
Turn Detection and Characterization with Inertial Sensors
Sean Pearson
1
, Martina Mancini
2
, Mahmoud El-Gohary
1
, James McNames
1
and Fay Horak
2
1
APDM Inc. Suite 130, 2828 Southwest Corbett Avenue, Portland, OR, U.S.A.
2
Oregon Health Sciences University, Neurology, 3181 SW Sam Jackson Park Rd, Portland, OR, U.S.A.
1 OBJECTIVES
Turn detection and characterization in the home is im-
portant for continuous assessment of gait and balance
in people with movement disability. Turning often re-
sults in falling in individuals with movement disor-
ders. Researchers and clinicians would benefit from
a system that identifies and characterizes their daily
mobility behavior to predict their risk of falling, ben-
efits or side effects of treatment, and progression of
disease. The goal of this study is to develop an algo-
rithm that is capable of reliably detecting turns dur-
ing gait with the goal of applying it over long periods
outside a lab environment. Performance of the algo-
rithm is validated against an optical marker system
and video analysis of a subset of the participants.
2 INTRODUCTION
Turning is ubiquitous during activities of daily living.
Nearly every task performed during the day requires
some amount of turning (Glaister et al., 2007). How-
ever, gait research has focused primarily on straight
ahead-walking (Studenski et al., 2003; Ganz et al.,
2007). Difficulty turning during gait is a major con-
tributor to mobility disability, falls and reduced qual-
ity of life in elderly and in people with movement dis-
orders. Falls during turning are particularly danger-
ous because they usually result in contact of the femur
with the ground, which results in eight times more hip
fractures compared with falls during straight-ahead
walking (Nevitt et al., 1991; Cumming and Klineberg,
1994; Feldman and Robinovitch, 2007). The ability
to modify our locomotor trajectory by turning safely
is important for functional independence but surpris-
ingly much more difficult for the nervous system to
control than straight-ahead walking.
Objective measures of turning mobility are more
sensitive than gait speed or clinical measures of
mobility to detect impaired mobility. Our studies
have shown that people with movement disability
may exhibit abnormal turning characteristics even
though they have normal straight-ahead walking (Ho-
rak et al., 1992; Salarian et al., 2009; King et al.,
2011). We found that turning measures in the clinic,
such as turning duration and peak turning velocity,
can distinguish between people with movement dis-
orders and healthy age-matched controls, even when
clinical measures of balance or gait did not (Spain
et al., 2010; Zampieri et al., 2010). Other stud-
ies found that measurements of turning discrimi-
nate elderly fallers from non-fallers (Dite and Tem-
ple, 2002). Researchers have suggested that turning-
related neural systems may be more vulnerable to im-
pairments than straight-ahead, linear gait. This is due
to the fact that turning involves more interlimb coordi-
nation, more coupling between posture and gait, and
modifications of locomotor patterns requiring frontal
lobe cognitive and executive function that plays a role
in postural transitions (King et al., 2012; Herman
et al., 2010).
In this study, we develop a new algorithms for ini-
tial sensors to detect and analyze a wide variety of
types of turning activities performed at different gait
speeds in the laboratory. We validate our algorithm
using a Motional Analysis system as a gold-standard.
As a second method of validating our inertial sensor
algorithms for turning, two raters review the videos
and annotate the beginning and end times of each turn.
In the following sections, we present the algorithm
and discuss the results and future work.
3 METHODS
We examined 17 healthy control subjects wearing a
set of four Motion Analysis reflective markers and
an Opal inertial sensor (APDM Inc.) on the lumbar
spine. Opal includes triaxial accelerometers, gyro-
scopes, and magnetometers and record signal data at
128 Hz. Subjects were instructed to walk on a path
composed of a mixed route with short straight seg-
ments and turns ranging from 30 to 180 degrees. Each
subject performed 12 repetitions: 4 at a slow speed, 4
at a preferred speed, and 4 at a fast speed.
19
Pearson S., Mancini M., El-Gohary M., McNames J. and Horak F..
Turn Detection and Characterization with Inertial Sensors.
DOI: 10.5220/0004647000190022
In Proceedings of the International Congress on Sports Science Research and Technology Support (icSPORTS-2013), pages 19-22
ISBN: 978-989-8565-79-2
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)
Figure 1: An example of the Opal (APDM Inc.) inertial
sensor placed on the lumbar.
For the purpose of turn detection and characteriza-
tion, the angular rate about the vertical axis (gravity
aligned) is an ideal measurement. A three-axis gyro-
scope is capable of measuring this vertical axis angu-
lar velocity, but aligning the sensor and maintaining
accurate alignment is difficult. An accelerometer can
be used to measure the direction of gravity during a
stationary period and then, the gyroscope measure-
ments could be projected on to that axis throughout
the trial.
Orientation angles are commonly estimated using
sensor fusing, taking advantage of the accelerome-
ter measurement of gravity to correct drift from inte-
gration of angular velocity measurements (El-Gohary
and McNames, 2012). We take advantage of the ori-
entation estimates to obtain angular velocity about the
vertical axis using appropriate transformation. Opal
sensor provide orientation estimates, q, in quaternion
form and can be used directly to transform body frame
sensor measurements into the inertial frame. We
transform the angular velocity measurements in the
body frame, ω
b
, to that in the inertial frame (with x-
y-z axes corresponding to magnetic North, East, and
Up), ω
i
using the following quaternion multiplication.
ω
i
= q ∗ ω
b
∗ q
−1
(1)
From the inertial frame angular velocity we extract
the z component, w
z
about the vertical axis. This an-
gular velocity about the vertical axis can be integrated
to obtain an estimate of the relative turn angle.
θ
z
=
Z
ω
z
(2)
This turn angle drifts over time due to integration er-
ror, but over short time periods is very accurate. The
Opal magnetometer could be used to help compen-
sate for this error. However, since only relative angles
during short period while turning are of importance
for detecting and characterizing turns, the potential
drawbacks of being susceptible to magnetic interfer-
ence from nearby objects outweigh the benefits of us-
ing the magnetometer (Bachmann et al., 2004).
The vertical axis angular velocity (ω
z
) is lowpass
filtered with a 1.5 Hz cutoff frequency Butterworth
filter to remove high frequency components. Candi-
date turns are then detected from segments where this
filtered angular velocity is greater than 15 degrees per
second. Start and end of each turn are set to the point
where the filtered angular velocity drops below 5 de-
grees per second. The precise cutoff value has little
effect on the total turn duration or angle, and is in-
tended to account for a slight bias which could prevent
the angular velocity from dropping exactly to zero. It
is difficult for humans to make more than a very slight
turn with a duration < 0.5 seconds or to complete an
extremely slow turn with a duration > 10 seconds,
during gait. Therefore, only turns with duration be-
tween 0.5 and 10 seconds, with turn angles over 45
degrees are considered. We combine any turns in the
same direction separated by a brief pause < 50 mil-
liseconds.
4 RESULTS
Turn detection was performed on the optical Motion
Analysis data. In a subset of trials, a standard video
was also reviewed by two raters who annotated begin-
ning and end times of turns. Timing accuracy of the
turn detection is important for characterizing turn du-
ration, therefore, we use one based on time intervals
rather than a turn by turn accuracy comparison. All
turn detection metrics were resampled at 128 Hz, and
comparison was calculated on a sample by sample ba-
sis, rather than by turns,
Table 1 shows sensitivity of the inertial algo-
rithm detecting turns compared to Motion Analysis
and video raters. Sensitivity of the inertial algorithm
is 0.86 compared with the optical marker algorithm.
Similarly, sensitivity for the inertial algorithm is 0.77
compared to both video rater 1 and 2. The optical al-
gorithm has sensitivity of 0.62 and 0.65 with video
rater 1 and2 respectively. Video rater 1 has a sensitiv-
ity of 0.89 compared with video rater 2.
Table 1: Sensitivity.
Optical Video 1 Video 2
Inertial 0.86 0.77 0.77
Optical 0.62 0.65
Video 1 0.89
Table 2 show specificity of the inertial algorithm
detecting turns compared to Motion Analysis and
icSPORTS2013-InternationalCongressonSportsScienceResearchandTechnologySupport
20
−1500 −1000 −500 0 500 1000 1500 2000
−2000
−1500
−1000
−500
0
500
1000
1500
X position (mm)
Y position (mm)
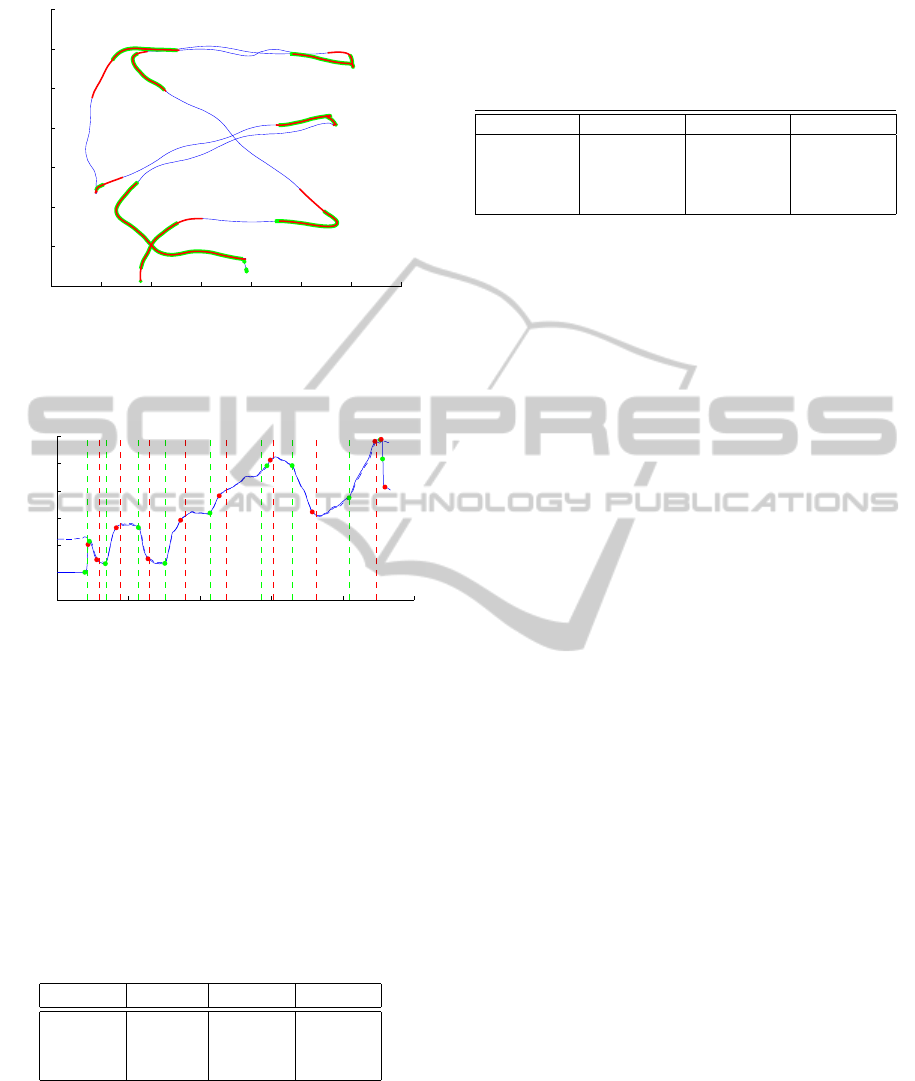
Figure 2: The blue trace is the X-Y position of the center of
mass from optical markers. Overlaid in red are the segments
detected as turns by the inertial algorithm, and in green the
segments detected as turns by the optical algorithm.
0 10 20 30 40 50
−100
0
100
200
300
400
500
Time (s)
Yaw Angle (deg)
Figure 3: The blue trace is the yaw angle from the optical
system. The dashed blue line is relative yaw angle from the
inertial algorithm. The dots represent onset (green) and end
(red) of turns detected by the optical algorithm. The vertical
dashed lines represent onset (green) and end (red) of turns
detected by the inertial algorithm.
video raters. Specificity of the inertial algorithm is
0.70, 0.66 and 0.54 with the optical marker algorithm,
video rater 1 and 2 respectively. The optical marker
algorithm has specificity of 0.77 and 0.68 with video
rater 1 and 2. Rater 1 has a specificity of 0.64 com-
pared with video rater 2.
Table 2: Specificity.
Optical Video 1 Video 2
Inertial 0.70 0.66 0.54
Optical 0.77 0.69
Video 1 0.64
The number of detected turns for the inertial al-
gorithm averaged 9.6 (sd = 1.4) across all subjects
and trials. The algorithm based on optical markers
detected an average of 10.4 turns (sd = 3.4). The pre-
scribed pattern had 10 turns larger than 45 degrees,
including one pair of 90 degree turns to pick up a bas-
ket. Table 3 shows turn metrics detected by the in-
ertial algorithm, including average number of terms,
turn peak and mean velocity in degrees per seconds,
and turn duration in seconds.
Table 3: Turn metrics.
Metric Slow (sd) Normal (sd) Fast (sd)
# of turns 9.6 (1.1) 9.6 (0.9) 8.3 (1.3)
Peak Vel. 112.2 (16.8) 131.2 (19.4) 169.7 (27.8)
Mean Vel. 56.8 (6.6) 64.0 (8.2) 76.8 (10.7)
Duration (s) 2.2 (0.3) 2.1 (0.3) 2.1 (0.4)
5 DISCUSSION
Turning is ubiquitous during activities of daily living.
Nearly every task performed during the day requires
some amount of turning (Glaister et al., 2007). How-
ever, gait research has focused primarily on straight
ahead walking. In this study, we use inertial sensors
including gyroscopes and accelerometers to charac-
terize turns during gait. We validated our inertial al-
gorithm using Motional Analysis system and turn data
from 2 raters analyzing video recordings of healthy
subjects.
Inertial sensors can be used to detect turns during
walking at least as well as an optical marker system.
Subjects were very inconsistent with the basket turns,
with some avoiding it altogether by picking up the
basket without any turning at the waist. In this close
pattern with the rapid series of turns it is sometimes
the case that multiple turns become blended together,
where a subject will transition fluidly from one to the
next rather than following the line precisely. Both of
these factors contribute to variability in the number of
detected turns, especially in the fast trials.
Turn detection and characterization in the home
is important for continuous assessment of gait and
balance in people with movement disability. Asking
an individual to execute a turn in a clinical environ-
ment often does not reveal their impairments. We
hypothesis that we can use the algorithm developed
in this study to measure locomotor activities and to
distinguish turning characteristics in healthy subjects
and individuals with movement disorders, in the home
throughout the day, using wearable inertial sensors.
ACKNOWLEDGEMENTS
Research reported in this study was supported by
the National Institute of Neurological Disorders and
Stroke (NINDS) of the National Institutes of Health
under award number R41NS076088-02.
TurnDetectionandCharacterizationwithInertialSensors
21

REFERENCES
Bachmann, E. R., Yun, X., and Peterson, C. (2004). An in-
vestigation of the effects of magnetic variations on in-
ertialklagnetic orientation sensors. In Proceedings of
the 2004 IEEE International Conference on Robotics
and Automation, pages 1115–1122.
Cumming, R. G. and Klineberg, R. J. (1994). Fall frequency
and characteristics and the risk of hip fractures. Jour-
nal of the American Geriatrics Society, 42(7):774.
Dite, W. and Temple, V. A. (2002). Development of a
clinical measure of turning for older adults. Amer-
ican journal of physical medicine & rehabilitation,
81(11):857–866.
El-Gohary, M. and McNames, J. (2012). Shoulder And El-
bow Joint Angle Tracking with Inertial Sensors. IEEE
Transactions on Biomedical Engineering, 59(9):577–
585.
Feldman, F. and Robinovitch, S. N. (2007). Reducing hip
fracture risk during sideways falls: evidence in young
adults of the protective effects of impact to the hands
and stepping. Journal of biomechanics, 40(12):2612–
2618.
Ganz, D., Bao, Y., Shekelle, P., and Rubenstein, L. (2007).
Will my patient fall. the journal of the American Med-
ical Association, 297(1):77–86.
Glaister, B., Bernatz, G., Klute, G., and Orendurff, M.
(2007). Video task analysis of turning during activ-
ities of daily living. Gait & Posture, 2(25):289–294.
Herman, T., Giladi, N., and Hausdorff, J. M. (2010). Prop-
erties of the ?timed up and go?test: more than meets
the eye. Gerontology, 57(3):203–210.
Horak, F., Jones-Rycewicz, C., Black, F., and Shumway-
Cook, A. (1992). Effects of vestibular rehabilitation
on dizziness and imbalance. Otolaryngol Head Neck
Surg, 106(2):175–180.
King, L., Mancini, M., Priest, K., and Salarian, A. (2011).
Instrumented and clinical measures of turning in
Parkinson’s disease. Journal Neurologic Physical
Therapy, page In Press.
King, L., Mancini, M., Priest, K., Salarian, A., Rodrigues-
de Paula, F., and Horak, F. (2012). Do clinical scales
of balance reflect turning abnormalities in people with
Parkinson’s disease? Journal of Neurologic Physical
Therapy, 36(1):25–31.
Nevitt, M. C., Cummings, S. R., and Hudes, E. S. (1991).
Risk factors for injurious falls: a prospective study.
Journal of gerontology, 46(5):M164–M170.
Salarian, A., Zampieri, C., Horak, F., Carlson-Kuhta, P.,
Nutt, J., and Aminian, K. (2009). Analyzing 180 de-
grees turns using an inertial system reveals early signs
of progression of Parkinson’s disease. In Proceedings
of the 2009 IEEE Eng Med Biol Soc, pages 224–227.
Spain, R., St George, R., Salarian, A., Bourdette, D., and
Horak, F. (2010). Validation of an instrumented test
of mobility, iMOBILITY, in multiple sclerosis. In
American Academy of Neurology 62
st
Annual Meet-
ing, Toronto, Canada. American Academy of Neurol-
ogy.
Studenski, S., Perera, S., Wallace, D., Chandler, J., Dun-
can, P., Rooney, E., Fox, M., and Guralnik, J. (2003).
Physical performance measures in the clinical set-
ting. Journal of the American Geriatrics Society,
51(3):314–322.
Zampieri, C., Salarian, A., Carlson-Kuhta, P., Aminian, K.,
Nutt, J., and Horak, F. (2010). The instrumented timed
up and go test: potential outcome measure for disease
modifying therapies in Parkinson’s disease. J Neurol
Neurosurg Psychiatry, 81(12):171–176.
icSPORTS2013-InternationalCongressonSportsScienceResearchandTechnologySupport
22
