
Does Being Monitored during Sleep Affect People on a Cognitive
and a Behavioral Level?
M. S. Goelema
1,2
, R. Haakma
1
and P. Markopoulos
2
1
Philips Group Innovation Research, Eindhoven, The Netherlands
2
Department of Industrial Design, Eindhoven University of Technology, Eindhoven, The Netherlands
Keywords: Self-monitoring, Reactivity, Wearable Devices, Sleep.
Abstract: Nowadays it is possible to monitor behavior or physiological features with specially-made devices that
make self-monitoring an accessible and simple activity. Unknown is the effect these wearable devices may
have on people’s lives and this also applies to the area of sleep monitoring devices. The aim of this
preliminary study is to address the extent to which sleep monitoring devices affect people on a cognitive and
behavioral level. Four participants aged from 34 to 60, filled out a sleep diary for three consecutive weeks
and wore in the latter two weeks a sleep monitoring device. Adjustments on a cognitive and behavioral level
were observed, but this was probably due to participating in this study and completing the sleep diary as was
indicated by the participants. Since the market for self-monitoring devices is rapidly developing and more
accessible for lay people, it is important to investigate the reactive outcomes of these devices as they may
have consequences for people who have a high adherence to self-control. Moreover, the knowledge about
self-monitoring will improve which will lead to better interventions carried out by, for example, sleep
coaches.
1 INTRODUCTION
An international collaboration between users and
producers of self-tracking devices has emerged,
called the ‘Quantified Self’ (www.quantifiedself.
com). By exchanging information and with reviews
of the products they keep each other updated. Due to
the monitoring, users achieve more knowledge about
their bodily functions and performance during the
day. Self-tracking devices may additionally operate
as an aid for interventions. The collected data are
then transferred to a ‘personal’ coach, for example,
through an application on the mobile phone. These
coaches are able to advice and monitor patients
remotely and for a sustained time period. Self-
tracking devices utilized for these kind of purposes
are rising (LeMaster et al., 2008; Going et al., 2003).
According to Swan (2012) the health care industry is
shifting towards an approach of personalized
preventive health maintenance and away from an
exclusive attention to disease treatment. For self-
monitoring this means that due to the development
of wearable devices the possibility emerges to
monitor unaware processes, such as physiological
features, instead of relying on self-reports.
Previous literature in diverse research areas
shows that when self-monitoring is used as an
intervention, successful results are obtained, for
example: weight loss (Burke et al., 2011; Boutelle
and Kirschenbaum, 1998; Wang et al., 2012; Butryn
et al., 2007) improved academic performance
(Amato-Zech et al., 2006; Maag et al., 1993;
Shimabukuro et al., 1999) control of blood glucose
levels (Karter et al., 2001; Martin et al., 2006) and
less substance use (Litt et al., 1998; Helzer et al.,
2002), although sometimes the effect of self-
monitoring is small or not found (Hufford et al.,
2002; O’kane et al., 2008). These results make the
effect of self-monitoring ambiguous, which may
have several causes, such as different study
populations (different size and patient populations),
diverse methods used and variable duration of the
studies.
Much attention has been paid to the reactivity of
self-monitoring. Reactivity is a phenomenon that
occurs when individuals adjust their performance or
behavior due to the awareness that they are being
observed (Korotitisch and Nelson-Gray, 1999). Self-
monitoring consists of two processes: firstly, self-
observation: one must discriminate or notice the
27
S. Goelema M., Haakma R. and Markopoulos P..
Does Being Monitored during Sleep Affect People on a Cognitive and a Behavioral Level?.
DOI: 10.5220/0004745700270033
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 27-33
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

occurrence of the target behavior. Secondly, self-
recording: one needs to record when the target
behavior is occurring (Korotitsch and Nelson-Gray,
1999). Kazdin (1974) investigated with the
performance on a sentence-construction task,
different aspects of self-monitoring, such as
response desirability, goal setting and feedback.
They found several interesting results, but
particularly relevant in this case were: (i) supplying
a performance goal or feedback enhanced the
reactive effects of self-monitoring, (ii) monitoring
one’s own behavior or being monitored by someone
else was equally reactive, (iii) the process of self-
recording, independently of observing the results,
led to behavior change. These results indicate that
when a person purely monitors himself, reactive
behavior is seen. Moreover, the impact of the
adjusted behavior can be augmented by setting a
goal and/or providing feedback and an insight in the
observed data is not necessarily needed to alter
behavior.
The study of McFall (1970) shows that effects of
self-monitoring can occur even without the
determination of a goal. The participants were not
motivated to stop smoking and every effort was
made to minimize the participant’s motivation to
stop smoking during the study period. After 13 days
of self-monitoring the frequency of having a
cigarette significantly increased in comparison to the
baseline condition, where the participants were
secretly monitored by others. The long-lasting effect
of a behavior modification after self-monitoring is
unclear and longitudinal studies are needed to
provide more insight in this matter. Subsequent
studies after the 70s put more emphasis on self-
monitoring as a tool for an intervention as opposed
to investigating the aspects related to the process of
reactivity of self-monitoring.
A recent article illustrated the possibility of
reactivity in the baseline assessment of physical
activity when using an accelerometer device (Motl et
al., 2012). Two identical studies were carried out
wherein persons with multiple sclerosis (MS) wore
an accelerometer for seven days to collect baseline
data and one week later wore a pedometer over a
seven days period (first week of a behavioral
intervention). They found a decrease of the average
steps per day over the first week of the behavioral
intervention compared to baseline measurements.
Apart from the study of Motl et al. (2012),
underemphasized are the consequences wearable
devices may have on a cognitive and behavioral
level.
This study investigates the reactivity effects of
wearing a monitoring device during sleep. As where
it is unclear to which extent people are affected
when being monitored during sleep, although one is
able to monitor their sleep at their own home and
independently. Being monitored during sleep,
regardless of the subconscious state of sleep, may
influence the behavior before going to bed as well as
the behavior after waking up. Additionally, persons
may modify their cognitions about sleep because
they become more aware of their sleeping habits. As
a result, the device might show different results than
it otherwise would have shown (normal night
without monitoring). Sleep studies have traditionally
required users to fill out a diary every morning
(Carney et al., 2012; Keklund and Åkerstedt, 1997),
but the opportunity arises to support sleep studies
with a monitoring device for the home or to replace
the diary altogether.
The sleep monitoring devices, available on the
consumer market, all postulate that they are
unobtrusive in a way that they do not disturb people
during their sleep. Nevertheless, they can have an
effect on a cognitive and behavioral level, but this
has not been researched. As a result, with the current
development of sleep monitoring devices
increasingly being used by lay people, the aim of
this explorative study is to address the extent to
which sleep monitoring devices affect people on a
behavioral and cognitive level. In this study the self-
monitoring is occurring automatically and no
specific attention is needed and no goal is set or
feedback is given. Moreover, the awareness of being
monitored plays an important role in this study.
2 METHODS
2.1 Participants
For this study four adults were recruited, aged
between 34-60 years. Men and women were equally
distributed. All participants stated that they do not
experience any sleeping problems, but one of the
participants reported sleeping somewhat different
than usual at the time of the study because of her
pregnancy. The participants were blind to the
experimental hypotheses and were told that the
purpose of this study was to research the overall
sleep experience when being monitored during
sleep.
2.2 Measures
The sleep quality at baseline was measured with the
HEALTHINF2014-InternationalConferenceonHealthInformatics
28

Pittsburgh Sleep Quality Index (PSQI) questionnaire
which determines sleep quality and disturbances
over an one-month time interval (Buysse, et al.,
1989). Based on a cut-off score of 5, participants can
be categorized into “poor” sleepers (> 5) or “good”
sleepers (≤ 5) The PSQI consists of 19 self-rated
questions, divided into seven components:
subjective sleep quality, sleep latency, sleep
duration, habitual sleep efficiency, sleep
disturbances, use of sleep medication and daytime
dysfunction. An overall PSQI score was calculated
from the seven components with a score range
between 0 and 21 and higher scores reflect worse
sleep quality. The sensitivity and specificity of the
PSQI are respectively 89.6% and 86.5% (Buysse et
al., 1989). In our sample it turned out that the two
men had a score of lower than 5 as where the women
had a score of 6. This suggests that the women may
have some sleeping problems. However, the scoring
range of sleeping problems runs from 6 to 21. The
score of 6 falls in the lower end of this range.
The sleep monitoring device used in this study
was the Actiwatch by Philips (Figure 1). It was
developed to distinguish between physical activity
and rest, and it is widely used in the sleep field for
detecting sleep-circadian rhythm disorders. The
Actiwatch uses an accelerometer to detect and log
wrist movement, also known as actigraphy that
indicates gross body movement. The model worked
with was the Actiwatch Spectrum; it weighs 21 g,
measures 31 x 28 x 10 mm and has a maximum
sampling frequency of 32 Hz (Philips / Respironics,
URL: http://www.healhcare.philips.com). The
Actiwatch feels and looks like a standard wristwatch
and was used as a tool to measure the effect of being
monitored during sleep as unobtrusively as possible.
As we believe the Zeo headband (Shambroom et al.,
2012) is more obtrusive to wear during sleep than a
wristwatch, since most people are already used to
wear a watch and not to wear a headband. In
addition, Cole et al., (1992) found that when
comparing polysomnography with actigraphy, a
wrist actigraph is able to measure sleep/wake
parameters relatively accurately.
Subjective sleep experience was assessed by the
Consensus Sleep Diary (CSD; Carney et al., 2012).
The CSD was developed with the intention that it
should be a consensus and standardized sleep diary
for sleep researchers, who before its development
would use a variety of divers diary formats.
For this study the core CSD was used
which
consisted of 8 items, including questions about
initiating and maintaining sleep as well as a
global appreciation of sleep (Table 1). Moreover, an
Figure 1: The Actiwatch Spectrum.
additional question was added to the diary whether
the participant was well rested the next morning, to
assess an insight in the sleep experience after
wearing the device. In addition, to obtain a more
complete answer on the behavioral effect of being
monitored another question was affixed to the diary,
namely: ‘What did you do in the last hour before
going to bed?’.
Table 1: Consensus Sleep Diary-Core.
Consensus Sleep Diary-Core
1. What time did you get into bed?
2. What time did you try to go to sleep?
3. How long did it take you to fall asleep?
4. How many times did you wake up, not
counting your final awakening?
5. In total, how long did these awakenings
last?
6. What time was your final awakening?
7. What time did you get out of bed for the
day?
8. How would you rate the quality of your
sleep? (very poor, poor, fair, good, very
good)
Three structured interviews were held to analyze the
cognitive and behavioral effects of sleep monitoring.
The questions in these interviews are self-made and
deal specifically with how participants experienced
the device and questions concerning the cognitive
and behavioral effects of wearing the sleep
monitoring device. Examples of questions are: ‘Did
you feel the device last night?’, ‘Did you wake up of
the device last week?’, ‘Did you think more of your
sleep during the two weeks of being monitored?’,
‘Did you change any sleeping habits during the two
weeks of being monitored?’ and ‘Did you sleep
differently last week?’. In all three interviews the
same questions were asked, including open as well
as closed (with response options) questions, and
some questions were only asked in the last
interview, as a consequence of withholding the
purpose of this study.
DoesBeingMonitoredduringSleepAffectPeopleonaCognitiveandaBehavioralLevel?
29
2.3 Procedure
At the start of baseline phase, the demographic
variables like age, gender and the PSQI were
assessed to characterize the sample. To establish
how sleep was when not being monitored by a
device, participants completed a sleep diary for a
week prior to the two weeks of wearing the
Actiwatch. In addition, participants also maintained
the sleep diary during the two weeks of being
monitored by the Actiwatch, as the sleep diary
contained supplementary questions about sleeping
habits. Participants were instructed to wear the
Actiwatch when they went to bed and to take off the
Actiwatch after the final awakening. During the two
weeks of wearing the Actiwatch the three interviews
were executed; after the first night, after one week
and after two weeks. The reason for the time period
of this study was that participants needed to get used
to wearing the Actiwatch. In the last interview
participants were debriefed regarding the purpose of
this study and questions were answered.
3 RESULTS
All participants answered to the question ‘if they
changed any sleeping habits’ negatively. However,
further on in the interview it became clear that one
participant did not drink any coffee anymore after
dinner time and tried not to work after 10:00 pm
(Table 2). As was indicated by the participant, this
adjustment was probably a result of participating in
this study. The same participant wanted to change
the time of going to bed due to filling out the sleep
diary, but did not succeed because of other
obligations. The three other participants did not
change any sleeping habits during the study period.
Participants held a particular regularity in their
activities before going to bed, according to the
answers given in the sleep diary. The most
prominent activity performed before going to bed
was watching television, closely followed by
browsing the web and reading. The activities
showering and having a conversation were also often
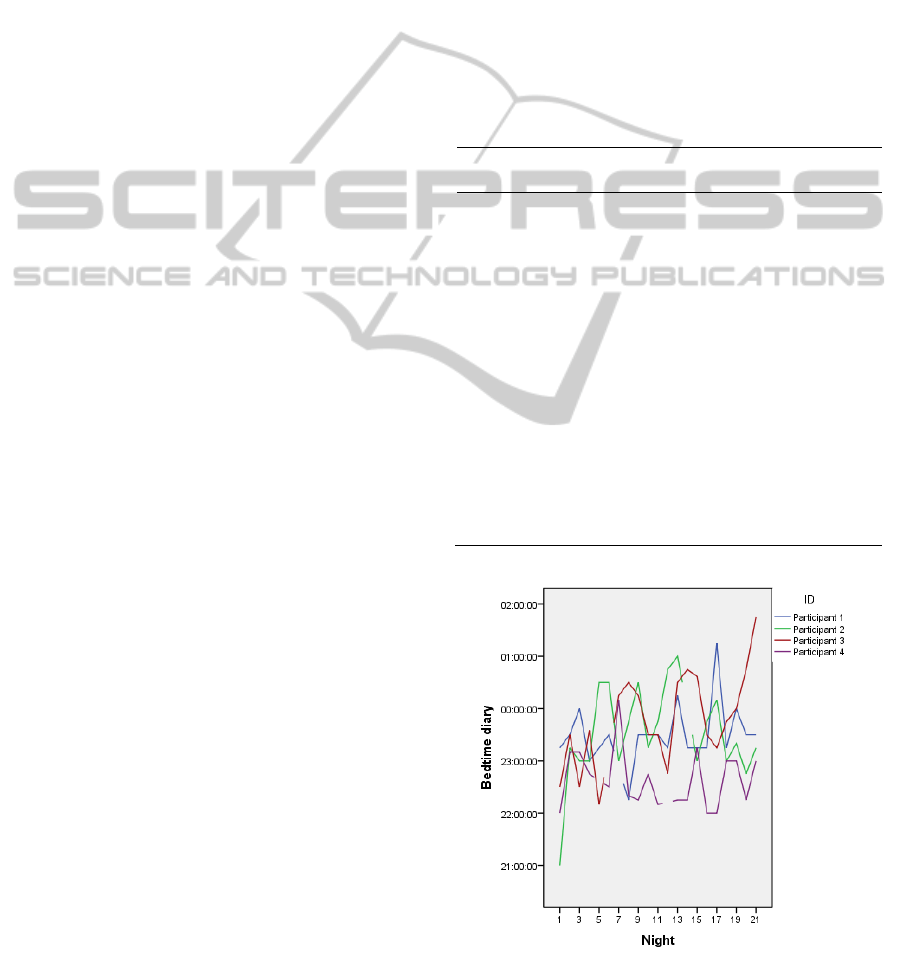
referred to. In addition, the bedtimes of the
participants did not vary between the week of non-
monitoring and the two weeks of being monitored
by the device, as was shown in the Actiwatch data
and the sleep diary (Figure 2). As answered in the
last interview participants did not have the feeling of
having slept differently when being monitored
during sleep.
On a cognitive level, two out of four did think
more about their sleep but stated that it was more a
result of filling out the diary than of wearing the
sleep monitoring device (Table 2). By completing
the sleep diary these two participants got more
conscious about their sleeping times. As said earlier,
one of those participants tried to shift the time of
going to bed to an earlier time, but accomplishing
that was harder than expected because of other
obligations. Two participants did not show any
adjustments on a cognitive and behavioral level. One
of the latter two had a strong ‘Big-Brother is
watching you’ feeling during the study, but as was
indicated by the participant, this feeling would be
less when being monitored for own purposes.
Table 2: Results of reactivity in this study.
Cognitive
changes
Behavioral
changes
Participant 1 Went to bed later
than expected.
Did not drink coffee
anymore after dinner
time. - Tried not to
work after 10:00 pm. -
Tried to go to bed
earlier but failed due
to other obligations.
Participant 2 Did not sleep as
much as thought.
No changes in
behavior towards
sleep.
Participant 3 No changes in
thoughts about
sleep.
No changes in
behavior towards
sleep.
Participant 4 No changes in
thoughts about
sleep.
No changes in
behavior towards
sleep.
Note. The cause of the changes above is not clear.
Figure 2: The diary bedtimes of the three weeks, displayed
separately for each participant.
HEALTHINF2014-InternationalConferenceonHealthInformatics
30

With regard to wearing the Actiwatch, after
wearing the device for the whole study period two
out of four did not feel the device anymore. The two
other participants still felt it a bit because of the
dimensions of the device and one of the latter two
was not used to wear a watch during the night. To
the question ‘if the device bothered them’ they all
responded negatively and their sleep was not
affected by the device. Two participants would wear
the device in the future, but then for limited periods
only.
4 DISCUSSION
This preliminary study shows adjustments on a
cognitive and behavioral level, but could not
separate whether these were due to the monitoring
device or hose to participation in the study as such,
and the daily diary keeping, as was indicated by the
participants. Completing the sleep diary was more
excitatory than wearing a sleep monitoring device. It
was expected that due to wearing the sleep
monitoring device people would pay more attention
to their sleep. However, in this study, two out of four
did not think more about their sleep. One
explanation may be that, apart from the awareness of
being monitored, utilizing the device was
commissioned by this study and probably the
participants were not interested enough in the
subject of sleep for themselves. This means that they
focused their attention to other concerns rather than
to their sleep or sleep related properties. The
medium obtrusiveness of the device may have
played a substantial role in this as well. Moreover,
the results may be dissimilar when there were
participants involved who experience sleeping
problems, but this point will be discussed in more
detail later.
Regarding the effect of being monitored during
sleep on a behavioral level, one participant did not
drink any coffee more after dinner time and tried not
to work after 10:00 pm. What the cause is of this
change is unclear. However the participant indicated
that due to participating in this study, the thought
about sleep increased and the participant decided to
carry out this behavioral change (also known as the
Hawthorne-effect). Additionally, the same
participant tried to modify his or her bedtime
because of filling out the diary, but failed to go to
bed earlier because of other obligations. No
behavioral changes were observed for the other three
participants. Kazdin (1974) proved with their study
that when setting a goal or providing feedback the
effect of change in behavior augmented. In our study
no goal was set and no feedback was given. Despite
this, our research indicates some behavioral
changes, even with the open setting of this study and
this is in comparison with the study of McFall
(1970).
As mentioned before, being active with the sleep
diary had a much greater impact on the study results
than expected. This means that solely completing the
sleep diary could have had a similar effect. Expected
was that filling out the sleep diary would become
more an automatic process, as is shown in several
other studies (Litt et al., 1998; Stone et al., 2003). To
know in the future whether these outcomes
attributed to completing the diary or wearing the
device, these measurements should become separate
conditions in a study setup. However, due to the
self-report nature of interviewing, the results found
in this study still can be a result of the process of
reactivity on wearing the device. Besides this, the
results found in this study might be different if the
sleep monitoring device would be more interactive
and providing feedback.
Additionally, results could be different if the
study population would comprise of people who
experience sleeping problems or people who want to
improve their sleep. This implies, when choosing
people with sleeping problems as the study
population, that a motivation or goal is implicitly set
and feedback may be provided. These conditions
could be expected to produce different results
(Kazdin, 1974; Motl et al., 2012). As the wearable
monitoring devices evolve into accessible objects for
everyone, ignoring the reactivity of self-monitoring
could be a serious omission. As is mentioned earlier,
in this study some reactivity was observed, even
with the open setting of this study. In contrast, two
participants did not show any reactivity on each of
the measurements (wearable device or sleep diary).
5 CONCLUSIONS
This explorative study shows that when people -
who experience no sleeping problems - use an
unobtrusive sleep monitoring device, it barely has an
effect on a cognitive and behavioral level.
Conversely, reactivity effects were observed,
although unclear is what the cause is of these effects.
It is important to note that due to the explorative
character of this study no hard conclusion can be
drawn. However, this study shows that filling out a
sleep diary may be more intrusive than wearing a
sleep monitoring device. As a result, we are
DoesBeingMonitoredduringSleepAffectPeopleonaCognitiveandaBehavioralLevel?
31

currently running a study which investigates the
reactivity of filling out a sleep diary. Additionally,
this study demonstrates that there are many
unknowns about the effect of being monitored
during sleep and this is also true for the wearable
device in general. Whereas there has been
substantial research into the development of
wearable devices, there remains considerable scope
for research on the effect these devices may have on
people’s lives. It is important to know the reactive
outcomes of self-monitoring devices as the market
for these devices is rapidly growing and this may
have consequences for people who have a high
adherence to self-control. Moreover, a better insight
in the consequences of wearing such devices may
improve interventions carried out remotely by, for
example, sleep coaches.
REFERENCES
Amato-Zech, N. A., Hoff, K. E., and Doepke, K. J. (2006).
Increasing on-task behavior in the classroom:
Extension of self-monitoring strategies. Psychology in
the schools, 34(2):211-221.
Boutelle, K. N. and Kirschenbaum, D. S. (1998). Further
support for consistent self-monitoring as a vital
component of successful weight control. Obesity
Research, 6(3):219-224.
Burke, L. E., Wang, J., and Sevick, M. A. (2011). Self-
monitoring in weight loss: A systematic review of the
literature. Journal of the American Dietetic
Association, 111(1):92-102.
Butryn, M. L., Phelan, S., Hill, J. O., and Wing, R. R.
(2007). Consistent self-monitoring of weight: A key
component of successful weight loss maintenance.
Obesity, 15(12):3091-3096.
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S.
R., and Kupfer, D. J. (1989). The Pitssburg Sleep
Quality Index: A new instrument for psychiatric
practice and research. Psychiatry Research, 28:193-
213.
Carney, C. E., Buysse, D. J., Ancoli-Israel, S., Edinger, J.
S., Krystal, A. D., Lichstein, K. L., and Morin, C. M.
(2012). The consensus sleep diary: standardizing
prospective sleep self-monitoring. Sleep, 35(2):287-
302.
Cole, R. J., Kripke, D. F., Greun, W., Mullaney, D. J., and
Gillin, J. C. (1992). Automatic sleep/wake
identification from wrist actigraphy. Sleep, 15(5):461-
469.
Going, S., Thompson, J., Cano, S., Stewart, D., Stone, E.,
Harnack, L., Hastings, C., Norman, J. and Corbin, C.
(2003). The effects of the Pathways Obesity
Prevention Program on physical activity in American
Indian children. Preventive Medicine, 37:S62-S69.
Helzer, J. E., Badger, G. J., Rose, G. L., Mongeon, J. A.,
and Searles, J. S. (2002). Decline in alcohol
consumption during two years of daily reporting.
Journal of studies on Alcohol and Drugs, 63(5):551-
558.
Hufford, M. R., Shields, A. L., Shiffman, S., Paty, J., and
Balabanis, M. (2002). Reactivity to Ecological
Momentary Assessment: An example using
undergraduate problem drinkers. Psychology Of
Addictive Behaviors, 16:205-211.
Karter, A. J., Ackerson, L. M., Darbinian, J. A.,
D’Agostino, R. B., Ferrara, A., Liu, J., and Selby, J. V.
(2001). Self-monitoring of blood glucose levels and
glycemic control: the Northern California Kaiser
Permanente Diabetes Registry. American Journal of
Medicine, 111:1-9.
Kazdin, A. E. (1974). Reactive self-monitoring: The
effects of response desirability, goal setting, and
feedback. Journal of Consulting and Clinical
Psychology, 42(5):704-716.
Keklund, G. and Åkerstedt, T. (1997). Objective
components of individual differences in subjective
sleep quality. Journal of Sleep Research, 6:217-220.
Korotitsch, W. J. and Nelson-Gray, R. O. (1999). An
overview of self-monitoring research in assessment
and treatment. Psychological Assessment, 11:415-425.
LeMaster, J. W., Mueller, M. J., Reiber, G. E., Mehr, D.
R., Madsen, R. W., and Conn, V. S. (2008). Effect of
weight-bearing activity on foot ulcer incidence in
people with diabetic peripheral neuropathy: feet first
randomized controlled trial. Physical Therapy
,
88(11):1385-1398.
Litt, M. D., Cooney, N. L., and Morse, P. (1998).
Ecological Momentary Assessment (EMA) with
treated alcoholics: Methodological problems and
potential solutions. Health Psychology, 17(1):48-52.
Maag, J. W., Reid, R., and DiGangi, S. A. (1993).
Differential effects of self-monitoring attention,
accuracy, and productivity. Journal of Applied
Behavior Analysis, 26(3):329-344.
Martin, S., Schneider, B., Heinemann, L., Lodwig, V.,
Kurth, H. -J., Kolb, H., and Scherbaum, W. A. (2006).
Self-monitoring of blood glucose in type 2 diabetes
and long-term outcome: An epidemiological cohort
study. Diabetologia, 49:271-278.
McFall, R. M. (1970). Effects of self-monitoring on
normal smoking behavior. Journal of Consulting and
Clinical Psychology, 35(2):135-142.
Motl, R. W., McAuley, E., and Dlugonski, D. (2012).
Reactivity in baseline accelerometer data from a
physical activity behavioral intervention. Health
Psychology, 31(2):172-175.
O’Kane, M. J., Bunting, B., Copeland, M., and Coates, V.
E. (2008). Efficacy of self monitoring of blood glucose
in patients with newly diagnosed type 2 diabetes
(ESMON study): Randomised controlled trial. British
Medical Journal, 336(7654):1174-1177.
Shambroom, J. R., Fábregas, S. E., and Johnstone, J.
(2012). Validation of an automated wireless system to
monitor sleep in healthy adults. Journal of Sleep
Research, 21(2):221-230.
HEALTHINF2014-InternationalConferenceonHealthInformatics
32

Shimabukuro, S. M., Prater, M. A., Jenkins, A., and
Edelen-Smith, P. (1999). The effects of self-
monitoring of academic performance on students with
learning disabilities and ADD/ADHD. Education and
treatment of children, 22:397-414.
Stone, A. A., Broderick, J. E., Schwartz, J. E., Shiffman,
S., Litcher-Kelly, L., and Calvanese, P. (2003).
Intensive momentary reporting of pain with an
electronic diary: reactivity, compliance, and patient
satisfaction. Pain, 104:343-351.
Swan, M. (2012). Health 2050: The realization of
personalized medicine through crowdsoursing, the
quantified self, and the participatory biocitizen.
Journal of Personalized Medicine, 2:93-118.
Wang, J., Sereika, S. M., Chasens, E. R., Ewing, L. J.,
Matthews, J. T., and Burke, L. E. (2012). Effect of
adherence to self-monitoring of diet and physical
activity on weight loss in a technology-supported
behavioural intervention. Patient Preference and
Adherence, 6:221-226.
DoesBeingMonitoredduringSleepAffectPeopleonaCognitiveandaBehavioralLevel?
33
