
Electrical Stimulation System to Relax the Jaw Elevation Muscles
in People with Nocturnal Bruxism
Pablo Aqueveque, Roberto Lopez and Esteban Pino
Department of Electrical Engineering, University of Concepcion, Concepción, Chile
Keywords: Bruxism, Electrical Stimulation, Stimulator.
Abstract: Nocturnal bruxism (NB) is a temporomandibular disorder characterized by an excessive clenching and
involuntary parafunctional grinding of the teeth during sleep. In this paper, we present a device that
generates electrical stimulation to produce an inhibitory action of the muscles involved in the elevation of
the jaw. The device measures the electromyographic (EMG) signal of the left temporalis anterior (LTa)
muscle to determine the intensity of contraction. It then, stimulates the right mental nerve to produce a
decrease in the contraction intensity of the jaw elevation muscles. The device was used by one bruxist
subject for 12 nights. The results showed that, on average, the percentage decrease of the EMG activity was
43.55% when a bruxism event occurred. The events of nocturnal bruxism appeared mostly one and three
hours after going to sleep. In conclusion, the electrical stimulation device generated an important inhibitory
action of the LTa muscle when the subject was performing nocturnal bruxism. Thus, this result indicates
that the device could be useful as a possible treatment for bruxism.
1 INTRODUCTION
Nocturnal bruxism (NB) is a temporomandibular
disorder that has periodic and stereotyped movements.
It is characterized by an excessive grinding and
involuntary clenching of the teeth during sleep
(ASDA, 1998). If left untreated, it causes irreversible
damage to the teeth, including the periodontium and
joint surfaces (Carlsson, 1999). In the short-term, NB
produces general fatigue, poor sleep quality, headache
and pain in the mandibular elevator muscles. Chronic
effects can include structural periodontium damage,
temporomandibular joint dysfunction (TMJ) and
severe tooth wear including broken teeth. The
prevalence of NB varies between 5% to 36% (Bader,
2000)(Abou-Atme, 2004) depending on the age of the
patient.
The treatments currently used for bruxism are only
of limited benefit. Therefore, we implemented a
device that is based on electrical stimulation to an
inhibitory sensory afferent (right mental nerve). When
this inhibitory afferent is activated, it induces a
decrease of contraction of the muscles that elevate the
jaw. Thus, theoretically, it should decrease the
intensity of events of NB (Jadidi, 2007)(Jadidi, 2011).
We performed an evaluation of the effects over
the masseter and temporalis anterior muscles in 28
subjects with and without bruxism when electrical
stimulation is applied to the right mental nerve. The
results showed that, on average, the percentage
decrease in the bruxist group for the right masseter
was 25.02% and for the left masseter 25.87%. These
results indicate that the inhibitory system produces an
important decrease in the electrical activity of the two
muscles, so it is a good starting point for a possible
treatment in patients with bruxism and to develop new
electronic stimulators (Aqueveque, 2013).
In this paper, we show the experiment that was
performed to evaluate if the our electrical stimulation
device causes a decrease in the electromyographic
(EMG) activity when it is used by a bruxist subject
during sleep. The experiment was conducted in one
bruxist subject, who used the device for 12
consecutive nights. We observed that the device
detects the events of NB and decreases the EMG
activity by electrically stimulating the mental nerve.
278
Aqueveque P., Lopez R. and Pino E..
Electrical Stimulation System to Relax the Jaw Elevation Muscles in People with Nocturnal Bruxism.
DOI: 10.5220/0004915402780282
In Proceedings of the International Conference on Biomedical Electronics and Devices (BIODEVICES-2014), pages 278-282
ISBN: 978-989-758-013-0
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
2 MATERIALS AND METHODS
2.1 Electrical Stimulation Device
The stimulation device used electrical stimulation on
the right mental nerve to generate a decrease in the
intensity of contraction of the jaw elevating muscles.
To measure the level of contraction, the device uses
the integrated EMG (iEMG) signal of the left
temporalis anterior (LTa) muscle. The EMG was used
because it is proportional to the bite force (Gonzalez,
2011) and is therefore, a good indicator of high and
low contractile activity of the muscles that elevate the
jaw (Cardenas, 2002).
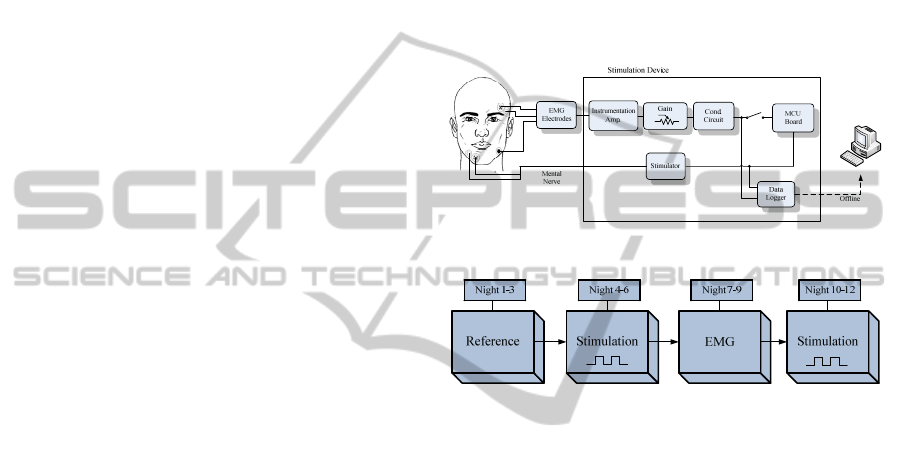
The diagram of the stimulation device is shown in
Fig. 1, where it can be observed that the EMG signal
is acquired with surface electrodes. The signal then
enters the device where it is amplified with an
instrumentation amplifier (INA128). The gain of the
amplification is variable and adapts the maximal
amplitude of the EMG to the range of entry permitted
by the microcontroller unit (MCU). This range of
entry is 0V to 3.3V.
In the conditioning circuit block the signal offset is
removed and filtered with a bandpass filter of second
order. The bandpass filter has cutoff frequencies of
10Hz and 500Hz, which is the bandwidth of the EMG.
Thereafter, the signal is rectified and smoothed to
obtain the iEMG. The iEMG is the signal used to
detect the events of NB in the MCU.
In the MCU block, the signal enters the MCU
when the onset switch is enabled. An algorithm is
implemented to detect the events of NB. The sampling
frequency of the digital to analog converter (DAC) is
4800Hz. The bruxism detection algorithm establishes
when the threshold of 25% of the maximal voluntary
contraction (MVC) is reached. During a window of
0.52 seconds the cumulative integral of the iEMG is
calculated to determine if there is presence of bruxism.
When this occurs, the MCU sends a stimulation signal
to the stimulator. The electrical stimulation is
activated by an ON/OFF control. The stimulation
waveform is a square-wave train with different values
of amplitude. A duration of 2 seconds was defined for
the stimulation. The frequency of the signal was
300Hz with a pulse width of 1.67ms.
The stimulator block receives the stimulation
signal sent by the MCU and modulates the amplitude
of the stimulation. The stimulator is voltage-regulated.
Once the stimulation is modulated, it is sent to the
right mental nerve, closing the circuit and generating
the biofeedback.
Finally, the data logger block registers the iEMG
signal and also the signal that activates the stimulation
in the MCU. Data is stored in an external memory to
perform an offline analysis in a PC later. The data is
analyzed with Matlab to obtain the iEMG signal and
calculate the percentage decrease of the area under the
curve (AUC) that denotes a reduction of the
contractile activity of the muscle. To calculate the
percentage decrease in Matlab, the bruxism detection
algorithm was used. In this case, we calculated the
AUC of the signal before and after the stimulation to
obtain it.
Figure 1: Diagram of the system.
Figure 2: Diagram of the study design.
2.2. Experimental Procedure
To evaluate the proper functioning of the stimulation
device, we asked one subject to use the device while
sleeping. This allowed us to observe if the device
detects the events of NB, stimulates electrically, and if
it produces a decrease of the iEMG signal when the
subject is performing nocturnal bruxism.
Informed consent based on the Helsinki protocol
was implemented to inform the patient a 25 year old
male bruxist, about the experiment.
Tests were performed during 12 consecutive
nights. The records started once the subject went to
sleep at midnight until he woke up. Fig. 2 shows the
diagram of the study design. During the first three
nights only the iEMG signal was recorded to establish
a reference of the subject signal, no stimulation was
applied. During nights 4 to 6 stimulation was applied
to the mental nerve while the subject was sleeping.
During nights 7 to 9 the signals were recorded without
stimulating electrically. Finally, during nights 10 to 12
the signals were recorded and electrical stimulation
was applied to the mental nerve.
The experiments were performed in the subject’s
ElectricalStimulationSystemtoRelaxtheJawElevationMusclesinPeoplewithNocturnalBruxism
279
home and the equipment used was the stimulation
device described above. The device registers the EMG
signal of the LTa and stimulates the mental nerve with
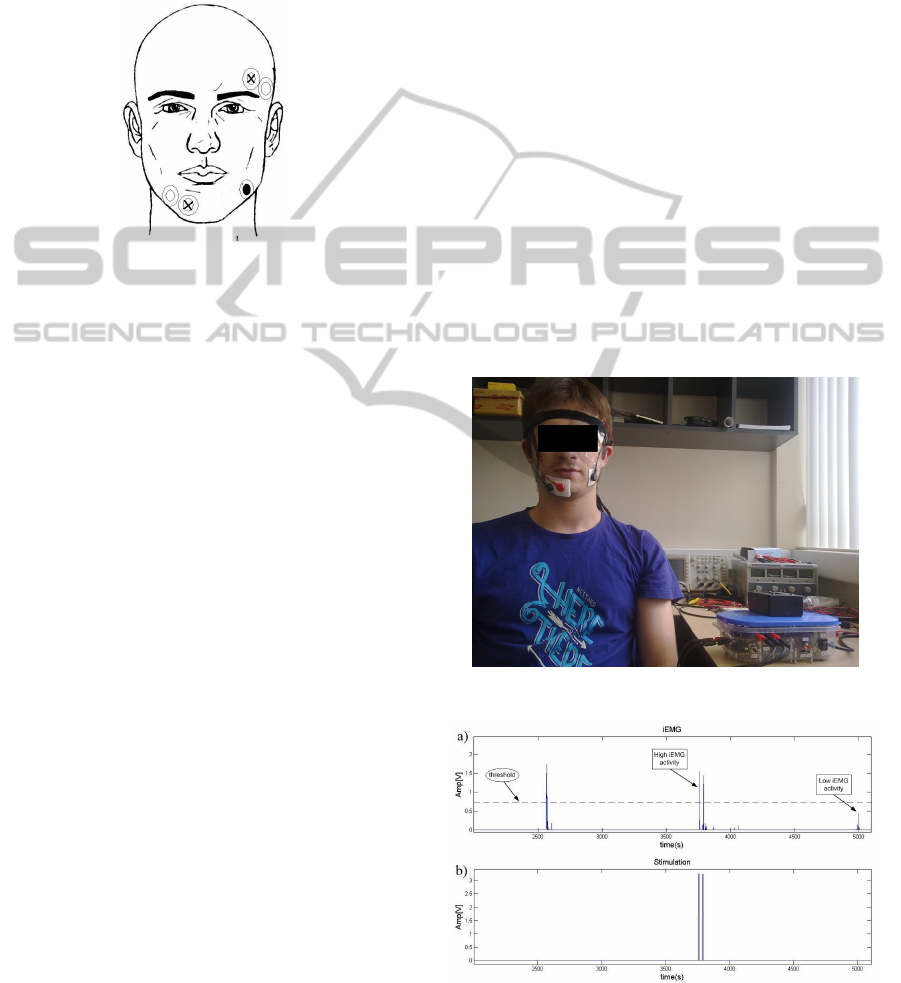
surface electrodes. The position of the positive (x),
negative (white) and reference (black) electrodes is
shown en Fig.3. The positive and negative electrodes
of the stimulator were placed on the chin.
Figure 3: Positioning of electrodes.
Each night the subject had to clean the places where
the electrodes were to be positioned. Later he had to
place the electrodes and mount a headband with the
electrode cables of the device. He then had to turn on
the device and adjust the amplification of the EMG
signal clenching his teeth at MVC to achieve the
maximum voltage accepted by the MCU.
Additionally, the amplitude of stimulation had to be at
0.5V with a frequency of 300Hz. These values were
defined by previous tests, which were carried out to
establish if the iEMG signal decreased when the
mental nerve was electrically stimulated.
Once these steps were performed, the onset switch
had to be enabled and the device started recording.
The subject could then go to sleep. When the subject
woke up, he had to turn off the device and take off
the headband.
3 RESULTS
Fig. 4 shows the complete electrical system for
measuring and detecting events of NB. The system
consists of the electrical stimulation device, the signal
and stimulation cables, and the surface electrodes.
The data obtained in this study was analyzed to
observe the effect of electrical stimulation on the
iEMG signal, and to calculate the percentage decrease
of the AUC of the iEMG when the mental nerve is
stimulated electrically. The length of time recorded
each night was 5.71 ± 1.37hrs. The average
percentage decrease of the AUC during the six days
with stimulation was 43.55 ± 26.07%.
Fig. 5 shows a segment of one record of the iEMG
signal acquired with the device: a) display the iEMG
of the subjectwith the threshold of detection
(25%MVC) and the different intensities of EMG
activity recorded. Fig. 5.b) shows the activation
stimulation signal that indicates the moments when the
stimulator is active. In this segment, the device
detected two events of NB when the iEMG activity
was high. This means that the activity exceeded the
threshold, and the cumulative integral calculated
within the window of 0.52s was sufficient to
determine it as a bruxism event. In the first high
activity, the algorithm did not detect bruxism.
Fig. 6 shows a zoom of the iEMG signal that
corresponds to a NB event detected. In a) the iEMG
and the activation stimulation signal are shown. The
legends Eve-Est and Eve-iEMG indicate the moment
when the stimulation was applied, corresponding to
the signal stimulation (Est) and iEMG respectively.
The iEMG decreases when the electrical stimulation is
applied to the mental nerve. Fig. 6.b) shows a NB
event detected when electrical stimulation was not
applied. The remarkable point when comparing both
Figure 4: System used for the study.
Figure 5: Segment of data recorded with the stimulation
device. a) iEMG, b) activation stimulation signal.
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
280
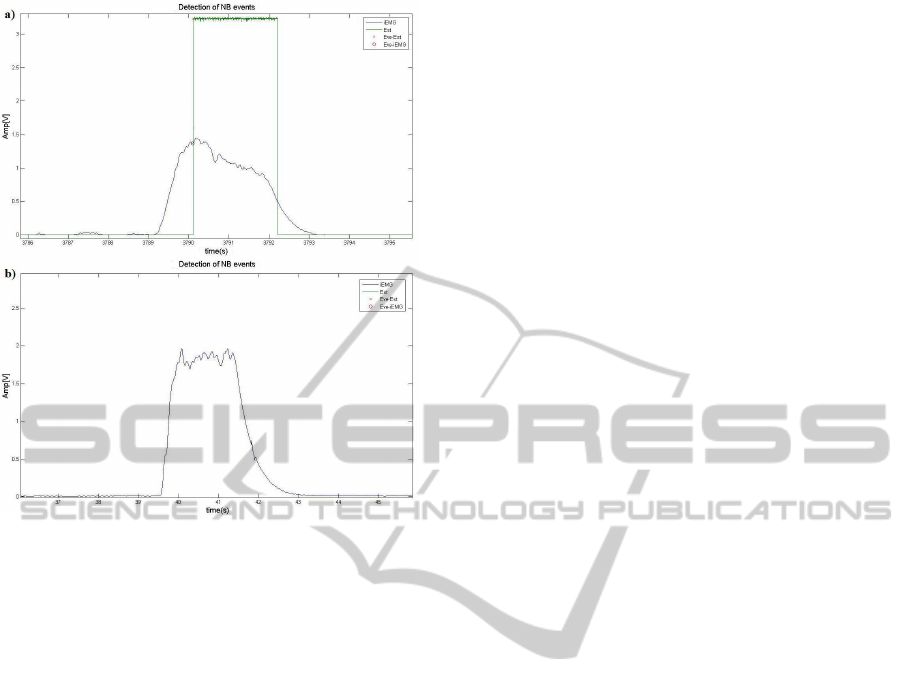
Figure 6: Nocturnal bruxism event with electrical
stimulation applied. a) event with stimulation, b) event
without stimulation.
records, a) and b), is that the iEMG signal decreases
when electrical stimulation is applied. However, when
a NB event is performed and no electrical stimulation
is applied, the amplitude of the iEMG remains high
until the NB event ends.
4 DISCUSSION
During the study the electrical stimulation device
recorded the EMG and the stimulation signal. It also
detected the activity related to bruxism when the
subject was sleeping, and then electrically stimulated
the mental nerve.
The percentage decrease of the EMG signal was
considerable (43.55%). This is consistent with the
results obtained in our previous studies with electrical
stimulation of the mental nerve in bruxist and non
bruxist subjects. Other studies (Jadidi, 2010) indicate
that electrical stimulation to inhibitory afferents of the
face can induce an inhibitory action while the bruxist
subjects were sleeping.
5 CONCLUSIONS
Electrical stimulation device caused an inhibitory
action in the intensity of muscle contraction elevating
the jaw. The average percentage decrease of the iEMG
signal for the complete study decreased by 43.55 ±
26.07%. This means that when the bruxist was
sleeping the stimulation of the mental nerve caused a
decrease of the bite force during a NB event.
Although the results of the study were
satisfactory, it should be repeated using a larger
sample of subjects and extended study time.
Additionally, the effectiveness of this electrical
stimulation device must be analyzed further.
REFERENCES
ASDA, 2001, American Sleep Disorders Association,
international classification of sleep disorders, revised:
Diagnostic and coding manual, Rochester, MN:
American sleep disorders association, pp. 182-185.
Aqueveque P., López R., Pino E., and Ogalde A., 2013,
“Electrical stimulation of the mental nerve to produce
inhibitory action in bruxism treatment”, Electronic
Letters, Vol. 49, issue 3, pp. 176-177.
Abou-Atme Y. S., Mellis M., and Zawawi K. H., 2004,
“Bruxism prevalence in a Selective Lebanese
Population” Journal of the Lebanese Dental
Association, vol. 41, No. 2.
Bader G. and Lavigne G., 2000, “Sleep bruxism; an
overview of an oromandibular sleep movement
disorder” Sleep Medicine Reviews, vol. 4, No. 1, pp.
27-43.
Cardenas H., Ogalde A., 2002, “Relationship between
occlusion and EMG activity of the masseter muscles
during clenching at maximal intercuspal position: A
comparative study between prognathics and controls”
Journal of Craniomandibular Practice, vol. 20, (2).
Carlsson G., and Magnusson T., 1999, “Bruxism and other
oral parafunctions” Management of
Temporomandibular Disorders in the General Dental
Practice, Cap. 5, Quintessence Publ. CO. Inc., pp. 33-
42.
Gonzalez Y., Iwasaki L. R., McCall W. D., Ohrbach R.,
Lozier E., and Nickel J. C., 2011, “Reliability of
electromyographic activity vs. bite-force from human
masticatory muscles” Eur J Oral Sci, vol. 119, pp. 219–
224.
Guyton A., Hall J. E., 2006, “Textbook of medical
physiology”, 11
th
edition.
Jadidi F., Wang K., Arendt-Nielsen L., Svensson P., 2010,
“Effects of different stimulus locations on inhibitory
responses in human jaw-closing muscles”, Journal of
Oral Rehabilitation, 38(7): 487-500.
Jadidi F., Castrillon E., and Svensson P., 2007, “Effect of
conditioning electrical stimuli on temporalis
electromyographic activity during sleep” Journal of
Oral Rehabilitation, vol. 35, (3), pp. 171-183.
Jadidi F., Norregaard O., Baad-Hansen L., Arendt-Nielsen
ElectricalStimulationSystemtoRelaxtheJawElevationMusclesinPeoplewithNocturnalBruxism
281

L., and Svensson P., 2011, “Assessment of sleep
parameters during contingent electrical stimulation in
subjects with jaw muscle activity during sleep: a
polysomnographic study”, Eur J Oral Sci, vol. 119,
pp.211-218.
Lavigne G., Rompré P., Montplaisir J., 1996, “Sleep
Bruxism: Validity of Clinical Research Diagnostic
Criteria in a Controlled Polysomnographic Study”, J
Dent Res, 75(1): 546-552.
Lavigne G., Guitard F., Rompré P., Montplaisir J., 2001,
“Variability in sleep bruxism activity over time”, J
Sleep Res, 10, 237-244.
Macaluso G., Guerra P., Di Giovanni G., Boselli M.,
Parrino L., Terzano M., 1998, “Sleep Bruxism is a
Disorder Related to Periodic Arousals During Sleep”, J
Dent Res 77(4): 565-573.
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
282
