
Evaluation of Motion Controlled Arm Support
A. Bergsma
1,2
, L. A. van der Heide
3,4
, J. M. N. Essers
1
, A. Murgia
5
, D. van der Pijl
6
, E. C. Cup
2
,
G. J. Gelderblom
3
, P. H. Verstegen
6
, I. J. M. de Groot
2
and K. Meijer
1
1
Maastricht University Medical Centre+, Department of Human Movement Sciences, Maastricht, The Netherlands
2
Radboud University Nijmegen, Medical Centre, Nijmegen Centre for Evidence based Practice,
Department of Rehabilitation, Nijmegen, The Netherlands
3
Zuyd University of Applied Sciences Heerlen, Research Center for Technology in Care, Heerlen, The Netherlands
4
Maastricht University, School for Public Health and Primary Care (CAPHRI), Maastricht, The Netherlands
5
University Medical Center Groningen, Center for Human Movement Sciences, Groningen, The Netherlands
6
FOCAL Meditech Bv, Tilburg, The Netherlands
1 OBJECTIVES
Assistive devices augmenting arm functionality in
the weak upper extremity were introduced
extensively after the polio epidemic in the 1940s.
Many attempts have been made to help people with
upper extremity limitations in daily life by means of
dynamic arm supports. Current devices vary from
passive supports, with low level of complexity and
easy to control, providing limited support in the
performance of ADL tasks to active arm supports
with many functionalities, large dimensions and
complex control (van der Heide, 2013). An example
of a new development is the motion-controlled arm
support (McArm) that aims to enhance the
functional benefit of support while maintaining the
user friendliness of the simple passive support
systems. In addition, it aims to stimulate the use of
residual muscle strength in the user (Focal Meditech
BV, 2013).
The effect of support on human arm movements
needs to be investigated to understand how support
can be optimized. The influence of assistive devices
that compensate weakened muscles on the
restoration of arm functions after stroke, has been
investigated by Prange et al. (Prange, 2009). They
have studied the effect of gravitational pull of arm
support systems with braces. They found that the
activity level of shoulder and upper arm muscles
during reaching movements using a forearm support
system are significantly decreased. However there is
still little evidence on how joint moments are
changed by a support system and whether zero
gravity support is the best biomechanical solution
that designers should aim for. Moreover, it is still
unclear how joint moments are affected in people
suffering from for example neuromuscular diseases
and how people perform with an arm support in a
daily life situation. Information on the effects of
dynamic arm supports on arm movements and use of
arm supports in daily life is needed to provide
insight in the limitations of current designs. That
knowledge can be used in the development of new
motion controlled arm support.
The aim of this study was to investigate the
impact of arm support systems on the arm function
and use in daily life. This was realized by studying
the effect of an available support system on the arm
function at various levels of the International
Classification of Functioning, Disability and Health
(ICF). This knowledge is integrated in the design of
the new McArm.
2 METHODS
A test battery has been developed that combines
questionnaires and ordinal clinical scales, with
quantitative measures such as 3D motion analysis
and EMG to provide a more complete picture of the
compensatory movement patterns used by patients
with proximal muscle weakness of the upper
extremities in patients with neuromuscular disorders.
Moreover, biomechanical models and inverse
dynamic software were used to calculate the
shoulder and elbow joint moments in three different
conditions (a control set-up, a gravity compensation
set-up and a simulated zero gravity environment).
These measures were used to investigate movement
capacities of people with various neuromuscular
disorders. To evaluate the performance in daily life,
a measurement protocol has been developed to
measure how people use the arms and the arm
support during daily activities.
The following paragraphs describe the structure
of the various measures and the first results.
Bergsma A., van der Heide L., M. N. Essers J., Murgia A., van der Pijl D., C. Cup E., J. Gelderblom G., H. Verstegen P., J. M. de Groot I. and Meijer K..
Evaluation of Motion Controlled Arm Support.
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

2.1 Questionnaires
A web-based questionnaire containing questions on
all ICF domains, was composed to evaluate overall
arm function and problems people encounter in daily
life. This questionnaire was distributed among
various groups of people with neuromuscular
diseases, namely Duchenne muscular dystrophy
(DMD), fascioscapulohumeral dystrophy (FSHD),
limb-girdle muscular dystrophy (LGMD) and spinal
muscular atrophy (SMA).
2.2 3D Kinematics and EMG
Motion analysis and electromyography (EMG) data
from various tasks (e.g. shoulder abduction/flexion,
reaching and hand to mouth movement) were
recorded during unsupported movement and during
supported movement with a passive Sling arm
support (Focal Meditech). In both cases the subject
was asked to move the dominant hand from an initial
position resting on a table in the sagittal plane to a
target placed at a distance of a stretched arm, at
shoulder height and one shoulder width on the
ipsilateral side. The movements were recorded with
a 3D camera Motion Capture system (Vicon).
Reflective markers were attached on the subject’s
body following the guidelines of the Vicon Upper
Limb model. These data were subsequently used in
simulations with a multi-body model of the arm to
calculates joint moments. EMG data were obtained
from biceps brachii, deltoid, triceps brachii,
trapezius, pectoralis and latissimus dorsi muscles
and were normalized as percentage of the EMG
during maximum voluntary contraction.
2.3 Muscle-skeletal Simulations
The coordinates of the reflective markers during the
unsupported and supported ipsilateral reaching
movements were used to drive the simulation model
in the AnyBody Modeling System (AnyBody
Technology). With the subject’s anthropometric
information derived from marker coordinates, the
software’s GaitFullBody model was scaled
according to body length and mass among others.
An inverse dynamic analysis was then carried out to
calculate the net joint moments at the shoulder and
elbow. The analysis on the unsupported movement
consisted of two parts: a normal gravity situation
and a simulated zero gravity situation, in which the
same motion data for the unsupported movement
were used but gravity was set to zero in AnyBody’s
model parameters. As a result the outputs of the
calculation were the net joint moments in three
conditions: I control, II gravity compensation with
Sling and III zero gravity environment. These
conditions were chosen to assess the influence of
gravity compensation (I vs. II), the influence of a
zero gravity environment (I vs. III) and the
difference between gravity compensation induced
either by a mechanism or resulting from a zero
gravity environment (II vs. III)(Essers, 2013).
2.4 Ambulatory Performance
To evaluate the effect of arm supporting devices in a
daily life setting, a protocol for monitoring the arm
activity outside a laboratory setting was developed.
A tri-axial accelerometer (MOX, Maastricht
Instruments) was placed on the upper arm just above
the elbow. The acceleration signals were post-
processed to obtain elevation and intensity of upper
arm movements. These data give an indication on
how and how often the arm support is used in daily
life (Annegarn, 2012).
3 RESULTS
Preliminary results for the various studies are
shown.
3.1 Questionnaires
In total of 315 boys/men with DMD, 88 with FSHD,
61 with LGMD and 73 with SMA participated.
Preliminary data show that pain, stiffness and
functional limitations increased with age in DMD.
Data of FSHD, LGMD and SMA are being
analysed.
3.2 3D Kinematics and EMG
The maximum shoulder elevation angles and the
minimal and maximal elbow flexion angles were
analysed in a group of 11 people with FSHD and in
a group of 8 healthy controls. The data depicted in
figure 1 represent the shoulder elevation angles of
the healthy control group and the data of the FSHD
subjects. Significant differences between the
shoulder angles of the FSHD and the healthy control
group were found for the shoulder elevation angle
during the abduction and flexion tasks and during
the two reaching tasks. Of the 11 subjects, only two
were able to elevate the arm above 90 degrees. The
EMG data showed higher percentages in the FSHD
FSHD group compared to the control group.
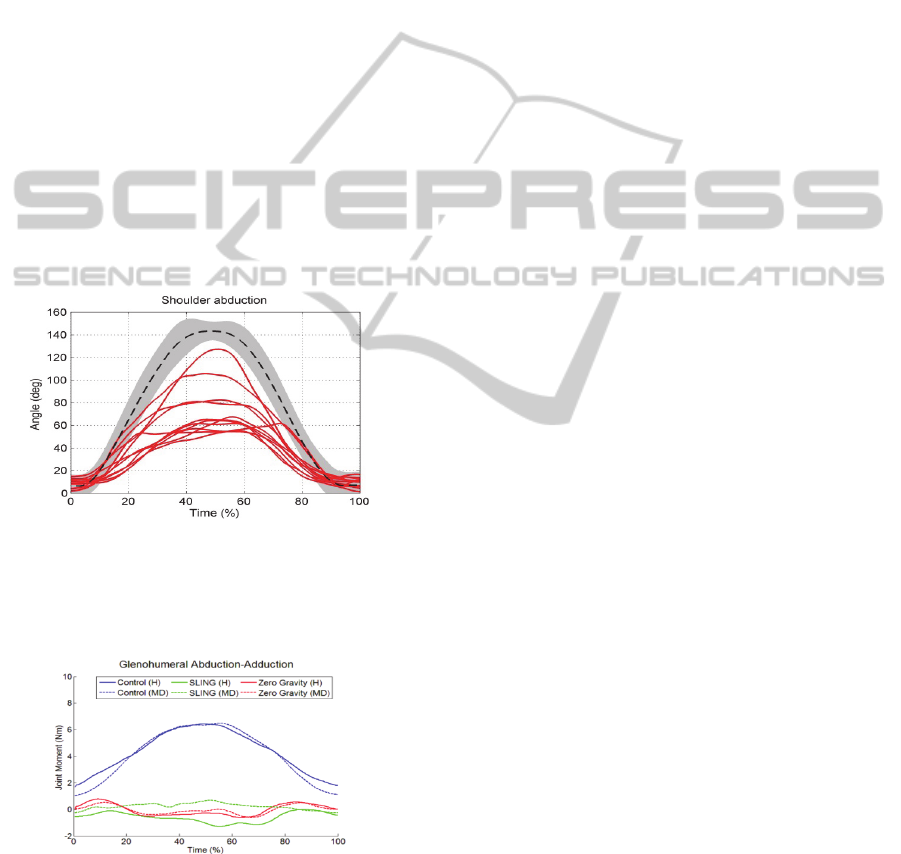
3.3 Muscle-skeletal Simulations
The ipsilateral reaching task was completed by all
subjects in all conditions. The FSHD subjects
required more time to complete the task in the
Control and the Sling condition than the healthy
group (respectively 2.6 vs. 3.7s and 2.8 vs. 4.7s).
Both groups required more time to complete the task
in the Sling condition than in the control situation. In
the control situation, the maximum value of the
moment was greater by more than one order of
magnitude than the moment in the Sling and the
Zero gravity conditions in both groups (Figure 2).
Between the two groups the signs of the average
moments in the Sling condition were different,
showing for the FSHD group a trend to maintain the
arm more elevated and the elbow more flexed. The
healthy group presented a lower mean moment in
the Sling condition than the FSHD group, showing a
trend to maintain the arm less elevated and the
elbow more extended when using the Sling (Essers,
2013).
Figure 1: maximum shoulder elevation angle of shoulder
abduction. The grey band represents the 95% confidence
interval of the control group, the dashed lines represent the
average of the control group and the continuous lines
represent a group of 11 FSHD subjects.
Figure 2: Joint Moments of glenohumeral abduction-
adduction.
3.4 Ambulatory Performance
In a group of 12 healthy men, the activity of the arm
that was performed in one day was measured. 40%
of the total upper arm activity was categorized as
low intensity and low elevation. Less than 2% was
classified as high elevation. The average number of
elevations above 90 degrees was for most subjects
less than 10 times per hour.
4 DISCUSSION
The current study presents some preliminary results
of initial evaluation measures. Application of these
evaluation measures for the next McArm prototype
is foreseen for the last stage of the project. The goals
of these evaluations are multiple: to see if design
goals and specifications are met, to gain first
outcomes on usage and usability of the new device,
and compare functionality with high- end existing
devices of this class. For this purpose several
existing measurement scales and instruments were
combined into a specific set. The availability of such
a set will be applicable for evaluation of support
systems.
ACKNOWLEDGEMENTS
The project McArm is a national Dutch ‘Pieken in
de Delta’ project, partially funded by Agentschap
NL.
REFERENCES
Annegarn, J. 2012. Assessment Of Intensity And
Elevation of Arm Movements during Activities of
Daily Life. Daily Activity Monitoring In Patients With
Copd.
Essers, J. M. N., Murgia, A., Bergsma, A., Verstegen, P.
H., Meijer, K. An Inverse Dynamic Analysis on the
Influence of Upper Limb Gravity Compensation
During Reaching. ICORR 2013, 2013 Seattle.
Focal Meditech Bv. 2013. Mcarm: Motion Controlled Arm
Support [Online]. Available: Http://Www.Mcarm.Eu/
The-Project-Aims-And-Goals.Html.
Prange, G. B., Kallenberg, L. A. C., Jannink, M. J. A.,
Stienen, A. H. A., Van Der Kooij, H., Ijzerman, M. J.,
Hermens, H. J. 2009. Influence of Gravity
Compensation on Muscle Activity during Reach And
Retrieval in Healthy Elderly. Journal of
Electromyography And Kinesiology, 19, 40–49.
Van Der Heide, L. A., Van Ninhuis, B. Bergsma, A.
Gelderblom, G.J. Van Der Pijl, D., De Witte, L.P.
2013. An Overview and Categorization of Dynamic
Arm Supports for People With Decreased Arm
Function. Prosthetics & Orthotics International, (In
Press).
