
CarolApp
A Mobile e-Health Software Project for Remote Monitoring of Children enrolled in
the Carolina Curriculum
Salvatore Cuomo
1
, Pasquale De Michele
1
, Francesco Piccialli
1
, Antonella Olivo
2
and Ennio Del Giudice
2
1
University of Naples “Federico II”, Department of Mathematics and Applications ”Renato Caccioppoli”, Naples, Italy
2
Fondazione Istituto Antoniano, Ercolano, Naples, Italy
3
University of Naples “Federico II”, Faculty of Medicine, Via Pansini, Naples, Italy
Keywords:
Mobile Technologies, Healthcare Applications, Health Care Management, Health Information Systems.
Abstract:
The Carolina Curriculum for Infants and Toddlers with Special Needs (CCITSN) is a well established assess-
ment curriculum-based for early intervention programs, where sequenced items data collection and analysis
allow for monitoring, incremental program change, and recognition of areas of relative strength and weakness
in children with mild, moderate, or severe disabilities. Unfortunately, this protocol, and the support developed
software C@rolin@, is concerned only with the medical aspects, which are basically recorded with a huge gap
of time intervals. Moreover, due to lack of funding in local health care facilities, the medical staff is not able to
care adequately the involved children that, as provided by this program, must perform most of the assessment
activities in their own homes, supported by parents that often are left alone during the period between two
medical visit. In order to reduce the gap between families and medical staff, this paper describes the design
and development of CarolApp, a mobile framework that allows, from one side, parents of enrolled children in
the Carolina Curriculum to capture situations by using collected photos and videos relating to the behaviors of
their children during the assessment period at home and to send these to the ad-hoc social network by means of
their mobile devices, and from the others side, medical staff to care adequately the patients in a “remote-way”,
analyzing and providing certified feedback, answers and if needed request an additional visit, by following the
progress of these children thanks to the received multimedia objects.
1 INTRODUCTION
The study of medical protocols for monitoring and
analyzing the cognitive development of children with
disabilities is a very spread out research area (Chap-
man and Hesketh, 2000). In this context, the Carolina
Curriculum for Infants and Toddlers with Special
Needs (CCITSN) (M. Nancy, 2014) is a well estab-
lished curriculum-based assessment for young chil-
dren with disabilities. Recently in Italy the Carolina
Curriculum has been adopted as a basic service
within several local Regional Service Systems (ASL)
(see (Del Giudice et al., 2006)). A full web applica-
tion software system, named Carolina, based on the
Carolina Curriculum protocol is available in (Cuomo
et al., 2011). This software allows, from one side, to
efficiently collect, represent, and evaluate the relative
data along the curriculum and, from the other side, to
support educators, doctors, parents, volunteers, thera-
pists, and the children themselves in the assessment-
intervention process of the children involved. Unfor-
tunately, the Carolina protocol, and so the software
developed in (Cuomo et al., 2011), takes care only
of the medical aspects, which are basically recorded
with a huge gap of time intervals.
Moreover, families and children cannot communicate,
ask questions and post experiences on the software.
Indeed, the missing of interaction makes the use of the
Carolina program less useful in practice. The major
difficulty that prevents a wide dissemination of this
medical protocol is the long time interval between a
medical visit and the next one. During this period, of
about four/six months, the enrolled child receives a
list of items (activities) that he has to improve through
specific practices; but although he’s constantly moni-
tored by his parents, in the majority of cases situations
that would require the medical intervention occurs.
To address this problem, we consider the applications,
473
Cuomo S., De Michele P., Piccialli F., Olivo A. and Del Giudice E..
CarolApp - A Mobile e-Health Software Project for Remote Monitoring of Children enrolled in the Carolina Curriculum.
DOI: 10.5220/0004911604730477
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2014), pages 473-477
ISBN: 978-989-758-010-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

services and tools that are web-based for health care
consumers, caregivers, patients, health professionals
and biomedical researchers.
The Social networking service embedded in the
Carolina software is a preliminary solution (Cuomo
et al., 2012); it involves the explicit modelling of con-
nections between people, forming a network of re-
lations, which in turn enables and facilitates collab-
oration and collaborative filtering processes. In the
proposed framework, this service enables the fami-
lies enrolled in the Curriculum to ask assistance to
medical operator by means of messages, web con-
ference, etc.; moreover, it enables to see what their
peers or others with a predefined relationship (“fam-
ilies friend”, “doctor”, “assistant operator”, etc.) are
doing in the same assessment; finally, it enables to
have supplementary medical advices on demand by
means of their smartphone. An increasing number
of healthcare professionals put into use smartphones’
applications that enable remote monitoring or health-
care management (Zorba et al., 2012). Moreover, lots
of patients already take advantage of m-health appli-
cations to improve and assist their own life and health.
According to this perspectives, this paper describes
the design and development of CarolApp, a mobile
framework that allows, from one side, parents of en-
rolled children in the Carolina Curriculum to capture
situations by using collected photos and videos relat-
ing to the behaviors of their children during the as-
sessment period at home and to send these to the ad-
hoc social network by means of their mobile devices,
and from the others side, medical staff to care ade-
quately the patients in a “remote-way”, analyzing and
providing certified feedback, answers and if needed
request an additional visit, by following the progress
of these children thanks to the received multimedia
objects. The outline of the paper is: Section 2 draws
some motivation and related work; in Section 3 we
describe the system framework; Section 4 explains a
first experiment. Finally, in the Section 5 we give the
conclusions.
2 MOTIVATION AND RELATED
WORK
Familiarizing people with smart devices and the con-
stantly growing use of medical related mobile appli-
cations enables complete and systematic monitoring
of a series of chronic diseases both by health profes-
sionals and by patients. A large number of mobile
applications have already been developed to support
medical staff and to record and manage information
related to chronic diseases. Handheld devices have
been exploited in many cases to facilitate health ori-
ented procedures. M-health can be defined as “mo-
bile computing, medical sensor, and communications
technologies for health-care”. This emerging concept
represents the evolution of e-health systems from tra-
ditional desktop “telemedicine” platforms to wireless
and mobile configurations (Altini et al., 2010). Devel-
opments in wireless communications integrated with
developments in pervasive and wearable technologies
will have a radical impact on future health-care deliv-
ery systems (Istepanian et al., 2004). Mobile appli-
cations solutions are becoming increasingly popular
because they can be used by a great number of people
and target different health issues or groups of patients
(Karan et al., 2012).
Many consumers nowadays take advantage of m-
Health applications to improve their lives and assist
their health (Fox, 2010). Benefits of m-Health Appli-
cations and Solutions are widely known and accepted.
Many existing applications meet the needs of individ-
ual specialties in medicine (Chemlal et al., 2011) and
work in similar ways, whether they are stand-alone
applications or they work online. These applications
usually have common characteristics; they record crit-
ical medical data and communicate with other appli-
cations in an effort to solve a health issue (Klug et al.,
2010). Data related to health records are often sent
to servers storing personal health record services or
directly to physicians (Boulos et al., 2011).
To better understand the motivations behind our work,
it is important to analyze the gap between the children
enrolled in the Carolina Curriculum and the medical
staff that should care them, throughout the period of
assessment at home. Provide the possibility for par-
ents of these children, to be assisted through a few
simple clicks on their mobile devices, during this pe-
riod, is a fundamental task. In fact, the guidelines of
this curricular protocol strongly recommend that the
child has to be constantly monitored during the course
of his daily activities at home, suggesting where nec-
essary correctives.
3 FRAMEWORK OVERVIEW
CarolApp is conceived to be a stand-alone applica-
tion, evaluated for iOS and Android platforms. Main
criteria used to develop CarolApp are: (i) operating
stand-alone on a mobile platform; (ii) increasing the
interactions between patients and medical operators
covering a wide range of specific topics. In the fol-
lowing, we highlight some important requirements, in
this case, were respected in the application develop-
HEALTHINF2014-InternationalConferenceonHealthInformatics
474
ment, namely:
• Medical Usability. The application should have
been easy to use for physicians. It should have
required minimal training and minimal mainte-
nance. It should have minimized power consump-
tion to avoid the inconvenience of recharging. It
should be portable so that all actors unrolled in the
assessment program can use the application any-
where they go and on several devices.
• Manageability. The application should be easy to
install, deploy, and maintain. It should have pro-
vided tools to assist solution to the clinical prob-
lem treated.
• Reliability. The application should have worked
specific security policies for preserving sensitive
informations stored in the web Carolina web ap-
plication.
The proposed framework design and implements an
architecture for enabling a remote support strongly
connected with the social networking healthcare plat-
form, by means of a mobile application that offering
the opportunity for parents to request medical sup-
port and feedbacks, during the assessment program
of their children at home. The overall information ob-
tained by the Carolina Curriculum therapy are elab-
orated by different software modules and the plan-
ning program in reported in Develop Progress Dia-
gram charts (see (Cuomo et al., 2011; ?)). We expand
the assistance due to the actors of this protocol with a
social network.
Taking some of the terminology from Carolina Cur-
riculum and mapping them to social networking, we
define the following terms:
Carolina Assessment Group: A group within a
buddy-list comprising of health-care professionals
and the patients.
Carolina Medical Group: A group within a
buddy-list comprising of health-care professionals
only.
Families Context: A group of families enrolled in
the Curriculum.
Supplementary service: Experts that sit in the
care groups offering predefined services to the users
of the group.
Social Networking Services: Instant Messaging
(IM), Web Conferences, Posted Messages, Wiki, etc.
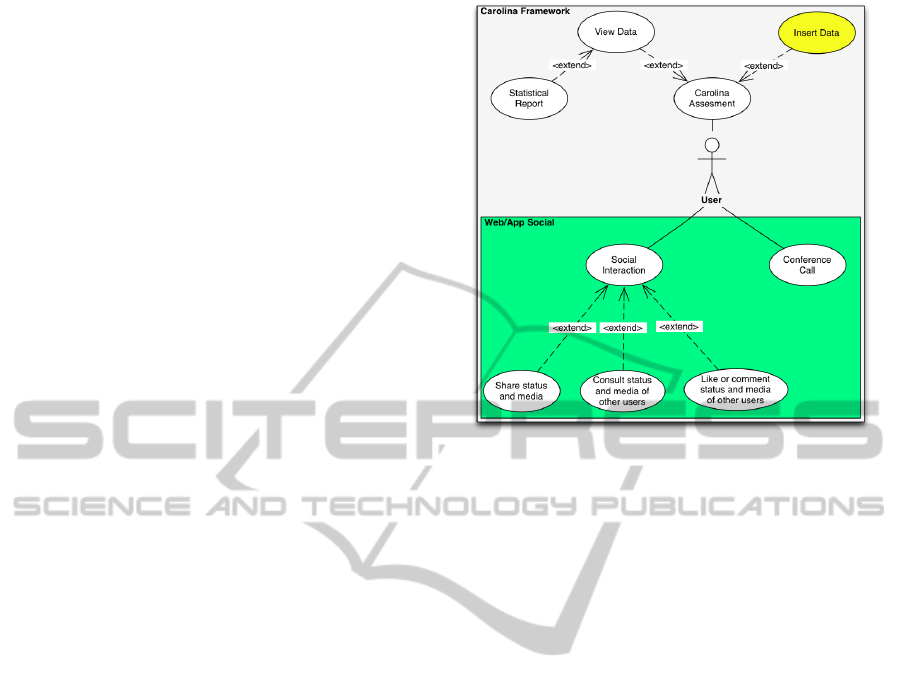
The following is an experimented scenario that shows
the integration of social networking terms into the
work of the Carolina community. In the Figure 1 we
report the use case diagram of the overall Carolina
framework. The Carolina web based features, named
Carolina Assessment, are integrated and extended
with the Social interactions in the green rectangle of
Figure 1: Use case Diagram.
the figure. All users can access to Carolina Assess-
ment, Social Interaction and Conference call system
modules. The Social Interaction is extended many
functionality options, as the possibility to share or
view video, photo, posts and media. In the proposed
software only power users, such as doctors or autho-
rized operators, are able to manage reserved data of
the Carolina medical protocol, reported in the yellow
chart of the use case diagram.
In this framework we have implemented new mod-
ules and services of the social networking without
changing the modular software infrastructure of the
Carolina Software (see (Cuomo et al., 2011)). In the
Figure 2 we report the graphical interface of the web
based social interaction module. Finally, in the next
section we reports preliminaries results.
4 A PRELIMINARY
EXPERIMENT
We test the alpha-version of the CarolApp with 5
medical operators that were involved in the care of
10 families (with children enrolled in the assessment
program). The families are split logically into care
groups associated with the age of patients. The pa-
tients within a fixed age group have to develop the
right skills in accordance to the age. Here for brevity
we report an interaction that has taken place in the
Carolina Assessments program through CarolApp. A
patient performs (see Figure 3) some of the tasks as-
signed to him for the achievement of a certain skill.
The family have posted the event and had a feedback
CarolApp-AMobilee-HealthSoftwareProjectforRemoteMonitoringofChildrenenrolledintheCarolinaCurriculum
475

Figure 2: Web Based Social interaction module.
from the Doctors. Consequently, the family decides to
post a request for assistance in Carolina Call Confer-
ence to the Carolina Medical Group. A parent of the
children decides to activate and schedule on-line as-
sistance service through the web conference tool pro-
vided by CarolApp (see Figure 4).
In the meanwhile, the community starts to answer and
post advices on the Group of Families Context, so ex-
ploit the services offered by social networking.
According to the model showed, four ideas emerge
from the Social Network service applied to Carolina,
succinctly described in the following. The Participa-
tion of families, patients and medical operators that
became active actors of the medical assessment pro-
gram. The Openness of the system that permits to in-
dividuals and healthcare organizations to operate by
a communal management decision-making process.
The Collaboration between all enrolled people of the
curriculum that work all together to improving the pa-
tients development skills. Finally, the Communica-
tion that enables the efficient exchange of experiences
and sharing emotional states. Our model is a multidi-
mensional scheme in which we have different levels
of interactions. Horizontal interactions between fam-
ilies and patients enrolled in the assessment. Vertical
communications between families and medical opera-
tors that work with Carolina. Each user of every group
has received a different level of training assessment.
Families and patients can be seen as experts and their
Figure 3: Carol App interaction: Share informations.
Figure 4: CarolApp Call Conference tab.
collective wisdom can and should be used. It is well
known that the health operator is an expert in identi-
fying disease, while the patients and families are ex-
perts in experiencing it. The Carolina framework has
a client tier, an application tier, and a data tier, work-
ing as follows: every single Regional Local Health
Department is connected to a Data Center in order to
store and manage the data of the medical protocol.
The Carolina portal and the Social Network represent
the two souls of the framework architecture, working
together in a virtuous way.
In the social networking service, a user-friendly
graphic interface (see Figure 3), allows the opera-
tors and families to easily share data among them,
have detailed information about scores and items of
the curriculum, monitor skills development along the
HEALTHINF2014-InternationalConferenceonHealthInformatics
476

time by means of system communication. Doctors,
patients and their families can share medical data as
well as personal experience and troubles, which turns
to be helpful both in the medical and emotional sides.
All these features guarantee that every child will have
a full assistance, corresponding to his specific needs.
5 CONCLUSIONS
In this paper we present CarolApp, an ongoing
e-health project for the CCITSN medical proto-
col, which extends the Carolina software with the
embedded Social networking service, implemented
in (Cuomo et al., 2011; Cuomo et al., 2012), by means
of the design and develop of a mobile application that
is able to collect texts, photos, and videos of real-
time situations of the child and to forward them to the
ad-hoc social network. The project is certainly am-
bitious, it aims to improve the health benefits of the
Carolina curriculum thanks to an ad-hoc infrastruc-
ture that relies on the ICT technologies; the main goal
of the described framework is to reduce the govern-
ment spending decreasing gradually the unnecessary
clinic visits. Preliminary experimental results showed
the usability of our approach and encourages further
research. Future work will be devoted to finish the de-
ploy of the entire system in the next months and col-
lect more complete and interesting experimental re-
sults about the real advantages of the proposed frame-
work also considering the related costs and benefits,
for example in terms of maintenance needs.
ACKNOWLEDGEMENTS
This paper is financial supported by Associazione
Italiana per lo Studio delle Malformazioni (ASM)
Onlus under the grant “Infrastrutture informatiche di
supporto, monitoraggio ed analisi di dati per bambini
con malattie rare congenite e disabilit
`
a”.
REFERENCES
Altini, M., Penders, J., and Roebbers, H. (2010). An
android-based body area network gateway for mobile
health applications. pages 188–189.
Boulos, M., Wheeler, S., Tavares, C., and Jones, R. (2011).
How smartphones are changing the face of mobile and
participatory healthcare: An overview, with example
from ecaalyx. BioMedical Engineering Online, 10.
Chapman, R. and Hesketh, L. (2000). Behavioral phenotype
of individuals with down syndrome. Mental Retar-
dation and Developmental Disabilities Research Re-
views, 6(2):84–95.
Chemlal, S., Colberg, S., Satin-Smith, M., Gyuricsko, E.,
Hubbard, T., Scerbo, M., and McKenzie, F. (2011).
Blood glucose individualized prediction for type 2 di-
abetes using iphone application.
Cuomo, S., Murano, A., and Piccialli, F. (2011). The
c@rolin@ software: A system for monitoring skills
development of children with down syndrome. pages
180–185.
Cuomo, S., Murano, A., Piccialli, F., and Del Giudice, E.
(2012). A social network framework for the carolina
software.
Del Giudice, E., Titomanlio, L., Brogna, G., Bonaccorso,
A., Romano, A., Mansi, G., Paludetto, R., Di Mita,
O., Toscano, E., and Andria, G. (2006). Early inter-
vention for children with down syndrome in southern
italy: The role of parent-implemented developmental
training. Infants and Young Children, 19(1):50–58.
Fox, S. (2010). Mobile health 2010, pew research centers
internet and american life project. Technical report.
Istepanian, R., Jovanov, E., and Zhang, Y. (2004). Introduc-
tion to the special section on m-health: Beyond seam-
less mobility and global wireless health-care connec-
tivity. IEEE Transactions on Information Technology
in Biomedicine, 8(4):405–414.
Karan, O., Bayraktar, C., Gmkaya, H., and Karlik, B.
(2012). Diagnosing diabetes using neural networks
on small mobile devices. Expert Systems with Appli-
cations, 39(1):54–60.
Klug, S., Krupka, K., Dickhaus, H., Katus, H., and Hilbel,
T. (2010). Displaying computerized ecg recordings
and vital signs on windows phone 7 smartphones. vol-
ume 37, pages 1067–1070.
M. Nancy, J.-M. (2014). The Carolina Curriculum for In-
fants and Toddlers With Special Needs.
Zorba, I., Paschou, M., Sakkopoulos, E., and Tsakalidis, A.
(2012). Appification of hospital healthcare and man-
agement.
CarolApp-AMobilee-HealthSoftwareProjectforRemoteMonitoringofChildrenenrolledintheCarolinaCurriculum
477
