
Virtual Arm Representation and Multimodal Monitoring
for the Upper Limb Robot Assisted Teletherapy
Gorka Epelde
1
, Xabier Valencia
2
, Aitor Ardanza
1
, Elsa Fanchon
1
, Alessandro De Mauro
1
,
Francisco Molina Rueda
3
, Eduardo Carrasco
1
and Shabs Rajasekharan
1
1
eHealth & Biomedical Applications, Vicomtech-ik4, Mikeletegi Pasealekua 57, 20009 San Sebastián, Spain
2
EGOKITUZ: Laboratory of HCI for Special Needs, School of Informatics,
University of the Basque Country / Euskal Herriko Unibertsitatea,
Manuel Lardizabal 1, 20018 Donostia, San Sebastian, Spain
3
Biomechanics and Motor Control Laboratory LAMBECOM, Faculty of Health Sciences, Rey Juan Carlos University,
Calle Tulipán s/n, 28933 Móstoles, Madrid, Spain
Keywords: Armeo Spring, Exoskeleton, Rehabilitation Robots, Virtual Reality, Realistic Virtual Reality, Multimodal
Monitoring, Online Assessment, Upper Limb, Virtual Arm Representation.
Abstract: The use of technology in rehabilitation therapies targets the sustainability of health systems and the
improvement of quality of life of the user (therapists, patients and informal carers). Robot or exoskeleton
assisted rehabilitation systems, which are based on neurorehabilitation principles, are tools that not only
help patients move the arm with precision; they also help reduce the fatigue of the therapist during the
process. One of the challenges of the virtual reality based robot assisted upper limb rehabilitation is patients’
immersion within the therapy to achieve an improved progress of the rehabilitation.
This paper, presents a new virtual reality therapy that has been created using the Armeo Spring exoskeleton.
A 3D representation of the arm serves as an interaction mechanism with the virtual world. This makes the
user more aware of the movements that he/she is making and improves the rehabilitation outcomes. It also
encourages the user motivation and engagement to the therapy. Additionally, an application for the
multimodal monitoring of the patient has been developed, together with tools for the online assessment of
patients. These developments allow the physician to review the therapy without being in the same place and
time, optimizing the use of hospital’s human resources.
1 INTRODUCTION
Cerebrovascular accidents (CVA) and spinal cord
injuries (SCI) are currently the most common causes
of paralysis and paresis with reported prevalence of
12,000 cases per million and 800 cases per million,
respectively. Disabilities that follow CVA
(hemiplegia) or SCI (paraplegia, tetraplegia)
severely impair motor functions (e.g., standing,
walking, reaching and grasping) and prevent the
affected individuals from healthy-like, full and
autonomous participation in daily activities.
Moreover, the societal habits increase the
number of such episodes. The risk factors of the
today’s society are reported by the World Health
Organization at (McKay et al., 2004). Together with
the societal habits, the progressive aging of society
(World Heath Organization, 2011) calls to urgently
find new systems that will help mitigate the effects
of resource demand of such patients on the
healthcare system. In the path to guarantee the
successful implementation, deployment and use of
the solution, these systems should also improve the
quality of life of the involved people (therapists,
patients and informal carers).
One of the possible intervention points to palliate
the burden of healthcare systems is stroke
rehabilitation. Neurorehabilitation is a process that
aims to recover the capabilities to carry out regular
activities, lost by a neurological disease, by re-
learning or by active problem resolution.
Neurorehabilitation is based on the concept of
Neuroplasticity. According to experts, the brain is
able to establish new conections between neurons
69
Epelde G., Valencia X., Ardanza A., Fanchon E., De Mauro A., Molina Rueda F., Carrasco E. and Rajasekharan S..
Virtual Arm Representation and Multimodal Monitoring for the Upper Limb Robot Assisted Teletherapy.
DOI: 10.5220/0004642300690080
In Proceedings of the International Congress on Neurotechnology, Electronics and Informatics (VirtRehab-2013), pages 69-80
ISBN: 978-989-8565-80-8
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

that are able to subtitute lost sinapsis to a greater or
lesser extent. This is usually targeted by repetitive
therapies.
Traditionally, neurorehabilitation processes have
been based on the mobilisation of paralysed
extremities to avoid the stiffness and retractions of
joints and muscles. The most common therapy is the
Bobath method (Bobath, 1990) based on the
hierarchical organisation of the Central Nervous
System (CNS). According to Bobath, the direct
handling of the body at key points such as the trunk
is able to control afferent input and facilitate normal
postural reactions. According to this concept,
postures must be used to inhibit spasticity and tonic
neck reflexes and to facilitate righting and
equilibrium reactions.
With pass of time, new approaches have been
defined (Cano-de-la-Cuerda et al., 2012), such as the
task oriented rehabilitation process, which is based
on the functional task achievement, rather than on
the automatisms that are used for the task
completion. This method argues the repetition-based
therapies in the cases where they lack a functional
purpose. This approach seeks training cognitive,
psychological and sensitive aspects not taken into
account by the Bobath therapy.
The introduced therapies require several human
resources such as doctors and different therapists
(physical, occupational…). In most cases, therapists
need to be present during the therapy execution.
The latest advancements in robotics and
neuroscience have shown that robotic systems or
exoskeletons can facilitate functional task oriented
rehabilitation processes. According to several
authors, this type of therapy is more efficient for the
reduction of the effects of altered motor control.
Robot or exoskeleton assisted rehabilitation systems,
which are based on neurorehabilitation principles,
are tools that not only help patients move the arm
with precision; they also help reduce the fatigue of
the therapist during the rehabilitation process. This
type of rehabilitation is usually developed together
with a virtual reality environment. Additionally, this
type of system provides the therapists with tools to
make complete and objective studies over the
evolution of the patients. The key factors for a
successful robotic-assisted therapy have been
already described in a previous study (De Mauro et
al., 2012).
One of the challenges of the virtual reality based
robot assisted upper limb rehabilitation, is patients’
immersion within the therapy, to achieve an
improved progress of the rehabilitation. This
challenge is mainly motivated by the lack of a
realistic representation of the arm in the available
games. The lack of realistic representation is caused
by a lack of bioinspiration of the solution. This lack
of realism creates a lack of identification of the
patient with the virtual world, which negatively
affects the active role of the patient, and their
motivation. Therefore, the development of more
realistic arm models will improve the three key
factors (bioinspiration, active role of the patient, and
motivation) implied in the identified challenge.
Additionally, the analysis of state of the art on
robotic device based rehabilitation therapies has
underlined the need of remote therapy support and
the definition of a structured movement
quantification data format, interoperable with other
rehabilitation systems.
The objective of the present work is to develop a
realistic representation of the affected arm with the
aim to increase users’ motivation. Furthermore, the
research also targets the design and implementation
of the architecture and data structure to support
remote therapy and guarantee the interoperability
with other rehabilitation systems.
In section 2, a state-of-the-art in the field is
presented. In section 3, we detail our solution’s
design and implementation while in section 4 we
present the main results obtained from our solution’s
implementation. Conclusions and future work are
presented in section 5.
2 STATE OF THE ART
The lost of mobility or paralysis of upper extremities
is identified among the possible consequences of a
person suffering a stroke. The rehabilitation process
followed in these cases is composed of active or
passive training of the limbs and articulations, in all
the possible directions and with the largest run
possible. This process is usually done by performing
a large number of repetitions, which exhausts,
mentally and physically, both the patient and the
therapist. Therefore, the use of virtual reality (VR)
systems can help motivate the user. Currently most
of the available VR systems are not accessible to the
people with critical impairments, such as those who
have suffered from stroke or cerebral palsy. Thus,
the scientific community has worked in the use of
VR systems with the assistance of robotic systems or
exoskeletons.
In the following section, the different
technologies related to the identified research topics
will be studied. First, VR or games based systems
for rehabilitation, (including the design concepts)
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
70

will be analysed. Exosketons and robotic solutions
used for upper limb rehabilitation will then be
examined.
At the end of this section, technologies and
further considerations related to the remote
monitoring of the therapy support will be presented.
2.1 Virtual Reality based
Rehabilitation
The virtual reality systems can be classified as fully-
, semi- or non-immersive systems (Prashun et al.,
2010). The classification refers to the level of
perception of presence in a non-physical world and
the technology used to present the virtual world to
the user. A monitor, a projector or VR glasses are
normally used for each of these modalities.
Alternatives include the combined use of real
objects, augmented reality and VR to create a
mixed-reality (Hilton et al., 2011). This way, the
tasks of the rehabilitation solution can be brought
closer to real life tasks. This leads to a larger level of
cognitive learning and user acceptance, while
carrying out exercises to improve mobility. Hilton et
al., also report on studies that present the benefits
training of daily-living activities in VR scenarios
has, beside the benefits of the realisation of the
exercises, on applying the learned tasks in their real
life.
The main variables used for the rehabilitation
assessment are the time needed to get to the target
position, the speed at which the task is completed,
the accuracy of the trajectories and the range of
movements. The duration and the frecuency of the
therapy varies from study to study(from 45 minutes
to one or even two hours). Frecuency also varies
from 3-5 weeks upto 11-13 weeks with a repetition
of 5 days per week.
2.1.1 Rehabilitation Game’s Design
and Adaptation
For the design of rehabilitation games, many factors
need to be taken into account. One of the most
important ones is the feedback received by the user,
from the action being carrying out. This feedback
can be of different types: e.g. auditory, haptic or
visual. Feedback makes user motivation to increase,
either being to achieve a concrete task, achieve a
higher score or else (Maclean et al., 2000).
Different studies (Burke et al., 2010; Sveistrup,
2004) have underlined that the representation of the
user or his affected extremity in a virtual world is
very positive for accepting and engaging with the
therapy. In this type of system there is a continuous
feedback, so the user can focus on the affected
extremity, being conscious of the movements he/she
is doing.
Alankus et al. stress the importance of adapting
the games to each user and their evolution based on
different factors (Alankus et al., 2010). One of the
identified factors is that games should allow the user
a certain error margin and that errors consequences
should be constructive rather than catastrophic.
Another important factor is the game’s difficulty.
An excessive difficulty level can lead the user to
stop playing the games. On the contrary, an
excessive simplicity would get the user bored.
A study by N. Hocine et al. (Hocine and
Gouaich, 2011) shows that a dynamical difficulty
adaptation system, while maintaining a stable
success rate, influences positively the perceived
difficulty, making the therapy more satisfying and
rewarding for the patient. It is therefore important to
gradually increase the game’s difficulty, based on
patient’s evolution. Besides, the gradual increase of
difficulty attracts user’s attention. This distraction
can be used to facilitate patient’s pain management,
since when the patient is entertained, he/she is not so
conscious of pain.
Moreover, the games should also adapt to the
evolving user mobility capabilities. At the beginning
of the rehabilitation user’s mobility is very limited,
so the working area of the game should be reduced
compared to more advanced phases of the
rehabilitation process.
As rehabilitation involves a motor learning
process (Krakauer, 2006), the use of a taxonomy of
tasks, such as Gentile’s (Adams, 1999), can be
relevant here for both assessing the patient abilities
and building a coherent therapy plan gradually
increasing the movements complexity. According to
Gentile, four factors are to be taken into account: the
environment (whether it is changing in time and
space or not), the intertrial variability (if the target
changes between trials), the patient’s body motion
and the use of extremity. Other factors pointed by A.
Reinthal et al. (Reinthal et al., 2012) include whether
the task performed is continuous or discrete and
whether it requires unilateral or bimanual dexterity.
By increasing the movements’ complexity, the
patient gradually learns again how to perform
successfully activities of daily living, which involves
coordination between complex movements and
variations of the environment. In the case of
rehabilitation, intertrial variability is a key factor to
trigger a process of generalization of the
movement,for example for the patient to be able to
VirtualArmRepresentationandMultimodalMonitoringfortheUpperLimbRobotAssistedTeletherapy
71

grab an object regardless of its position (Krakauer,
2006).
Even if there is an increasing amount of games
targeted to rehabilitation, until now not all
entertainment possibilities present at mainstream
games are being exploited (Rego et al., 2010). For
example, there are no rehabilitation games, where
competitive, collaborative or net gaming is possible
among multiple users. These functionalities would
probably increase patients’ motivation.
2.2 Exoskeletons and Upper Limb
Rehabilitation Systems
The actual exoskeletons’ market is limited in
available models and their price is very high. These
are the main reasons for their low deployment.
Following, some of the commercially available or
scientifically reported exoskeletons are presented.
The Armeo Spring (Hocoma, 2013) is a
exoskeleton that embraces the whole arm, from
shoulder to the hand. This model is indicated for
those patients that have lost partially or completely
upper limb functionality, either caused by a brain,
spinal or muscular damage. This model has six
degrees of freedom (three in the shoulder, one in the
elbow and two in the wrist) without any robotic
actuator. Therefore, it is considered a passive
system. The Armeo Spring can be adjusted to patient
arm’s weight, so that patient doesn’t need to practise
any force to hold his arm. This way, a patient can
make use of his residual upper limb functionality.
With the aim of increasing the motivation and
acceptation of the therapy by the patient, the Armeo
Spring comes with different games that provide
auditory and visual feedback to the user. The
exercise area of the patient can be personalised to
the patient’s mobility range in each phase. Once the
game has finished, the session’s data is written into
an excel spreadsheet for patient’s evolution
assessment.
InMotion (InMotion, 2013) is an upper limb
(hand, arm, and shoulder) rehabilitation system. The
system is composed of three robotic systems:
InMotion Arm Robot, InMotion Hand Robot and the
InMotion Wrist Robot. These robotic systems have a
force-feedback system that helps users with mobility
limitations or users that lack coordination for
completing the objectives. As the patient evolves
and regains movement capabilities, the system
decreases the provided assistance in order to keep a
certain level of difficulty.
Qiu et al. defined a system (Qiu et al., 2010)
combining a force-controlled haptic interface
(Haptic Master) with a ring gimbal obtaining a six
degree of freedom, force-controlled robot targeted to
the upper limb rehabilitation. Adding the ring
gimbal as the end effector adds the possibility of
forearm rotation and records three more angles of
freedom. The system includes different games and
the possibility to limit the working area to adjust the
therapy to each patient’s capabilities.
With regard to exoskeleton systems based
combined therapies, August et al. defined a
rehabilitation system (August et al., 2011) that was
composed of computers, projectors, semi-transparent
mirrors, and light emitters to build a multisensory
therapy space, where the user can interact with both
real and virtual objects. The main idea behind this
type of therapy is that some users can lose the
perception of their body and their localisation while
participating in a virtual reality based therapy, which
is overcome with the integration of real object. The
mix of real and virtual objects can help improving
the motivation, as well as the auto-perception of the
body.
Some systems use the electromyography (EMG)
to monitor the biofeedback of the user. The objective
of this type of systems is to improve patient’s
abilities and his muscular activity. With this aim,
games are designed to use this type of biofeedback
to control some game elements. One of the games
(Ma et al., 2010) proposes to shoot balls to a target.
The proposed system for the game uses a movement
tracking system to move the shooter left-right and
up-down, while the EMG signal is used for shooting
the ball.
Similarly, other systems use brain computer
interaction (BCI). These systems are used to know
the emotional or the concentration state, to assist the
users with limb movement through robotic systems.
Ang et al. created a system (Angob et al., 2010)
combining a BCI system and a haptic robot (MIT-
Manus) for rehabilitation therapy. The users had to
make some initial tests for the system to identify the
signals related to their hand and arm movements.
After the initial signal training, neuro-feedback is
used to assist the user in completing the targeted
task. Even if the obtained results were worst than
those with the haptic robot itself, the help and the
information that these systems can provide to the
therapists, is clear. The information on the brain
activity complements the input for assessing
patient’s evolution.
2.3 Rehabilitation Remote Delivery
Telerehabilitation applications are categorized
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
72
(Brienza and McCue, 2013) into two main operating
models. The first application type is named as real-
time interactivity application, and it refers to those
applications that mimic face-to-face interactivity in a
medical facility. The second application type is
named as store-and-forward application, and follows
an asynchronous communication. A good insight
into the state of art of telerehabilitation systems can
be found at (Parmanto and Saptono, 2009).
Regarding the remote delivery of exoskeleton or
robotic system based rehabilitation, Oboe et al.
propose a haptic robot based remote rehabilitation
(Oboe et al., 2010). Their system allows the therapy
execution, even if the therapist and the patient are in
remote locations. The patient is provided with a
slave device, which transmits both the movement
and the applied force to the master device, hosted at
the therapist’s side. Since the haptic system works
two-ways, the therapist can assist or correct patient’s
movement.
Following, table 1 identifies the gaps and the
consequences detected during the state of art study.
Table 1: Gaps and consequences detected over the State of
the art.
Gap Consequences
Lack of realistic upper
limb representation in
the rehabilitation games.
Lack of patient’s
identification with the
virtual world. Lack of
motivation.
Lack of possibility to
carry out actions
remotely.
Need of specialised
personal in place.
The punctuations and
timing of the games are
not always significant
for the patient’s
evolution assessment.
Cannot objectively
evaluate patient’s
evolution.
Lack of exercise
recordings for offline
studies.
Systems do not allow
reproducing movement
or visualising patients,
neither locally nor
remotely.
Lack of standardised
movement data format
to compare it with other
tools.
Data cannot be
complemented with
information from other
systems, such as Kinect
based solutions.
3 SOLUTION’S DESIGN
AND IMPLEMENTATION
As presented in the previous section, traditional and
new robotic device based rehabilitation therapies
have some limitations. This paper’s implementation
tries to overcome the following:
Lack of realistic upper limb representation
Remote control / action impossibility and lack of
interactive online evaluation tool
Lack of exercise recordings for offline studies,
lack of medical evaluation oriented measures, and
lack of standardised movement data.
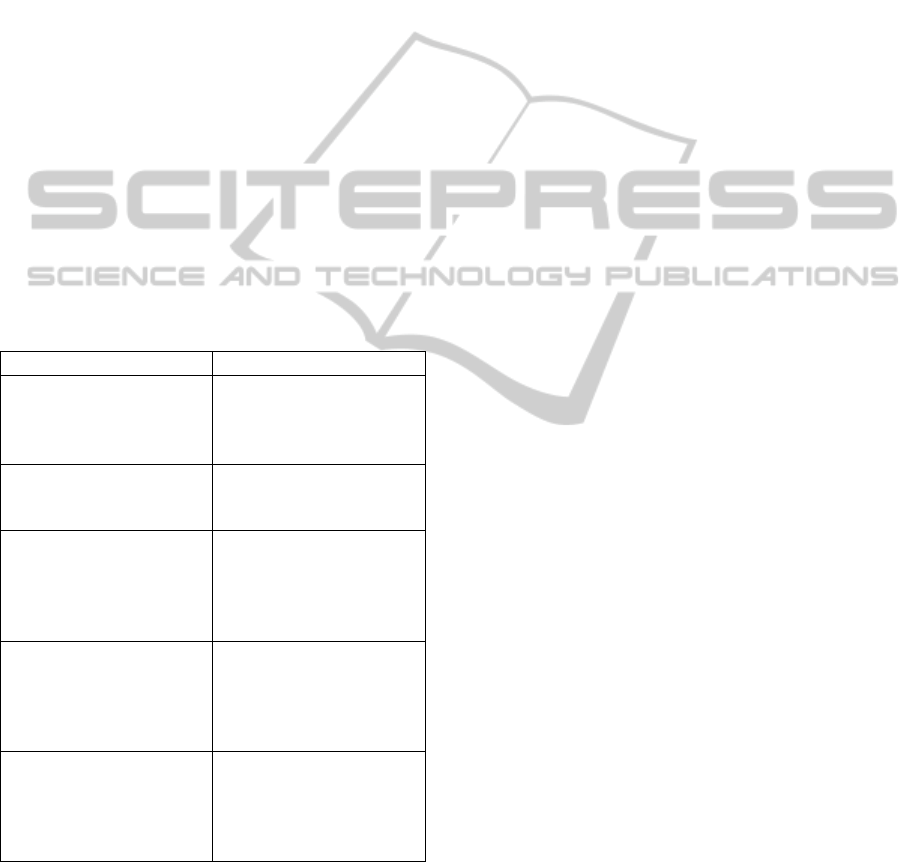
3.1 Architecture Design
An architecture has been designed for coping with
the limitations identified. To guide the reader, the
defined architecture is depicted at Figure 1. The
designed architecture is composed of three elements:
Rehabilitation Centre (PC + Armeo), Service Layer
(PC) and Medical Professional’s Client (PC).
The Rehabilitation Centre is the responsible to
provide the user with the necessary games to carry
out the rehabilitation exercises. While the user is
doing the exercises, the system monitors and records
multimodal data. On the one hand, a webcam
records the user for an offline analysis of the
movement. On the other hand, joint’s movement
data is recorded for a more exhaustive study of the
exercises carried out by the user. Joint’s movement
data is later processed and presented graphically by
visualisation tools.
The Server layer stores and provides access to
the multimodal (data and videos) patient recordings
and the interactive online evaluation tool. This tool
has been developed using a visualisation toolkit and
Java Applet technology, with the aim to deploy it in
different platforms.
The Medical Professional’s Client is a graphical
rehabilitation sessions playback tool. From this
client, the medical professional is able to visualise
both the recorded data and videos. This client
integrates the server layer’s interactive online
evaluation tool, which graphically represents the
recorded data and allows evaluating data through
functionalities such as the distance measurement
between two points.
The developed architecture design, allows the
different tools to work independently from their
location. This enables robotic device based
rehabilitation therapists to conduct the therapy
remotely, not needing to have an expert present at
the rehabilitation sessions.
3.2 Rehabilitation Centre
The rehabilitation centre’s client is composed of an
VirtualArmRepresentationandMultimodalMonitoringfortheUpperLimbRobotAssistedTeletherapy
73
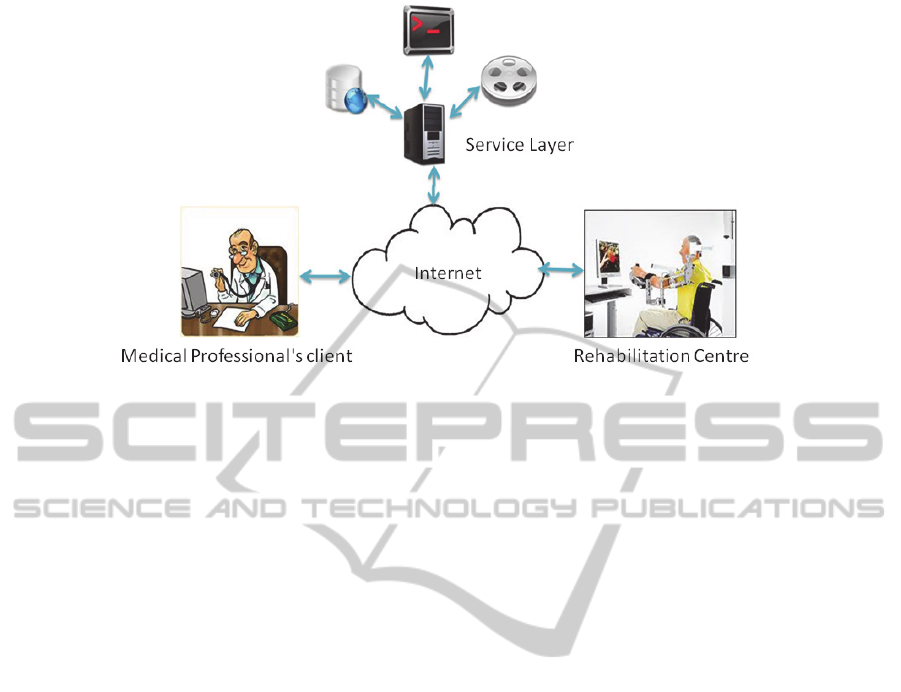
Figure 1: Architecture Design.
Armeo Spring exoskeleton, a PC, a webcam and the
developed software. The rehabilitation centre’s
software has been developed using C++
programming language, based on the Open Scene
Graph (OSG) library. The C++ programming
language has been selected to meet the Armeo
Exoskeleton application programming interface
requirements. OSG has been selected as the game
development platform, because it is open, it is a
high-level programming language and allows
loading models and animations with a base on
rotation transformation and allows the translation of
loaded objects. This geometric object manipulation
features facilitate representing a 3D arm, parting
from a robotic model of the Armeo. The
rehabilitation centre’s software is composed of three
modules: Games Module, Video Recording Module,
and Data Recording Module.
3.2.1 Games Module
The games module is the responsible for capturing
the movement data from the Armeo, for graphically
representing the user movements and for
implementing the games’ logic.
Movement Data Capture from the Armeo
Once the data is gathered from the Armeo, the data
is processed translating the gathered data into the
movements of the virtual arm. This process cannot
be publicly described, due to a confidentially
agreement signed with Hocoma, Armeo’s developer.
In case of needing related information, the reader
should contact Hocoma.
Graphical Representation
All the objects created for the virtual world have
been developed using the Autodesk Maya 3D tool.
Maya 3D has been selected due to the facilities it
provides to animate skeletons. Since most of the
developed objects are simple, the following
explanation is limited to the developed arm’s model.
For the movement generation of the virtual arm,
skeletal animation techniques have been used. These
techniques mainly consist on dividing the model in
two parts for animation development; the skin
representation and the hierarchical interconnection
of bones.
In order to develop a realistic arm model,
skinning technique has been used. This technique
consists on associating the bones with the vertices.
In some cases, the vertices can be associated to more
than one bone, therefore, weights are established so
the vertices act as real as possible. Figure 2 shows
the representation of the developed virtual arm.
Arm’s skeleton is represented in green, while the
vertices are indentified by the purple colour.
Figure 3 shows the weights influence. Weight
distribution in the wrist can be appreciated in the
form of a stronger white colour in areas where there
is more weight influence.
The virtual arms’ representation has six degrees
of freedom (DOF): two in the shoulder, two in the
elbow and two in the wrist, which allows
representing arm’s movements with certain fidelity.
To generate the movement of the virtual arm, the
data gathered from the Armeo has been processed to
obtain the angles at the six DOFs. From the
processed angles, rotations have been applied to the
respective points in the skeletons, through functions
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
74
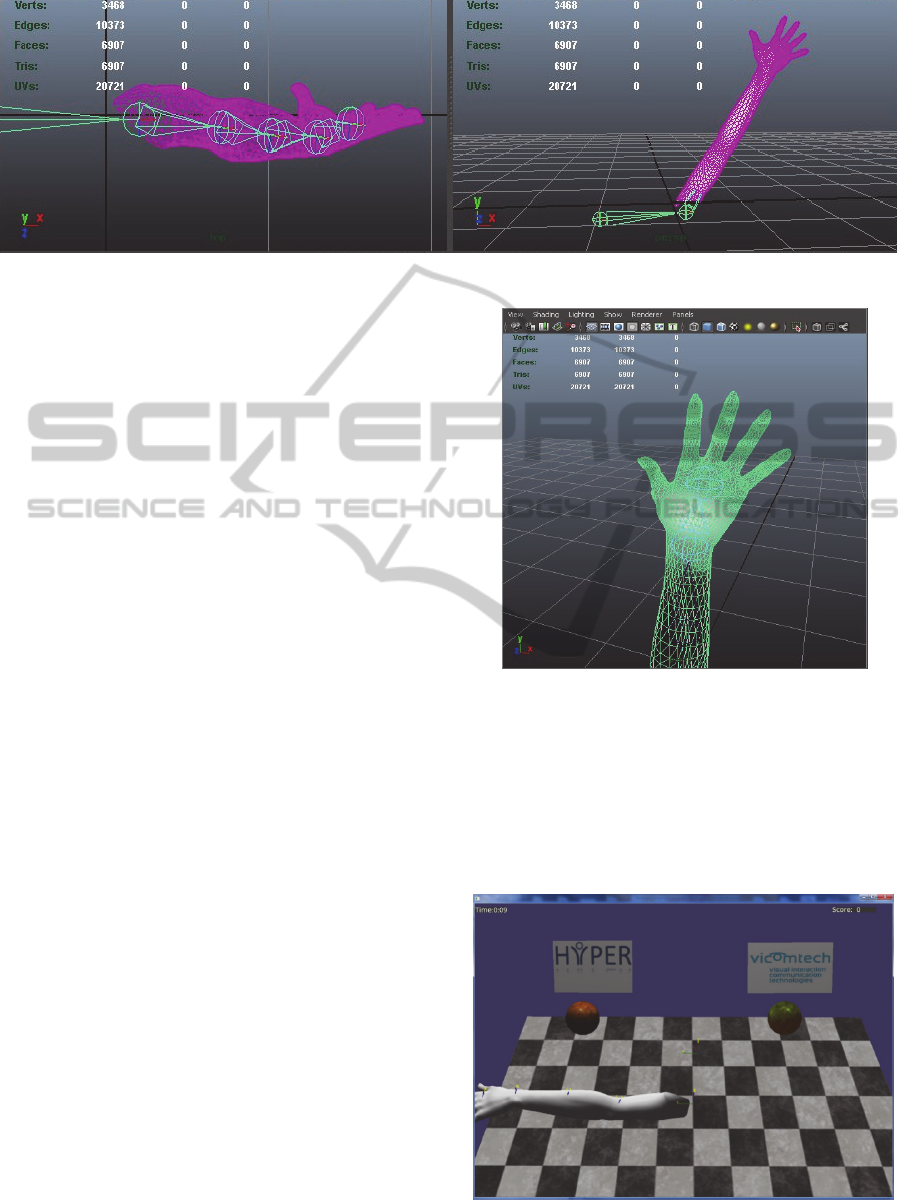
Figure 2: Virtual Arm’s Representation.
implemented by the OSG library. Rotations, as well
as translations are automatically generated by the
OSG library.
The realistic representation of the arm permits
the user to be conscious of the movements he/she is
doing as shown by studies in immersive virtual
reality used with patients with phantom limb pain
(Murray et al., 2007). Many people who has suffered
a cerebrovascular accident, is not conscious of their
upper limb movements. Hence, a virtual
representation of their limb can help them seeing an
action and reaction effect. This effect can make
patients feel more identified with their limbs, which
can increase their motivation with the rehabilitation,
obtaining better results on the rehabilitation process.
3.2.1.3 Game’s Logic
With the aim of providing the user with a more
entertaining rehabilitation process, two games have
been developed. The games are based on the objects
reaching and grasping tasks. These tasks have been
selected because they are repeatedly used in users’
daily living activities.
In the first game, the user has to touch two balls
located on the left and right top ends. Once the user
touches the green ball, it changes its colour and the
other ball is changed to green, and so on and so
forth. Whenever the user completes a series of
touching both balls, a point is added to the marker.
A screenshot of this game is included in Figure 4.
The second game is based on a ball that changes
its location every time the ball is touched and adds a
point to the marker. Both games have a duration of
two minutes.
The main benefit of these games is having the
user conscious of his movements, thanks to the
virtual representation of his arm. As the patient
evolves and it is capable of doing movements easier,
the mobility range can be increased.
Figure 3: Weight’s distribution in the wrist.
3.2.2 Video Recording Module
The Video Recording Module records video of the
rehabilitation sessions, for its later offline study. The
development of this module has been based on the
Open Source Computer Vision Library (OpenCV
Library). The OpenCV library is a multiplatform
Figure 4: Rehabilitation Game.
VirtualArmRepresentationandMultimodalMonitoringfortheUpperLimbRobotAssistedTeletherapy
75
library targeted to real time image processing.
Additionally, OpenCV has supplementary libraries
for machine learning, that implement different
algorithms, such as k-nn and Naive Bayes.
The Video Recording Module is started
whenever the user selects one of the available games
and is stopped when the user finishes playing the
game. The video is recorded in a separate thread of
the application to avoid interference with the games.
Videos are recorded in colour at a resolution of
640x480 and 25 frames per second, which can be
easily modified.
The video recording is done through a webcam
connected to the PC controlling the Armeo
exoskeleton and placed in front of the Armeo.
3.2.3 Data Recording Module
Patient’s movement data is recorded by the Data
Recording Module. As for the video recording, the
movement data is recorded while the user is playing
a game. The data is saved in XML format. For the
XML structure handling, the Xerces library has been
used.
The Xerces library allows to do many XML
related tasks (e.g. parse, validate and handle). The
library implements the main parsing standards.
Since the main targeted use of the data collection
is the visualisation and evaluation of graphical data,
the selected XML format for structuring the
movement data has been GraphML. GraphML
enables to specify data following a graph structure
description approach. Additionally, is possible to
add specific information required by the application.
The resulting data structure is depicted on the left
side of Figure 5. A person can have data from
exercises done on different days. The exercises
contain data on the movement and position of
interest. The regions of interests are the shoulder, the
elbow and the hand. Each joint has an associated
graph, which is composed of measurement nodes
with values on the X, Y and Z axis.
On the right side of Figure 5, an example of the
defined interoperability structure is given. This
example shows the file’s namespace definition, user
data, the exercises carried out, and the results of the
shoulder’s movement data recording.
3.3 Service Layer
3.3.1 Interactive Online Evaluation Tool
With the aim of deploying a multiplatform
interactive tool for patient evaluation, an interactive
online evaluation has been developed using a
visualisation toolkit and Java Applet technology.
After an analysis of different visualisation
toolkits, Java Prefuse library was selected, due to the
capability of running developments as part of Java
Applets. The developed tool is able to compare the
points obtained for the joints, during the different
sessions of the therapy.
Each session of each game is represented in a
different colour and it is possible to choose both the
Figure 5: Data interoperability XML structure.
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
76
days and the axis for visualisation. Moreover, it is
possible to zoom and move through the display to
analyse a specific region in detail. A button of the
application allows going back to initial visualisation,
centring the image to the workspace of the Applet.
In addition to the presented functionalities, the
Applet is capable of calculating the distance between
two nodes by selecting them in the display.
The Applet works by reading the following
parameters: file’s directory, username, timestamp,
game, joint and axis. Based on these parameters, the
XML is read and organised in classes for easier data
manipulation and the Applet executes the actions
needed for the required graph visualisation.
Screenshots of the tool are given in the Medical
Professional’s client section where it is integrated in
a final application.
3.3.2 Web Services
The service layer has been defined to be as
compatible with different platforms as possible.
Therefore, for the development of this layer, Web
services technologies have been used and deployed
over an Apache Tomcat server.
Three services have been defined: (1) To store
patient’s session’s XML in the server; (2) To modify
the script parameters that launch the Applet; (3) To
obtain the urls for the recorded videos.
The client enters as parameters the
username/password and the XML file with the data
recording. The server is responsible for storing and
organising the data in the server.
The Medical Professional’s Client integrates
with the web service to modify the script parameters
that launch the Applet. This integration allows the
medical professional to choose easily the graph
he/she needs to visualize. The client sends the
script’s parameter he/she wants to modify and its
corresponding value as an input to the Web Service.
In addition, the Medical Professional’s Client
needs to load the videos paths to play them in the
display. For this task, username and the time range is
sent to the Web Service and the response contains an
array with the paths to the recorded videos.
3.4 Medical Professional’s Client
The requirements defined for the Medical
Professional’s Client were that the client should be
able to play rehabilitation session videos and the
visualisation Applet without the user having the
feeling of using an external application.
After testing different technological options, the
application was developed using C# programming
language, with .NET Framework version 2.5.
This technology has allowed creating the
Medical Professional’s Client, playing videos and
visualising data natively. From the user interface, a
target patient name is selected. The application then
communicates with the server and obtains the videos
and the visualisation data with the default
parameters.
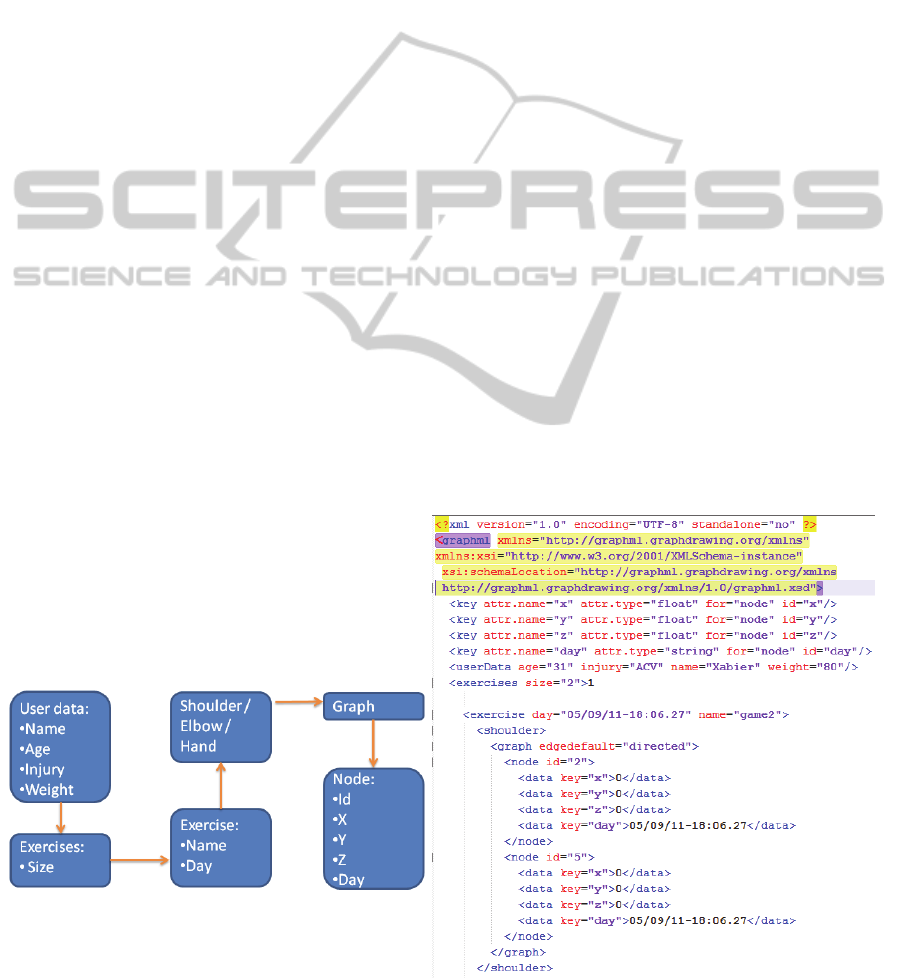
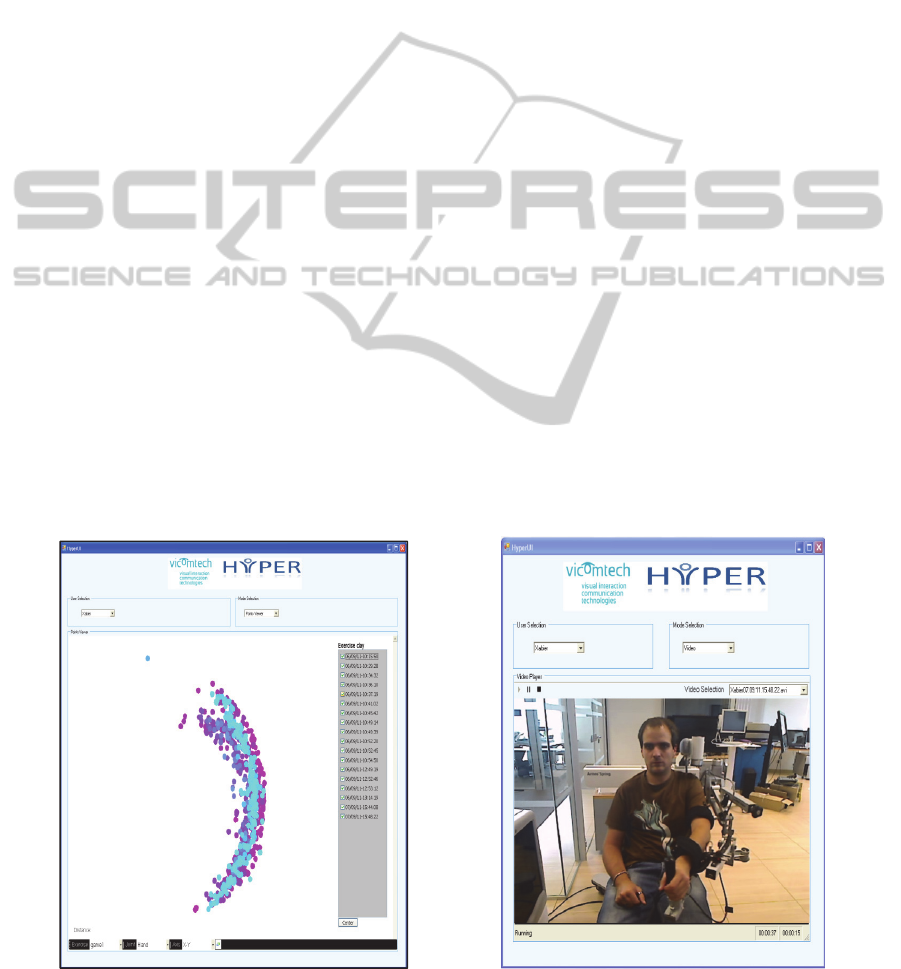
Following, Figure 6 presents two screenshots of
the Medical Professional’s Client. On the image on.
Figure 6: Medical Professional’s Client: Analysis Data tool (left) and recorded video in the execution of the rehabilitation
tasks (right).
VirtualArmRepresentationandMultimodalMonitoringfortheUpperLimbRobotAssistedTeletherapy
77

the left, the data visualisation functionality is shown
on the image on the right the functionality of
rehabilitation sessions’ video playback is shown.
4 RESULTS
The main result of the presented work is an
exoskeleton based telerehabilitation platform, which
targets the improvement of user’s motivation and
adherence to therapy. The developed platform is a
preliminary answer to the gaps detected in the study
of the state of the art.
The representation of the patients arm in a virtual
world achieves a larger identification of the patient
with the virtual world and a larger level of
consciousness of his movements, with the benefits
of motivation and progress it implies. The developed
games, allow carrying the repetitive task in a more
entertaining way.
Through the new tools the doctors will be able to
be either present at therapy execution or guide the
therapy remotely. This allows delegating the therapy
setup to less qualified personnel if needed.
The provision of online tools allows improving
the care processes at hospitals which helps the
sustainability of healthcare systems. Furthermore, it
allows experts from different hospitals to analyse the
results, building better diagnostics and therapies.
Once the user has completed a therapy session,
the specialised personnel can remotely evaluate both
the recorded video and the visualisation of
movements. Each joint and exercise has its graphical
representation and is possible to select the days to be
shown and to compare the evolution of the selected
joint during the selected day range.
The data recorded by the platform is available to
other programs, which enables the comparison of the
results with other rehabilitation platforms. This
allows validating the obtained information with
other experimental systems such as the Kinect based
rehabilitation systems. Additionally, the definition of
an interoperable data structure enables the
combination of different rehabilitation therapies,
allowing different device (Armeo vs Kinect) based
rehabilitation therapies for hospital and home.
5 CONCLUSIONS AND FUTURE
WORK
The characteristics of the developed rehabilitation
platform can help patients, doctors and the
healthcare system, as presented in the results section.
But, in order to validate the real impact of the
development, the system needs to be tested with real
patients.
As introduced in the previous section, it is
important to integrate the developments with other
rehabilitation systems such as the ones based on the
Kinect for the development of an integral approach
to the rehabilitation. This way, the user would be
able to continue the rehabilitation therapy at home,
as an extension to the therapy started at medical
facilities.
The cost of acquiring an Armeo Spring or similar
robotic systems is not a cost that all hospitals are
able to assume. Therefore, research is needed on
tools for hospitals, whose cost is not too elevated. In
addition, a detailed analysis of the economic and
quality of life of the involved persons, comparing
the robotic system tools with conventional therapies,
can help clarify the real benefits of these systems,
for all involved stakeholders.
Regarding the improvement of the platform, new
functionalities to ease the medical professional’s
work could be implemented. For example, hiding
points not contributing to evaluation, adding a
functionality to delimit the areas for calculating the
mobility range, an automatic comparison between
sessions, etc.
With regard to the video visualisation, an
implementation of video on demand and streaming
technologies will improve the content management
and the performance of the platform. Additionally,
image analysis algorithms implementation could
help complementing the movement data captured.
Another interesting research line identified
during the present research is the development of
collaborative and competitive game modes for
robotic system based rehabilitation. These games
could be deployed over the net or at medical
facilities where robotic system based rehabilitation
is being carried out. Nowadays, there are many
successful conventional online games, which lead
the authors to think that the life collaboration or
competition with other patients can increase their
motivation and as a consequence improve their
progress.
Due to the fact that each stroke patient has
different needs and preferences, games should be
customisable, so the virtual world or its containing
objects could be adapted. This way, games could be
adapted to the specific preferences and needs of each
person, which would improve the resulting
rehabilitation process.
Last but not least, due to the limited scope of the
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
78

presented research, the work on security
implementation has been limited. Taking into
account the confidentially and security needs of
using health data, the security aspects of this
implementation should be revised for real scenario
deployment.
ACKNOWLEDGEMENTS
This work was partially funded by the Spanish
Government CONSOLIDER-INGENIO 2010
Programme (Hyper Project).
REFERENCES
Adams, D. L. (1999). Develop Better Motor Skill
Progressions with Gentile’s Taxonomy of Tasks.
Journal of Physical Education, Recreation & Dance,
70(8), 35–38. doi:10.1080/07303084.1999.10605704.
Alankus, G., Lazar, A., May, M., & Kelleher, C. (2010).
Towards customizable games for stroke rehabilitation.
In Proceedings of the SIGCHI Conference on Human
Factors in Computing Systems (pp. 2113–2122). New
York, NY, USA: ACM. doi:10.1145/
1753326.1753649.
Angob, K. K., Guan, C., Sui Geok Chua, K., Ang, B.-T.,
Kuah, C., Wang, C., … Zhang, H. (2010). Clinical
study of neurorehabilitation in stroke using EEG-
based motor imagery brain-computer interface with
robotic feedback. In Engineering in Medicine and
Biology Society (EMBC), 2010 Annual International
Conference of the IEEE (pp. 5549–5552).
doi:10.1109/IEMBS.2010.5626782.
August, K. G., Guidali, M., Sellathurai, M., Jenu, S.,
Bleichenbacher, D., Klamroth-Marganska, V., …
Riener, R. (2011). A system for sensory motor
rehabilitation of the upper limb with virtual reality,
exoskeleton robot, and real objects. In Technologies
for Practical Robot Applications (TePRA), 2011 IEEE
Conference on (pp. 54–63). doi:10.1109/
TEPRA.2011.5753482.
Bobath, B. (1990). Adult hemiplegia: evaluation and
treatment. Butterworth-Heinemann Oxford.
Brienza, D. M., & McCue, M. (2013). Introduction to
Telerehabilitation. In S. Kumar & E. R. Cohn (Eds.),
Telerehabilitation (pp. 1–11). Springer London.
Retrieved from http://dx.doi.org/10.1007/978-1-4471-
4198-3_1.
Burke, J. W., McNeill, M. D. J., Charles, D. K., Morrow,
P. J., Crosbie, J. H., & McDonough, S. M. (2010).
Augmented Reality Games for Upper-Limb Stroke
Rehabilitation. In Games and Virtual Worlds for
Serious Applications (VS-GAMES), 2010 Second
International Conference on (pp. 75–78).
doi:10.1109/VS-GAMES.2010.21.
Cano-de-la-Cuerda, R., Molero-Sánchez, A., Carratalá-
Tejada, M., Alguacil-Diego, I. M., Molina-Rueda, F.,
Miangolarra-Page, J. C., & Torricelli, D. (2012).
Teorías y modelos de control y aprendizaje motor.
Aplicaciones clínicas en neurorrehabilitación.
Neurología, (0), -. doi:10.1016/j.nrl.2011.12.010.
De Mauro, A., Carrasco, E., Oyarzun, D., Ardanza, A.,
Frizera-Neto, A., Torricelli, D., … Florez, J. (2012).
Advanced Hybrid Technology for Neurorehabilitation:
The HYPER Project. In T. Gulrez & A. Hassanien
(Eds.), Advances in Robotics and Virtual Reality SE -
4 (Vol. 26, pp. 89–108). Springer Berlin Heidelberg.
doi:10.1007/978-3-642-23363-0_4.
Hilton, D., Cobb, S., Pridmore, T., Gladman, J., &
Edmans, J. (2011). Development and Evaluation of a
Mixed Reality System for Stroke Rehabilitation. In S.
Brahnam & L. Jain (Eds.), Advanced Computational
Intelligence Paradigms in Healthcare 6. Virtual
Reality in Psychotherapy, Rehabilitation, and
Assessment (pp. 193–228). Springer Berlin
Heidelberg. doi:http://dx.doi.org/10.1007/978-3-642-
17824-5_10.
Hocine, N., & Gouaich, A. (2011). Therapeutic games’
difficulty adaptation: An approach based on player's
ability and motivation. Computer Games (CGAMES),
2011 16th International Conference on.
doi:10.1109/CGAMES.2011.6000349.
Hocoma. (2013). Armeo Spring. Retrieved from
http://www.hocoma.com/products/armeo/armeospring/.
InMotion. (2013). InMotion Robots for Rehabilitation.
Retrieved from http://interactive-motion.com/.
Krakauer, J. W. (2006). Motor learning: its relevance to
stroke recovery and neurorehabilitation. Current
Opinion in Neurology, 19(1). Retrieved from
http://journals.lww.com/co-neurology/Fulltext/2006/
02000/Motor_learning__its_relevance_to_stroke_reco
very.14.aspx.
Ma, S., Varley, M., Shark, L., & Richards, J. (2010). EMG
Biofeedback Based VR System for Hand Rotation and
Grasping Rehabilitation. In Information Visualisation
(IV), 2010 14th International Conference (pp. 479–
484). doi:10.1109/IV.2010.73.
Maclean, N., Pound, P., Wolfe, C., & Rudd, A. (2000).
Qualitative analysis of stroke patients’ motivation for
rehabilitation. BMJ, 321(7268), 1051–1054.
doi:10.1136/bmj.321.7268.1051.
McKay, J., Mensah, G. A., & Greenlund, K. (2004). The
atlas of heart disease and stroke. World Health
Organization.
Murray, C. D., Pettifer, S., Howard, T., Patchick, E. L.,
Caillette, F., Kulkarni, J., & Bamford, C. (2007). The
treatment of phantom limb pain using immersive
virtual reality: Three case studies. Disability and
Rehabilitation, 29(18), 1465–1469. doi:10.1080/
09638280601107385.
Oboe, R., Daud, O. A., Masiero, S., Oscari, F., & Rosati,
G. (2010). Development of a haptic teleoperation
system for remote motor and functional evaluation of
hand in patients with neurological impairments. In
Advanced Motion Control, 2010 11th IEEE
VirtualArmRepresentationandMultimodalMonitoringfortheUpperLimbRobotAssistedTeletherapy
79

International Workshop on (pp. 518–523).
doi:10.1109/AMC.2010.5464078.
Parmanto, B., & Saptono, A. (2009). Telerehabilitation:
State-of-the-Art from an Informatics Perspective.
International Journal of TeleRehabilitation, 1(1).
doi:doi: 10.5195/ijt.2009.6015.
Prashun, P., Hadley, G., Gatzidis, C., & Swain, I. (2010).
Investigating the Trend of Virtual Reality-Based
Stroke Rehabilitation Systems. In Information
Visualisation (IV), 2010 14th International
Conference (pp. 641–647). doi:10.1109/IV.2010.93.
Qiu, Q., Fluet, G. G., Saleh, S., Ramirez, D., &
Adamovich, S. (2010). Robot-assisted virtual
rehabilitation (NJIT-RAVR) system for children with
cerebral palsy. In Bioengineering Conference,
Proceedings of the 2010 IEEE 36th Annual Northeast
(pp. 1–2). doi:10.1109/NEBC.2010.5458203.
Rego, P. A., Moreira, P. M., & Reis, L. P. (2010). Serious
games for rehabilitation: A survey and a classification
towards a taxonomy. In Information Systems and
Technologies (CISTI), 2010 5th Iberian Conference
on (pp. 1–6).
Reinthal, A., Szirony, K., Clark, C., Swiers, J., Kellicker,
M., & Linder, S. (2012). ENGAGE: Guided Activity-
Based Gaming in Neurorehabilitation after Stroke: A
Pilot Study. Stroke research and treatment, 2012.
Sveistrup, H. (2004). Motor rehabilitation using virtual
reality. Journal of NeuroEngineering and
Rehabilitation, 1(10). doi:10.1186/1743-0003-1-10.
World Heath Organization. (2011). Global Health and
Aging.
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
80
