
Route2Health
A Novel Routing Service to Assist in Increasing Physical Activity
Hassan A. Karimi and Monsak Socharoentum
Geoinformatics Laboratory, School of Information Sciences, University of Pittsburgh,
135 N. Bellefield Ave, Pittsburgh, PA 15213
Keywords: Health, Walking, Multi-modal Transportation, Active Transport, Physical Activity.
Abstract: Walking is the simplest and most common mode of transportation and is widely recommended for a healthy
lifestyle. However, other modes of transportation such as driving and riding are usually dominant when
distances are too long to walk. Existing routing and direction services are designed to mainly serve common
transportation requirements such as shortest distance, shortest travel time, minimum bus transfer, nearest
bus stop, or closest parking lot. Existing services do not consider however, user’s preference for walking as
the primary option, especially when multi-modal transportation is involved. This paper presents the concept
of a new service called Route2Health where walking, due to its several benefits including health, is
considered as the preferred mode of transportation. Route2Health, as a multi-modal transportation planning
service, recommends either walking, if feasible, between pairs of origin and destination locations as the only
mode of transportation or a combination of walking with other modes of transportation. Route2Health, if
used frequently, is potential to help increase physical activity levels overtime. A prototype Route2Health is
also discussed.
1 INTRODUCTION
Walking is an essential mode of transportation,
independent of vehicles or parking locations, and
does not rely on specific service routes or schedules.
Roads in urban and residential areas usually include
sidewalks to connect building entrances and other
locations that can be reached on foot. Walking plays
an important role in multi-modal transportation
planning. For example, when a person drives from
home (origin) to another location (destination),
walking maybe required between the parking lot and
the location of destination. In the case of public
transit, walking from an origin to a particular transit
stop, from a transit stop to the destination, and
between transit stops is commonplace.
Besides serving as a transportation mode,
walking can offer interesting and desired benefits to
travellers. For example, walking is considered as a
physical activity that can generally be performed by
many people regardless of geographic locations. It is
recommended by the United States Department of
Health and Human Services (1996) that moderate
intense activities such as 30 minutes of brisk
walking can lead to health benefits in adults.
Numerous studies (e.g., see Besser et al. 2005; Sallis
et al. 2004; Edwards 2008; and MacDonald et al.
2010) suggest that walking should be promoted as
part of daily public transportation to prevent or
mitigate various health conditions such as heart
disease and obesity. Morabia et al. (2010) conducted
a study and found that switching from private car to
public transportation when commuting to work
increased energy expenditure (more than 124
kilocalories/day) which is equivalent to the loss of 1
pound of body fat per 6 weeks. In an analysis of
cross-sectional health and travel data at country,
state, and city levels, Pucher et al. (2010) found
negative relationships between active travel (waking
and cycling) and self-reported obesity and negative
relationships between active travels and diabetes. As
a national agenda, walking is also promoted in
Healthy People 2020
1
project which sets a goal to
increase walking by at least 10%.
There is considerable variability in walking. For
example, some people usually choose to walk up to
a certain threshold, beyond which they will turn to
other means of transportation. The threshold varies
1
http://www.healthypeople.gov/2020/
43
Karimi H. and Socharoentum M..
Route2Health - A Novel Routing Service to Assist in Increasing Physical Activity.
DOI: 10.5220/0004750400430051
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 43-51
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

according to individual characteristics, for example,
weight, gender, behavior, health, and age. Younger
people with good health may be able to walk farther.
Older people may prefer shorter distances, lower
uphill slope, and better sidewalk surface conditions
than younger people. For instance a negative
relationship between age and speed of walking is
reported by Himann et al. (1988). People who have
an active lifestyle tend to walk faster, longer and
more frequent compared to those who are less
active. For example, a study by Bassett et al. (2008)
shows that in Europe, North America, and Australia
obesity rates have negative correlation with
percentage of trips taken by active transportations
(walking, bicycling, and public transit). Traveller’s
behavior also plays an important role, for example,
health conscious and active people may accept
longer and more intense walking paths than others.
Given that walking is a common mode of
transportation, highly susceptible to individual
differences, and beneficial for good health, a new
service that searches all feasible routes between a
given pair of origin-destination locations and
recommends one that includes walking is highly
desirable. Finding walking paths that are optimal by
taking into account multiple criteria through such a
service is challenging. Current routing services, such
as Google Maps, only consider common
transportation criteria, for example, shortest travel
time, shortest travel distance, fewest bus transfers, or
minimum walking. Furthermore, none of the
existing services takes into account individual health
conditions.
The paper contributes by presenting a novel
routing service, called Routh2Health, that
recommends walking session(s), if feasible, for any
trip. By taking origin, destination, and traveller’s
individual conditions as inputs, Route2Health
recommends a sequence of transportation modes
along with specific details about each mode that is
most optimal (personalized).
The rest of the paper is
structured as follows. Section 2 discusses related
work. Section 3 describes background information.
Section 4 describes Route2Health in detail. Section
5 describes Route2Health prototype, and summary
and future research are given in Section 6.
2 RELATED WORK
Multi-criteria routing research is focused on finding
optimal transportation paths by considering multiple
criteria (objectives) simultaneously. Bit et al. (1992)
combined fuzzy set theory and linear multi-criteria
programming to address a multi-objective
transportation problem. Their fuzzy programming
approach has been claimed to be able to address
problems with large number of objectives and to be
applicable to both minimum and maximum
optimization problems. Modesti et al. (1998)
proposed a utility measure that takes into account
the overall travel expense, travel time, and bus
crowded with passengers on public transport during
rush hour. The utility values from the measure are
then used as costs to find the optimum path using
Dijkstra's algorithm. Das et al. (1999) proposed a
solution to multi-objective transportation problems
by expressing objective functions as interval
degradation allowance values and then applying a
fuzzy programming technique. Li et al. (2000)
introduced a multi-objective linear programming
model for transit itinerary planning and used it in a
two-phase heuristic algorithm. The first phase
generates all feasible paths with the objective of
minimizing total travel time. The second phase is to
evaluate the feasible paths by taking into account
such decision criteria as number of transfer points,
bus headway or frequency, and total travel expense,
among other criteria.
Multi-modal public transport planning is another
related area. Karimi et al. (2004) developed an
Internet-based application for bus route planning
with a minimum number of bus-to-bus transfers.
Rehrl et al. (2007) designed a mobile application
that provides personalized multi-modal trip
planning, navigation assistance for transferring
between buildings, and pedestrian routes in
outdoors. Li et al. (2010) introduced a multi-modal
trip planning system that incorporated real-time
transit data into park-and-ride recommendations.
Their system uses a prediction model (based on the
regression analysis and historical data) to estimate
the real-time transit arrival time. Tsolkas et al.
(2012) described an architecture for a personalized
mobile application and a multi-modal dynamic
routing algorithm which takes into account real-time
traffic information and individual routing
preferences.
The work which is closely related to
Route2Health was conducted by Sharker et al.
(2012). The study discusses a new weight for
segments of a pedestrian network to compute health-
optimal routes. The weight, which is pre-computed
and assigned to each segment, is calculated by
taking into account physical space factors (such as
segment length and safety), environmental factors
(such as weather condition), and individual factors
(such as body mass index, walking speed, and
HEALTHINF2014-InternationalConferenceonHealthInformatics
44

calories to burn). There is currently a void in the
literature about routing services that consider
walking and health together in multi-modal
transportation.
3 BACKGROUND
3.1 Calorie Estimation
The American College of Sports Medicine (ACSM)
2
has investigated the amount of calories burned
(energy expenditure) for several activities (e.g.,
walking, running, and stepping). The result of this
investigation is an equation for walking which is
adopted for the work in this paper. The ACSM
walking equation (Tharrett et al. 2012) expresses
walking energy expenditure as:
0.1∙ 1.8∙ ∙ 3.5
∙ ∙ ∙0.005
(1)
where
EE is walking energy expenditure
(kilocalories)
S is walking speed (meters/minute)
is grade (slope) in decimal form (e.g., 0.02 for
2% grade)
BM is traveller’s body weight (kilograms)
t is walking time (minutes)
Eq. 1 is based on the assumption that the
traveller walks at a constant speed during the time t,
and the slope G is homogeneous. The equation is
only accurate for the speed between 1.9 and 3.7
miles per hour (51-99 meters per minute) (Glass et
al. 2007). To ensure slope homogeneity, a walking
path may be split into n walking segments where
each segment has homogeneous slope. This will
result in the total energy expenditure (
) for all
the walking segments as:
(2)
where
is the energy expenditure of the i
th
segment, estimated by Eq. 1. The i subscript in Eq. 2
indicates that each segment may have a different
walking speed, walking time, and slope.
3.2 Multi-criteria Optimization
Multi-criteria optimization has been used in many
areas such as economics and engineering. Multi-
criteria optimization (also known as multi-objective
optimization) is “the process of optimizing
2
http://www.acsm.org/about-acsm/
systematically and simultaneously a collection of
objective functions” (Marler and Arora 2004). The
objective functions are formulated to quantify the
solution of a decision problem based on the defined
objectives. For example, consider a decision
problem where a traveller may want an optimal
walking path such that it: (1) can help burn around
40 kilocalories, (2) has no downhill slopes greater
than 5%, (3) allows 2-2.5 miles per hour (54-67
meters per minute) walking speed, and (4) has least
walking time. Considering these preferences, there
are four objective functions in this example, one for
calories burned, one for slope calculation, one for
walking speed, and one for walking time, which are
used for path optimization. The path optimization
using the objective functions
follows the form:
min
,
,…,
(3)
is the i
th
objective function;
1,2,…,
;and 1
Eq. 3 indicates that among all path alternatives
(in the set ), the optimal path is the one which is
minimum with respect to the objective functions
to
. Note that in cases of conflicts among
some criteria, a trade-off is needed and a different
path may be chosen as optimal. Such a trade-off
among criteria can be controlled using the weighted-
sum method which allows travellers to control the
contribution of each objective function through the
weight factors. In the weighted-sum method, each
criterion is assigned a weight factor value, and the
sum of all weight factors has to be a constant
(usually 1). The larger the weight factor value, the
more contribution to the final weighted-sum value.
The optimization problem based on the weighted-
sum method can be formulated as:
min
∈
∗
(4)
where
is the set of path alternatives
is the i
th
objective function
is the weight factor for the objective
function
is the i
th
normalizing function
1,2,…,
;and 1
Eq. 4 is used to find optimal path alternatives in
which various objective functions are
homogeneously combined and normalized.
3.3 Multi-modal Transportation Model
and Routing
In general, transportation refers to a means for
Route2Health-ANovelRoutingServicetoAssistinIncreasingPhysicalActivity
45

carrying passengers or goods from one location to
another. In the context of this paper, transportation
refers to the traveling of people between locations
by vehicles or on foot. Transportation can be
classified into uni-modal, where only one mode of
transportation (e.g., walking, driving) is involved or
multi-modal, where more than one mode of
transportation (e.g., driving and walking) are
involved. Trip refers to traveling from an origin to a
destination. Trip can be uni-modal or multi-modal.
Path is a possible physical connection between
origin and destination for the purpose of traversing
by uni-modal or multi-modal transportation. There
could be multiple possible paths for a trip, and
travellers usually choose the one they consider
optimal based on one or more criteria. Finding an
optimal path requires a transportation network
which, in addition to geometry of the infrastructure,
contains topology of the transportation infrastructure
(e.g., road, bridge, tunnel, intersection, and
sidewalk).
Transportation networks are commonly modelled
as graphs of nodes and links. Each node represents a
location where travellers must make a traversing
decision (e.g., turn left/right, get on/off vehicle,
switch between modes) and a link connects two
nodes representing traversable passage (e.g., road
segment, sidewalk segment). Usually each link is
assigned a cost between its start and end nodes.
Example costs are distance, time, expense, air
pollution, and slope. Transportation networks
suitable only for one mode of transportation are uni-
modal, and a multi-modal network is formed by
combining different uni-modal networks with
designated existing or new nodes or links for
switching between them.
In this paper, a multi-modal network is formed
by combining a non-vehicular network (pedestrian
network) and a vehicular network. A pedestrian
network is a type of transportation network
involving only walking modality. A vehicular
network is a type of transportation network
associated with vehicular modalities which include,
but are not limited to, personal cars and buses.
Example vehicular networks are road networks (for
personal cars) and bus networks. The proposed
multi-modal network requires “walking transfer”
nodes that facilitate switching between the
pedestrian network and the vehicular network. An
example of how walking transfer is used is as
follows. Suppose a traveller wants to travel from
home to a meeting location in downtown by taking
three modes of transportation: driving, walking, and
riding. The traveller can drive from home to a
parking lot and then walk to a bus stop to take a bus
to the meeting location (assuming walking from the
bus stop to the meeting location is feasible). For the
driving-walking transfer, a node (
) representing a
parking lot (which can be reached by car and on
foot) is required. For the walking-riding transfer, a
node (
) representing a bus stop (which can be
reached on foot and by bus) is required. In practice,
the criteria for choosing nodes
and
are based
on traveller’s preferences. For example, suppose the
traveller wants to avoid expensive parking fee in a
downtown area and less expensive parking lots are
available just outside of that area. In this case, the
total sum of parking fee and bus fare should be less
than the parking fee in downtown. Furthermore, the
criteria for choosing the parking lot and the bus stop
may vary depending on the context. For instance, the
next day, the same traveller may want to increase
physical activity to burn some calories through a
brisk walk. For this, walking transfer nodes that
increase walking distance between the parking lot
and the bus stop (and/or between the bus stop and
the destination) are of high priority. The problem of
finding appropriate walking transfer nodes will
become more complex if the traveller, in addition to
the physical activity criterion, prefers to minimize
parking fee and bus fare. All these considerations
indicate that walking transfer plays an important role
in multi-modal trips.
4 Route2Health ARCHITECTURE
Route2Health is a service designed based on four
principles. First, it must support both uni-modal
transportation and multi-modal transportation. This
means that Route2Health recommends a multi-
modal path between a pair of origin-destination
locations only if an optimal walking path is not
feasible. Second, it must take into account individual
preferences in finding optimal paths. Third, the
objective functions must be normalized so that they
can be homogeneously combined and
simultaneously optimized. Last, it must allow
travellers to prioritize criteria to find personalized
paths. Figure 1 shows the architecture of the
Route2Health service which is composed of six
components: (1) Walking Transfer Selector, (2)
Vehicular Path Alternative Generator, (3) Walking
Path Alternative Generator, (4) Path Combiner, (5)
Objective Function Normalizer, and (6) Multi-
Criteria Optimizer. Walking Transfer Selector is the
component that takes as input origin, destination,
HEALTHINF2014-InternationalConferenceonHealthInformatics
46
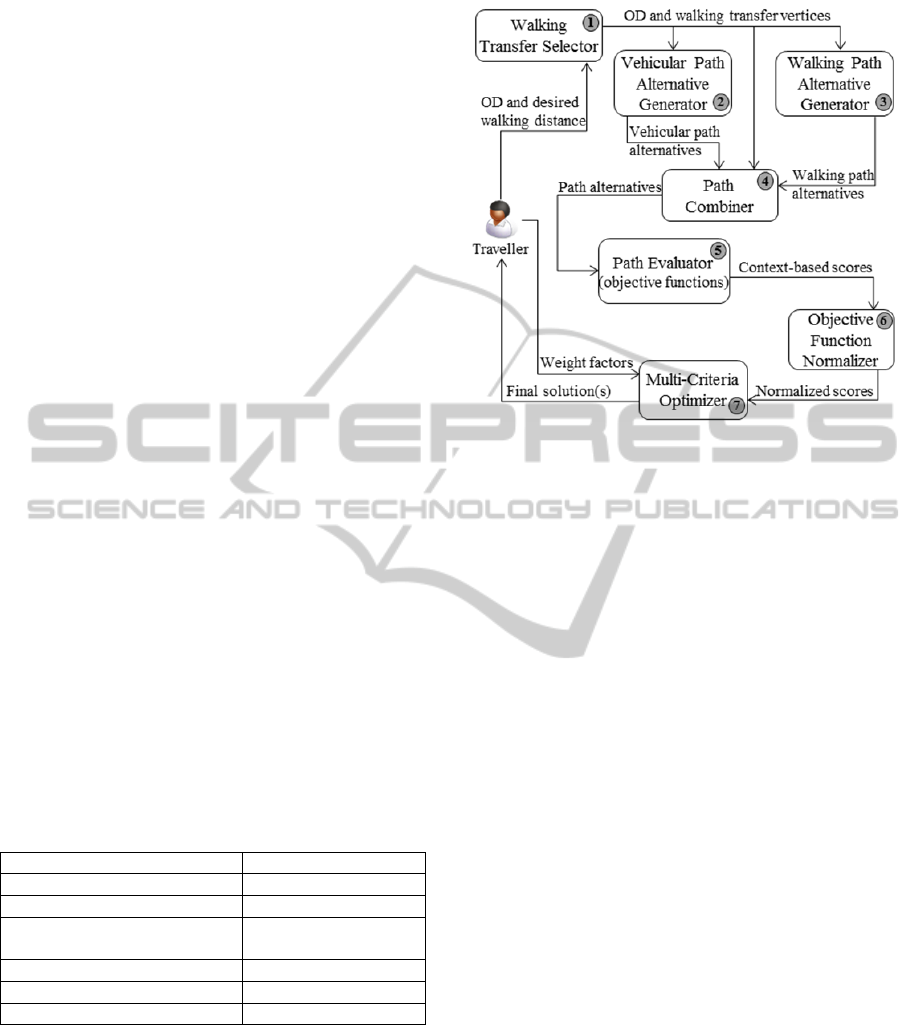
and personal walking distance limit. Based on the
inputs, Walking Transfer Selector would find all
possible feasible walking transfers. Then based on
the origin, the destination, and the identified walking
transfers, the relevant walking path alternatives and
vehicular path alternatives are computed by Walking
Path Alternative Generator and Vehicular Path
Alternative Generator, respectively. The path
alternatives of the two modes are then combined into
a complete path alternative by the Path Combiner. In
the Objective Function Normalizer, the path
alternatives are quantified using objective functions,
and the outputs from the objective functions are
normalized. The normalized values are then
optimized by the Multi-Criteria Optimizer to obtain
the final solution (optimal path).
5 Route2Health PROTOTYPE
5.1 External Data and Services
Route2Health relies on a number of external data
and services (listed in Table 1) for its computation.
Google Directions API is used to implement the
Vehicular Path Alternative Generator and Walking
Path Alternative Generator components. Google
Directions API provides up to three alternative paths
(ordered by their estimated travel time) between a
given pair of origin-destination locations. The paths
retrieved from Google Directions API are evaluated
as path alternatives. Google Elevation API is used to
retrieve elevations along the walking path to
calculate slopes of walking segments.
Table 1: External data and services used by Route2Health.
Information retrieved Services
Based map Google Maps API
Street address of a location Google Geocoding API
Parking lot and bus stop
locations
Google Places API
Driving and riding paths Google Directions API
Walking paths Google Directions API
Elevations along walking path Google Elevation API
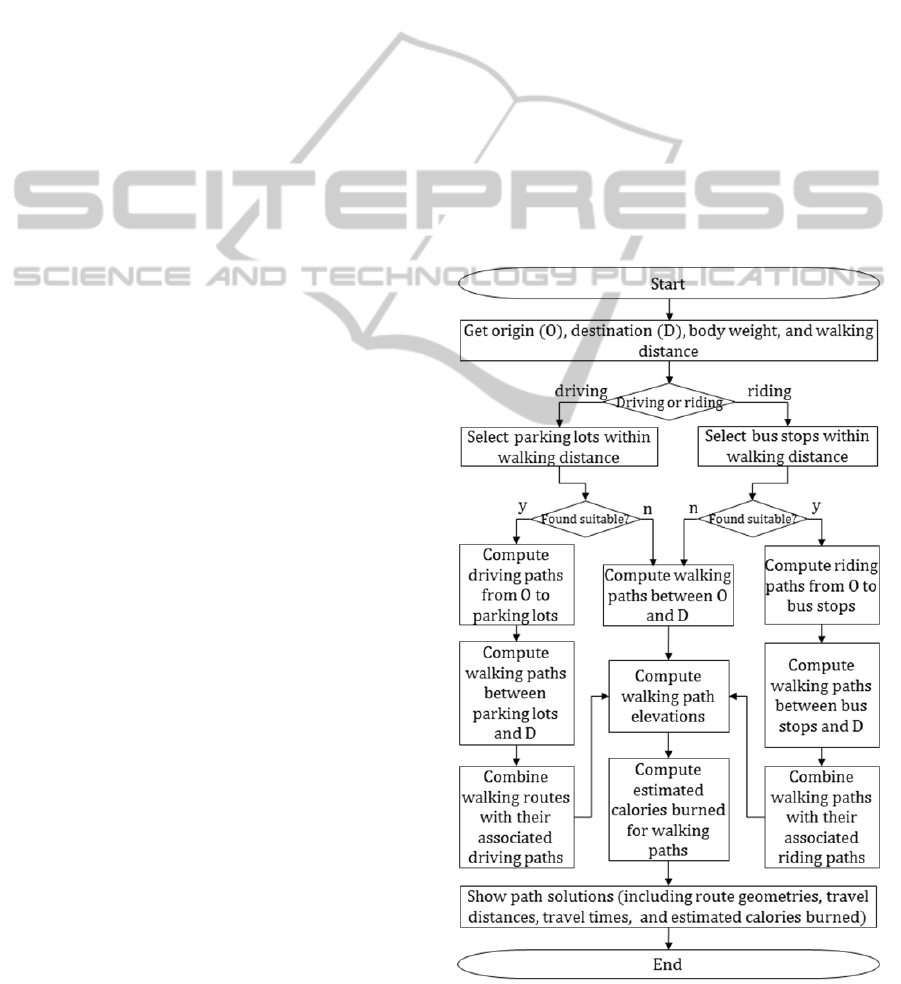
5.2 Route2Health Algorithm
The outcome of Route2Health is an optimal walking
path for each trip request, where walking is either
the only mode or one of the two modes of
transportation. An algorithm was developed to
compute optimal walking paths (see Figure 2). The
inputs to the algorithm are an origin, a destination,
Figure 1: Route2Health architecture.
body weight, walking distance, and the desired mode
of vehicular transportation (driving or riding).
Walking transfer nodes, located within an acceptable
walking distance, are retrieved and used for
vehicular and walking path computation. In the
absence of walking transfer nodes that satisfy the
requested walking distance, the algorithm computes
only feasible walking paths that connect the origin
and the destination. If walking transfer nodes
(parking lots or bus stops) are found, the associated
vehicular paths (driving or riding) are computed.
Once vehicular and walking paths are computed,
the results (walking paths and vehicular paths) are
combined to form a multi-modal path linking the
origin, walking transfer nodes, and the destination.
The number of walking transfer nodes determines
the number of walking path alternatives. Once all
walking path alternatives are identified, based on Eq.
1, the calorie burns for each walking path alternative
is estimated. Slope of each segment of a walking
path is estimated by using high-resolution Digital
Elevation Model (DEM) data. Walking speed is
provided by the traveller, or could be calculated
based on walking path distance and estimated
duration of walking. For each optimal path, path
geometry, travel distance, travel time, and estimated
calories burned are presented to the traveller.
5.3 Route2Health Application
A web-based prototype application was developed to
demonstrate the Route2Health concept. The
application’s interface features two panels (Figure
Route2Health-ANovelRoutingServicetoAssistinIncreasingPhysicalActivity
47
3), map panel (the left panel) and parameter
inputting panel (the right panel). Through the
parameter inputting panel, the traveller specifies
profile and preferences including body weight,
walking speed, walking distance limit (round trip),
and preferred transportation modes (i.e., driving-
walking or riding-walking). In the current version of
the prototype, walking close to destination is
implemented. This means that driving-walking
involves driving from origin to a parking lot then
walking to the destination, and riding-walking
involves riding (bus) from origin to a bus stop then
walking to the destination. If the traveller does not
specify walking speed, the application will calculate
the speed based on the walking path distance and
duration retrieved from Google Directions Service.
Based on the requested walking distance limit, either
parking lots or bus stops (depending on the preferred
mode within a walking distance limit) will be
identified and used for path alternatives
computation. Once all parameters are included, path
alternatives (up to 20 in the current version of the
prototype) are computed and listed. For each path
alternative, a link to detailed information, such as
travel distance, travel duration, and estimated
calories burned, is provided. By clicking on the link,
the detailed information will appear in the table in
the results section and the associated path is
displayed in the map panel.
Figure 4 shows two optimal driving-walking
paths (P1 and P2) and Figure 5 shows two riding-
walking paths (P3 and P4) between origin (A) and
destination (B). The travel distance, travel duration,
and estimated calories burned for each path are
summarized in Table 2. In these examples, the round
trip walking distance limit is set to 3.0 miles (around
1.5 miles each way). For driving-walking, P2
contains a better one-way walking distance than P1
(1.45 miles versus 1.14 miles) and requires only one
minute longer than P1 (44.6 minutes versus 45.5
minutes) to travel. For riding-walking, P3 and P4
require almost the same total travel time (75.0
minutes and 75.8 minutes), but P3 can help burn 170
kilocalories for 1.58 miles walking distance which is
much better than P4 which helps burn 111
kilocalories for 1.09 miles.
Another scenario is when the origin and
destination are close to each other. Figure 6 shows
traveller’s request for a riding-walking path (with
walking distance limit set at 3.0 miles), but since
Route2Health finds that the walking path is only 1.2
miles long, the walking path is recommended
instead of a riding-walking path.
In case of a destination located within a
downtown area (which usually has high road
density and large number of parking lots), the
number of driving-walking path alternatives will be
large. However, in a hilly area, like downtown in
Pittsburgh, the computed path alternatives are not
very different. In Figure 7, there are 16 parking lots
suggested by Route2Health, but the walking paths
from the 16 parking lots merge into only three paths
close to the destination which is located in
downtown Pittsburgh. The reason for this may be
alluded to the fact that the walking paths, computed
by Google Directions Service, are chosen based on
their flatness. The background terrain map in Figure
7 shows least variation in elevation on the paths in
the north-east direction. The flat walking paths seem
to be reasonable in general, but, as discussed in the
previous section, some people may prefer more
challenging (hilly) paths than flat paths. The
example also confirms the claim that the existing
routing services do not fully support the concept of
Route2Health.
Figure 2: Route2Health algorithm.
HEALTHINF2014-InternationalConferenceonHealthInformatics
48
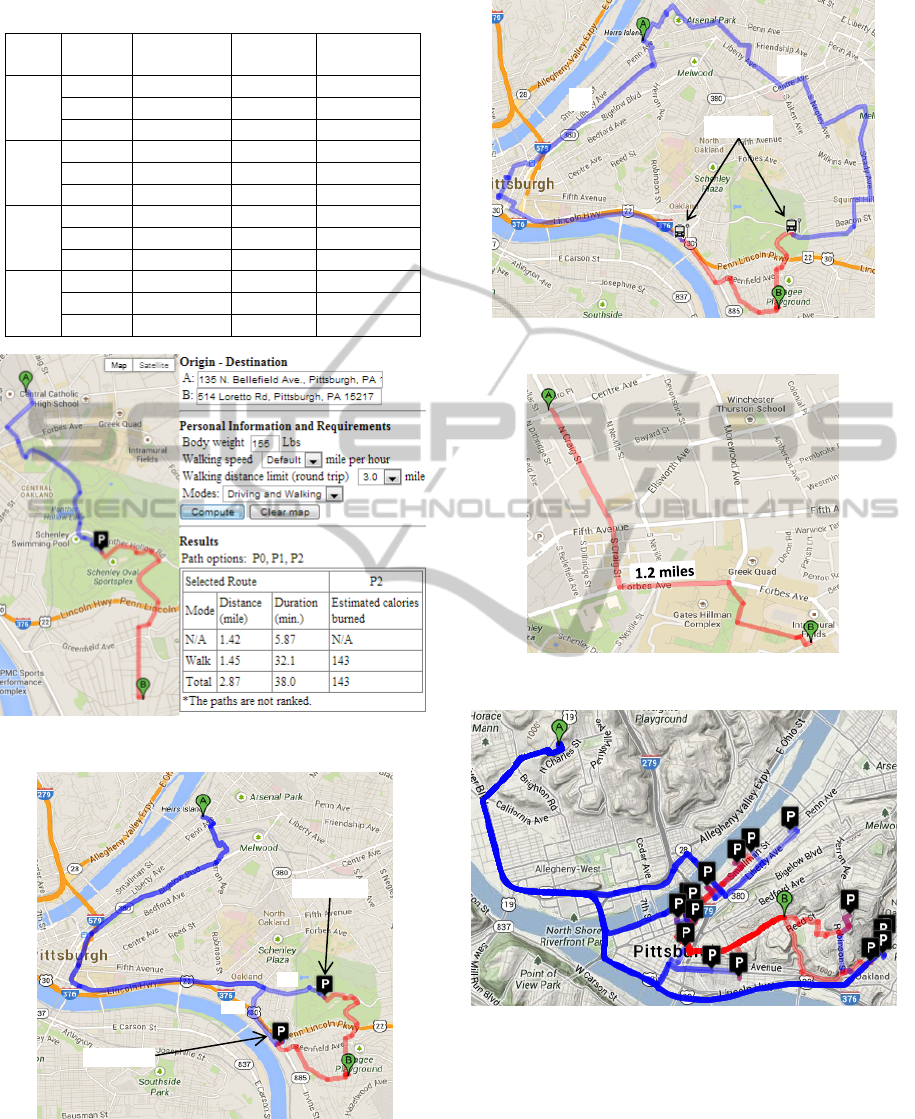
Table 2: Path alternatives summary.
Path Mode
Distance
(miles)
Duration
(minutes)
Calories
(kilocalories)
P1
Drive 5.90 15.2 N/A
Walk 1.14 29.4 131
Total 7.04 44.6 131
P2
Drive 5.73 13.4 N/A
Walk 1.45 32.1 143
Total 7.18 45.5 143
P3
Ride 5.19 36.9 N/A
Walk 1.58 38.1 170
Total 6.77 75.0 170
P4
Ride 5.97 50.9 N/A
Walk 1.09 24.9 111
Total 7.06 75.8 111
Figure 3: Route2Health user interface.
Figure 4: Driving-walking paths from A to B.
For driving-walking, when the destination is
close to an area with a large number of parking lots
(such as a downtown area), the parking lots selected
Figure 5: Riding-walking paths from A to B.
Figure 6: Walking path for destination close to origin.
Figure 7: Multiple parking lots in Pittsburgh downtown
area.
by Walking Transfer Selector may spatially cluster
together within the area. Figure 8 (upper map) shows
an example of the aforementioned scenario. One
problem with clustered parking lots is the possibility
of impractical path alternatives. In Figure 8 (lower
map), the parking lots cluster on one side of the
river, while the origin and destination are both
P1
P2
Parkinglot
Parkinglot
Busstop
P3
P4
Route2Health-ANovelRoutingServicetoAssistinIncreasingPhysicalActivity
49

Figure 8: Parking lots cluster in downtown area.
Figure 9: Cluster of selected bus stops along roads.
located on the other side. This means that regardless
of the paths the traveller chooses, the river must be
crossed by car, the car must be parked on the other
side of the river, and the river must be crossed on
foot to the destination. Similar situations may occur
with bus stops. In Figure 9, as the area of interest has
a large number of bus stops, most of the candidate
bus stops linearly cluster just right next to each other
on the same road. From traveller’s perspective, the
linear sequence of bus stops is representing the same
riding path. The two examples (Figure 8 and Figure
9) support the claim (discussed in the previous
section) that walking transfer plays an important role
in multi-modal transportation trip planning.
6 SUMMARY AND FUTURE
WORK
Route2Health, as a new approach helping increase
physical activity by considering walking always as
one mode in multi-modal transportation trip
planning, is presented. The algorithms for
computing a walking session for each trip along with
the components of the Route2Health service are
discussed. A prototype Route2Health was developed
and sample scenarios were described.
Two directions for future research are evaluation
and deployment of Rout2Health. Evaluation could
be based on pre- and post-testing analysis to
determine the level of physical activity (indicated by
the number of trips with walking sessions) before
and after using Rour2Health. Deployment of
Route2Health as a web application accessible
through both desktop platforms and mobile devices
is considered. The application will be used for both
trip planning and real-time navigation. With position
and speed obtained through GPS sensors embedded
in smart phones, a progress report on position,
speed, time, distance, and calories can be provided
to the traveller in real time and more accurately.
Trips, once completed, along with relevant
parameters, can be stored for performance
assessment of walking over time. The mobile
version can also be integrated with existing physical
activity monitoring devices such as BodyMedia
3
,
FitBit
4
, Nike+FuelBand
5
, and Jawbone
6
. These
devices are wearable sensors that help monitoring
physical activities such as walking, running,
sleeping, and energy expenditures. Data from such
sensors can provide more accurate walking speed
and energy expenditures to Route2Health.
REFERENCES
Bassett Jr, D. R., Pucher, J., Buehler, R., Thompson, D. L.,
& Crouter, S. E., 2008. Walking, cycling, and obesity
rates in Europe, North America, and Australia. J Phys
Act Health, 5(6), 795-814.
3
http://www.bodymedia.com/explore.html
4
http://www.fitbit.com/
5
http://nikeplus.nike.com/plus/what_is_fuel/
6
https://jawbone.com/
HEALTHINF2014-InternationalConferenceonHealthInformatics
50

Besser, L. M., Dannenberg, A. L., 2005. Walking to
Public Transit Steps to Help Meet Physical Activity
Recommendations. American Journal of Preventive
Medicine, 29 (4). 273-280.
Bit, A. K., Biswal, M. P., & Alam, S. S., 1992. Fuzzy
programming approach to multicriteria decision
making transportation problem. Fuzzy sets and
systems, 50(2), 135-141.
Edwards, R. D. (2008). Public transit, obesity, and medical
costs: assessing the magnitudes. Preventive Medicine,
46(1), 14-21.
Das, S. K., Goswami, A., & Alam, S. S. (1999).
Multiobjective transportation problem with interval
cost, source and destination parameters. European
Journal of Operational Research, 117(1), 100-112.
Glass, S., & Dwyer, G. B. (Eds.). (2007). ACSM's
Metabolic Calculations Handbook. Lippincott
Williams & Wilkins, 19 & 26.
Himann, J. E., Cunningham, D. A., Rechnitzer, P. A., &
Paterson, D. H., 1988. Age-related changes in speed of
walking. Med Sci Sports Exerc, 20(2), 161-166.
Karimi, H. A., Peachavanish, R. and Peng, J., 2004.
Finding Optimal Bus Service Routes: An Internet-
Based Methodology to Serve the Transit Patrons.
ASCE Journal of Computing in Civil Engineering.
18(2), 83-91.
Li, Q., & Kurt, C. E., 2000. GIS-based itinerary planning
system for multimodal and fixed-route transit network.
In Proceedings of the MID-Continent Transportation
Symposium, 47-50.
Li, J. Q., Zhou, K., Zhang, L., & Zhang, W. B., 2010. A
multimodal trip planning system incorporating the
park-and-ride mode and real-time traffic/transit
information. In Proceedings of the 17
th
ITS World
Congress.
MacDonald, J. M., Stokes, R. J., Cohen, D. A., Kofner, A.,
& Ridgeway, G. K., 2010. The effect of light rail
transit on body mass index and physical activity.
American journal of preventive medicine, 39(2), 105-
112.
Marler, R. T., & Arora, J. S., 2004. Survey of multi-
objective optimization methods for engineering.
Structural and multidisciplinary optimization, 26(6),
369-395.
Modesti, P., & Sciomachen, A., 1998. A utility measure
for finding multiobjective shortest paths in urban
multimodal transportation networks. European
Journal of Operational Research, 111(3), 495-508.
Morabia, A., Mirer, F. E., Amstislavski, T. M., Eisl, H.
M., Werbe-Fuentes, J., Gorczynski, J., & Markowitz,
S. B., 2010. Potential health impact of switching from
car to public transportation when commuting to work.
Journal Information, 100(12).
Pucher, J., Buehler, R., Bassett, D. R., & Dannenberg, A.
L., 2010. Walking and cycling to health: a
comparative analysis of city, state, and international
data. American Journal of Public Health, 100(10),
1986-1992.
Rehrl, K., Bruntsch, S., & Mentz, H. J., 2007. Assisting
multimodal travelers: Design and prototypical
implementation of a personal travel
companion.Intelligent Transportation Systems, IEEE
Transactions on, 8(1), 31-42.
Sallis, J. F., Frank, L. D., Saelens, B. E., & Kraft, M. K.,
2004. Active transportation and physical activity:
opportunities for collaboration on transportation and
public health research. Transportation Research Part
A: Policy and Practice, 38(4), 249-268.
Sharker, M., Karimi, H. and Zgibor, J., 2012. Health-
Optimal Routing In Pedestrian Navigation Services.
ACM SIGSPATIAL HealthGIS'12. Redondo Beach,
CA, 1-10, ACM.
Tsolkas, D., Passas, N., Xenakis, C., Papataxiarhis, V., &
Tsetsos, V., 2012. Busfinder: a personalized
multimodal transportation guide with dynamic routing.
In Informatics (PCI), 2012 16
th
.Panhellenic
Conference on, 25-30, IEEE.
Tharrett, S. J., & Peterson, J. A. (Eds.), 2012. ACSM's
health/fitness facility standards and guidelines.
Human Kinetics.
U.S. Department of Health and Human Services, 1996.
Physical Activity and Health: A Report of the Surgeon
General. Atlanta, GA: U.S. Department of Health and
Human Services, Centers for Disease Control and
Prevention, National Center for Chronic Disease
Prevention and Health Promotion.
Route2Health-ANovelRoutingServicetoAssistinIncreasingPhysicalActivity
51
