
New Developments in the Gesture Therapy Platform
Past, Present and Future of our Research
Felipe Orihuela-Espina
1
, Paloma
´
Alvarez-C
´
ardenas
2
, Lorena Palafox
3
, Israel S
´
anchez-Villavicencio
3
,
Alberto L. Mor
´
an
4
, Jorge H
´
ernandez-Franco
3
and Luis Enrique Sucar
1
1
National Institute for Astrophysics, Optics and Electronics (INAOE), Sta. Mar
´
ıa Tonantzintla, Puebla, Mexico
2
Universidad Veracruzana, Xalapa, Veracruz, Mexico
3
National Institute of Neurology and Neurosurgery, Mexico D.F., Mexico
4
Universidad Autonoma de Baja California (UABC), Ensenada, Baja California, Mexico
Keywords:
Virtual Rehabilitation, Stroke, Cerebral Palsy.
Abstract:
Gesture Therapy (GT) is a virtual rehabilitation tool for the upper arm that has been in the making since
2008, and by now has successfully demonstrated therapeutic validity in two small clinical trials for stroke
survivors. During this time, our group has published a number of contributions regarding different aspects of
this platform ranging from hardware controllers to artificial intelligence algorithms guiding different aspects
of the serious games behaviour, and clinical trial data from observable improvements in dexterity to changes
in functional neuroreorganization. As we continue our research efforts in virtual rehabilitation and realising
this knowledge in the GT platform, this paper presents an overview of the latest developments as well as a
roadmap for future research.
1 INTRODUCTION
Virtual rehabilitation (VR) (Levin, 2011) is becoming
an accepted alternative therapy, as evidence slowly
piles up suggesting benefits comparable to traditional
alternatives (Parsons et al., 2009; Snider et al., 2010;
Sucar et al., 2013). Yet, the full potential has not
been unleashed and evidence is still insufficient to
draw conclusions (Laver et al., 2011). Although by
now a few dozens of VR platforms exist most of them
are still confined to research labs. In most if not all
cases, VR is administered by means of serious games,
which are used for proposing, delivering, monitoring
and evaluating the therapeutic exercises in an engag-
ing and safe virtual environment.
VR platforms capable of assisting rehabilitation
must support rehabilitation principles: promote rep-
etition, task oriented training, appropriate feedback
and a motivating environment (Holden, 2005). As
such, development of these platforms is an artcraft
requiring to harmonize complex elements and pro-
cesses. Work in this area is highly multidisciplinary
involving both technical input including hardware and
electronics, software engineering, human-computer
interaction and virtual reality, and of course, clini-
cal input; rehabilitatory, neurological and psycholog-
ical. Figure 1 illustrates this multidisciplinary envi-
ronment.
Since 2008, our group has been proposing contri-
butions in VR research across the many subdomains
Figure 1: Developing a VR platform requires a multidisci-
plinary work.
106
Orihuela-Espina F., Álvarez-Cardenas P., Palafox L., Sánchez-Villavicencio I., L. Morán A., Hérnandez-Franco J. and Sucar L..
New Developments in the Gesture Therapy Platform - Past, Present and Future of our Research.
DOI: 10.5220/0004663801060113
In Proceedings of the International Congress on Neurotechnology, Electronics and Informatics (VirtRehab-2013), pages 106-113
ISBN: 978-989-8565-80-8
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

of the field. From engineering to clinical applications,
and from traslational research to neuroergonomics;
we have contributed with controllers for arm and fin-
ger exercising (Sucar et al., 2013), different artifi-
cial intelligence based adaptation algorithms to make
the therapy adjusts to the changing needs of the pa-
tient as well as learning instructions from the ther-
apist (
´
Avila-Sansores et al., 2013), a compensation
detection algorithm that can ensure trunk compensa-
tion is avoided (Sucar et al., 2009), an initial set of
necessary design criteria for serious games develop-
ment in VR (Oropeza Salas, 2012), a set of serious
games formulated capitalizing on these design princi-
ples (Oropeza Salas, 2012; Sucar et al., 2013), clini-
cal evidence of the validity of the technique as com-
pared to occupational therapy (Sucar et al., 2010),
and an initial picture of how the brain responds to
VR in terms of functional reorganization strategies
(Orihuela-Espina et al., 2013). In parallel to this re-
search efforts, we have been developing the platform
Gesture Therapy (GT) (Sucar et al., 2010; Sucar et al.,
2013), the practical realization of all the knowledge
we have been gathering. Of course, the field of neu-
rorehabilitation is still in its infancy with rehabilita-
tion treatments having a disappointingly modest ef-
fect on impairment (Krakauer et al., 2012) and thus
the journey has just begun.
This paper presents some of the latest features
added to the GT platform; two more new games, a
brand new interface inspired in the home paradigm
that serious games should reflect functional tasks of
daily living, and the new user profiling capabilities.
The goal pursued by the incorporation of these fea-
tures is facilitating translational research e.g. mak-
ing possible point-of-care patient application, as well
as enabling more ecological testing environments e.g.
the patient’s home. This paper also presents prelimi-
nary steps taken to demonstrate (i) that the same plat-
form can be shared across different medical condi-
tions responsible of upper limb impairment, in partic-
ular from stroke to cerebral palsy, and (ii) that serious
games originally developed for VR can also be useful
beyond their original intended domain and can further
help to ease cognitive decline. Finally, we also want
to use this paper to sketch some of the work ahead.
2 GESTURE THERAPY (GT)
GT is a VR platform for the motor rehabilitation of
the impaired upper limb. GT was conceived for home
usage and consequently exhibits low cost. The plat-
form has two major hardware elements pictured in
Figure 2; a computer with a webcam and a controller
Figure 2: The Gesture Therapy platform. The user interacts
with the games by means of the gripper.
or gripper. This specifically designed controller facil-
itates arm and hand tracking and incorporates a pres-
sure sensor for flexion of fingers. The solution mixes
hardware and software elements in an integrated plat-
form with five major modules schematically depicted
in Figure 3.
• The physical system encompasses the hardware
platform incorporating a computer, a webcam for
tracking and specifically designed controllers e.g.
a handgrip.
• The monocular tracking system is the software
responsible for tracking the arm surrogated by the
controller’s ball. Tracking is based on a particle
filter using colour and texture and is capable of
estimating depth.
• The simulated environment presents the games
and interacts with the user. It is also responsible
for providing visual and auditory feedback.
• The trunk compensation detector controls the
platform response to detected compensatory
movements with the trunk by the patients. It cap-
italizes on Haar features and a cascade of classi-
fiers.
• Finally, the adaptation module adjusts the 3D
space in which the exercise occurs intra-game in
real time tailoring the challenge to the progress of
the patient. The underlying algorithm exploits so-
phisticated artificial intelligence decision models.
Further details of the platform status before this pub-
lication can be found in (Sucar et al., 2013). This pa-
per presents the new modifications and enhancements
made to the platform since then.
2.1 Clinical Trials
So far, we have carried out two clinical trials, both
in Mexico at the National Institute of Neurology and
Neurosurgery and focused on stroke patients.
NewDevelopmentsintheGestureTherapyPlatform-Past,PresentandFutureofourResearch
107

Figure 3: Conceptual modules of the GT platform.
• Clinical Trial I. 42 patients were randomised to
two groups; a control group of 22 patients re-
ceived 21 sessions of 60 minutes of occupational
therapy, and the intervention group received an
equal amount of virtual reality based rehabilita-
tion therapy with Gesture Therapy. Both groups
presented a significant improvement in terms of
motor recovery assessed using Fugl-Meyer (Fugl-
Meyer et al., 1975) and Motricity Index (De-
meurisse et al., 1980) scales (Wilcoxon; p <
0.05). Differences in improvement between the
therapies were not significant. Motivation as
evaluated with the Intrinsic Motivation Inventory
(IMI) (McAuley et al., 1989) was stronger among
patients treated with Gesture Therapy. Patients
treated with GT demonstrated greater interest and
claimed higher importance and utility. Full details
can be found in (Sucar et al., 2010).
• Clinical Trial II. 28 subjects were allocated to 3
groups; group one received 20 sessions of 45 min-
utes of occupational therapy, whilst groups 2 and
3 received equal amount of Gesture Therapy, with
the third group further undergoing neuroscans for
exploration of the neural underpinnings respon-
sible for behavioural improvements. Both thera-
pies exhibited significant motor improvements as
evaluated with Fugl-Meyer and Motricity Index
(Mann-Whitney U; p < 0.05), and differences in
improvements between them were not significant.
GT matched the control improvements for hand,
wrist and elbow. Prefrontal cortex and cerebel-
lar activity were found to be the driving forces of
the recovery associated with Gesture Therapy. We
found that those with stronger disabilities appear
to benefit the most from this paradigm (Orihuela-
Espina et al., 2013).
3 NEW TECHNICAL FEATURES
FOR GT
3.1 New Games
Two new games have been added to the game set of
GT that until now had 3 games. The new games at-
tend the obvious necessity for a larger variety of tasks
to reduce boredom caused by excessive repetition of
games in a game set. Also by diversifying the tasks
the enlarged game set might appeal to other patients.
Screenshots of the games are pictured in Figure 4.
• Spiders on the Wall. In this game the pa-
tient armed with a hammer as an unlikely tool
for killing spiders has to combat these annoy-
ing creatures creeping up the wall. The distance
at which the next spider appears is dictated by
the challenge level at play which in turn is gov-
erned by the adaptation policy, optimally designed
to ensure matching user progress. The game
favours bidirectional movements including eleva-
tion/depression and abduction/adduction.
• Fungi in the Sink. Cleaning time. The sink is
dirty and the patient has to clean the mold stains.
Similarly, the distance at which the next mold
stain appears is dictated by the challenge level
again ruled by the adaptation module. The game
also favours bidirectional movements including
elevation/depression and abduction/adduction.
Similarly to previous games in GT, these have
been developed using the Torque game engine and
communicate with the rest of the platform by means
of a shared memory address. They both incorporate
visual and audio feedback and this is given in the
two classical flavours; knowledge of performance and
knowledge of results (Deutsch et al., 2008). These
games still have to face clinical trialling.
3.2 New Interface
The home paradigm is our conceptualization that ex-
ercises promoted by the serious games should mimic
natural movements inspired in functional tasks of
daily living mostly occurring in the home environ-
ment, thus stressing the rehabilitation goal of mak-
ing the patient self-sufficient (at home). Although the
paradigm has been integral to GT for a while now
(Oropeza Salas, 2012), it has not been until recently
that we have developed a brand new interface that re-
ally exploits this paradigm. The new interface inte-
grates the menus to be navigated by the patient within
different views of a house from outside and from the
inside as illustrated in Figure 5. A lighting effect
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
108

Figure 4: Screenshots of the two new games added to GT’s
game set.
highlights buttons as the user crosses above them with
the cursor. Currently, navigation through the interface
is made by means of the mouse, but we expect the GT
gripper to be also an optional input device for the in-
terface very soon, thus further facilitating the use by
the impaired person without help from thirds.
3.3 User Profiling Capabilities
User profiling refers to all the managerial capabili-
ties to track patients and physicians use of the system,
as well as the therapy compliance of the former and
the clinical annotations of the latter. We have now en-
riched GT with user profiling capabilities, a necessary
addition for regular use whether at home or in health
institutions. The user profiling capabilities of GT con-
form a new module (to add to those in Figure 3) that
tracks all activity occurring in an instance of GT.
The database is implemented in postgreSQL and
permits tracking of user activity. From the patient
point of view it tracks times spent on the therapy,
and in each particular game individually. It further
keeps track of the traces of the user avatar at all times
Figure 5: The new interface inspired in the home paradigm.
Top: Different elements of the facade of the house (i.e. win-
dows) disguise the main menu. Bottom: The house inte-
rior permits access to the different games in different rooms
highlighting the relation between the exercise and the func-
tional task associated.
and records timestamps and performances associated.
Therapies can be delivered following game selection
by the therapist or a pre-dictated plan. The therapist
can add clinical annotations to every session played
by the patient. The Entity-Relation diagram of the
database is shown in Figure 6.
4 CLINICAL EXPLORATION
BEYOND STROKE
4.1 Extension to other Motor Impairing
Conditions: Cerebral Palsy
Because of the large prevalence and incidence of
stroke (Roger et al., 2012), GT was originally de-
veloped focused on these patients. However, as the
main principles of motor rehabilitation are shared
with other motor impairing medical conditions, it is
likely that a platform developed for stroke would also
be suitable for treating the rehabilitation process of
these other conditions. In this sense, we have already
started a clinical trial to test the feasibility of using
GT in children with cerebral palsy. However, as the
game set of GT was thought for adults, we have tem-
porally borrowed games from the Armeo system (Ho-
coma, 2013); an strategy that we already used in the
past before GT had its initial game set.
NewDevelopmentsintheGestureTherapyPlatform-Past,PresentandFutureofourResearch
109
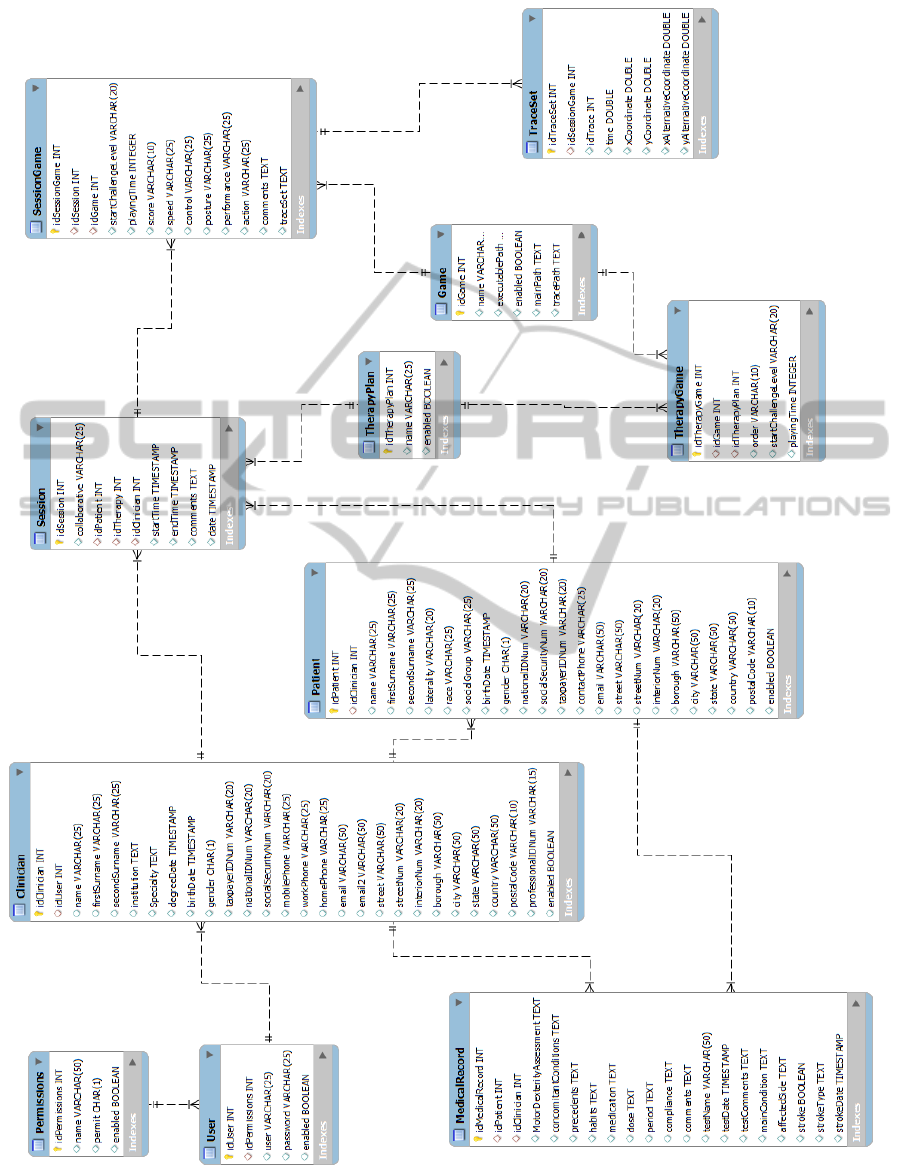
Figure 6: The diagram representing the database supporting the user profiling capabilities.
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
110
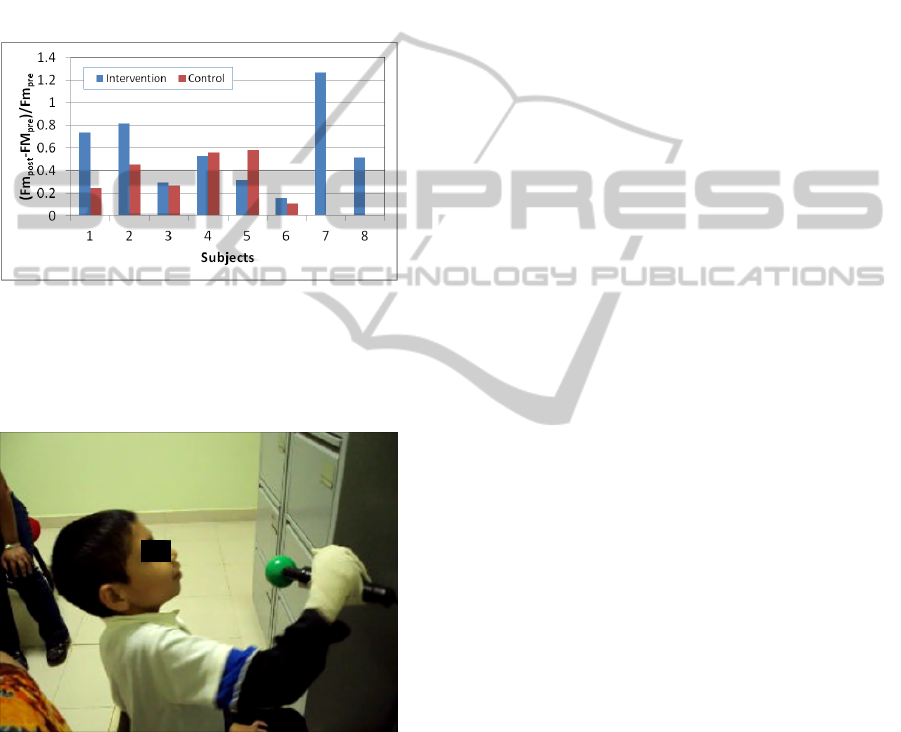
So far data from 14 patients of palsy have been
collected from two groups following a between
groups pre-post design; a control group following an
occupational therapy and an intervention group that
has been administered Gesture Therapy. Motor dex-
terity improvements have been measured by means of
Fugl-Meyer scale (Fugl-Meyer et al., 1975) measured
prior to therapy onset and after therapy ends. Inter-
mediate results so far are illustrated in Figure 7. A
patient of palsy using GT during the most recent trial
is shown in Figure 8.
Figure 7: Normalised improvement achieved by the patients
in the ongoing clinical trial. Pairing of bars is only for il-
lustrative purposes, but it is not meant to represent the ex-
perimental design (between groups). Large benefits can be
appreciated in those patients allocated to the intervention
group.
Figure 8: A patient of palsy using GT during the most recent
trial.
4.2 Extension to other Medical
Domains: Cognitive Decline
A current trend in VR is exploiting commercially
available platforms such as the Wii, the Xbox, the
PlayStation or the Kinect to reduce costs and afford
faster developing times. Off-the-shelf game sets for
these platforms hardly ever are suited for rehabilita-
tion and may lack essential components for ensuring
therapeutic effectiveness. An unconventional alterna-
tive might be to bridge domains, and reutilize seri-
ous games out of their original intended context. The
hypothesis is that serious games specifically designed
for a certain purpose can escape their realm to be used
in other more or less related purposes.
In this sense, we are evaluating the appealing of
virtual games originally developed for motor rehabil-
itation in GT, to be used for enhancing cognitive stim-
ulation of older adults (Mor
´
an et al., 2013).
We have chosen cognitive stimulation as a target
application for exporting virtual rehabilitation games
because the population affected by cognitive decline,
i.e. elders, is also the population most affected by
stroke; the original target population of GT. The se-
lection of this sufficiently close domain can boost the
chances of the exported games to be successful in
their new domain; yet, the new functional require-
ments in the new domain (cognitive stimulation) are
different enough from the original domain (virtual re-
habilitation) to represent a considerable challenge in
the migration.
Towards this end we conducted a usability evalu-
ation of GT as a cognitive stimulation tool with 32 el-
ders from a local municipal third-age support group.
Participants were exposed to a subset of the games
currently available from the GT platform (steak cook-
ing, window cleaning and fly killer). The elderly were
asked to evaluate the platform in terms of perceived
usefulness, ease of use and user experience. The main
goal was to assess GT’s usability aspects as a bor-
rowed platform from the rehabilitation domain.
Elders were introduced to the use of the tool (2-
minute demo), later they were allowed to freely ex-
plore its use to familiarize with it and solve any doubts
regarding its use (3-minute training session), and then
they were allowed to play a complete session with
each of the three games (15-minute play session in
total). Finally, the elders answered an on-exit ques-
tionnaire regarding their perception on the use of the
tool using a set of TAM-based items (Venkatesh and
Davis, 2000) and open questions.
Results from the analysis of the TAM-based items
support that elders perceived the GT platform as a
useful (93.75/100), easy to use (93.75/100) and plea-
surable to use (91.66/100) cognitive stimulation tool.
However, results from the open questions data pro-
vide evidence about elders considering the proposed
activities (games) as being entry level cognitive stim-
ulation activities, and recommended to include ad-
ditional more challenging activities such as puzzles,
memory games or simple math problems.
These results suggest that the transfer of games
across realms could be, in some cases, a feasible
NewDevelopmentsintheGestureTherapyPlatform-Past,PresentandFutureofourResearch
111

enterprise but their effectiveness and usability may
be compromised, thus demanding small adaptations.
This is encouraging as small adaptations might be less
costly and faster to perform than starting new games
from scratch.
5 ROADMAP FOR RESEARCH
ASSOCIATED WITH GT
During this journey GT has become a solid piece of
research in virtual rehabilitation with contributions in
many aspects of the domain. Yet, research continues
at our laboratory. These are a few of the efforts we
plan to make in the near future:
• Games Design Criteria. The design criteria tax-
onomy in (Oropeza Salas, 2012) is a naive effort.
Encompassing the rehabilitation goals is arduous,
but a few game design criteria are already spring-
ing for facilitating the development of rehabilita-
tory serious games e.g. (Flores et al., 2008), an
effort which is so far uncoordinated. It is desir-
able to establish a framework of serious game de-
sign criteria and guidelines for virtual reality re-
habilitation, and identifying critical elements that
make a game an effective tool for rehabilitation.
We aim to demonstrate that by better understand-
ing the necessities of rehabilitation games, spe-
cific aspects of the development process of seri-
ous games for rehabilitation can be streamlined,
thus speeding up the development of platforms for
supporting virtual reality based therapies.
• Transfer of Knowledge. The question of how
virtual practice translates to the real world is not
new (Holden, 2005), yet remains largely unex-
plored. The overlap between the real and the vir-
tual task must be understood to optimize or facil-
itate transfer. It is not sufficient simply to demon-
strate that training does transfer in a given situa-
tion; rather, it is crucial to identify whether a spe-
cific skill is being transferred (Sveistrup, 2004).
We believe it is critical to investigate indispens-
able elements that make a serious game an effec-
tive tool for rehabilitation, with special emphasis
on transfer of knowledge from the virtual to the
real world and identifying game elements that in-
crease adherence to the games and by extension
to the therapy. Additionally, this may reduce the
excessive reliance on premature clinical trials.
• Functional Reorganization of the Brain.
Krakauker got it right (Krakauer et al., 2012);
training of compensatory strategies have minimal
impact on impairment. Current understanding
of motor learning and brain plasticity has to be
a primary research direction. Our only study
so far in this direction (Orihuela-Espina et al.,
2013) was just an initial step, and was limited by
the enforced imagery-based task imposed by the
fMRI neuroimaging modality. We believe that
employing other neuroimaging techniques such
as diffuse optical neuroimaging (Villringer and
Chance, 1997) will permit us to interrogate the
brain with higher ecological validity, even if that
means sacrificing some spatial resolution.
6 CONCLUSIONS
This paper has summarised our current research ef-
forts in the different areas of VR, and in particular
how these efforts are being coordinated around the
GT platform. By enlarging our gameset, the new
games will give patients more variability and we ex-
pect this to result in higher motivation and adherence
to therapy. The new interface makes the platform
more user friendly, dropping the need for a researcher
or therapist trained in the platform to be present at
all times. In this sense, installation and application
launch are now trivial, software is all integrated in a
single executable (previously the tracking and games
have to be launched separately), and menu naviga-
tion is expected to be more natural. Also, the new
user profiling capabilities was a necessary step be-
fore more ecologically aggressive trials could be at-
tempted opening the door for releasing the platform
to more rehabilitation wards and ultimately, the pa-
tient’s home without direct or on-site clinical super-
vision. Efforts are being also made to extrapolate the
virtual paradigm of GT beyond stroke. First steps in-
volve extension to other motor impairing conditions
(e.g. palsy) and other less similar medical domains
(e.g. cognitive decline). Preliminary results in both
directions are promising. Finally, we have also re-
flected about near future research that we think might
make an impact on VR. We look forward to keep ad-
vancing knowledge that can consolidate VR as a cut-
ting edge alternative for motor rehabilitation and re-
covery from impairment.
ACKNOWLEDGEMENTS
The authors would like to thank R. Leder, R. L.
Vel
´
azquez, H. Avil
´
es-Arriaga, S.
´
Avila-Sansores, J.
Oropeza-Salas and D. Carrillo who have actively col-
laborated in the building of the Gesture Therapy plat-
form. This work has been funded by the following
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
112

projects: SALUD-2007-C01-70074 from the CONA-
CYT, Project 95185 from the FONCICYT (European
Union-Mexico), and the MARSRERC program of the
Rehabilitation Institute of Chicago.
REFERENCES
´
Avila-Sansores, S. M., Orihuela-Espina, F., Sucar, L. E.,
and
´
Alvarez-C
´
ardenas, P. (2013). Adaptive deci-
sion models for virtual rehabilitation environments.
In International Conference on Machine Learning
(ICML’2013) Workshop on Role of Machine Learning
in Transforming Healthcare (WHEALTH), page 9 pp.,
Atlanta, USA.
Demeurisse, G., Demol, O., and Robaye, E. (1980). Motor
evaluation in vascular hemiplegia. European Neurol-
ogy, 19:382–389.
Deutsch, J. E., Borbely, M., Filler, J., Huhn, K., and
Guarrera-Bowlby, P. (2008). Use of low-cost, com-
mercially available gaming console (wii) for rehabil-
itation of an adolescent with cerebral palsy. Physical
Therapy, 88(10):1196–1207.
Flores, E., Tobon, G., Cavallaro, E., Cavallaro, F. I., Perry,
J. C., and Keller, T. (2008). Improving patient mo-
tivation in game development for motor deficit reha-
bilitation. In Inakage, M. and Cheok, A. D., editors,
Proceedings of the 2008 International Conference
on Advances in Computer Entertainment Technol-
ogy (ACE’2008), pages 381–384, Yokohama, Japan.
ACM.
Fugl-Meyer, A. R., Jsk, L., Leyman, I., Olsson, S., and
Steglind, S. (1975). The post-stroke hemiplegic pa-
tient. 1. a method for evaluation of physical per-
formance. Scandinavian Journal of Rehabilitation
Medicine, 7(1):13–31.
Hocoma (2013). Armeo therapy concept. http://
www.hocoma.com/products/armeo/.
Holden, M. K. (2005). Virtual environments for motor re-
habilitation: Review. CyberPsychology & Behavior,
8(3):187–211.
Krakauer, J. W., Carmichael, S. T., Corbett, D., and Witten-
berg, G. F. (2012). Getting neurorehabilitation right:
what can be learned from animal models? Neurore-
habilitation and Neural Repair, Epub ahed of print:9
pp.
Laver, K. E., Stacey, G., Thomas, S., Deutsch, J. E., and
Crotty, M. (2011). Virtual reality for stroke rehabili-
tation. Cochrane Database of Systemic Reviews, 9:70
pp.
Levin, M. F. (2011). Can virtual reality offer enriched envi-
ronments for rehabilitation? Expert Reviews of Neu-
rotherapeutics, 11(2):153–155.
McAuley, E., Duncan, T., and Tammen, V. V. (1989). Psy-
chometric properties of the intrinsic motivation inven-
tory in a competitive sport setting: a confirmatory
factor analysis. Research Quarterly for Exercise and
Sport, 60(1):48–58.
Mor
´
an, A. L., Orihuela-Espina, F., Meza-Kubo, V.,
Grimaldo-Mart
´
ınez, A. I., Ram
´
ırez-Fern
´
andez, C.,
Garc
´
ıa-Canseco, E., Oropeza-Salas, J. M., and Sucar,
L. E. (2013). Borrowing a virtual rehabilitation tool
for the physical activation and cognitive stimulation
of elders. In 6th Latin American Conference on Hu-
man Computer Interaction (CLIHC 2013).
Orihuela-Espina, F., Fern
´
andez del Castillo, I., Palafox,
L., Pasaye, E., S
´
anchez-Villavicencio, I., Leder, R.,
Hern
´
andez-Franco, J., and Sucar, L. E. (2013). Neu-
ral reorganization accompanying upper limb motor re-
habilitation from stroke with virtual reality-based ges-
ture therapy. Accepted in Topics in Stroke Rehabilita-
tion, page 27 pp.
Oropeza Salas, J. M. (2012). Dise
˜
no de un ambiente
virtual orientado a la rehabilitaci
´
on de las extremi-
dades superiores. BSc thesis, Benem
´
erita Universidad
Aut
´
onoma de Puebla.
Parsons, T. D., Rizzo, A. A., Rogers, S., and York, P. (2009).
Virtual reality in paediatric rehabilitation: a review.
Developmental Neurorehabilitation, 12(4):224–238.
Roger, V. L., (and 39 other authors on behalf of the Ameri-
can Heart Association Statistics Committee, and Sub-
committee), S. S. (2012). Heart disease and stroke
statistics - 2010 update a report from the American
Heart Association. Circulation, 125:e2–e220.
Snider, L., Majnemer, A., and Darsaklis, V. (2010). Vir-
tual reality as a therapeutic modality for children with
cerebral palsy. Developmental Neurorehabilitation,
13(2):120–128.
Sucar, L. E., Luis, R., Leder, R., Hernndez, J., and Snchez,
I. (2010). Gesture therapy: A vision-based system for
upper extremity stroke rehabilitation. In 32nd Annual
International Conference of the IEEE Engineering in
Medicine and Biology Society (EMBS), pages 3690 –
3693, Buenos Aires, Argentina. IEEE.
Sucar, L. E., Molina, A., Leder, R., Hernndez, J., and
Snchez, I. (2009). Gesture therapy: a clinical eval-
uation. In 3rd International Conference of the Insti-
tute for Computer Sciences, Social-Informatics and
Telecommunications Engineering (ICST) on Perva-
sive Computing Technologies for Healthcare (Perva-
sive Health 2009), pages 1–5, London, UK. IEEE.
Sucar, L. E., Orihuela-Espina, F., Vel
´
azquez, R. L.,
Reinkensmeyer, D. J., Leder, R., and Hern
´
andez-
Franco, J. (2013). Gesture therapy: An upper limb vir-
tual reality-based motor rehabilitation platform. Sub-
mitted to IEEE Transactions on Neural Systems and
Rehabilitation Engineering, page 10pp.
Sveistrup, H. (2004). Motor rehabilitation using virtual re-
ality. Journal of NeuroEngineering and Rehabilita-
tion, 1:10 (8 pp.).
Venkatesh, V. and Davis, F. (2000). A theoretical extension
of the technology acceptance model: four longitudinal
field studies. Management Science, 46(2):186–204.
Villringer, A. and Chance, B. (1997). Non-invasive optical
spectroscopy and imaging of human brain function.
Trends in Neuroscience, 20(10):435–442.
NewDevelopmentsintheGestureTherapyPlatform-Past,PresentandFutureofourResearch
113
