
Laser Speckle Contrast Images
Processing of Data to Analyze Microvascular Variations in Hand Skin of Healthy
Subjects
Anne Humeau-Heurtier
1
, J´er´emy Dexet
1
, Pierre Abraham
2
and Guillaume Mah´e
3
1
Universit´e d’Angers, LARIS - Laboratoire Angevin de Recherche en Ing´enierie des Syst`emes,
62 avenue Notre Dame du Lac, 49000 Angers, France
2
Universit´e d’Angers, CHU d’Angers, Laboratoire de Physiologie et d’Explorations Vasculaires,
UMR CNRS 6214-INSERM 1083, 49033 Angers cedex 01, France
3
Pˆole imagerie m´edicale et explorations fonctionnelles, CHU de Rennes, Universit´e de Rennes 1,
Hˆopital Pontchaillou, 35033 Rennes Cedex 9, France
Keywords:
Laser Speckle Contrast Imaging, Microvascular Blood Flow, Spatial Variation, Hand.
Abstract:
Diseases such as frostbite, Raynaud’s phenomenon, carpal tunnel syndrome, systemic sclerosis, hand burns,
hand flaps or hand wounds lead to microvascular dysfunctions. These diseases can affect only one hand
and even sometimes only some fingers. Therefore, in order to quantify the microvascular alterations, it can
be useful to compare microvascular perfusion of both hands (altered versus healthy hand). However, skin
microvasculature presents spatial variations and the possibility to directly compare perfusion values of the two
hands has not been studied yet. We therefore propose to quantify these spatial variations. For this purpose,
perfusion values from laser speckle contrast images (LSCI) of the two hands (dorsal faces) from seven young
healthy subjects are acquired simultaneously and then processed. The results show that the dorsal faces of
the two hands in our young healthy subjects present close perfusion values (average coefficient of variation
less than 9% for our subjects). These findings are preliminary observations to quantify the microvascular
alterations in the above-mentioned diseases. The coefficient of variation in diseased states remains to be
studied in order to see whether LSCI could be of interest to improve the diagnosis of hand skin pathologies.
1 INTRODUCTION
Microvascular dysfunction in hands is an early
stage in several pathologies. Thus, for diseases
such as frostbite (Foray, 1992), Raynaud’s phe-
nomenon (Brown, 2012; Gladue et al., 2013), carpal
tunnel syndrome (Shannon and Rizzolo, 2012), sys-
temic sclerosis (Wigley, 2009; Herrick, 2000), hand
burns (Meier et al., 2011; Barachini et al., 2004), hand
flaps (Du et al., 2011; Soderstrom et al., 1999) or hand
wounds, hand skin microvasculatureis specifically af-
fected: morphological abnormalities of the capillaries
(enlarged loops, giant capillaries, ramifications, cap-
illary disorganization), microhemorrhages or lower
density (capillary loss) (DeAngelis et al., 2009). Al-
tered hand skin microvascular function could there-
fore be a surrogate marker for the above-mentioned
diseases. In order to quantify such vascular dysfunc-
tions, accurate and sensitive measurement techniques
have become a key issue.
Recently, the laser speckle contrast imag-
ing (LSCI) technique has been proposed for skin mi-
crocirculation monitoring (Humeau-Heurtier et al.,
2013a; Rege et al., 2012; Mahe et al., 2012b; Mahe
et al., 2012c; Miao et al., 2010; Draijer et al., 2009).
LSCI gives a 2D map of the microvascular blood
perfusion (see an example in Fig. 1). The princi-
ples of LSCI rely on the illumination of tissues (op-
tically rough surface) by a laser light. Raw speckle
reflectance images are collected with a CCD cam-
era. Motions (e.g., blood flow) in the tissues alter the
speckle pattern over time. A faster blood flow leads
to more blurring in the captured image than slower
flow or no flow. The degree of blurring is quanti-
fied as the local speckle contrast value, with zero con-
trast (no speckle pattern) corresponding to high blood
flow, and unity contrast (fully developed speckle pat-
tern) to no flow. The speckle contrast K is defined as
the ratio of the standard deviation to the mean inten-
sity hIi, as (Briers and Webster, 1996)
K =
σ
s
hIi
, (1)
55
Humeau-Heurtier A., Dexet J., Abraham P. and Mahé G..
Laser Speckle Contrast Images - Processing of Data to Analyze Microvascular Variations in Hand Skin of Healthy Subjects.
DOI: 10.5220/0004892900550058
In Proceedings of the International Conference on Bioimaging (BIOIMAGING-2014), pages 55-58
ISBN: 978-989-758-014-7
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
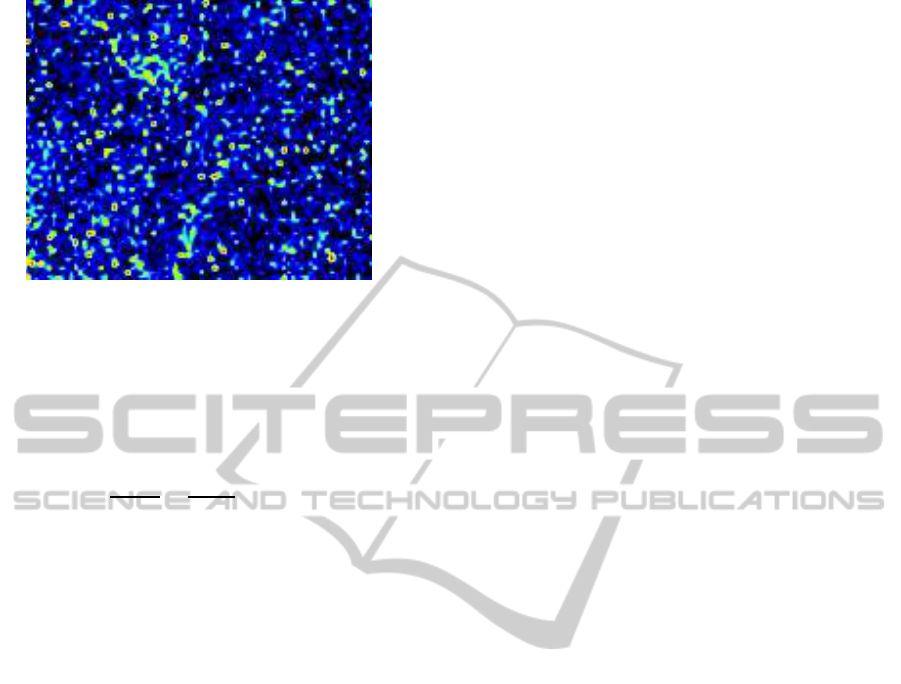
Figure 1: Laser speckle contrast image of a zone on the
dorsal face of the hand from a healthy subject.
where σ
s
refers to the spatial standard deviation of the
speckle intensity. The speckle contrast K is a function
of the exposure time T of the camera and is related to
the autocovariance of the intensity fluctuations in a
single speckle (Fercher and Briers, 1981)
K
2
=
σ
2
s
(T)
hIi
2
=
1
ThIi
2
Z
T
0
C
t
(τ)dτ, (2)
whereC
t
(τ) is the autocovarianceof the intensity fluc-
tuations in a single speckle. The contrast value is
used to form the microvascular blood perfusion im-
age (Draijer et al., 2009).
In diseases such as frostbite, Raynaud’s phe-
nomenon, carpal tunnel syndrome, systemic sclero-
sis, burns, flaps and wounds, skin microvascular al-
terations and vascular dysfunctions may affect only
one hand (the diseased one). In order to quantify such
alterations and dysfunctions, it can be useful to com-
pare skin perfusion values of the diseased hand to skin
perfusion values of the healthy hand. However, due
to spatial variations of perfusion in skin, the question
relative to the possibility to directly compare LSCI
perfusion values of the two hands still has to be an-
swered. Thus, in the case of no disease, are perfusion
values of both hands similar? Are there variations
from one hand to the other? If yes, is it possible to
quantify them?
In order to quantify spatial variations between the
perfusion values of two hands from healthy subjects,
we herein propose to process laser speckle contrast
images acquired simultaneously in the two hands of
voluntary subjects.
2 MATERIALS AND METHODS
2.1 Measurement Procedure
Seven Caucasian healthy subjects participated in the
study (six men, one woman; 22.6 ±5 years old). All
the subjects provided written, informed consent prior
to participation and the study was carried out in accor-
dance with the Declaration of Helsinki. Each subject
was sitted confortably in a quiet room with controlled
temperature and without any air movements (Mahe
et al., 2012a). They were asked to position the ventral
face of each hand on a table. LSCI data of both hands
were acquired in laser speckle perfusion units (LSPU)
with a PeriCam PSI System (Perimed, Sweden) hav-
ing a laser wavelength of 785 nm and an exposure
time of 6 ms. The distance between the laser head to
skin was set around 24 cm (Mahe et al., 2011), which
gave an average image resolution of 0.6 mm. Laser
speckle contrast images were acquired and stored for
5 min with a sampling frequency of 18 Hz on a com-
puter and analyzed off-line.
2.2 Image Processing Procedure
After the acquisitions, five pixels on each hand were
randomly chosen on the first image of the LSCI se-
quence. These pixels are thereafter noted as P
i
, with i
varying between 1 and 5. Then, for each pixel P
i
, the
amplitude value was followed with time on the image
sequence (5 min) to obtain a time-evolution signal,
noted thereafter as sP
i
(t). Around each of these five
pixels P
i
, five square regions of interest (ROI), each
of different size, were also determined: 3.2 mm
2
(3
pixels×3 pixels), 29.1 mm
2
(9 pixels×9 pixels),
81.0 mm
2
(15 pixels×15 pixels), 190.4 mm
2
(23
pixels×23 pixels), 345.9 mm
2
(31 pixels×31 pix-
els) (see (Humeau-Heurtier et al., 2013b)). Pixel val-
ues inside each ROI were averaged and followed with
time on the image sequence (5 min) to obtain time-
evolution signals, noted thereafter as sROI
j
P
i
(t) for
the ROI j around the pixel P
i
, j corresponding to the
size of the square value (3, 9, 15, 23, or 31). Then, for
each hand, the five time-evolution signals sP
i
(t) were
averaged in time to obtain five LSCI perfusion val-
ues which were averaged together. The same was per-
formed for the five time-evolution signals sROI
j
P
i
(t).
For each hand and for each of the seven subjects,
we therefore had one LSCI perfusion value corre-
sponding to the five pixels and one LSCI perfusion
value corresponding to each of the five ROI sizes (see
Fig. 2).
The coefficient of variation (CV) was computed
to compare the LSCI perfusion values between each
hand. The CV was calculated according to the proce-
dure proposed by Hopkins (Hopkins, 2000). For this
purpose, the perfusion value from the five pixels P
i
of
one hand was compared to the perfusion value from
the five pixels P
i
of the other hand. The same was
BIOIMAGING2014-InternationalConferenceonBioimaging
56
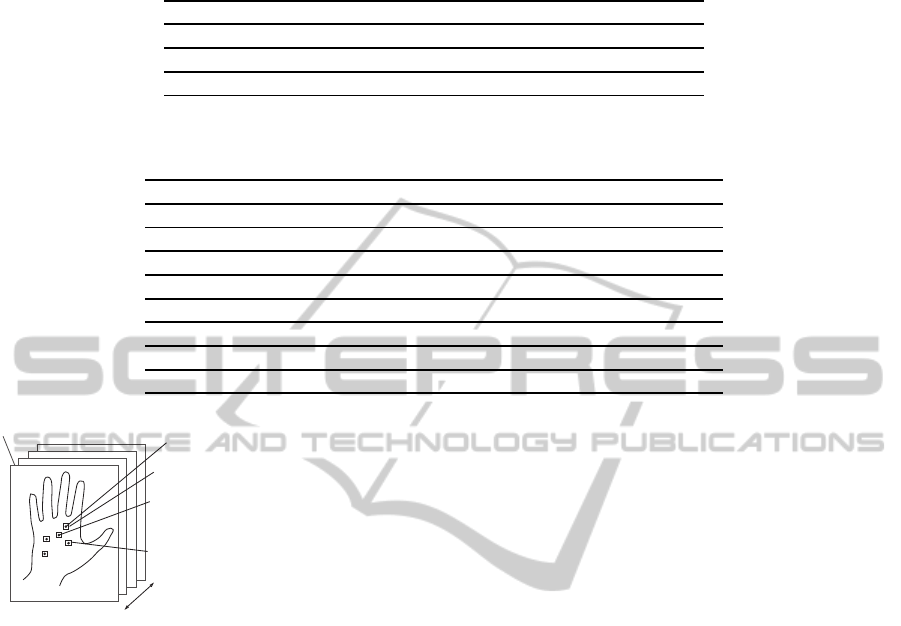
Table 1: Average perfusion values in LSPU for the 7 subjects for each ROI size and for the two hands. ROI sizes are in pixels
× pixels (see text for details).
Size of ROI Pixel 3×3 9×9 15×15 23×23 31×31
Left hand 65.0 64.6 64.0 63.8 64.3 65.9
Right hand 67.6 67.4 67.1 67.5 67.8 69.1
Average 66.3 66.0 65.6 65.6 66.1 67.5
Table 2: Coefficient of variation (CV, in percentage) between the perfusion values of the two hands of healthy subjects. ROI
sizes are in pixels × pixels (see text for details).
Size of ROI Pixel 3×3 9×9 15×15 23×23 31×31
CV for subject 1 7.9 8.2 6.9 7.1 7.2 7.9
CV for subject 2 6.7 5.4 4.0 6.7 6.8 5.0
CV for subject 3 10.3 10.3 6.7 3.9 2.4 2.2
CV for subject 4 5.9 5.1 5.8 5.1 5.4 6.6
CV for subject 5 8.2 8.4 8.8 7.1 4.6 3.8
CV for subject 6 5.4 5.2 3.5 3.9 4.1 5.1
CV for subject 7 16.2 16.2 11.4 10.1 10.1 9.7
Average CV 8.7 8.4 6.7 6.3 5.8 5.8
pixel P
i
(1 ≤ i ≤ 5)
ROI around P
i
sP
i
(t)
g
averaging in time
g
one perfusion
value for each pixel P
i
sROI
j
P
i
(t)
g
averaging in time
g
one perfusion
value for each ROI size and for
each pixel P
i
5 min
laser speckle contrast image
Figure 2: Schematic representation of the signals processed.
Only one hand is represented here. On our recordings, the
two hands were present on each image.
performed for each ROI size.
3 RESULTS AND DISCUSSION
The results obtained for the analysis of the spatial
variations are shown in Tables 1 and 2. From Ta-
ble 1 we observe that the average perfusion value is
66.1 LSPU when the two hands are considered to-
gether (average perfusion value between 65.6 LSPU
and 67.5 LSPU). When the two hands are considered
separately, we observe that the average perfusion val-
ues are verysimilar for both hands butthat the average
perfusion value is slightly higher for the right hand
than for the left hand, whatever the ROI size (see Ta-
ble 1). In that case, the standard deviation varies from
11.5 LSPU and 15.4 LSPU. The slightly higher value
for the perfusion in the right hand compared to the
one of the left hand may be due to the fact that all
our subjects were right-hander. To analyze these re-
sults, we computed the standard deviation of the per-
fusion values obtained on a white surface (same mea-
surement procedure as for the hands). For the same
ROI sizes as for the hands, we obtain standard devia-
tion values of the difference between the points in the
white surface between 0.7 LSPU and 4.3 LSPU (0.7
LSPU for a ROI of 31×31 pixels and 4.3 LSPU for a
ROI of the size of the pixel). For the white surface,
the standard deviation decreases for larger ROI sizes
since we have less noise in the perfusion values when
more data points are used for the analysis. These stan-
dard deviations on the white surface are much lower
than the ones found for the hands.
Moreover, from Table 2 we note that the CV be-
tween the perfusion values of the two hands varies be-
tween subjects but is always lower than 16.2% for a
ROI of the size of a pixel for a subject, and lower than
9.7% for a ROI size of 31 pixels×31 pixels for a sub-
ject. The average CV for the 7 subjects is low (< 9%)
for each size of ROI analyzed (see Table 2). Further-
more, the larger the ROI size (between 3.2 mm
2
and
345.9 mm
2
), the lower the average CV value.
All these results show that, despite the spatial
variations in skin microcirculation, the dorsal face of
the two hands in healthy subjects present close per-
fusion values (average CV < 9%). These findings
lead to the suggestion that, for patients with diseases
affecting one hand (e.g., frostbite, Raynaud’s phe-
nomenon, carpal tunnel syndrome, systemic sclero-
sis, hand burns, hand flaps or hand wounds), it may
be possible to quantify skin microvascular alterations
and vascular dysfunctions by comparing laser speckle
contrast images perfusion of the two hands.
LaserSpeckleContrastImages-ProcessingofDatatoAnalyzeMicrovascularVariationsinHandSkinofHealthy
Subjects
57

4 CONCLUSIONS
Spatial variations in perfusion values from the two
hands of healthy subjects are herein studied from laser
speckle contrast images. We show that the dorsal face
of the two hands in healthy subjects present close
perfusion values (CV < 9.7% for a ROI size of 31
pixels×31 pixels). The possible increase of CV in
diseased states remains to be studied in order to see
whether LSCI could be of interest to improve the di-
agnosis of diseases such as frostbite, Raynaud’s phe-
nomenon, carpal tunnel syndrome, systemic sclerosis,
hand burns, hand flaps or hand wounds.
ACKNOWLEDGEMENTS
The authors would like to thank Fredrik Salomonsson
from Perimed for its useful comments regarding the
analysis of the data on white surface.
REFERENCES
Barachini, P., Vezzoni, G. M., Palombo, C., Franzoni, F.,
and Bigalli, G. (2004). Skin blood flow pattern in
burns outcomes. Burns, 30:312–316.
Briers, J. D. and Webster, S. (1996). Laser speckle contrast
analysis (lasca): a non- scanning, full-field technique
for monitoring capillary blood flow. J. Biomed. Opt.,
1:174–179.
Brown, S. (2012). Diagnosis and management of patients
with raynaud’s phenomenon. Nurs. Stand., 26:41–46.
DeAngelis, R., Grassi, W., and M.Cutolo (2009). A grow-
ing need for capillaroscopy in rheumatology. Arthritis
Rheum., 61:405–410.
Draijer, M., Hondebrink, E., van Leeuwen, T., and Steen-
bergen, W. (2009). Review of laser speckle contrast
techniques for visualizing tissue perfusion. Lasers
Med. Sci., 24:639–651.
Du, Z., Zan, T., Li, H., and Li, Q. (2011). A study of blood
flow dynamics in flap delay using the full-field laser
perfusion imager. Microvasc. Res., 82:284–290.
Fercher, A. F. and Briers, J. D. (1981). Flow visualiza-
tion by means of single-exposure speckle photogra-
phy. Opt. Commun., 37:326–330.
Foray, J. (1992). Mountain frostbite. current trends in prog-
nosis and treatment (from results concerning 1261
cases). Int. J. Sports Med., 13:S193–S196.
Gladue, H., Maranian, P., Paulus, H. E., and Khanna, D.
(2013). Evaluation of test characteristics for outcome
measures used in raynaud’s phenomenon clinical tri-
als. Arthritis Care Res (Hoboken), 65:630–636.
Herrick, A. L. (2000). Vascular function in systemic scle-
rosis. Curr. Opin. Rheumatol., 12:527–533.
Hopkins, W. G. (2000). Measures of reliability in sports
medicine and science. Sports Medicine, 30:1–15.
Humeau-Heurtier, A., Guerreschi, E., Abraham, P., and
Mahe, G. (2013a). Relevance of laser doppler and
laser speckle techniques for assessing vascular func-
tion: state of the art and future trends. IEEE Trans.
Biomed. Eng., 60:659–666.
Humeau-Heurtier, A., Mahe, G., Durand, S., and Abraham,
P. (2013b). Multiscale entropy study of medical laser
speckle contrast images. IEEE Trans. Biomed. Eng.,
60:872–879.
Mahe, G., Durand, S., Humeau, A., Leftheriotis, G.,
Rousseau, P., and Abraham, P. (2012a). Air move-
ments interfere with laser speckle contrast imaging
recordings. Lasers Med. Sci., 27:1073–1076.
Mahe, G., Haj-Yassin, F., Rousseau, P., Humeau, A., Du-
rand, S., Leftheriotis, G., and Abraham, P. (2011).
Distance between laser head and skin does not influ-
ence skin blood flow values recorded by laser speckle
imaging. Microvasc. Res., 82:439–442.
Mahe, G., Humeau-Heurtier, A., Durand, S., Leftheriotis,
G., and Abraham, P. (2012b). Assessment of skin
microvascular function and dysfunction with laser
speckle contrast imaging. Circulation: Cardiovasc.
Imaging, 5:155–163.
Mahe, G., Humeau-Heurtier, A., Durand, S., Leftheriotis,
G., and Abraham, P. (2012c). Impact of experimen-
tal conditions on non-contact laser recordings in mi-
crovascular studies. Microcirc., 19:669–675.
Meier, T. O., Guggenheim, M., Vetter, S. T., Husmann, M.,
Haile, S. R., and Amann-Vesti, B. R. (2011). Mi-
crovascular regeneration in meshed skin transplants
after severe burns. Burns, 37:1010–1014.
Miao, P., Rege, A., Li, N., Thakor, N. V., and Tong, S.
(2010). High resolution cerebral blood flow imag-
ing by registered laser speckle contrast analysis. IEEE
Trans. Biomed. Eng., 57:1152–1157.
Rege, A., Senarathna, J., Li, N., and Thakor, N. V.
(2012). Anisotropic processing of laser speckle im-
ages improves spatiotemporal resolution. IEEE Trans.
Biomed. Eng., 59:1272–1280.
Shannon, H. and Rizzolo, D. (2012). Carpal tunnel syn-
drome: symptoms, diagnosis, and treatment options.
JAAPA, 25:22–26.
Soderstrom, T., Svensson, H., Koop, T., and Moller, K. O.
(1999). Processing of laser-doppler signals from free
flaps. Technol. Health Care, 7:219–223.
Wigley, F. M. (2009). Vascular disease in scleroderma. Clin.
Rev. Allergy Immunol., 36:150–175.
BIOIMAGING2014-InternationalConferenceonBioimaging
58
