
Assessment of the Suitability of the Motorized Ankle-Foot Orthosis as a
Diagnostic and Rehabilitation Tool for Gait
Guillermo As
´
ın
1
, Filipe A. Barroso
1,2
, Juan C. Moreno
1
and Jos
´
e L. Pons
1
1
Bioengineering Group, Spanish National Research Council (CSIC),
Crtra. Campo Real km. 0,200 28500, Arganda del Rey (Madrid), Spain
2
Adaptive System Behaviour Group - Industrial Electronics Department, University of Minho, Gimar
˜
aes, Portugal
Keywords:
Motorized Ankle-foot Orthosis, Gait, TOP-DOWN, EMG, Neuroengineering, Kinematics.
Abstract:
A unilateral powered exoskeleton (Motorized ankle-foot orthosis, MAFO) is presented in this work, with the
aim of studying muscle and kinematics short-term adaptations of the ankle during rehabilitation tasks. For this
purpose, we conducted this study during gait over a treadmill, measuring surface electromyography activation
and biomechanical data, in different conditions of assistance. This pilot study also aims to demonstrate that the
tool is suitable for measuring biomechanical data while allowing EMG measurements, proving it as a useful
tool during gait assessment and rehabilitation. Gastrocnemius Medialis activation presents slightly higher
amplitude with higher assistances, so the subjects performed a higher range of motion gait pattern. Tibialis
Anterior EMG activation presents consistent data with previous studies. Ankle angle at lower assistances
makes the robot force less the subject to reach the imposed gait pattern, and so the range of motion diminishes.
Regarding ankle angular velocity, at higher assistances, higher velocities are reached. The torque between the
subjects foot and the robot. For lower assistances, the imposed reference pattern is less restrictive, and so the
force the user exerts against the robot is lower.
1 INTRODUCTION
Stroke is the principal neurological disease in the de-
veloped world that culminates in physical disability.
Most promising interventions for the rehabilitation
of locomotor function are based on robotic systems
which are focused on the rehabilitation of the function
by acting at the periphery of the body (BOTTOM-UP
approach). It is unclear how effective these treatments
are, and one of the biggest problems they have is the
non-adherence of the patient to the therapy.
The opposite approach, which focuses on neu-
rological interventions that are based on the state
of the brain after the pathology to alter periph-
eral behavioural outcomes is known as TOP-DOWN
approach(Belda-Lois et al., 2011). Iosa and col-
leagues applied this approach in the framework of the
European Project BETTER with a new tool in which
a specifically designed ankle-foot orthosis (AFO) is
combined with sEMG (surface electromyography)
and kinematics sensors to provide the user a contin-
uous online feedback of his/her performance (Iosa
et al., 2012).
Several motorized devices for training during
overground gait have been described in the litera-
ture. The WalkTrainer is intended for a patient to re-
learn gait by combining a hybrid orthosis with func-
tional electrical stimulation (Stauffer et al., 2009)
with a BWS (body-weight-support) portable mech-
anism. The IHMC (Institute for Human and Ma-
chine Cognition) Mobility Assist Exoskeleton (Kwa
et al., 2009), the externally powered lower limb or-
thosis (Saito et al., 2005), and the Lower Body Ex-
oskeleton (Costa and Caldwell, 2006) are other simi-
lar devices that allow over ground and treadmill gait
rehabilitation. Focusing on exoskeletons that target
single joints like the device used in this work, the
literature describe apparatuses such as the powered
KAFO (knee-ankle-foot orthosis), a unilateral KAFO
that actuates proportionally to surface EMG signals
from the patient (Sawicki and Ferris, 2009) by actu-
ating artificial pneumatic muscles. GAIT is a quasi-
passive KAFO that was developed as a low-power de-
vice (Moreno et al., 2008), where the knee is actively
powered, but the ankle relies on a springed passive
actuator to avoid foot drop while providing mobility.
The variable impedance AFO described by Blaya and
Herr (Blaya and Herr, 2004), an ambulatory version
161
Asín G., Barroso F., Moreno J. and Pons J..
Assessment of the Suitability of the Motorized Ankle-Foot Orthosis as a Diagnostic and Rehabilitation Tool for Gait.
DOI: 10.5220/0004652101610166
In Proceedings of the International Congress on Neurotechnology, Electronics and Informatics (SensoryFusion-2013), pages 161-166
ISBN: 978-989-8565-80-8
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)
of the AnkleBot (Krebs and Hogan, 2006; Wheeler
et al., 2004), is an AFO that impedes foot drop by
regulating the impedance via a series elastic actua-
tor. Galle and colleagues propose an assistive bilat-
eral AFO exoskeleton (Galle et al., 2013) based on an
adaptive sEMG controller and pneumatic actuators, to
reduce the metabolic cost of walking. Ferris and col-
leagues in several papers presented the use of an AFO
powered by artificial pneumatic muscles for the study
of EMG activation of dorsiflexors (Tibialis Anterior)
and/or plantar flexors (Soleus, Gastrocnemius) while
gait (Ferris et al., 2005; Ferris et al., 2006; Sawicki
and Ferris, 2008; Gordon and Ferris, 2007; Kao and
Ferris, 2009; Kao et al., 2010a; Kao et al., 2010b); but
highlighted the main limitation of this kind of actua-
tors: they make the exoskeleton not readily portable.
A motorized AFO developed in the framework of
the BETTER project (MAFO, motorized AFO) (As
´
ın
et al., 2012) has been proposed as a controllable or-
thosis that can alter the ankle joint neuromuscular
control and therefore be applied to assist in locomo-
tion training after neurological injury.
Our goal is to study muscle and kinematics short-
term adaptations of the ankle with the use of a unilat-
eral powered exoskeleton. For this purpose, we con-
ducted this study during gait over a treadmill, measur-
ing EMG activation and biomechanical data, in dif-
ferent conditions of assistance (ratio between “robot
in charge” and “patient in charge” (Van der Kooij
et al., 2006) concepts). This pilot study also aims
to demonstrate that the tool is suitable for measur-
ing biomechanical data while allowing EMG mea-
surements, proving it as a useful tool during gait re-
habilitation.
2 MATERIALS AND METHODS
2.1 Subjects
Three healthy right-handed subjects (2 male, 1 fe-
male, age 25 ± 1.73 years, body mass 75.67 ± 16 kg)
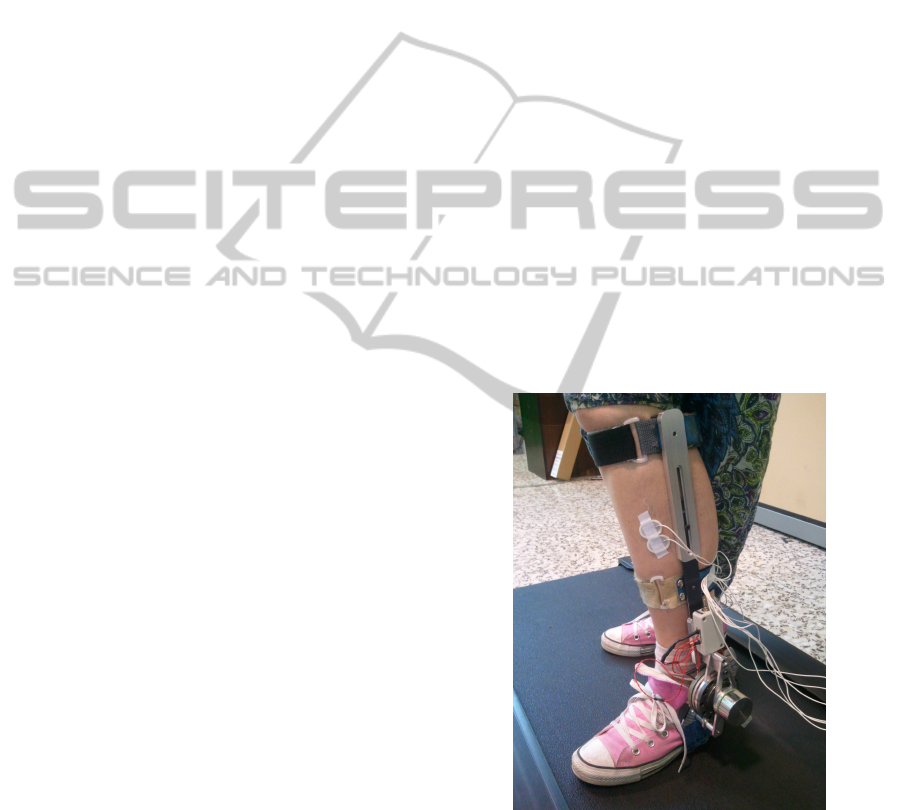
were enrolled in this study. A left MAFO (see Fig-
ure 1) weighting 1.1 kg was used. It was adjusted to
match each of the subjects lower leg length and malle-
oli position. The insole is located inside the sports
footwear of the subject as a means of tight attachment
to the foot, to reliably transmit the movement to the
joint. A rubber insole of the same height as the robots
insole has been located inside the contralateral shoe
to compensate the height difference.
2.2 Procedure
The subjects underwent robot-aided walking on a
treadmill (TC-450 by Domyos) at 1 m/s with the
MAFO under these conditions:
1. Full Assistance (refer to 2.2.1 for an explanation
of this parameter) (FA): robot in charge, i.e. the
robot performs all the movement with no need of
any contribution from the subject.
2. Medium Assistance (MA): the robot performs
50% of the movement, i.e., the robot is only able
to reach 50% of the targeted trajectory. The re-
maining 50% is accomplished by the subject.
3. Low Assistance (LA): the same as MA condition,
being the ratio 10% from the robot and 90% from
the subject.
As a partial aim of the study was to study angu-
lar position while walking with the orthosis, subjects
were asked to walk as if they were not wearing the
robot, but forcing the robot if needed in order to try
to perform a normal gait pattern. They had no vi-
sual reference so they were just focused on walking.
They had to walk without resting the hands on the
bars of the treadmill, to emulate as close as possible
overground walking.
Figure 1: MAFO (motorized ankle foot orthosis), worn by
one of the subjects of the study.
The trials (summarized in Table 1) had a duration
of 3 minutes and were separated in time by at least
half an hour to ensure independence between trials
and let muscles rest to eliminate fatigue due to the
exercise.
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
162
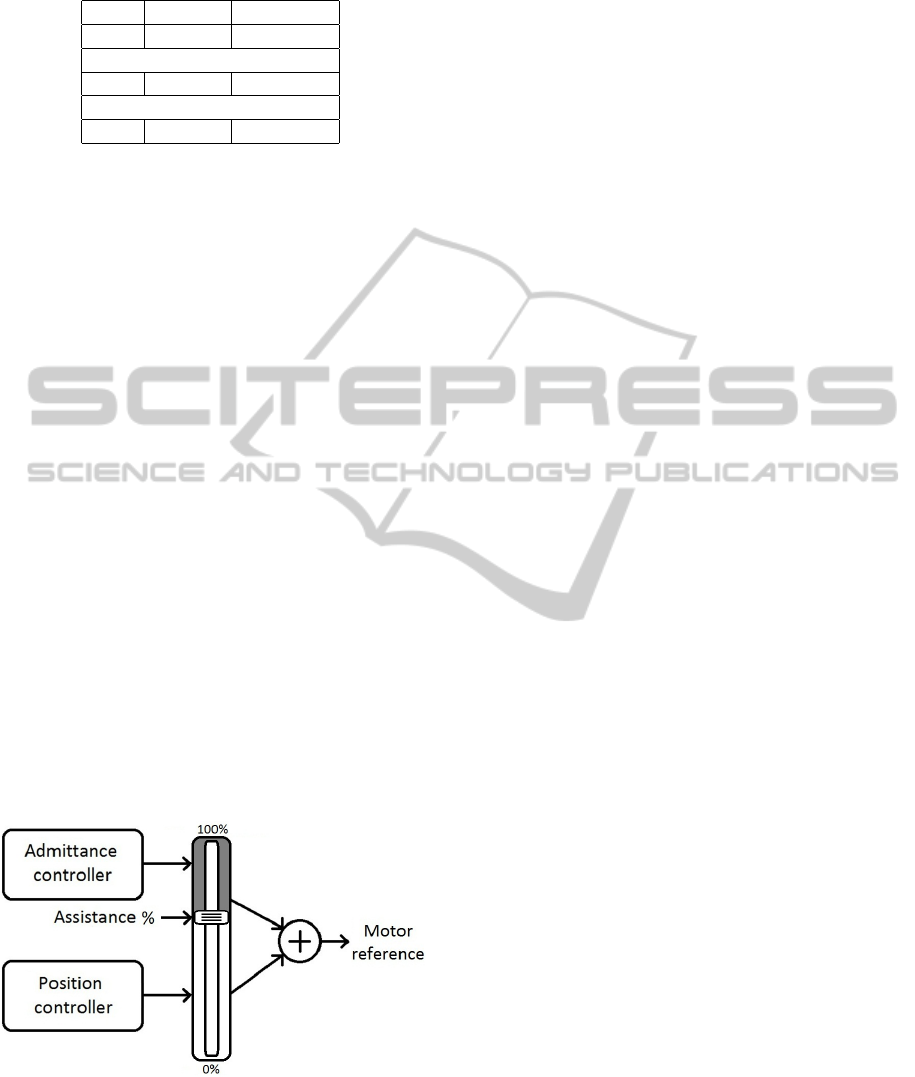
Table 1: Study conditions.
Trial Velocity Assistance
FA 1 m/s 100%
30 minutes rest
MA 1 m/s 50%
30 minutes rest
LA 1 m/s 10%
2.2.1 Hybrid Controller
The device is controlled using a hybrid controller
where the value of contribution of a position con-
troller and an admittance controller (based on the
measured torque) is selected prior to the beginning of
the exercise (see Figure 2). A parameter called “as-
sistance”, with values from 0 to 100 per cent, modu-
lates the output from the controller. 100 per cent of
assistance indicates that the controller output depends
only on the position controller; at 0 per cent, the con-
troller output comes from the admittance controller;
and so at values in between the controller output is
distributed with “assistance” percentage from the po-
sition controller, and 100 minus “assistance” percent-
age from the admittance controller. This parameter
was calibrated by measuring the percentage of ankle
range of motion the robot was able to reach while per-
forming a dorsi-plantar flexion continuous movement
at different velocities.
The gait pattern is pre-recorded from a healthy
subject as in (Hitt et al., 2009) and modulated as a
function of the stride time as in (Ward et al., 2006).
The admittance controller is dependent on the gait
phase, with a lower stiffness in the swing phase than
in the stance phase, i.e. a higher proportional gain in
the swing than in the stance phase, to avoid the effect
of the interaction torque against the ground.
Figure 2: Hybrid controller conceptual scheme.
2.3 Data Acquisition and Analysis
The MAFO records ankle joint angular position, an-
gular velocity, and torque resulting from the in-
teraction between the foot and the orthosis. Two
footswitches were located at the heel and the toe to
record heel strike and toe-off conditions respectively,
for the identification of the gait phase. This allows the
robot to synchronize to users gait phase.
Two muscles have been measured in the study:
Tibialis Anterior (dorsiflexion) and Gastrocnemius
Medialis (plantar flexion). These distal muscles ex-
ert the more powerful EMG signals involved in the
control of the ankle joint. Furthermore, as the ankle
joint produces the majority of the positive mechani-
cal work during stance in human walking (Kao et al.,
2010b), further studies with this hardware could lead
to mechanical analysis of the whole limb. They have
been recorded with the equipment EMG-USB by OT
Bioelettronica, in a bipolar configuration according to
SENIAM recommendations (Hermens et al., 1999),
with both DRL and reference at the subjects left wrist.
Kinematic signals were sampled at 1200 Hz, and
EMG signals at 2048 Hz. Raw EMG data were high-
pass filtered (3rd order Butterworth digital) at 20 Hz
and envelopes for each signal were extracted. Indi-
vidual stride cycles were separated with gait events
determined using the footswitches data, obtaining for
the three-minute sessions 90 ± 5 steps. Kinematic
signals were resampled to 2048 Hz sampling fre-
quency to match EMG data sample frequency. The
smoothed EMG and kinematic signals were then av-
eraged (stride-by-stride and for all the subjects) to ob-
tain averaged time-normalized gait cycles for all con-
ditions and data for the comparison between condi-
tions.
3 RESULTS
3.1 EMG Activation
The subjects were asked to walk as normally as pos-
sible, so the hypothesis was that the activation pat-
terns may remain almost unchanged in such a short
exercise. Figure 3 shows the activation of the Tibialis
anterior (TA) and Gastrocnemius Medialis (GM) for
the three subjects. GM presents slightly higher ampli-
tude with higher assistances (FA), which responds to
the fact that at higher assistances, the subjects per-
formed a higher range of motion gait pattern (see
section 3.2 for further details on biomechanical sig-
nals). TA presents, according to gait phases in Table 2
(Perry, 1992), a less difference between the values of
muscle activation at the endpoints in the figure (heel
strike moment, i.e. initial loading and terminal-swing
moments) and EMG values from mid-stance to mid-
AssessmentoftheSuitabilityoftheMotorizedAnkle-FootOrthosisasaDiagnosticandRehabilitationToolforGait
163
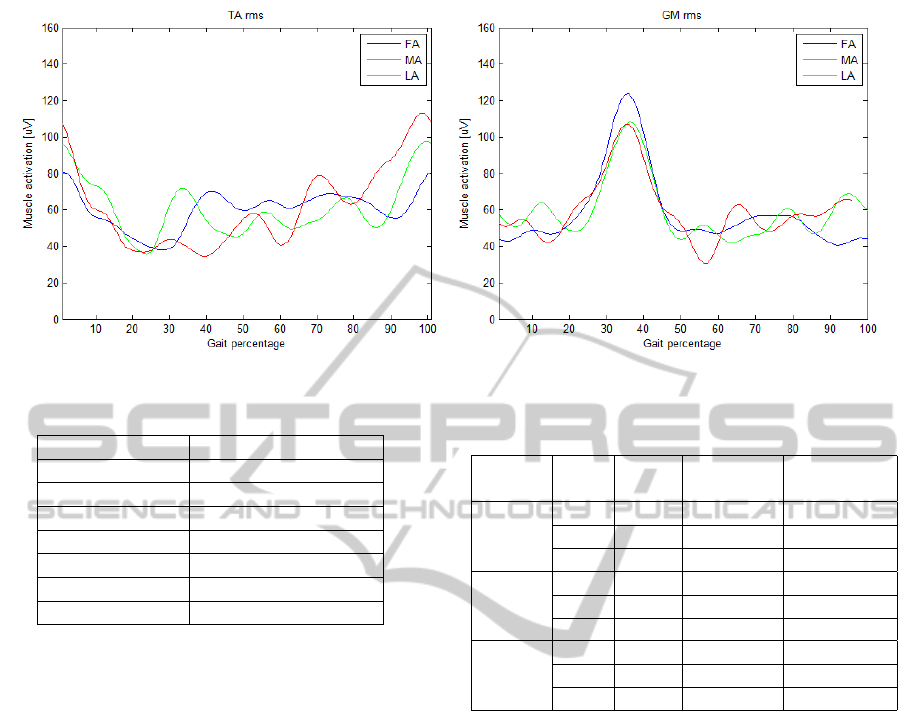
Figure 3: Mean RMS TA and GM activation; per gait phase percentage.
Table 2: Phases of the gait cycle.
Phase Percent of gait cycle
Initial loading 0 – 12
Mid-stance 12 – 30
Terminal-stance 30 – 50
Pre-swing 50 – 62
Initial-swing 62 – 75
Mid-swing 75 – 87
Terminal-swing 87 – 100
swing. These signals are consistent with data pre-
sented by Hidler and Wall (Hidler and Wall, 2005).
3.2 Biomechanical Data
Figure 4(a) presents the ankle angle. These data
shows that for lower assistances, the robot forces less
the subject to reach the imposed gait pattern, and so
the range of motion diminishes. Although the user
was told to perform a normal gait, for very low as-
sistances (LA condition) the lack of a gait reference
imposition maybe the cause of the lower range of mo-
tion.
Figure 4(b) presents the ankle velocity. These data
is a direct consequence of the angle, so the data ex-
tracted is consistent to the data for the ankle angle:
higher assistances lead to higher range of motion and
so higher velocities.
Figure 4(c) presents the torque between the sub-
ject’s foot and the robot. For lower assistances, the
imposed reference pattern is less restrictive, and so
the force the user exerts against the robot is lower, as
the robot tries to follow subject’s movements.
Mean values for the range of motion and maxi-
mum values for the velocity and torque are presented
in Table 3 for the three subjects and the three condi-
tions.
Table 3: Mean range of motion and maximum velocity and
torque for the three subjects.
Subject Trial ROM Top speed Max torque
[
◦
] [
◦
/ s] [N· m]
1 FA 24.40 84.84 10.36
MA 18.29 72.21 6.34
LA 7.15 31.32 3.68
2 FA 27.40 88.25 7.92
MA 21.38 89.20 8.25
LA 6.15 29.62 3.30
3 FA 26.50 87.87 6.61
MA 22.84 79.80 5.11
LA 14.31 57.54 4.56
4 DISCUSSION AND FUTURE
WORK
This work presented a tool to assist physiotherapists
in the rehabilitation tasks, providing not only the
movement task, but measurements to assess func-
tional improvements. The tool proved to be suitable
for these rehabilitation and assessment tasks, being
much more portable than artificial-muscle-powered
devices.
A deeper study is to be carried out enrolling more
subjects, and modifying the protocol of the current
study to perform a long term experiment, to be able to
observe the evolution on the measurements due to the
rehabilitation exercises. This will lead to the obser-
vation of short-term adaptations in muscle activation
and kinematic signals. Due to its portability, another
future could be performed overground and not over a
treadmill, thus eliminating the reflex to walk when the
“ground” moves. This approach makes the presented
experiment set-up prone to be combined with elec-
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
164
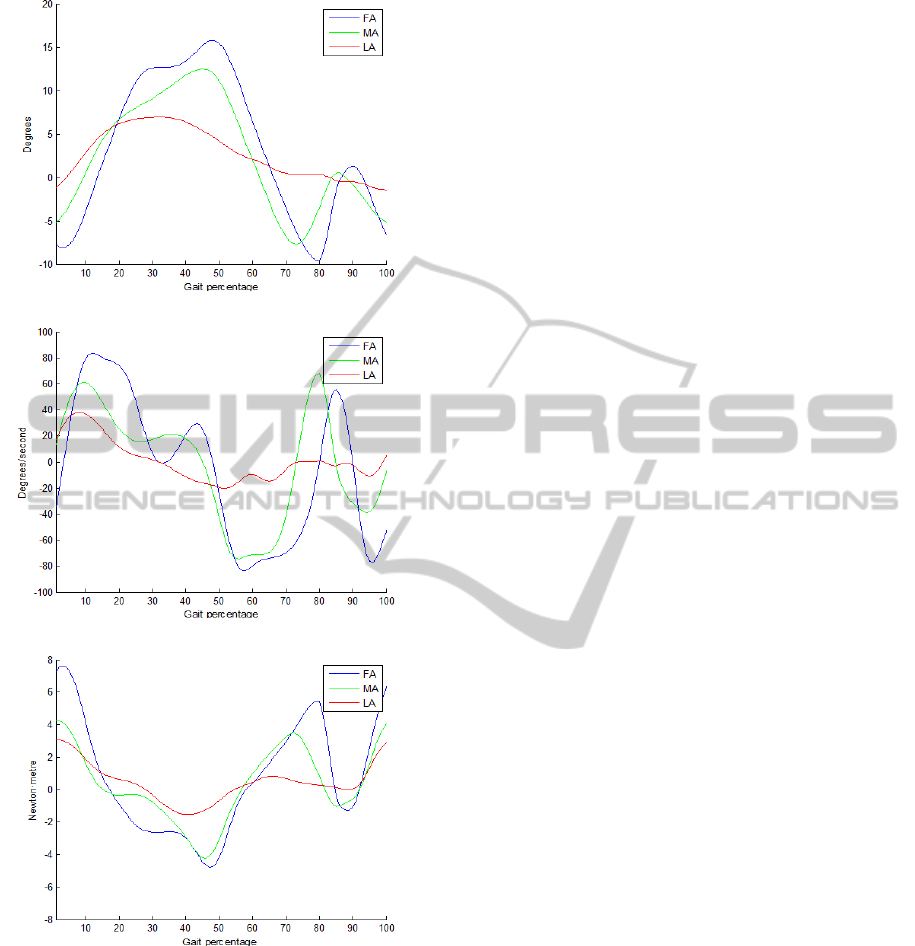
(a)
(b)
(c)
Figure 4: Biomechanical signals: angle (a), velocity (b),
and torque (c).
troencephalography to study walking intention, and
further combination of EEG and EMG data could lead
the device to be an assistive device based on a brain-
neural-computer interface.
ACKNOWLEDGEMENTS
This study has been funded by grant from the
European Commission, within the Seventh Frame-
work Programme (FP7-ICT-2009-247935: BETTER
BNCI-driven Robotic Physical Therapies in Stroke
Rehabilitation of Gait Disorders). It also has been
partially funded by grant from the Spanish Ministry of
Science and Innovation CONSOLIDER INGENIO,
project HYPER (Hybrid NeuroProsthetic and Neuro-
Robotic Devices for Functional Compensation and
Rehabilitation of Motor Disorders, CSD2009-00067).
REFERENCES
As
´
ın, G., Collantes, I., Moreno, J. C., and L, P. J. (2012).
Dise
˜
no de una
´
ortesis motorizada de tobillo para reha-
bilitaci
´
on de ictus con un enfoque top-down. In Sum-
mer School on Neurorehabilitation, 2012.
Belda-Lois, J.-M., Mena-del Horno, S., Bermejo-Bosch, I.,
Moreno, J. C., Pons, J. L., Farina, D., Iosa, M., Moli-
nari, M., Tamburella, F., Ramos, A., et al. (2011). Re-
habilitation of gait after stroke: a review towards a
top-down approach. Journal of neuroengineering and
rehabilitation, 8(1):66.
Blaya, J. A. and Herr, H. (2004). Adaptive control of a
variable-impedance ankle-foot orthosis to assist drop-
foot gait. Neural Systems and Rehabilitation Engi-
neering, IEEE Transactions on, 12(1):24–31.
Costa, N. R. and Caldwell, D. G. (2006). Control of a
biomimetic soft-actuated lower body 10dof exoskele-
ton. Proceedings of the 8th International IFAC Sym-
posiumon Robot Control SYROCO, pages 6–8.
Ferris, D. P., Czerniecki, J. M., Hannaford, B., et al. (2005).
An ankle-foot orthosis powered by artificial pneu-
matic muscles. Journal of Applied Biomechanics,
21(2):189.
Ferris, D. P., Gordon, K. E., Sawicki, G. S., and Peetham-
baran, A. (2006). An improved powered ankle–foot
orthosis using proportional myoelectric control. Gait
& posture, 23(4):425–428.
Galle, S., Malcolm, P., Derave, W., and De Clercq, D.
(2013). Adaptation to walking with an exoskeleton
that assists ankle extension. Gait & Posture.
Gordon, K. E. and Ferris, D. P. (2007). Learning to walk
with a robotic ankle exoskeleton. Journal of biome-
chanics, 40(12):2636–2644.
Hermens, H. J., Freriks, B., Merletti, R., Stegeman, D.,
Blok, J., Rau, G., Disselhorst-Klug, C., and H
¨
agg, G.
(1999). European recommendations for surface elec-
tromyography. Roessingh Research and Development
The Netherlands.
Hidler, J. M. and Wall, A. E. (2005). Alterations in muscle
activation patterns during robotic-assisted walking.
Clinical biomechanics (Bristol, Avon), 20(2):184–
193.
Hitt, J., Sugar, T., Holgate, M., Bellman, R., and Hollander,
K. (2009). Robotic transtibial prosthesis with biome-
chanical energy regeneration. Industrial Robot: An
International Journal, 36(5):441–447.
AssessmentoftheSuitabilityoftheMotorizedAnkle-FootOrthosisasaDiagnosticandRehabilitationToolforGait
165

Iosa, M., Tamburella, F., Moreno, J. C., Collantes, I., As
´
ın,
G., Aloise, F., Pisotta, I., Muzzioli, L., Mattia, D.,
Molinari, M., Pons, J. L., and Cincotti, F. (2012). Neu-
rorehabilitation after stroke: a new tool for a top-down
approach. In Terzo Congresso Gruppo Nazionale
Bioingegneria (GNB 2012).
Kao, P.-C. and Ferris, D. P. (2009). Motor adaptation during
dorsiflexion-assisted walking with a powered orthosis.
Gait & posture, 29(2):230–236.
Kao, P.-C., Lewis, C. L., and Ferris, D. P. (2010a). Invariant
ankle moment patterns when walking with and with-
out a robotic ankle exoskeleton. Journal of biome-
chanics, 43(2):203–209.
Kao, P.-C., Lewis, C. L., and Ferris, D. P. (2010b). Short-
term locomotor adaptation to a robotic ankle ex-
oskeleton does not alter soleus hoffmann reflex ampli-
tude. Journal of neuroengineering and rehabilitation,
7(1):33.
Krebs, H. I. and Hogan, N. (2006). Therapeutic robotics:
A technology push. Proceedings of the IEEE,
94(9):1727–1738.
Kwa, H. K., Noorden, J. H., Missel, M., Craig, T., Pratt,
J. E., and Neuhaus, P. D. (2009). Development of the
ihmc mobility assist exoskeleton. In Robotics and Au-
tomation, 2009. ICRA’09. IEEE International Confer-
ence on, pages 2556–2562. IEEE.
Moreno, J. C., Brunetti, F., Rocon, E., and Pons, J. L.
(2008). Immediate effects of a controllable knee an-
kle foot orthosis for functional compensation of gait
in patients with proximal leg weakness. Medical &
biological engineering & computing, 46(1):43–53.
Perry, J. (1992). Phases of gait. In Gait Analysis: Normal
and Pathological Function, pages 9–16. Slack, Tho-
rofare, NJ.
Saito, Y., Kikuchi, K., Negoto, H., Oshima, T., and
Haneyoshi, T. (2005). Development of externally
powered lower limb orthosis with bilateral-servo ac-
tuator. In Rehabilitation Robotics, 2005. ICORR
2005. 9th International Conference on, pages 394–
399. IEEE.
Sawicki, G. S. and Ferris, D. P. (2008). Mechanics and ener-
getics of level walking with powered ankle exoskele-
tons. Journal of Experimental Biology, 211(9):1402–
1413.
Sawicki, G. S. and Ferris, D. P. (2009). A pneumatically
powered knee-ankle-foot orthosis (kafo) with myo-
electric activation and inhibition. Journal of neuro-
engineering and rehabilitation, 6(1):23.
Stauffer, Y., Allemand, Y., Bouri, M., Fournier, J., Clavel,
R., Metrailler, P., Brodard, R., and Reynard, F. (2009).
The walktrainer-a new generation of walking reeduca-
tion device combining orthoses and muscle stimula-
tion. Neural Systems and Rehabilitation Engineering,
IEEE Transactions on, 17(1):38–45.
Van der Kooij, H., Veneman, J., and Ekkelenkamp, R.
(2006). Compliant actuation of exoskeletons. Mo-
bile robotics-towards new applications, Mammendorf.
ISBN, pages 978–3.
Ward, J. A., Hitt, J., Sugar, T., and Bharadwaj, K. (2006).
Dynamic pace controller for the robotic gait trainer.
ASME.
Wheeler, J. W., Krebs, H. I., and Hogan, N. (2004). An
ankle robot for a modular gait rehabilitation system.
In Intelligent Robots and Systems, 2004.(IROS 2004).
Proceedings. 2004 IEEE/RSJ International Confer-
ence on, volume 2, pages 1680–1684. IEEE.
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
166
