2% Operative Mortality for a Group of 100 Male
Patients All Aged 75 years.
Figure 3: Distribution of Patients Who Developed Symptoms, Did Not Develop Symptoms, Underwent AVR Surgery,
Survived or Died over the Five Year Study Period; from Pellikka et al., (2005, p. 4, Figure 2 with modified wording).
Pellikka et al., (2005, p. 6) similarly sensed this
reality by stating “Early referral to aortic valve
surgery, even in the asymptomatic patient, probably
would have improved survival”.
3.2 Kang et al., (2010) Study Comparing
Early AVR Actual Surgery Survival to
Watchful Waiting Survival
A noteworthy recent study by Kang et al., (2010)
uniquely compares early AVR actual surgery results
58,0
58,5
59,0
59,5
60,0
60,5
61,0
61,5
62,0
74,6 74,8 74,10 75,0 75,2 75,4 75,6 75,8 75,10 76,0 76,2 76,4 76,6
%SURVIVORS
AGE[Yr,Mo's]
The2%Surgery‐
Non‐survivors
General
Population
% Survivors
Surgery‐
OptingASAS
Patients
The98%
Surgery
Survivor
s
30‐Day
Aging
Mortality
45
died
162
survived
76
died
14
survived
41
died
104
survived
103
died
77
survived
622PATI ENTS
297develop
symptoms
325re ma i n
asymptomatic
207have
surgery
90no
surgery
145have
surgery
180no
surgery
CARDIOTECHNIX2013-InternationalCongressonCardiovascularTechnologies
54

against conventional treatment (watchful waiting)
results in a group of 197 asymptomatic very severe
aortic stenosis patients. That group was split into
two subgroups, one slated for early AVR surgery
and the other subgroup for traditional watchful
waiting. Very severe aortic stenosis is defined by the
authors as “a critical stenosis in the aortic valve,
area ≤ 0.75 cm
2
, accompanied by either a peak
aortic jet velocity ≥ 4.5 m/s or a mean transaortic
pressure gradient ≥ 50 mm Hg. There were no
significant differences between the two subgroups in
terms of age, gender, or LV ejection fraction”. AVR
surgery was performed on 102 patients and
conventional treatment [ed. watchful waiting] was
employed for the other group of 95 patients whose
mean age was 63.
The authors (Kang et al., 2010, p. 1, Abstract)
state “During a median follow-up of 1501 days the
operated group had no operative mortalities, no
cardiac deaths, and 3 non-cardiac deaths; the
conventional treatment [ed. watchful waiting] group
had 18 cardiac deaths and 10 non-cardiac deaths”.
Admittedly this is a small study, but the results
nevertheless are very compelling. Early, or
preemptive, AVR surgery won hands down
compared to watchful waiting. Additional
comparative experimental studies to validate these
results are recommended.
3.3 Two Studies of Elderly Patients
with Severe Aortic Stenosis
Comparing their Long-term
Survival from AVR Surgery to
No-AVR (Watchful Waiting) and to
a Control Group
These are two important studies for two reasons:
(1) They directly compare the long term survival of
(A) Severe Aortic Stenosis (SAS) patients who
underwent AVR surgery to (B) SAS patients in
watchful waiting who did not have AVR surgery,
and to (C) control group of U.S. general population
that is matched for age and gender.
(2) Elderly patients with severe aortic stenosis are
often denied AVR surgery because of their advanced
age. Both studies’ results, shown below, strongly
refute the advanced-age argument.
The respective results of the two studies, by
Varadajaran and Kapoor, (2006) and Egrie and
Gaudiani, (2010) are shown in Table 2.
Table 2: Elderly SAS patients’ long-term survival
comparison with AVR, No-AVR, and control group.
Varadajaran, et al.,
(2006)
1 year 2 year 5 year
US GP 85 year Male 89% 79% 50%
AVR Group (n = 55) 87% 78% 68%
No-AVR (n= 222) 52% 40% 22%
Egrie et al., (2010) 1 year 2 year 5 year
US Age and Gender
Matched, ≥ 75 years
89% 79% 51%
Isolated-AVR (n = 371) 91% 87% 67%
No-AVR Group (n = ?) 65% 41% 8%
3.3.1 Varadajaran et al., (2006) Elderly
ASAS Patients, Aged 85 ± 4 Years,
AVR Long-term Survival Study
277 ASAS patients, 85 ± 4 years had aortic valve
area < 0.84 cm
2
in this retrospective study. The 1, 2,
and 5 year survival percentages of the AVR group
are vastly superior to the No-AVR group, and the 5-
year survival of the AVR group is also significantly
superior to the reference US general population 85-
year male expected survival per the U.S. Life
Expectancy Calculator (2013).
3.3.2 Egrie et al., (2010) Elderly, Age > 75
Years, Isolated-AVR Surgery
Long-term Survival Study
371 aortic stenosis patients aged 75 and over
underwent Isolated AVR surgery from 2004 to 2008
and were followed through 5 years after surgery.
Importantly, it should be noted that all 371 patients
were screened to be free of coronary disease or
cancer, otherwise they would not have been selected
for Isolated AVR surgery. The 1, 2, and 5 year
survival percentages of the Isolated-AVR surgery
group are greatly superior to corresponding
percentage survivors in the No-AVR group.
Moreover, the 2 and 5 year Isolated-AVR survival
percentages also are significantly superior to the age
and gender matched U.S. general population.
4 CONCLUSIONS
1. Predicted and actual survival from preemptive
early AVR surgery with either 2% or 5% operative
mortality risk are shown to be overwhelmingly
superior compared to watchful-waiting protocol in
studies of 717 asymptomatic severe aortic Stenosis
(ASAS) patients.
DecisionMakingforPatientswithAsymptomaticSevereAorticStenosis-TheCaseforPreemptiveAorticValve
ReplacementSurgery
55

2. Actual long-term survival of 426 elderly, 75-90
year old patients with severe aortic stenosis who
underwent AVR surgery is vastly superior to
survival of those similarly afflicted patients without
AVR surgery; and their survival rates are also
significantly superior to expected survival of age and
gender-adjusted general population control group.
3. ACC/AHA 2006 Guidelines
in Bonow (2006) for
management of aortic stenosis disease should be
revised to recommend preemptive early AVR
surgery when aortic stenosis disease has progressed
to their defined “severe” level regardless of whether
the patient is symptomatic or asymptomatic.
4. Mortality risk from just a single month of
watchful waiting after onset of aortic stenosis
symptoms equates or exceeds the 30-day 1% to 2%
operative mortality risk from Isolated AVR surgery.
5. Onset of symptoms from aortic stenosis disease
is often masked causing delayed detection. Also,
symptoms are sometimes mistaken for benign
effects of ageing, and are sometimes not promptly
communicated to the monitoring cardiologist. Such
delays increase mortality risk by 2% per month, one
month of which equates or exceeds the 1% to 2%
operative mortality risk of Isolated AVR surgery.
6. ASAS patients should be thoroughly apprised of
the vastly superior probable survival from early
AVR surgery compared to the more risky watchful-
waiting protocol. Moreover, advanced age should,
by itself, never be reason to preclude AVR surgery.
REFERENCES
Bonow, R., Carabello, B., Chatterjee, K., Faxon, D.,
Freed, M., Gaasch, W., Lytle, B., Nishimura, R.,
O’Gara, P., O’Rourke, R., Otto, C., Shah, P.,
Shanewise, J. 2006. ACC/AHA 2006 guidelines for
the management of patients with valvular heart
disease: a report of the American College of
Cardiology/American Heart Association Task Force
on Practice Guidelines. Circulation. 2006;114:e84 –
e231. DOI:10.1161/CIRCULATIONAHA.106.176857
Carabello, B. 2012. Should Severe Aortic Stenosis Be
Operated on Before Symptom Onset?: Aortic Valve
Replacement Should Be Operated on Before Symptom
Onset. 2012. [Internet] Available from:
<http://circ.ahajournals.org/content/126/1/112.full>
[Accessed 7 April 2013].
Egrie, E., Gaudiani, V., Mitruka, S., Oka, T., Shah, S.,
Spowart, G., Tsau, P., Vial, C. 2010. Adult Cardiac
Surgery Results. 2010. Pacific Coast Cardiac &
Vascular Surgeons 2010 Edition. [Internet]. Available
from: <http://www.pccvs.com/files/documents/PAC_
Cardio_Brochure_R1.pdf> [Accessed 8 April 2013].
Kang, D., Park, S., Rim, J., Yun, S., Kim, D., Song, J.,
Choo, S., Park, S., Song, J., Lee, J., Park, P. 2010.
Early surgery versus conventional treatment in
asymptomatic very severe aortic stenosis. Circulation.
2010;121:1502–1509.
Life expectancy calculator. 2013. [Internet]. Available
from <http://life-span.findthedata.org/> Data is based
on 2007 period-life table for the Social Security area
population. [Accessed 7 April 2013].
Pellikka, P., Sarano, M., Nishimura, R., Malouf, J., Bailey,
K., Scott, C., Barnes, M., Tajik, A. 2005. Outcome of
622 adults with asymptomatic, hemodynamically
significant aortic stenosis during prolonged follow-up.
Circulation. 2005;111:3290–3295.
Shah, P. 2012. Severe Aortic Stenosis Should Not Be
Operated on Before Symptom Onset (Part ll of a 2-part
article). Circulation: Volume 126(1)3 July 2012 p
118–125.
Stanford, SHC. 2013. Stanford Surgical Outcome Reports
for Isolated AVR, page 4 of 6. 2013. Stanford School
of Medicine. [Internet]. Available from
<http://ctsurgery.stanford.edu/patient_care/outcomes2.
html#isoAVR> [Accessed 7 April 2013].
Varadarajan, P., Kapoor, N., Bansal, R., Pai, R. 2006.
Survival in elderly patients with severe aortic stenosis
is dramatically improved by aortic valve replacement:
Results from a cohort of 277 patients aged ≥ 80 years.
Eur J Cardiothorac Surg. 2006 Nov 30(5):722-7.
CARDIOTECHNIX2013-InternationalCongressonCardiovascularTechnologies
56
