
Comparison of Neural Networks for Prediction of Sleep Apnea
Yashar Maali and Adel Al-Jumaily
University of Technology, Sydney (UTS), Faculty of Engineering and IT, Ultimo, Australia
Keywords: Sleep Apnea, Neural Networks, Prediction.
Abstract: Sleep apnea (SA) is the most important and common component of sleep disorders which has several short
term and long term side effects on health. There are several studies on automated SA detection but not too
much works have been done on SA prediction. This paper discusses the application of artificial neural net-
works (ANNs) to predict sleep apnea. Three types of neural networks were investigated: Elman, cascade-
forward and feed-forward back propagation. We assessed the performance of the models using the Receiver
Operating Characteristic (ROC) curve, particularly the area under the ROC curves (AUC), and statistically
compare the cross validated estimate of the AUC of different models. Based on the obtained results, gener-
ally cascade-forward model results are better with average of AUC around 80%.
1 INTRODUCTION
Sleep Apnea (SA) is one of the most common types
of sleep disorders with around 3% prevalence in
industrialized countries (Young, Palta et al. 1993).
SA is characterized by a repeated and temporary
cessation or reduction of breathing during sleep
(Guilleminault et al., 1978). Clinically, apnea is de-
fined as the total or near-total absence of airflow.
This reduction becomes significant once the decline
of the breathing signal amplitude is at least around
75% with respect to the normal respiration and oc-
curs for a period of 10 seconds or longer. A hypop-
nea is an event of less intensity; it is defined as a
reduction in baseline signal amplitude around 30–
50%, also lasting 10 seconds in adults (Flemons et
al., 1999). Sleep apnea also can be categorized to
three types as; obstructive, central and mixed. The
SA has several short term and long term side effects
(Chokroverty et al., 2009). Short-term effects lead to
impaired attention and concentration, reduce quality
of life, increased rates of absenteeism with reduced
productivity, and increased the possibility of acci-
dents at work, home or on the road. Long-term con-
sequences of sleep deprivation include increased
morbidity and mortality from increasing automobile
accidents, coronary artery disease, heart failure, high
blood pressure, obesity, type 2 diabetes mellitus,
stroke and memory impairment as well as depression.
Long-term consequences, however, remain open
(Chokroverty, 2010).
Unfortunately, as many patients are asymptomat-
ic, sleep apnea may go undiagnosed for years
(Kryger et al., 1996); (Ball et al., 1997). Usually it is
patients’ spouses, roommates, or family members
who report the apnea periods alternating with arous-
als and accompanied by loud snoring (Stradling and
Crosby 1990; Hoffstein 2000). Symptomatic patients
with SA are usually assessed by sleep medicine
Specialists and diagnosed through an overnight sleep
study in a sleep clinic. SA is diagnosed by a manual
analysis of a polysomnographic record, an integrated
device comprising of the EEG, EMG, EOG, ECG,
and oxygen saturation (SPO2) (Penzel et al., 2002).
The polysomnography also contains records of air-
flow through the mouth and nose, along with the
thoracic and abdominal effort signals (Kryger,
1992), and the position of the body during sleep.
The conventional scoring of the polysomnographic
recording is laboured intensive and time-consuming
(Kirby et al., 1999); (Sharma et al., 2004). There-
fore, many efforts have been done to develop sys-
tems that score the records automatically (Cabrero-
(Canosa et al., 2003); (de Chazal et al., 2003);
(Cabrero-Canosa et al., 2004). For this reason sever-
al automated algorithms are used in this area such
as; fuzzy rule-based system (Maali and Al-Jumaily,
2011), genetic SVM (Maali and Al-Jumaily, 2011)
and PSO-SVM (Yashar and Adel, 2012) which have
been proposed in our previous works.
As mentioned, there are several works on appli-
cations of predicting in different areas, but there are
60
Maali Y. and Al-Jumaily A..
Comparison of Neural Networks for Prediction of Sleep Apnea.
DOI: 10.5220/0004701400600064
In Proceedings of the International Congress on Neurotechnology, Electronics and Informatics (NEUROTECHNIX-2013), pages 60-64
ISBN: 978-989-8565-80-8
Copyright
c
2013 SCITEPRESS (Science and Technology Publications, Lda.)

few studies in sleep apnea prediction. One of the
earliest work was published by Dagum and Galper
in 1995 (Dagum and Galper, 1995). This paper
developed a time series prediction by using belief
networks models and then this algorithm used in
sleep apnea. This paper used a multivariate data set
contains 34000 recordings, sampled at 2 Hz, of heart
rate (HR), chest volume (CV), blood oxygen con-
centration (SaO
2
), and sleep state from the time se-
ries competition of the Santa Fe Institute in 1991.
Based on this study, prediction with the CV signal
has more bias than HR and SaO2, because of rapid
and erratic oscillations of the CV series.
Another pioneer work in sleep apnea prediction,
we can can be found in Bock and Gough paper in
1998 . This study use 4.75 hz of heart rate, respira-
tion force, and blood oxygen saturation (SaO
2
) col-
lected from a chronic apnea patient. They use simple
recurrent networks (SRN) proposed by Elman
(Elman, 1991). Each of three time series variables
(heart rate, breathing, and blood oxygenation) were
used as inputs for network training and testing oper-
ations. Each variable was introduced to a unique
network node at the input layer; this network had 18
nodes in the hidden layer. «
One of the newest paper in this area is the work
of Waxaman, Graupe and Carley in 2010 (Waxman
et al., ). They predicted apnea 30 to 120 seconds in
advance. They use Large Memory Storage And Re-
trieval (LAMSTAR) neural network (Graupe and
Kordylewski, 1998). LAMSTAR is a supervised
neural network that can process large amount of data
and also provide detailed information about its deci-
sion making process. Input signals for this algorithm
are EEG, heart rate variability (HRV), nasal pres-
sure, oronasal temperature, submental EMG, and
electrooculography (EOG). It must be noted that
LAMSTAR has this ability to determine most im-
portant input (signal) in predicting process. In pre-
processing phase, data that segmented of 30, 60, 90
and 120 seconds was normalized. They trained sepa-
rate LAMSTAR for each 30, 60, 90 and 120 seconds
segment. Results show that best prediction belongs
to next 30 seconds and they obtained lower perfor-
mance for longer lead time, however, most of pre-
dictions up to 60 seconds in the future is correct.
Also, prediction of non-REM (NREM) events is
better than REM events, generally. For example, for
apnea prediction using 30-second segments and a
30-second lead time during NREM sleep, the sensi-
tivity was 80.6 ± 6 5.6%, the specificity was 72.78 ±
66.6%, the positive predictive values (PPV) was
75.16 ± 3.6%, and the negative predictive values
(NPV) was 79.4 ± 6 3.6%. REM apnea prediction
demonstrated a sensitivity of 69.36 ± 10.5%, a speci-
ficity of 67.46 ± 10.9%, a PPV of 67.4 6 ± 5.6%,
and an NPV of 68.8 ± 6 5.8%. Analyses also showed
that the most important signal for the predicting
apnea into the next second is submental EMG, and
RMS value of the first wavelet level is the most
important feature. But, for the 60 seconds prediction,
nasal pressure is most important signal.
This paper discusses the development of super-
vised artificial neural networks, Elman, cascade-
forward and feed-forward back propagation to pre-
dict sleep apnea. In the rest of this paper, the three
NNs are introduced. Then the issues related to net-
work design and training, especially how to avoid
over fitting, are addressed. The use of AUC as per-
formance measure of the models, and the statistical
comparison of the overall performance of the models
by means of cross-validation, are outlined. The re-
sults and conclusions are presented at the end of the
paper.
2 PRELIMINARIES
2.1 Elman Neural Networks
The Elman neural network is one kind of globally
feed-forward locally recurrent network model pro-
posed by Elman (Li et al., 2009). It occupies a set of
context nodes to store the internal states. Thus, it has
certain dynamic characteristics over static neural
networks, such as the Back-Propagation (BP) neural
network and radial-basis function networks. The
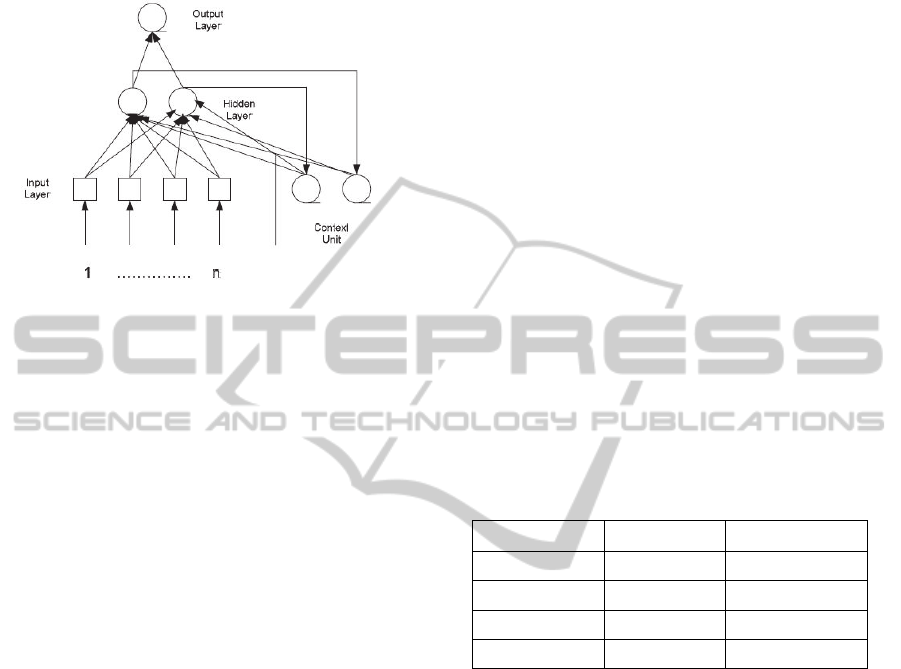
structure of an Elman neural network is illustrated in
Figure 1.
It is easy to observe that the Elman network con-
sists of four layers: input layer, hidden layer, context
layer, and output layer. There are adjustable weights
connecting every two adjacent layers. Generally, the
Elman neural network can be considered as a special
type of feed-forward neural network with additional
memory neurons and local feedback. The distinct
‘local connections’ of context nodes in the Elman
neural network make its output sensitive not only to
the current input data, but also to historical input
data, which is useful in time series prediction. The
training algorithm for the Elman neural network is
similar to the back-propagation learning algorithm, as
both based on the gradient descent principle. Howev-
er, the role that the context weights as well as initial
context node outputs play in the error back-
propagation procedure must be taken into considera-
tion in the derivation of this learning algorithm. Due
to its dynamical properties, the Elman neural network
ComparisonofNeuralNetworksforPredictionofSleepApnea
61
has found numerous applications in such areas as
time series prediction, system identification and
adaptive control (Gao and Ovaska, 2002).
Figure 1: Structure of an Elman neural network model.
2.2 Cascade-forward Neural Network
Models
Cascade-forward models are similar to feed-forward
networks, but include a weight connection from the
input to each layer and from each layer to the suc-
cessive layers. While two-layer feed-forward net-
works can potentially learn virtually any input-
output relationship, feed-forward networks with
more layers might learn complex relationships more
quickly. For example, a three layer network has
connections from layer 1 to layer 2, layer 2 to layer
3, and layer 1 to layer 3. The three-layer network
also has connections from the input to all three lay-
ers. The additional connections might improve the
speed at which the network learns the desired rela-
tionship. Cascade-forward artificial intelligence
model is similar to feed-forward back propagation
neural network in using the back propagation algo-
rithm for weights updating, but the main symptom of
this network is that each layer of neurons related to
all previous layer of neurons. This network is a
Feed-Forward network with more than one hidden
layer. Multiple layers of neurons with nonlinear
transfer functions allow the network to learn more
complex nonlinear relationships between input and
output vectors (Abdennour, 2006).
3 PROPOSED APPROACH
In this paper three input signals as; airflow, ab-
dominal and thoracic movement signals are used as
had been found in our previous work as the most
important signals for SA studies (Maali and Al-
Jumaily, 2012). In the present work data collected
from 5 patients which events of them are annotated
by an expert were collected in the concord hospital
in Sydney. We extracted data segments of 30, 60,
90, and 120 seconds. Also, Different lead times as
30, 60, 90 and 120 seconds are investigated in this
paper. Also, AUC is considered as performance
measure in this paper.
3.1 Feature Generation
Each signal from each segment was normalized by
dividing by its mean value. A discrete wavelet trans-
form was then applied. For each windows a variety
of features were extracted from the nasal airflow,
abdominal and thoracic movement signals. Features
are generated from coefficients of wavelet packet
and the original signals. Daubechies wavelet packet
of order 4 and 7 levels is used and different statisti-
cal measures are generated from the coefficients and
original signal. These features represent the inputs of
the NNs algorithm. Full list of proposed features are
included in the Table 1.
Table 1: List of statistical features, x is coefficients of the
wavelet.
logmeanx^2 kurtosisx^2 geomeanabsx
stdx^2 varx^2 madx
skewnessx^2 meanabsx meanx^2
skewnessx kurtosisx varx
geomeanx^2 madx^2 stdx
More details about these statistical measures are presented in
the Appendix
3.2 Early Stopping
Usually standard neural network architectures such
as the fully connected multi-layer perceptron almost
always are prone to overfitting. While the network
seems to get better and better (the error on the train-
ing set decreases), at some point during training it
actually begins to get worse again, (the error on
unseen examples increases).
There are basically two ways to fight overfitting:
reducing the number of dimensions of the parameter
space or reducing the effective size of each dimen-
sion. The corresponding NN techniques for reducing
the size of each parameter dimension are regulariza-
tion such as weight decay or early stopping
(Prechelt, 1998). Early stopping is widely used be-
cause it is simple to understand and implement and
has been reported to be superior to regularization
methods in many cases. This method can be used
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
62

either interactively, i.e. based on human judgment,
or automatically, i.e. based on some formal stopping
criterion. In this paper automatic stopping criteria is
used based on the increases of validation error.
4 RESULTS
The results for prediction of apnea in the immediate-
ly following segment as the segment duration are
varied between 30, 60, 90 and 120 seconds are com-
putes for each of three NNs. For each experiments10
validation is performed and average and standard
deviation of these results are shown in table 2, 3 and
4. ANOVA test on these data shows that the average
of AUC of these segmentations are significantly
different and performing pair t-test shows that per-
formances are generally better for 30-seconds seg-
ment, and as the segment duration is increased, the
performance is decreased. Also, increase of the lead
time results in increasing of the performances.
Table 2: AUC of apnea prediction by Cascade-forward
model.
Lead Time
30 60 90 120
30
71.05 2.42 75.29 3.79 78.15 5.75 82.22 3.93
60
67.71 1.93 72.55 7.29 77.68 5.92 79.66 5.79
90
66.29 4.43 71.85 8.17 80.47 4.54 81.05 4.97
120
63.40 1.54 73.44 6.26 78.19 7.72 77.52 7.18
Table 3: AUC of apnea prediction by feed-forward model.
Lead Time
30 60 90 120
30
68.12 2.43 74.88 5.77 73.61 5.76 82.31 7.19
60
65.56 2.72 72.90 7.48 71.71 6.23 80.45 6.50
90
65.95 4.43 69.31 5.20 73.08 8.67 72.90 7.53
120
61.12 1.47 67.12 7.83 76.39 8.38 79.72 6.52
Table 4: AUC of apnea prediction by Elman model.
Lead Time
30 60 90 120
30
69.32 2.24 74.88 5.77 73.61 5.76 78.31 7.19
60
67.59 2.53 77.64 7.34 78.49 4.81 79.16 6.43
90
64.87 1.68 77.02 5.90 77.62 6.85 79.99 5.94
120
65.57 2.28 72.88 7.14 76.46 8.31 79.83 5.19
Also, ANOVA test shows that performance of
these models are not same, and in general cascade
model results in better prediction, but not for all of
the experiments, this shows that each model can
predict some type of samples better than other mod-
els. Therefore using ensemble of neural networks
maybe helpful and should be considered (Li et al.,
2009).
5 CONCLUSIONS
In this study, we present the first step of an ongoing
investigation into the prediction of individual events
of sleep apnea with different artificial neural net-
works. Experimental results of Elman, cascade-
forward and feed-forward back propagation neural
networks shows that, generally cascade-forward NN
can predict the sleep apnea events better, but this
advantage is not for all samples and investigation on
ensemble of these NNs is subject to future works.
Also, this study shows that increasing the lead time
can improve the performances, in the most cases.
REFERENCES
Abdennour, A. (2006). "Evaluation of neural network
architectures for MPEG-4 video traffic prediction."
Ieee Transactions on Broadcasting 52(2): 184-192.
Ball, E. M., R. D. Simon, et al. (1997). "Diagnosis and
treatment of sleep apnea within the community - The
Walla Walla project." Archives of Internal Medicine
157(4): 419-424.
Bock, J. and D. A. Gough (1998). "Toward prediction of
physiological state signals in sleep apnea." Ieee Trans-
actions on Biomedical Engineering 45(11): 1332-
1341.
Cabrero-Canosa, M., M. Castro-Pereiro, et al. (2003). "An
intelligent system for the detection and interpretation
of sleep apneas." Expert Systems with Applications
24(4): 335-349.
Cabrero-Canosa, M., E. Hernandez-Pereira, et al. (2004).
"Intelligent diagnosis of sleep apnea syndrome." Ieee
Engineering in Medicine and Biology Magazine 23(2):
72-81.
Chokroverty, S. (2010). "Overview of sleep & sleep disor-
ders." Indian Journal of Medical Research 131(2):
126-140.
Chokroverty, S., C. Sudhansu, et al. (2009). Sleep depriva-
tion and sleepiness. Sleep Disorders Medicine (Third
Edition). Philadelphia, W.B. Saunders: 22-28.
Dagum, P. and A. Galper (1995). "Time-series prediction
using belief network models." International Journal of
Human-Computer Studies 42(6): 617-632.
de Chazal, P., C. Heneghan, et al. (2003). "Automated
processing of the single-lead electrocardiogram for the
detection of obstructive sleep apnoea." Ieee Transac-
tions on Biomedical Engineering 50(6): 686-696.
Elman, J. L. (1991). "Distribute representations, simple
ComparisonofNeuralNetworksforPredictionofSleepApnea
63

recurrent networks, and gramimatical structure." Ma-
chine Learning 7(2-3): 195-225.
Flemons, W. W., D. Buysse, et al. (1999). "Sleep-related
breathing disorders in adults: Recommendations for
syndrome definition and measurement techniques in
clinical research." Sleep 22(5): 667-689.
Gao, X. Z. and S. J. Ovaska (2002). "Genetic Algorithm
training of Elman neural network in motor fault detec-
tion." Neural Computing & Applications 11(1): 37-44.
Graupe, D. and H. Kordylewski (1998). "A large memory
storage and retrieval neural network for adaptive re-
trieval and diagnosis." International Journal of Soft-
ware Engineering and Knowledge Engineering 8(1):
115-138.
Guilleminault, C., J. van den Hoed, et al. (1978). "Over-
view of the sleep apnea syndromes. In: C. Guillemi-
nault and Wc Dement, Editors, Sleep apnea syn-
dromes, Alan R Liss, New York." 1-12.
Hoffstein, V. (2000). Snoring. Principles and practice of
sleep medicine. M. H. Kryger, T. Roth and D. W. C.
Philadelphia, PA: W.B., Saunders: 813-826.
Kirby, S. D., W. Danter, et al. (1999). "Neural network
prediction of obstructive sleep apnea from clinical cri-
teria." Chest 116(2): 409-415.
Kryger, M. H. (1992). "management of obstractive sleep-
apnea." Clinics in Chest Medicine 13(3): 481-492.
Kryger, M. H., L. Roos, et al. (1996). "Utilization of
health care services in patients with severe obstructive
sleep apnea." Sleep 19(9): S111-S116.
Li, Y., D. F. Wang, et al. (2009). A Dynamic Selective
Neural Network Ensemble Method for Fault Diagnosis
of Steam Turbine.
Maali, Y. and A. Al-Jumaily (2011). Automated detecting
sleep apnea syndrome: A novel system based on ge-
netic SVM. Hybrid Intelligent Systems (HIS), 2011
11th International Conference on.
Maali, Y. and A. Al-Jumaily (2011). "Genetic Fuzzy Ap-
proach for detecting Sleep Apnea/Hypopnea Syn-
drome." 2011 3rd International Conference on Ma-
chine Learning and Computing (ICMLC 2011).
Maali, Y. and A. Al-Jumaily (2012). Signal selection for
sleep apnea classification. Proceedings of the 25th
Australasian joint conference on Advances in Artifi-
cial Intelligence. Sydney, Australia, Springer-Verlag:
661-671.
Penzel, T., J. McNames, et al. (2002). "Systematic com-
parison of different algorithms for apnoea detection
based on electrocardiogram recordings." Medical &
Biological Engineering & Computing 40(4): 402-407.
Prechelt, L. (1998). "Automatic early stopping using cross
validation: quantifying the criteria." Neural Networks
11(4): 761-767.
Sharma, S. K., S. Kurian, et al. (2004). "A stepped ap-
proach for prediction of obstructive sleep apnea in
overtly asymptomatic obese subjects: a hospital based
study." Sleep Medicine 5(4): 351-357.
Stradling, J. R. and J. H. Crosby (1990). "Relation be-
tween systemic hypertension and sleep hypoxemia or
snoring- analysis in 748 men drawn from general-
practice." British Medical Journal 300(6717): 75-78.
Waxman, J. A., D. Graupe, et al. "Automated Prediction
of Apnea and Hypopnea, Using a LAMSTAR Artifi-
cial Neural Network." American Journal of Respirato-
ry and Critical Care Medicine 181(7): 727-733.
Yashar, M. and A.-J. Adel (2012). A Novel Partially Con-
nected Cooperative Parallel PSO-SVM Algorithm
Study Based on Sleep Apnea Detection. Accepted in
IEEE Congress on Evolutionary Computation. Bris-
bane, Australia.
Young, T., M. Palta, et al. (1993). "the occurrence of
sleep-disordered breathing among middle-aged
adults." New England Journal of Medicine 328(17):
1230-1235.
APPENDIX
Mean, variance (VAR) and standard deviation
(STD) are common and well known statistical tools,
so other statistical features, in this study, are re-
viewed here.
Kurtosis: The kurtosis of a distribution is a measure
of how outlier-prone a distribution is, and defined as
follow
^4/^4
Geomean: Geomean is the geometric mean and com-
puted as follow:
∏^1 ⁄
Skewness: Skewness is a measure of the asymmetry
of the data around the sample mean, and defined as
follow
^3/^3
Mad: mad is mean absolute deviation of the sample
as, | |.
NEUROTECHNIX2013-InternationalCongressonNeurotechnology,ElectronicsandInformatics
64
