
Cost-effective Design of Real-time Home Healthcare Telemonitoring
Po-Chou Liang and Paul Krause
Department of Computing, University of Surrey, Guildford, U.K.
Keywords: Cost-effectiveness, Healthcare, Telemonitoring, Vital Sign Monitoring, Fall Detection, Movement Pattern
Monitoring, Smart Home, Internet of Things, Mobile Cloud Computing.
Abstract: The importance of telehealthcare for elderly and out-patients has been widely recognized. However, the
adoption rate of home healthcare telemonitoring remains low due to limited evidence for cost-effectiveness.
Our core objective of this work is the cost-effective design of a real-time home healthcare telemonitoring
system based on mobile cloud computing. A second objective is to develop a simulation environment for
evaluating the cost-effectiveness of a telemonitoring system and exploring technology choices. We are at an
early stage, yet the results so far have been encouraging. Whilst we may not be able to deliver a complete
solution, the methodological contribution of test environment plus simulation models will enable us to put
the evaluation of telehealth solutions prior to moving to full-scale trials on a more scientific basis.
1 INTRODUCTION
The rise in both ageing and chronic disease
populations has become a global issue which calls
for a top policy priority to provide proper access to
quality healthcare. Though information and
communications technologies (ICTs) have been used
in almost all aspects of our life, there remains a
considerable question of low adoption rate of remote
healthcare technologies. One of the main reasons, as
indicated by a number of studies (McLean, Prott and
Sheikh, 2011; Limburg et al., 2011), is a lack of
robust evidence for cost-effectiveness.
To address this issue, we set up as our core
objective the cost-effective design of a real-time
home healthcare telemonitoring system based on
mobile cloud computing. Our hypothesis is that the
increasing availability of commodity sensor
technology and computation resource can
dramatically reduce the infrastructure costs of
telemonitoring. In addition, the usability of the
technology is making significant advances -
especially in terms of minimising intrusion on the
patients’ lifestyle (Liang and Krause, 2013).
Our second objective is to develop a simulation
environment in order for us to produce robust
evidence for the cost-effectiveness of a
telemonitoring system so as to explore technology
choices prior to moving to full-scale trials.
Accordingly, a framework based on data from
simulated trials and literature review for conducting
comparative cost-effectiveness analysis is also
proposed. Here, home healthcare telemonitoring is
defined as “the use of ICTs to monitor the vital signs
and activities of in-home patients or elderly
remotely.”
The remainder of this paper is organised as
follows.
In Section 2, we briefly introduce the
development trends in several related areas, such as
telehealthcare, Smart Home and mobile cloud
computing based on literature review. In Section 3,
we present our design and experimental work for the
proposed system. Finally, Section 4 provides our
concluding remarks and future work.
2 LITERATURE REVIEW
AND RELATED WORK
To better understand the development of remote
healthcare, as well as the implications of recent ICT
advances, such as sensor technologies, smart home,
and mobile cloud computing, we have conducted a
broad review of literature in related fields.
2.1 Telehealthcare
The concept of telehealthcare (i.e. the use of ICTs to
provide healthcare remotely) has been explored for
more than thirty years, as evidenced by the
5
Liang P. and Krause P..
Cost-effective Design of Real-time Home Healthcare Telemonitoring.
DOI: 10.5220/0004723800050015
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 5-15
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

emergence of nurse call centres in the 1970s in the
UK. As mentioned in Section 1, in recent years, the
problem of ageing and increasing number of people
with chronic diseases have further underpinned the
importance of telehealthcare. Therefore, a great
number of studies on remote home care have
emerged. However, the problem of lacking robust
evidence for cost-effectiveness of related solutions
remains.
A review (Koch, 2006) of the existing scientific
literature on home telehealth during 1990-2003
classified 578 articles from the Medline database as
being relevant to the targeted research field of home
telehealth. Two of the conclusions drawn by this
review were that the impact on those designs for
special user groups, such as elderly, needs to be
further explored, and that in general, evaluation
studies are rare and further research is critical to
determine the impacts, benefits and limitations of
potential solutions.
Another systematic review (Barlow et al., 2007)
identified summaries of 8,666 studies available as of
January 2006 in 17 electronic databases, for
example, the Medline and WTO library. Of those
studies, 98 randomised trials and observational
studies were included in the review. The key
findings included that most studies focused on
people with diabetes (31%) and heart failure (29%),
and that cost-effectiveness of these interventions
was less certain. In addition, there was insufficient
evidence of the effects of home safety and security
alert systems.
Then a systematic review of economic
evaluations (Bergmo, 2010) found only 33 articles
that measured both costs and non-resource
consequences of using telemedicine in direct patient
care. However, the review regarded this as a
considerable increase. It concluded that the
effectiveness measures were more consistent and
well reported than the costings, and that most studies
lacked information about perspective and costing
method.
2.1.1 Cost-effectiveness Analysis
The increasing demand for better healthcare is
manifested in the need to provide better evidence for
informed decision making through economic
evaluation. In this context, Evidence-based Medicine
(EBM), Health Technology Assessment (HTA) and
Comparative Effectiveness Research (CER) have
been used respectively in many organisations to
evaluate the benefits and harms of alternative
treatments, technologies or healthcare deliveries.
Among all techniques of economic evaluations in
healthcare, Cost-effectiveness Analysis (CEA) is
widely adopted.
The National Institute for Health and Clinical
Excellence (NICE) in the UK (2013) defines cost
effectiveness analysis as: “an economic study design
in which consequences of different interventions are
measured using a single outcome, usually in
‘natural’ unit (for example, life-years gained, deaths
avoided, heart attacks avoided or cases detected).
Alternative interventions are then compared in terms
of cost per unit of effectiveness.”
To conduct cost effectiveness analysis, Phillips
(2009) and Muenning (2008) suggested that three
types of costs need to be considered:
Direct costs: such as drugs, staff time, equipment,
transport of patients;
Indirect (or Productivity) costs: production losses,
other uses of time; and
Intangibles: pain, suffering, adverse effects.
The effects of an intervention generally refer to the
changes in patients’ health status. Since there is no
direct way to measure health status, a cost-
effectiveness analysis instead examines patients’
quantity and quality of life with a given health status
(Muenning, 2008). Figure 1 represents the concept
that there are changes in the health status, associated
costs and resulting quality of life and life expectancy
of an observed group of patients having received an
intervention for a period of time
Figure 1: Components of a Cost-effectiveness Analysis,
after (Muenning, 2008).
For independent interventions, the cost-effectiveness
ratio (CER) is calculated to estimate the effects of
different interventions by dividing the costs (C) of
each intervention by its health effects (E) produced,
e.g. life-years gained (LYG) or quality adjusted life
years (QALYs):
CER = C / E (1)
For mutually exclusive interventions, the
incremental cost-effectiveness ratio (ICER) is
calculated by dividing the difference in costs (C)
by the difference in health effects (E) between two
interventions:
ICER =
C / E
(2)
HEALTHINF2014-InternationalConferenceonHealthInformatics
6

2.1.2 The Whole System Demonstrator
(WSD) Cluster Randomised Trial
In order to better evaluate telecare and telehealth
technologies and their implications for elderly and
people in independent living, the Department of
Health in England (2011) launched the Whole
System Demonstrator (WSD) programme in May
2008. Three sites, Kent, Cornwall and Newham,
were selected to be part of a cluster randomised
controlled trial. With 238 General Practitioners
(GPs) and 6,191 patients with diabetes, chronic
obstructive pulmonary disease (COPD), and
coronary heart disease (CHD), it was believed that
this trial is the world’s largest randomised controlled
trial of telecare and telehealth.
Under this trial, each intervention participant was
given a home unit together with a pendant alarm and
up to 27 peripheral devices for functional monitoring
(such as the home unit and bed and chair occupancy
sensors), security monitoring (such as infrared
movement sensors and property exit sensors) and
standalone devices (not connected to a monitoring
centre, such as big button phones) (Steventon et al.,
2013).
With regard to the key findings of this trial, the
Department of Health in England (2011) announced
that if used correctly telehealth can deliver a 15%
reduction in Accident and Emergency (A&E) visits,
a 20% reduction in emergency admissions, a 14%
reduction in elective admissions, a 14% reduction in
bed days, and a 45% reduction in mortality rates.
However, several in-depth studies on the effect and
cost-effectiveness of this trial reached some
unfavourable conclusions, as in the following:
Steventon et al., (2012) concluded that, though
both hospital admissions and mortality for
intervention patients were lower, there were no
significant differences between the intervention
group and the control group both in the number
of elective admissions, outpatient attendance,
and emergency visits and in notional hospital
costs to commissioners of care.
Henderson et al., (2013) found that the QALY
gained by patients using telehealth in addition to
usual care was similar to that by patients
receiving usual care only, and that total costs in
relation to telehealth were also higher. As such,
this study concluded that telehealth does not
seem to be a cost effective addition to standard
support and treatment.
Steventon et al., (2013) concluded that telecare
did not significantly reduce the use of health and
social care services.
Another study (Sanders et al., 2012) identified that
concerns about both competency to operate
equipment and threats to identity, independence and
self-care (which might be undermined, among
others, by not getting outside, but doing monitoring
indoors even on holidays) are two of the main
barriers to adoption of telehealth and telecare
interventions within this trial.
Based on the abovementioned findings, we
consider that the WSD trial could serve as an
important reference for conducting cost comparison,
selecting inexpensive technologies, devising proper
service models and designing workable system
architecture for the proposed home healthcare
telemonitoring system.
2.2 Smart Home and Internet
of Things
The concept of the so-called “smart home” or
“digital home” has been proposed for more than a
decade, aiming to transform our home environment
into an intelligence-embedded living space. This
paper uses these two terms alternately. According to
Elderly Accommodation Counsel (2003), the UK’s
Department of Trade and Industry’s “Smart Homes
Project” defined smart home as “A dwelling
incorporating a communications network that
connects the key electrical appliances and services,
and allows them to be remotely controlled,
monitored or accessed.”
There were several industrial initiatives for smart
home driven mainly by manufacturers and network
providers. For instance, the Open Service Gateway
Initiative (OSGi) Alliance founded in 1999 focuses
on open specifications for remote management and
the delivery of services into the home. At almost the
same time, the Konnex Association was formed in
1999 to promote an open standard, called KNX, for
home and building control. Other similar effort
included the establishment of Universal Plug & Play
(UPnP) Forum in 1999 and the Digital Living
Network Alliance (DLNA, originally named
“Digital Home Working Group”) in 2003.
Since their inception, these industrial initiatives
have gradually expanded and gained wider support
across different industrial sectors and players. For
example, today PS2, XBOX 360 and personal
computers with MS Windows 7 installed all support
DLNA standards, and both OSGi and DLNA
specifications support UPnP standards. However, on
the service side, the market has only developed to a
very limited extent.
With regard to smart home monitoring systems,
Cost-effectiveDesignofReal-timeHomeHealthcareTelemonitoring
7
Gaddam, Mukhopadhyay and Sen Gupta (2011)
stated that when more sensors are added to a smart
home system, the system becomes complicated to
handle and the maintenance becomes a challenge. In
our opinion, this is also quite true to home
healthcare telemonitoring, as remote home
healthcare is generally considered as a subcategory
of smart home (Wu et al., 2009).
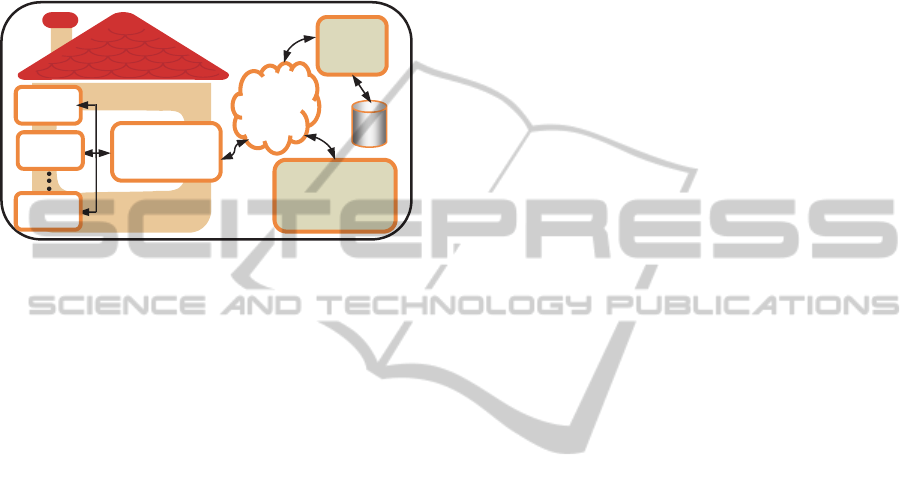
Figure 2: The Concept Diagram of a Typical Smart Home
System.
Generally, a home gateway or a control hub (see
Figure 2) interconnects one or more home networks
and the Internet/access network (sometimes a cable
modem or router is also needed), and controls other
in-home devices and sensors (den Hartog, et al. 2004;
Wei et al., 2010). For a commercialised smart home
service package, the central server, i.e. one or a
group of computers, is usually located at the service
provider’s premise. However, in other cases it is
common to see that the proposed system
architectures require one or multiple servers (or
called controllers) to be set up within the smart
home environment, one for each platform that is
being used by a controlled device (Zimmermann1
and Vanderheiden, 2007). From our viewpoint, this
kind of design would increase the complexity of
system installation and maintenance.
One important evolution of recent ICTs, which
has great implications for the development of smart
home, as well as home healthcare telemonitoring, is
the emergence of the Internet of Things (or IOTs).
The International Telecommunication Union (ITU)
(2005) described the IOTs as a new form of
communication between people and things, and
between things themselves, which “connects the
world’s objects in both a sensory and an intelligent
manner.”
The basic architecture of the IOTs consists of
three layers: application layer, network layer and
sensor layer (Kang et al., 2011), which in our
opinion can be naturally fitted into the concept
framework of a smart home system as depicted
previously in Figure 2.
According to the Cluster of European Research
Projects on the Internet of Things (CERP-IoT), a
large number of application domains in the field of
IoTs have been identified (Sundmaeker et al., 2010).
We believe that among others, Intelligent Buildings,
Healthcare (monitoring of parameters, positioning,
real time location systems), Independent Living
(wellness, mobility), and Environment Monitoring,
are all applicable to supporting our envisioned smart
home, as well as home healthcare telemonitoring.
A 2011 study (McCullagh and Augusto, 2011)
investigating the potential of IoTs to monitor health
and wellness concluded that the underlying
technology is available but needs to be turned into a
solution which can become pervasive in society.
This is the gap that this research intends to fill by
using low-cost, off-the-shelf technologies to build up
evidence for a solid solution.
2.3 Sensor Technologies
As mentioned in Section 2.1, sensors form an
indispensable component of a smart home system, as
well as a healthcare telemonitoring system. In
general, a sensor is capable of detecting three but
intrinsically related categories of events (Faludi,
2010):
Direct or proximal phenomena: events that
directly trigger the sensor device;
Indirect or distal phenomena: remote causes of
the local events actually triggering the sensor;
and
Context and subtext: the situation surrounding an
event.
However, contextual information inferred from both
direct and indirect phenomena might still involve
some degree of uncertainty. This demonstrates the
importance of a well-designed event reasoning
algorithm that can increase the accuracy of context
inference based on a limited set of monitored data.
Today there are a great variety of electronic
sensors available in the marketplace. In the field of
telehealthcare, there are also increasing focuses on
the development of the so-called Body Sensor
Networks (BSNs) for on-body applications. For the
purpose of our cost-effective design of home
healthcare telemonitoring, this research pays special
attention to existing inexpensive, portable and easy-
to-use sensor technologies/platforms.
2.3.1 ZigBee
ZigBee is a standards-based low-power wireless
Home Gateway
/Control Hub
Device 1
Internet
Central
Server
Remote Control
Panel/Context
Status Checking
Device 2
Device n
HEALTHINF2014-InternationalConferenceonHealthInformatics
8

technology mainly operating in the 2.4GHz radio
frequency band. It is based on the IEEE 802.15.4
standard with add-on network and security layers
and an application framework. The ZigBee Alliance
was established in 2002 to develop relevant
specifications and to promote ZigBee standards
adoption. Today, the ZigBee Alliance has over six-
hundred certified products, ranging from home
appliances, energy efficiency apparatuses,
networking devices, to health and fitness sensors.
ZigBee Health Care was introduced to provide an
industry-wide standard for exchanging data between
a variety of medical and non-medical devices
(ZigBee Alliance, 2009).
Based on different topologies, such as pair, star
and mesh, a ZigBee sensor network consists of one
coordinator node and at least one router or one end-
device node (Faludi, 2010). In a ZigBee network,
each node can communicate with all the others by
way of its nearest neighbour so that only small
amount of power is needed for radio transmission.
In addition, with the embedded capability to perform
self-healing, a ZigBee mesh network can reconfigure
itself and route around a problem area when some
nodes are failed or removed. Other important
features of Zigbee 2012 specifications (ZigBee
Alliance, 2012) include data security based on
Advanced Encryption Standard (AES), low-power
consumption for better battery life, and low cost in
comparison with other wireless technologies.
At the time of this writing, there are only a few
kinds of sensors available in the health and fitness
sub-category. Besides, ZigBee’s limited
programming capacity to perform software
logic/data processing suggests that all raw data
needs to be dealt with by other layers in a smart
home or IoT system. This would result in a greater
amount of data traffic and lower data reliability.
2.3.2 Arduino
Arduino is an open-source microcontroller platform
for physical computing. It was originally designed in
2005 to provide students with an inexpensive
microcontroller to drive their robotic projects. To
date, it has evolved into a popular tool kit for
prototyping and do-it-yourself work.
By attaching different combinations of various
sensors and actuators to a programmable
microcontroller board, many different tasks, such as
environmental (e.g. temperature and humidity)
monitoring and home automation (e.g. door/window
opening), can be performed in a way that is based on
the user-uploaded software programme. There are
also a number of different communications modules,
such as serial port (e.g. USB), Wi-Fi, Bluetooth, and
web server, available for use to transmit the
programmed outputs, such as the status of the board
and/or the monitored data, to other devices or a web
client.
According to Arduino website (2013), the main
advantages offered by Arduino include: low-cost as
compared with other microcontroller platforms,
cross-platform (among MS Windows, OS X, and
Linux), simple programming environment, and open
source with extensible software and hardware. From
our point of view, the capabilities both to conduct
on-board data processing by the microcontroller to
provide more reliable and meaningful monitored
data, and to interconnect and interoperate with a
variety of devices, such as smartphone and ZigBee,
are two other important features that enable Arduino
to provide more flexible sensory solutions.
2.4 Mobile Cloud Computing
and Home Healthcare
Along with the recent prevalence of smart mobile
devices in our daily life, hundreds of thousands of
available mobile applications, or the so-called
“Apps” are targeting a great diversity of consumer
segments. According to Sarasohn-Kahn (2010), “as
of February 2010, there were 5,805 health, medical,
and fitness applications in the Apple AppStore. Of
these, 73% were intended for use by consumer or
patient end-users, while 27% were targeted to health
care professionals.” There were also Apps using
available sensors, including accelerometers, infrared
photo-detectors and glucometers, for home
measuring. These figures and developments
represent both challenges and opportunities to this
research.
Meanwhile, both mobile computing and mobile
cloud computing have recently gained increasing
attention from ICT researchers and developers.
According to Huang (2011), mobile computing
research refers to the study on how mobile devices
learn their own status and surrounding contexts to
better support mobile applications.
Regarding mobile cloud computing, there are
two different viewpoints (Qureshi et al., 2011). One
refers mobile cloud computing as making use of
cloud resources, such as computing power and
storage, to help perform tasks or store data from
mobile devices, which generally have limited
computing capacity and data storage. The other
recommends that with mobile cloud computing, both
data processing and storing be done by the mobile
Cost-effectiveDesignofReal-timeHomeHealthcareTelemonitoring
9

device. For the purpose of this research, we take
both views to give a broader definition of mobile
cloud computing. With this, it is apparent that by
adopting mobile cloud computing, an application
can be further empowered by mobility together with
the main advantages, such as on-demand self-
service, resource pooling, rapid elasticity, and pay-
per-use, derived from cloud computing.
Some sophisticated system architectures have
been proposed so that several mobile devices can
work together to perform a particular task or each
device can provide its remaining resources for other
devices. For example, Hyrax (Marinelli, 2009), a
mobile cloud computing platform, was proposed
based on Hadoop to provide data sharing and
distributed data processing among a group of
networked mobile phones. In its implementation,
Hyrax used two conventional computers to perform
Hadoop-related NameNode and JobTracker
processes and cluster initialisation. Clearly, such
complex system architecture would not fit into our
requirements.
Cheng and Zhuang (2010) proposed a Bluetooth-
enabled, in-home patient monitoring system for
early detection of Alzheimer’s disease. The
proposed system required every room in the house to
be equipped with a Bluetooth access point (AP), and
all APs needed to be connected to a local database
(i.e. a laptop). A Bluetooth-enabled pocket PC was
carried by the target person in the house and tried to
find an AP with strongest signal to which to connect.
If the target entered another room, the pocket PC
would try to connect to another AP. By such an
approach, the movement pattern of the target could
be identified and stored in the local database. The
data could then be transmitted to a remote medical
practitioner for diagnosis, or be analysed by an
assumed decision engine to see if the target had any
early signs of Alzheimer’s disease. From our
perspective, this proposal was not very practical, as
both the physical locations of each AP and the
layout of the house would seriously affect the
detectable Bluetooth signal strength and in some
cases would even cause failures in establishing
Bluetooth connection. Accordingly, the deployment
of Bluetooth APs could be very complex.
MoCAsH (Hoang and Chen, 2010) was a
proposed mobile cloud for assistive Healthcare. Its
system architecture included (i) sensors and mobile
agents, (ii) a context-aware middleware, (iii) a
collaborative cloud, and (ix) a cloud portal. The
cloud portal allowed authorized users to access
offered services, including checking sensor status,
updating context-aware rules, and accessing back-
end cloud platform management centre. It also
proposed a P2P federated cloud model to schedule
distributed clouds and their resources, and to
enhance data security. In our view, this project could
have served as a good reference for our prototyping
and design. However, it put its main focus on how to
integrate mobile devices into a federated cloud
architecture without addressing how to implement
non-built-in sensors’ deployment and patient
monitoring.
Wang et al. (2008), as well as Yang and Zhao
(2011), proposed to place a tri-axial accelerometer at
the head level with a pre-defined position and angle
to detect human falls. In our opinion, this kind of
physical setting is not only impractical in home
patient/elderly monitoring, but also intrusive to the
monitored people. Viet, Lee and Choi (2012) used
an Android smart phone which has a built-in
accelerometer and an orientation sensor to perform
human fall detection. It was concluded that the
proposed system reached 85% accuracy in 260 trials.
However, since the implementation was based on a
standalone mobile phone, the proposed system did
not possess any remote monitoring capability.
3 RESEARCH DESIGN
AND CURRENT WORK
3.1 Requirements and Considerations
Based on the preceding technology reviews we have
identified the following set of requirements for a
cost effective telemonitoring system.
3.1.1 Functional Requirements
Vital sign monitoring: This refers to the on-
demand monitoring of patients’ vital sign
parameters, such as body temperature, heartbeat
rate, oxygen in blood, blood pressure, blood
glucose, cardiogram, and sweat level.
Safety monitoring: The main function will be
real-time human fall detection with alerts being
sent automatically to designated caregivers
and/or healthcare professionals via a healthcare
dashboard, SMS and video phone.
Emergency call-for-help tool kits: This refers to
the provision of a portable alarm; once pressed
by a patient, it would send out an alert to
designated caregivers and healthcare
professionals via the healthcare dashboard with
configurable, automated SMS and video phone
call out and call in functions.
HEALTHINF2014-InternationalConferenceonHealthInformatics
10
Activity monitoring: This includes movement
pattern monitoring, bed and chair occupancy
sensing and property exit sensing for social care
purposes.
Service portal/management console and
healthcare dashboard: The service
portal/management console allows authenticated
in-home patients, as well as remote caregivers
and healthcare professionals to control and
manage the sensors. It also allows them to set
their preferences and care plans for healthcare
monitoring, as well as to manage and access
context/health data via a healthcare dashboard.
Authenticated database management and access:
This refers to a database system that provides
authenticated users with remote management and
access to the large volume of monitored data.
3.1.2 Basic Considerations
The following considerations with criteria for
evaluation need to be addressed throughout the
whole system development life cycle to ensure that
the research objective can be successfully fulfilled.
Low-cost: There should be no significant amount
of capital expenditures (Capex) and operational
expenditures (Opex) on system setup and
operations.
Easy-to-deploy-and-use: In general, the end-
users, especially those living independently,
should be able to set up and operate the system.
Less intrusive: Generally, the monitoring should
not hinder patients’ normal daily routine and
mobility.
Robust enough: The system should embrace
fault-tolerant and resilient design to maximise
service availability. When the Internet is not
available or the cloud side is unreachable, the
application on the mobile device as well as the
monitoring task should be able to continuously
function properly.
Security and data privacy: The system should
employ proper access control, user
authentication, data encryption, and secured data
transmission to enhance data privacy and
security.
No vendor lock-in: The system design should
avoid or at least minimise the impact of vendor
lock-in issue by taking the portability of each
monitored patient’s data into account.
Good performance and elasticity: The system
performance and elasticity need to be well
managed to provide streamlined user experience
and service provision.
3.2 System Design
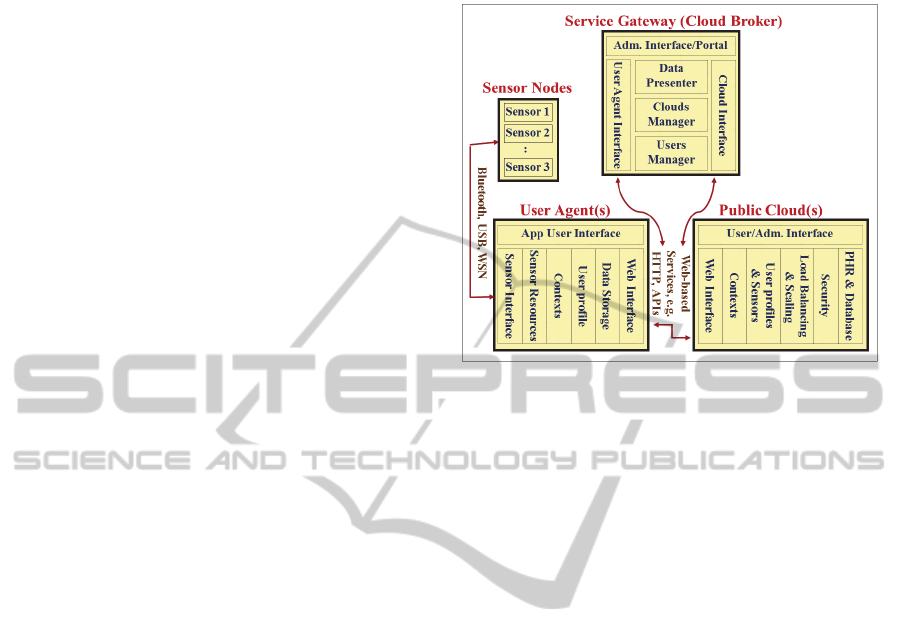
Figure 3: High-level System Architecture.
As shown in Figure 3, the proposed system
architecture for the home healthcare telemonitoring
system consists of four main modules, i.e. Sensor
Nodes, User Agent(s), Service Gateway (Cloud
Broker) and Public Cloud(s). The main functionality
of each module is illustrated below:
The User Agent(s) Module: Its main functions
include: (i) a user interface for users to control
and manage the sensors, to set their preferences
and care plans for healthcare monitoring and to
manage context and health data; (ii) an
intelligent data aggregator that connects with a
variety of sensors, collects real-time sensor data
through high-level sensor APIs and transmits it
to cloud storage, and performs context/health
data reasoning based on preset parameters and
algorithms to automatically trigger an alert; and
(iii) a portable personal healthcare assistant that
can work with, and without an Internet
connection (Liang and Krause, 2013). Figure 4
illustrates the architecture diagram of this
Module.
The Service Gateway Module: Its essential
functions include: (i) a management console both
for performing administrative tasks and for
providing caregivers and healthcare professionals
with a service portal for remote patient data
access and alert notification via a healthcare
dashboard; and (ii) a cloud manager/broker that
performs protocol translations for requests and
responses between the User Agent(s) and the
Public Cloud(s), and allocates cloud resources
based on user preferences or performance
criteria.
Cost-effectiveDesignofReal-timeHomeHealthcareTelemonitoring
11
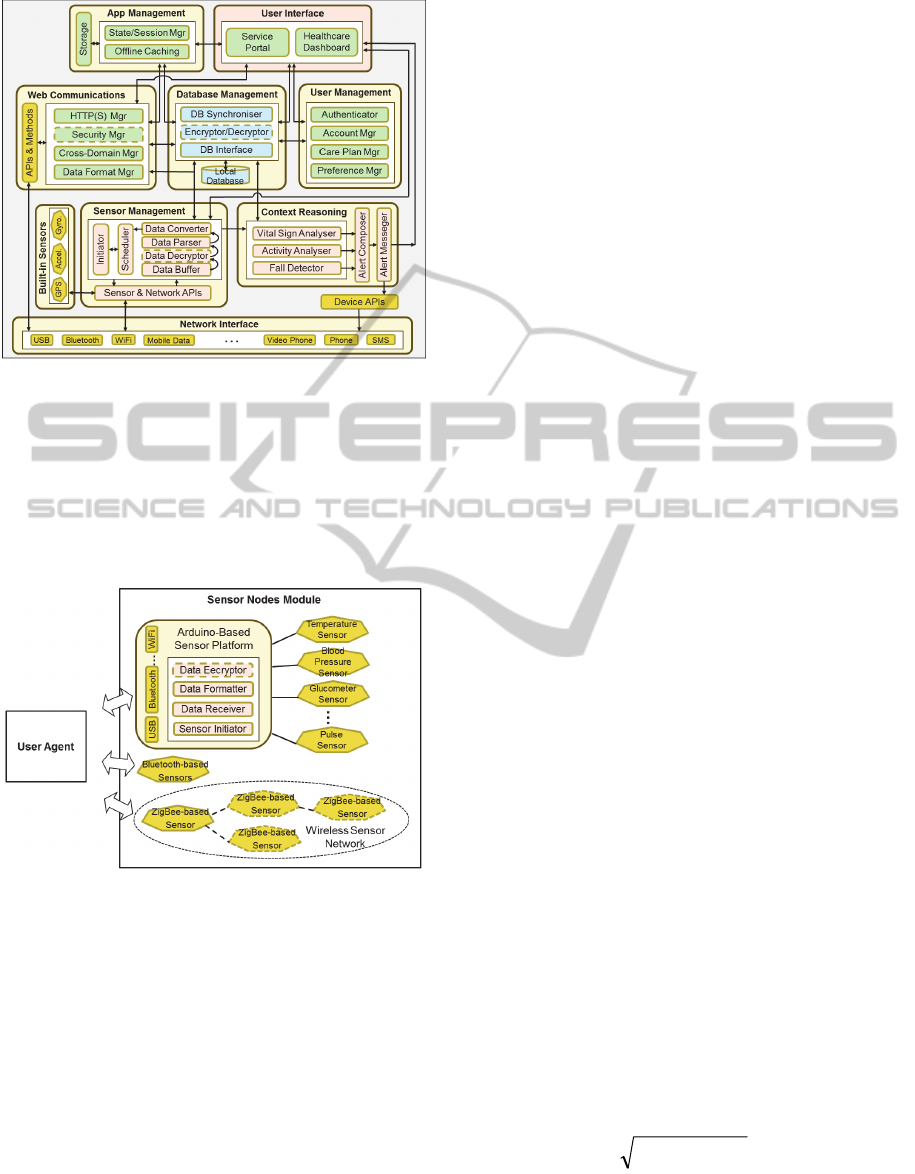
Figure 4: Architecture Diagram of the User Agent Module
(Liang and Krause, 2013).
The Public Cloud(s) Module: With the help of
the Service Gateway Module, this Module can
consist of a variety of cloud platforms, such as
AWS, GAE, cloud-based Social networking
websites, and free cloud-based health data
storage, e.g. HealthVault.
Figure 5: Architecture Diagram of the Sensor Nodes
Module.
Sensor Nodes: This module is composed of a
number of off-the-shelf portable sensor devices
(see Figure 5) to collect data for vital sign
monitoring, safety monitoring and activity
monitoring.
3.3 Experimental Design
and Cost-effectiveness Analysis
3.3.1 Limitations
Due to limited resources, time and funding in
particular, it is impractical for this research to design
and implement a randomised controlled trial to
measure costs and effects over several years, as
normally done in the health sector. Instead, this
research will only conduct some simulated trials and
adopt a revised comparative effectiveness analysis
approach for economic evaluations. The purpose
behind this is to evaluate whether there is a case for
designing a full scale trial without committing to the
expense of such a trial.
Another limitation is the unavailability of low-
cost, portable, programmable, and, most
importantly, clinically certified, sensor devices in
healthcare. As a result, this research will have to use
uncertified sensor devices, making a real clinical
trial unrealisable.
3.3.2 Experimental Design and Results
To date, a proof-of-concept prototype using Ruby on
Rails framework has been developed mainly based
on expanding and integrating three standalone
projects under the same theme of “Medical Alert
Management” in the Department of Computing,
University of Surrey, UK. Each of them had
different focuses, ranging from data presentation,
sensor data collection, to data storage.
Meanwhile, the development of the Sensor
Nodes Module and the integration of a real-time
remote monitoring function and those three projects,
as well as the implementation of the User Agent
Module on iPhone 5, are underway. Currently, by
using a web browser, an authorised remote user such
as a registered GP can use the dashboard to access
and review historical patient monitored data stored
in a remote server’s MySQL database. In addition,
the user can switch some panels inside the
dashboard to display dynamic real-time monitored
data, such as body temperature, heartbeat rate and
ambient temperature, which is first received by the
User Agent Module through either a Bluetooth
wireless connection or wired.
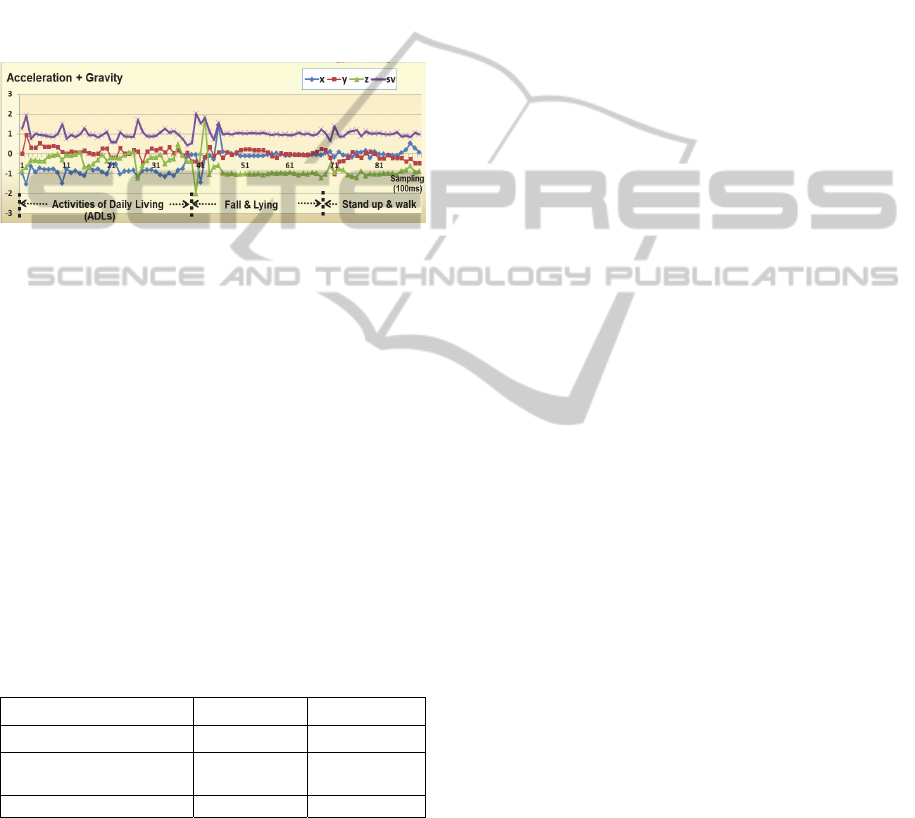
For the purpose of human fall detection, we
currently adopt a wearable device approach, mainly
based on accelerometry-related parameters, such as
the sum vector (SV) of acceleration in X-Y-Z axes
(see Equation 3). Figure 6 shows both SV and
acceleration signatures in an intentional forward fall
using the on-board accelerometer of the Texas
Instruments’ SensorTag.
222
zyx=SV
(3)
When building our fall detection algorithm, we first
assumed that a fall followed by lying motionless is
an emergency that needs to trigger an alert. 30
HEALTHINF2014-InternationalConferenceonHealthInformatics
12
simulated activities of daily living (ADL), each
followed by an intentional forward fall on a cushion,
were performed by locating either a SensorTag or an
iPhone with a built-in accelerometer at different
places of a volunteer’s body, such as ear side, jacket
pocket, shirt chest pocket, pants pocket, or handheld
(Liang and Krause, 2013). To make our simulated
falls closer to reality, we did not strictly confine the
sensors to a certain tilting angle or orientation. Such
a research design is apparently different from a
number of studies (Kangas et al., 2007; Yang and
Zhao, 2011; He, Li and Bao, 2012).
Figure 6: Changes of SV and Acceleration in X-Y-Z Axes
in an Intentional Forward Fall.
The results from 22 falls (eight falls were
excluded due to noisy data) revealed that when SV
first drops below 0.79g (1
st
threshold) before
bouncing over 1.48g (2
nd
threshold) and then after a
few oscillations it remains in the interval between
1.125g and 0.89g (3
rd
threshold) for more than 2
seconds, a serious fall might have occurred.
Nevertheless, dropping or throwing an
accelerometer could produce similar SV signature.
Consequently, we add another threshold at 0.15g (4
th
threshold) to detect a free fall situation, which
enables us to distinguish all device drops/throws
from human falls.
Table 1: Results of fall detection using 3-threshold or 4-
threshold algorithms (Liang and Krause, 2013)
(accelerometer range: ±2g, sampling rate: 10Hz).
3 thresholds 4 thresholds
Sensitivity 95.5% 95.5%
Specificity for device
drops/throws
0% 100%
Specificity for ADLs 95.5% 95.5%
In Table 1, sensitivity is defined as the
percentage of successfully identified falls and
specificity is the percentage of successfully
identified non-fall tests. Indeed, we have also
developed another algorithm to identify intentional
device shaking events, which sometimes can
produce almost identical SV signatures to human
falls. However, instead of using the new algorithm at
the expense of less sensitivity, we add a function to
ask for user confirmation before an alert is sent to
remote caregivers.
Regarding vital sign monitoring, we use an
Arduino-compatible platform (Seeeduino Stalker
v2.1 shield manufactured by Seeed Studio) and
clinically uncertified sensors (e-Health Sensor
Platform v1.0 with optional sensor kits, such as
pulse, oxygen in blood, body temperature and body
position sensors by Cooking Hacks). Nevertheless,
the accuracy and reliability of the used sensors have
been disappointing so far. For example, the highest
body temperature measured by the e-Health Sensor
Platform’s thermometer was under 30 degree
Celsius and the body position sensor just did not
work. According to the manufacturer of the e-Health
Sensor Platform, a possible reason might be
incompatibility between the e-Health Platform and
the Seeeduino Stalker shield, as the former is
designed for Arduino. However, after some
relatively minor modifications to the sensors and
wiring, our User Agent Module can start receiving
meaningful data from some of the sensors. We
believe the results can be further improved with
more work (Liang and Krause, 2013).
As for movement pattern monitoring, we plan to
use received signal strength from three triangular
deployed reference sensors, such as SensorTags, for
in-home patient location and movement estimation.
However, due to limited resources, we currently
have only one SensorTag. By measuring received
signal strength from a man-carried SensorTag, we
can roughly estimate the distance between the man
and the User Agent with an accuracy of around two
to three meters.
3.3.3 Cost-effectiveness Analysis
Due to the above-mentioned limitations, this
research calculates neither CER nor ICER directly,
but performs simulated trials to predict the
effectiveness of the proposed system and then
conduct cost-effectiveness analysis based on a
revised comparative effectiveness analysis approach.
Four types of comparisons, including the
comparison between simulated control and
intervention groups, for building up evidence of
cost-effectiveness are made.
Figure 7 shows the concept diagram for a
comparative effectiveness analysis approach which
compares our simulated trials with existing
randomised controlled trials. Data about the costs
and effects (the resulting changes in a group of
patients’ health status from Health Status X to
Cost-effectiveDesignofReal-timeHomeHealthcareTelemonitoring
13
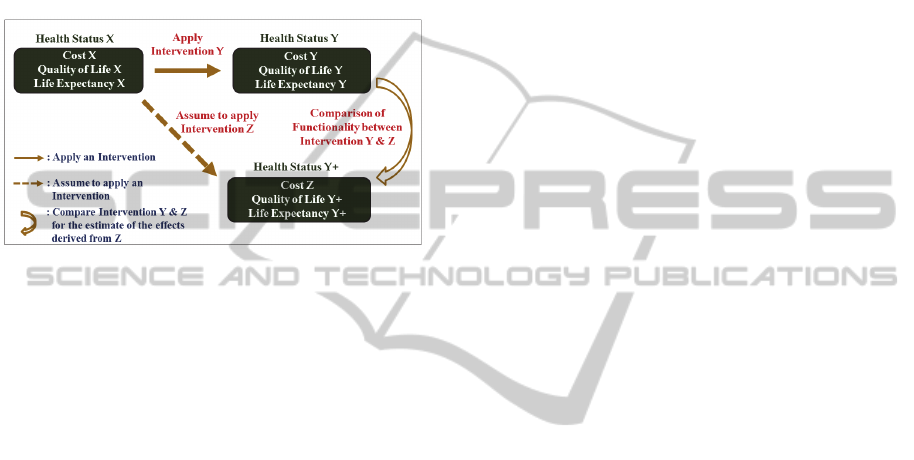
Health Status Y) of a known Intervention Y is first
obtained from literature review. Then we can claim
that our proposed Intervention Z can provide the
same QALY effects or better QALY effects (i.e.
Health Status Y+ with Quality of Life Y+ and Life
Expectancy Y+) than Intervention Y, if Intervention
Z has the same or better functionality/performance.
Finally, Cost Z and ICER of Intervention Z are
calculated for cost-effectiveness analysis (Liang and
Krause, 2013).
Figure 7: Concept Diagram for a Comparative
Effectiveness Analysis Approach (Liang and Krause,
2013).
To enable ourselves to satisfactorily conduct
cost-effectiveness analysis and to make claims about
the generalisability of this research, we first need to
further improve the reliability and accuracy of both
our event reasoning algorithms and the sensors. The
technical problem of incompatibility among devices
also needs to be better resolved. Meanwhile, a more
stable and well-defined testing environment has to
be carefully designed to make our simulation more
meaningful and robust.
4 CONCLUSIONS
In this paper, we have discussed the long-standing
problem of lacking robust evidence for cost-
effectiveness of healthcare technologies. To tackle
this issue, we have broadly assessed the implications
of recent advances in sensor technologies, smart
home, Internet of Things and mobile cloud
computing in support of achieving a cost-effective
design of a home healthcare telemonitoring solution.
We then have proposed a system architecture based
on mobile cloud computing and developed a proof-
of-concept prototype together with a novel
comparative cost-effectiveness analysis approach
based on simulated trials. Through the experimental
design, we believe that the proposed system is a
good foundation for moving forward.
In addition to the future work mentioned in
Section 3.3.3, we will also work on the development
of the Service Gateway Module to integrate all the
proposed system components as a whole, and
complete simulated trials and cost-effectiveness
analysis. Whilst we may not be able to deliver a
complete solution, we are confident that the
methodological contribution of test environment
plus simulation models will enable us to put the
evaluation of telehealth solutions prior to moving to
full-scale trials on a more scientific basis.
REFERENCES
Arduino website, 2013, “Arduino – Introduction”, viewed
28 Apr. 2013, <http://arduino.cc/en/Guide/
Introduction>.
Barlow, J., Singh, D., Bayer, S. & Curry, R., 2007, “A
systematic review of the benefits of home telecare for
frail elderly people and those with long-term
conditions”, Journal of Telemedicine and Telecare,
vol. 13, no. 4, pp. 172-179.
Bergmo, T., 2010, “Economic evaluation in telemedicine
– still room for improvement”, Journal of
Telemedicine and Telecare, Vol. 16, no. 5, pp. 229-
331.
Cheng, H.T. & Zhuang, W., 2010, “Bluetooth-enabled in-
home patient monitoring system: Early detection of
Alzheimer's disease”, IEEE Wireless
Communications, Vol. 17, Issue 1, pp.74 – 79.
den Hartog, F. T. H. et al. 2004, “Convergence of
Residential Gateway Technology”, IEEE
Communications Magazine, May 2004, pp. 138-143.
Department of Health, 2011, “Whole System
Demonstrator Programme: Headline Findings”.
Elderly Accommodation Counsel, 2003, “Smart Home - A
Definition”, viewed 5 Jan. 2013,
<http://www.housingcare.org/information/detail-2545-
smart%20home-a-definition.aspx>.
Faludi, R., 2010, “Building Wireless Sensor Networks”,
O’REILLY, CA, USA.
Gaddam, A., Mukhopadhyay, S.C., Sen Gupta, G., 2011,
“Trial & experimentation of a smart home monitoring
system for elderly”, IEEE Instrumentation and
Measurement Technology Conference (I2MTC).
He, Y., Li Y. & Bao, S.D., 2012, “Fall Detection by Built-
In Tri-Accelerometer of Smartphone“, IEEE-EMBS
International Conference on Biomedical and Health
Informatics (BHI 2012), Conference Proceedings, p.
184-187.
Henderson, C. et al., 2013, “Cost effectiveness of
telehealth for patients with long term conditions
(Whole Systems Demonstrator telehealth
questionnaire study): nested economic evaluation in a
pragmatic, cluster randomised controlled trial”,
BMJ2013;346:f1035 doi: 10.1136/bmj.f1035.
Hoang, D. B. & Chen, L., 2010, “Mobile Cloud for
HEALTHINF2014-InternationalConferenceonHealthInformatics
14

Assistive Healthcare (MoCAsH)“, 2010 IEEE Asia-
Pacific Services Computing Conference (APSCC),
Conference Proceedings, pp.325 – 332.
Huang, D., 2011, “Mobile Cloud Computing”, Multimedia
Communications Technical Committee, IEEE
Communications Society, E-Letter, Vol. 6, No. 10, pp.
1-4.
International Telecommunication Union (ITU), 2005,
“ITU Internet Reports 2005: The Internet of Things”.
Kang, B. et al. 2011, “Design of an Internet of Things-
based smart home system”, the 2nd International
Conference on Intelligent Control and Information
Processing, Conference Proceedings, pp.921-924.
Kangas, M. et al., 2007, “Determination of simple
thresholds for accelerometers for fall detection”, The
29th Annual International Conference of the IEEE
EMBS”, Conference Proceedings, p.1367-1370.
Koch, S., 2006, “Home telehealth – Current state and
future trends”, International Journal of Medical
Informatics, Volume 75, Issue 8, Pages 565–576.
Liang, P.C. & Krause P., 2013, “Cost-effective Healthcare
Telemonitoring”, Conference on Mobile and
Information Technologies in Medicine 2013
(MobileMed), Conference Paper 4.
Limburg, M., Gemert-Pijnen, J., Nijland, N., Ossebaard,
H., Hendrix, R. & Seydel, E., 2011, “Why Business
Modeling is Crucial in the Development of eHealth
Technologies”, Journal of Medical Internet Research
(JMIR), 13(4): e124.
Marinelli, E., 2009, “Hyrax: Cloud Computing on Mobile
Device Using MapReduces”, Carnegie Mellon
University, MSc Thesis.
McCullagh, P. & Augusto, J., 2011, “The Internet of
Things: The Potential to Facilitate Health and
Wellness”, CEPIS UPGRADE, Vol. XII, Issue no. 1,
pp. 59-68.
McLean, S., Prott, D. & Sheikh, A., 2011, “Telehealthcare
for long term conditions”, BMJ 2011; 342:d120, doi:
10.1136/bmj.d120.
Muenning, P., 2008, “Cost-Effectiveness Analysis in
Health: A Practical Approach”, 2
nd
ed., Jossey-Bass,
Hoboken, NJ, USA.
National Institute for Health and Care Excellence, 2013,
“Guide to the methods of technology appraisal 2013”.
Phillips, C., 2009, “What is cost-effectiveness?”, Health
economics, 2
nd
ed., viewed 17 Apr. 2013,
<http://www.medicine.ox.ac.uk/bandolier/painres/dow
nload/whatis/Cost-effect.pdf>.
Qureshi, S. et al. 2011, “Mobile cloud computing as future
for mobile applications - Implementation methods and
challenging issues”, IEEE International Conference on
Cloud Computing and Intelligence Systems (CCIS),
Conference Proceedings, pp.467 – 471.
Sanders, C. et al., 2012, “Exploring barriers to
participation and adoption of telehealth and telecare
within the Whole System Demonstrator trial: a
qualitative study”, BMC Health Services Research
2012.
Sarasohn-Kahn, J., 2010, “How Smartphones Are
Changing Health Care for Consumers and Providers”,
California Healthcare Foundation.
Steventon, A. et al., 2012, “Effect of telehealth
interventions on use of secondary care and mortality:
findings from the Whole System Demonstrator cluster
randomised trial”, BMJ2012;344:e3874 doi:
10.1136/bmj.e3874.
Steventon, A. et al., 2013, “Effect of telecare on use of
health and social care services: findings from the
Whole System Demonstrator cluster randomised trial”,
Age and Ageing 2013; 0: 1-8 doi:
10.1093/ageing/aft008.
Sundmaeker, H. et al., 2010, “Vision and Challenges for
Realising the Internet of Things”, European
Commission.
Viet, V. Q., Lee, G. & Choi, D., 2012, “Fall Detection
based on Movement and Smart Phone Technology”,
2012 IEEE-RIVF International Conference on
Computing and Communication Technologies,
Conference Proceedings, pp.1-4.
Wang, C. C. et al., 2008, “Development of a Fall
Detecting System for the Elderly Residents”, The 2nd
International Conference on Bioinformatics and
Biomedical Engineering 2008, Conference
Proceedings, pp.1359-1362.
Wei, Z. et al,. 2010, “A Residential Gateway Architecture
Based on Cloud Computing”, 2010 IEEE International
Conference on Software Engineering and Service
Sciences (ICSESS), IEEE Conference Publications,
pp.245-248.
Wu, C. Y. et al. 2009, “Introduction and Application of
Important Digital Home Standard Alliances” (in
Chinese), TLTECHNICAL Journal, Vol. 39, No.5, pp.
601-620.
Yang, Y. & Zhao, X., 2011, “Development of a Fall
Detection Algorithm based on a Tri-axial
Accelerometer”, The 4th International Conference on
Biomedical Engineering and Informatics (BMEI),
Conference Proceedings, Vol. 3, pp.1371-1374.
ZigBee Alliance, 2009, “ZigBee Wireless Sensor
Applications for Health, Wellness and Fitness”.
ZigBee Alliance, 2012, “ZigBee 2012 Specification
Features At-A-Glance”.
Zimmermann1, G. & Vanderheiden, G., 2007, “The
Universal Control Hub : An Open Platform for
Remote User Interfaces in the Digital Home”, Lecture
Notes in Computer Science, Vol. 4551, pp.1040-1049.
Cost-effectiveDesignofReal-timeHomeHealthcareTelemonitoring
15
