
Leveraging Adaptive Sessions Based on Therapeutic Empathy
Through a Virtual Agent
Adrián Bresó, Juan Martínez-Miranda and Juan Miguel García-Gómez
Grupo de Informática Biomédica, Instituto ITACA, Universitat Politècnica de València, Spain
1 STAGE OF THE RESEARCH
This document describes the work under
development as part of a PhD Thesis carried out in
the context of the European Project “Help4Mood –
A Distributed System to Support the Treatment
of Patients with Major Depression”
(www.help4mood.info) [FP7-ICT-2009-4; 248765].
Help4Mood aims to support the treatment of patients
with Major Depression using Information and
Communications Technology (ICT). The resultant
Personal Health System (PHS) of Help4Mood uses a
set of activity sensors (such as wrist watch, key ring,
or under-mattress sensor) that gather information
about the daily physical and sleep activities from the
patient. This information and other data obtained
through standardized questionnaires are analysed in
order to infer some recommendations (or alerts) and
offer adaptive and tailored tasks as part of the
treatment in the form of daily interactive sessions
provided by a Virtual Agent (VA).
The initial developed work for the project
resulted in the MSc Thesis entitled “Generic Data
Processing & Analysis Architecture of a Personal
Health System to Manage Daily Interactive
Sessions in Patients with Major Depression”
(Bresó, 2013) within the Artificial Intelligence,
Pattern Recognition and Digital Imaging MSc
program at the Technical University of Valencia. In
this MSc Thesis, the author describes the design and
the implementation of the Data Processing &
Analysis layer of the Help4Mood’s PHS. It had been
conceived as the module responsible to analyse
relevant patient’s data, plan the daily interactive
sessions and recommend a set of tailored activities
configured by clinicians that help in the recovery of
the patient. Additionally, this system included an
initial cognitive-emotional module aimed to infer the
specific set of emotions to be displayed by the VA
during the interaction
The research work presented in this document is
an extension of the work done in the MSc's Thesis.
The proposed extension will allow a deeper research
on how to improve current Human-Agent
Interactions particularly addressed to users that are
under treatment of Major Depression. Some theories
in the areas of psychology and cognitive science will
be the basis of a computational model that is
expected to improve the production of the daily
session’s content and the adequate –emotional–
fashion for a better engagement of the users
promoting the long-term use of the system.
2 OUTLINE OF OBJECTIVES
The proposed research work is focused on the
improvement of the treatment adherence and the
user acceptability through two main contributions in
the computer-based psychotherapy:
1. Get a modular and flexible computational
architecture to improve Human-Agent
Interactions during the daily sessions provided
as part of treatment to patients with Major
Depression.
2. Encourage the system’s realism and reliability
through the generation of VA’s empathic
responses based on a modelling of Therapeutic
Empathy.
3 RESEARCH PROBLEM
Depression is expected to be the disorder with the
highest disease burden in high-income countries by
the year 2030 (WHO, 2012). Patients with Major
Depression should follow a specific and continued
treatment based on therapeutic sessions (and/or
drugs) and evaluations to treat the illness and
achieving recovery and prevent future relapse
(Vittengl, 2007). The lengthening of treatment and
relapses increases the healthcare resources and the
46
Bresó A., Martínez-Miranda J. and Miguel García-Gómez J..
Leveraging Adaptive Sessions Based on Therapeutic Empathy Through a Virtual Agent.
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

healthcare costs, and reduces the quality of life in
the patients.
The magnitude of the lack of therapeutic
adherence is estimated close to 50% in patients with
chronic diseases (Sabatâe, 2003). In particular, non-
adherence in psychiatric disorders is 75% (Rigueira,
2001). The benefits of the therapy are drastically
diminished due to the lack of adherence (Sotoca-
Momblona, 2006). Despite the wide range of studies
on interventions to improve adherence to treatment
(DiMatteo, 1993; Dulmen, 2007; Sabatâe, 2003;
Coombs, 2003; Katon, 1996; Thompson, 2012),
there is no clear evidence on the effect to promote
compliance or clinical parameters (Márquez, 2001;
Rigueira, 2001).
Currently, the use of ICT in mental health is
fairly new and there are open questions and
challenges to effectively apply it. In particular,
patients with Major Depression often have
associated a distorted and negative thinking which
makes them prone to suffer anxiety when interacting
with computer systems (Safford, 1999). Much effort
is needed to develop systems that can be widely
accepted and improve the adherence to computer-
based psychotherapy.
4 STATE OF THE ART
4.1 Human-Agent Interaction in
Mental Health
The development of Human-Agent Interactions
(HAI) applied to Mental Health is a difficult task
because many of the content in therapeutic sessions
are related with personal issues (e.g. thoughts,
emotions and feelings). Therefore, a feasible
computer-based psychotherapy must gain an
acceptable level of trust from the patient.
Particularly important is the content of the message
disclosed to the patient, and the way in which the
VA displays the message.
Systems based on VA have evolved greatly over
the past two decades, improving the interactions
with users. Many studies have demonstrate the
utility of using VAs for training and learning
purposes (Core, 2006; Martínez-Miranda, 2008;
Castellano, 2013), and games (Gebhard, 2008;
Mateas and Stern, 2003; Andrist, 2013).
Regarding the health context, we can find
systems that train clinicians (Raij, 2007; Kenny,
2007), control patient adherence to medication
(Bickmore and Pfeifer, 2008), and promote physical
exercise (Bickmore, 2006). There are also works
applied to mental health, as the system that support
patients with phobias (Krijn, 2004; Brinkman,
2008), post-traumatic stress disorder (Rizzo and
Josep, 2011), systems aimed at children with autism
(Tartaro and Casell, 2008; Bernardini, 2013),
support interventions to reduce alcohol consumption
(Yasavur, 2013) or systems that implements
standardized questionnaires in order to treat
depression (Pontier and Siddiqui, 2008).
Although initial results are promising, much
effort is still needed to develop systems in which
human-agent interactions are widely accepted for its
use in computer-based psychotherapeutic
interventions. Initiatives such as the developed in the
project Help4Mood would never be able to replace
psychotherapists with the same level of
competences, but may become essential tools to
offer personalized and remote support on daily basis
during the treatment. The key lines of research in
Help4Mood include the mechanism for the planning
of the daily sessions, the generation of the verbal
and nonverbal behaviour in the VA, and the
continuous collection of physical and sleep activities
from the patient through a monitoring system.
Taking the particular characteristics of the addressed
users, the Human-Agent ·Interactions need to be
carefully designed to avoid counter-productive
effects in the target users.
Our proposal, as part of the PhD Thesis is the
construction of a computational model that improve
the current developed system through the generation
of better adaptive sessions regarding to patient’s
condition and the production of an adequate
emotional behaviour in the VA that simulates
therapeutic empathy reactions during the interaction
with the user.
4.2 Treatment Adherence
Treatment adherence was defined by World Health
Organization (WHO) in 2001 as “the extent to which
a person’s behaviour – taking medication, following
a diet, and/or executing lifestyle changes,
corresponds with agreed recommendations from a
health care provider”.
Accurate assessment of adherence behaviour is
necessary for effective and efficient treatment
planning, and for ensuring that changes in health
outcomes can be attributed to the recommended
regimen. Adherence may be measured using either
process-oriented or outcome-oriented definitions.
Outcome-oriented definitions use the end-result of
treatment, e.g. cure rate, as an indicator of success.
LeveragingAdaptiveSessionsBasedonTherapeuticEmpathyThroughaVirtualAgent
47

Process-oriented indicators make use of intermediate
variables such as appointment-keeping or pill counts
to measure adherence.
There are some variables which researchers are
studying in order to determine if they are influencing
the treatment adherence. Neil et al. (Neil, 2009)
investigated personal predictors of adherence in
people who use a Cognitive Behaviour Therapy
website. Neil et al. (Neil, 2009) found to be
associated with increased adherence were lower
baseline rates of depression, younger age, female
gender, and less knowledge of psychological
treatments. Regarding the factors that an ICT
solutions can influence in the treatment adherence,
we can found reviews on treatment adherence based
on "Interventions on technical solutions" (Yildiz,
2004) which are aimed at simplifying the medication
regimen in order to improve the adherence. Other
are based on "Educational interventions”
(Vergouwen, 2003) which are aimed at informing
the patient about the disease and the treatment in
order to empower him to take a more active
participation in disease management. Some others
are based on "Behavioral interventions” (Yildiz,
2004; Pampallona, 2002) such as alerts and
reminders to improve adherence.
Regarding the interventions on technical
solutions, the treatment complexity has been
identified as a cause of poor adherence. It may be
considered therefore reasonable to think that
interventions aimed at simplification would improve
compliance (Orueta, 2005). Therefore, treatment
must be customized and adapted to the daily needs
of the patient and should be less invasive as
possible.
The educational interventions strategies that
increase knowledge about the disease and treatment
seem necessary, but not sufficient to change
behaviour regarding adherence (Orueta, 2005).
However, other studies focused on schizophrenia
claim that psycho-educational interventions have no
effect on adherence (Dolder, 2003; Zygmunt, 2002;
Lincoln, 2007). In depression studies are less
numerous and with inconclusive results.
Additionally, the systems which provide
information and education about the disease, get
empower patients. The most relevant for obtain the
expected therapeutic results factor is the quality of
the doctor-patient communication (Márquez, 2001;
Donovan, 1997; Thompson, 2012). In the
psychological domain, good communication is
achieved through active listening and therapeutic
empathy.
Health care providers must understand behaviour
change as part of an interpersonal process.
Effective behavioural interventions involve the
actions that help the patients to become responsible
for their own decisions and self-care behaviours.
This behaviour change can be reflected into an
increment of treatment adherence. ICT solutions can
contribute to this change through reminders, alerts,
recommendations, self-reflection, or the planning of
routines (Delamater, 2006). Specifically, in the
treatment of major depressive disorders,
psychologists use several tools such as self-
reflection techniques that may improve
psychological outcomes (Delamater, 2006).
It is easier to make assessments of adherence
when drug treatment is performed (e.g. by applying,
Directly-Observed Therapy (DOT)). But when
treatment involves psychotherapeutic sessions, the
assessment is often made through comparisons about
Treatment Adherence Therapy (TAT) (Staring,
2006) versus Treatment As Usual (TAU) as control
group (Staring, 2010; Gilden, 2011) or using
questionnaires (Titov, 2013; Lin, 2012).
5 METHODOLOGY
The main hypothesis under research in this thesis is
that “The use of a computational model that plans
personalized daily sessions and generates
appropriate empathic responses will improve the
adherence in depressed patients avoiding an early
discontinuation of the treatment, which can result in
new episodes or relapses into major depression”.
The following sections outline the proposed
experiments and methodologies designed to address
the proposed hypothesis.
5.1 Adaptive and Flexible Daily Session
Planning
We are extending the generic and flexible session
planner implemented in the previous MSc. Thesis
(Bresó, 2013). The session planner is able to process
and analyse data from different sources (activity
sensors, demographical data, questionnaire scores,
etc.) in order to infer the patient’s condition and
generate an appropriate set of more than 10 tasks
(such as the collection of speech patterns, the
negative thoughts reflexion activity, sleep
questionnaire, or daily mood check questionnaire) as
part of the treatment. For instance, when the patient
answers the Patient Health Questionnaire (PHQ-9),
the system infers and updates the patient’s
ICAART2014-DoctoralConsortium
48

depression level. If the system detects a health
deterioration compared to historical values, the
system will provide a message for the patient to
contact clinical staff and switch the system to the
“emergency mode”. In this mode the system will
plan only a basic set of essential tasks specified by
the clinicians. A complementary example is when
the system detects a critical situation such as suicidal
risks. This situation can be inferred from different
questionnaires. When it is inferred, the planning of
the system is stopped and only one task will be
planned: “crisis plan” task, which will try to calm
and inform the patient about local emergency
telephones to contact for assistance.
All defined tasks are managed in order to
generate an adaptive daily session which is used by
the VA as the core content to communicate with the
users. In this sense, we are working to improve the
treatment adherence as follows:
Interventions based on improved technical
solutions: Future sessions may be more
personalized and suitable to patient’s condition in
order to reduce the complexity of the treatment. This
personalization will be carried out by improving the
analysis of patient activity data for the patient to
estimate objectively the patient’s condition and
expanding the set of activities available to make
more suitable recommendations. The more tasks we
add to the system, more variability and more
personalization can be done. For instance, the
system should be able to automatically adjust the
length of the session to patient stamina level in order
to the patient does not get tired. Currently we are
obtaining the patient stamina level subjectively
through a direct question: “What length of session
you prefer (short/medium/long)?”. We are working
in order to infer the stamina level from the trend of
the past sessions and from gathering activity data.
Educational interventions: The system
provides a full weekly report which contains the
patient progress and the highlights values. We would
add some psycho-educational tasks such as those
used to inform the patient about recommendations
on good habits. For instance, if the system analyses
the data acquired from mattress sensor device and
from sleep questionnaire and it detects a disturbance
in sleep, the system should provide information
related to healthy rest and sleep tips.
Behavioural interventions: Currently, the
system alerts the patient when he/she is not using the
system or the sensors devices. We plan to generate
more sessions with content-related alerts or
recommendations such as “You reject this suggested
activity twice, are you sure that you want to reject it
again?” Additionally, we are defining a behaviour
activation task in order to suggest (and check its
execution) the patient with a set recommended
activities such as walking or socializing. Other
interesting task that we are implementing is the
relaxation task, in which the patient listen a set of
relaxing exercises in order to facilitate relaxation
and self-reflection.
Currently, some of the tasks defined in the
system are based on Cognitive Behaviour Therapy
(CBT) (Gray et al., 2002), which have demonstrated
high adherence because it uses effective cognitive
and behavioural strategies to motivate patients to
complete homework, modify their maladaptive
thinking and behaviour, and solve problems on their
own (Safren, 2012).
Clinicians can configure the available set of
tasks, their frequency, constrains and priorities in
order to customize the system to different clinical
centres, patients or different stages of the treatment.
This Planner is implemented using a (1) Rule Based
System (RBS) running with the JESS engine
(http://herzberg.ca.sandia.gov/) and a (2) planning
algorithm that we have developed.
The rule based system allows to generate the
inference of a clinically adequate set of suggested
tasks. The easy replacement of the set of rules gives
the flexibility to adapt the planner to different
clinical domains such as other mental disorders
(anxiety, phobias, panic, or bipolar). The current
rules are codding the clinical preferences of the
clinician staff involved in the project but it is also
able to code rules from clinical guidelines. Finally,
our designed architecture infers clinical concepts
(using SNOMED-CT terminology) in order to store
valuable information for clinical research purposes.
Most of these concepts have been inferred from the
analysis of the activity sensor data (e.g. “Restless”
and “Activity Sleep Time”).
Regarding the planning algorithm, it is in charge
of planning a personalised daily patient session
based on clinical specifications (frequencies,
constrains, etc.), historical tasks executions,
currently user responses, and the level of stamina.
5.2 Therapeutic Empathy Responses
The modelling of emotional competence in virtual
agents is an active research area where theoretical,
technical, and ethical considerations need to be
addressed. There are currently some computational
models of emotion developed to cover specific
components of the emotional phenomenon.
The selection of a specific emotion theory as the
LeveragingAdaptiveSessionsBasedonTherapeuticEmpathyThroughaVirtualAgent
49

basis of a computational model depends on the
aspects of emotion that the computational model
tries to represent. From the current existent theories
of emotion, the one that predominates above the
others in the efforts dedicated to implement
computational models of emotions is the cognitive
appraisal theory of emotions (Lazarus, 1991;
Scherer, 2001). The core concept of appraisal
theories refer that the events in a person‘s
environment are constantly identified and evaluated
by the individual. This cognitive evaluation (or
appraisal) process leads to an emotional response
(according to the event‘s relevance for the person)
which in turn generates a specific behaviour to cope
with the appraised events.
In the context of the Help4Mood project and in
the subsequent MSc's Thesis (Bresó, 2013), we
developed a Cognitive-Emotional module which is
responsible to produce emotional responses in the
VA during the interaction with the user. This module
has been developed as a stand-alone Java application
which makes use of the FAtiMA (FearNot Affective
Mind Architecture) software libraries
(http://sourceforge.net/projects/fatima-modular/)
(Dias, 2011). FAtiMA is one of the existent
(appraisal theory based) computational architecture
of emotions which its initial objective was the
creation of empathic agents interacting in a virtual
environment to tackle and eventually help to reduce
bullying problems in schools.
With the use of FAtiMA, the emotional
behaviour of a virtual agent has been generated
through the authoring (in a XML-based format) of
their emotional reactions, action tendencies, goals
and actions based on the detection and appraisal of
the events occurred in the agent‘s environment. The
environment of the VA in Help4Mood is basically
composed from all the data received (directly and
indirectly) from the user. These data include the
objective user‘s information collected through the
sensor devices (i.e. actigraphs to identify sleep and
physical activity patterns) and the subjective self-
reported information through standardised
questionnaires. All this information is interpreted
and transformed into the specific events used as the
input to the cognitive emotional module. The
received events will produce the specific VA‘s
emotional behaviour during the interaction with the
user according to the specific goals, emotional
reactions and action tendencies defined as the
internal state of the VA.
The detection and appraisal of the events
produced in the VA’s environment lead to the
selection of specific dialogues which are jointly used
with some facial expressions to display the
emotional behaviour in the VA. When an event is
appraised as desirable for the VA (e.g. the daily
logging of the user into the system facilitating the
VA’s goal related to maintain a good level of
adherence in the patient) or desirable for the
patient’s well-being (e.g. good self-reports about
moods or thoughts) positive emotions are generated
in the VA. These emotions will disclose specific
utterances that complement the VA’s feedback
dialogues such as “Thanks for logging in today, I am
happy to see you again” or “Great! I‘m glad to hear
that”. Negative emotions are produced when the
detected events are appraised as not desirable for the
VA or the patient, which in turn produce feedback
such as “I’m sorry to know that” or “That’s not
really good”.
The displaying of negative emotions when
interacting with people recovering from depression
should be addressed carefully. In this sense, one of
the research lines proposed in this PhD is an
extension of the current implemented cognitive-
emotional module to better cope with the negative
situations reported or detected in the patient. A key
difference in the empathic behaviour of the
Help4Mood‘s VA regarding the original application
of FAtiMA is that the empathic responses (aimed to
be displayed through the dialogue content and some
facial expressions) needs to be modulated according
to the special characteristics of the target users. Our
VA must not display a “pure emotional” empathic
behaviours by adopting the same typically negative
mood of the patient. The disadvantage is that these
behaviours can be interpreted as sympathetic
expressions of condolence that may imply a sense of
unintended agreement with the patients (negative)
views (Clark, 2007). What is most beneficial from a
clinical perspective is not to produce “only” natural
empathic reactions as response to the patient’s input,
but to generate therapeutic-empathy responses in the
agent.
It is important to distinguish natural empathy
(experienced by people in everyday situations) from
therapeutic empathy in order to provide the patients
with useful feedback for their particular condition.
One of the differences between natural and
therapeutic empathy is the “addition of the cognitive
perspective-taking component to the emotional one;
the cognitive component helps the therapist to
conceptualize the client’s distress in cognitive
terms” (Thwaites, 2007). That means that a therapist
should “assume both the role of an emotional
involvement in an interview with a patient and an
ICAART2014-DoctoralConsortium
50
emotional detachment that allows for a more
objective appraisal” (Clark, 2007).
The extension proposed for the VA’s cognitive-
emotional module is focused in the modelling of a
perspective-taking component aimed to produce in
the VA the required emotional detachment or
emotional distance at specific stages of the
interaction with patients with major depression. The
main idea is the implementation of some strategies
for emotion regulation as defined in (Gross, 2007).
One of these strategies is the cognitive change
(through the re-appraisal process) used to assess
with a different (more positive) perspective a
particular event. This reappraisal mechanism will be
integrated as an extension of the FAtiMA
architecture.
When a new event is received from the
environment a prospective appraisal will be
executed to assess if the event derives from a
desirable or undesirable situation in terms of the
VA’s goals. The result of this prospective appraisal
is the projection of the potential emotional state
produced by this event. In other words, our model
“simulates” the appraisal and affect derivation
processes to analyse the emotional consequences of
the current situation, but without producing the full-
blown emotional responses. If the projected
emotional state includes the activation of a negative
emotion with intensity greater than a pre-defined
maximum threshold, the corresponding pre-defined
alternative event(s) is selected for reappraisal which
would construct a more positive meaning of the
original situation.
An example of this process is when the patient is
reporting a low mood during the today session. The
VA can appraise this event as highly undesirable for
the patient’s condition generating a strong negative
emotion. The new reappraisal component can
change the meaning of this situation using an
alternative view. In the example, the VA can analyse
the results obtained in the mood questionnaire
during previous sessions (stored in the model of the
patient) and check whether these results show a
positive tendency in the patient’s condition during
the past days. If a positive tendency is found, the
original event would be reappraised as “not much
undesirable” to the patient (thought the current level
of patient’s mood is not the optimal). This
reappraisal can change the emotional state or the
emotion’s intensity in the VA which is reflected in
the feedback provided to the patient, something like
“Ok, it seems that your current mood is not very
good, but in general terms you are making good
progresses in the last days”.
This proposed extension of the emotional responses
is expected to improve the VA-patient interaction
and increase the patient engagement, and therefore
contribute with the adherence to the treatment.
5.3 Clinical Pilots
There are planned 3 incremental pilots (see Table 1)
to evaluate the Help4Mood system in three
European clinical centres: (1) The Clinical Centre of
Psychology and Psychotherapy at the University of
Babes-Bolyai (Cluj-Napoca), (2) the Health
Foundation of Sant Joan de Deu (Llobregat,
Bacelona), and (3) the Centre for Population Health
Sciences, University of Edinburgh (Edinburgh, UK).
Table 1: Help4Mood pilots.
Pilot Country Patients Tasks Days
1 Edinburgh 5 1 7
2 Cluj-Napoca 4 5 15
3 Catalonia >10 >5 >15
3 Edinburgh >10 >5 >15
3 Cluj-Napoca >10 >5 >15
The first and second one has already been
performed, the third one is under development and it
is planned the first semester of 2014. The last pilot
will include the new developments that are described
in this paper. So the final testing results will evaluate
the work carry out in this PhD Thesis.
At the end of each pilot the clinicians administer
a personal interview to the patients in order to obtain
data about acceptability for each of the system’s
components.
5.4 Statistical Analyses
The gathering data from all these pilots will be
analysed to test our main hypothesis and study 3
factors: (1) system usage, (2) system engagement,
and (3) adherence to the treatment. .
A clinical requirement is that the system must be
used daily, so we can check in system logs the
patient logins in order to obtain the system usage.
Additionally, clinicians set the minimal and maximal
executions of each task to be offered to the user. In
the first pilot, only one task was configured, which
should be performed once per day during the seven
days of the system’s use. In the second pilot,
clinicians establish 5 tasks (see Table 2). In order to
obtain the adherence to the treatment, we calculated
the ratio between the maximal executions
established by clinicians with the number of tasks
completed by the user using the system.
LeveragingAdaptiveSessionsBasedonTherapeuticEmpathyThroughaVirtualAgent
51
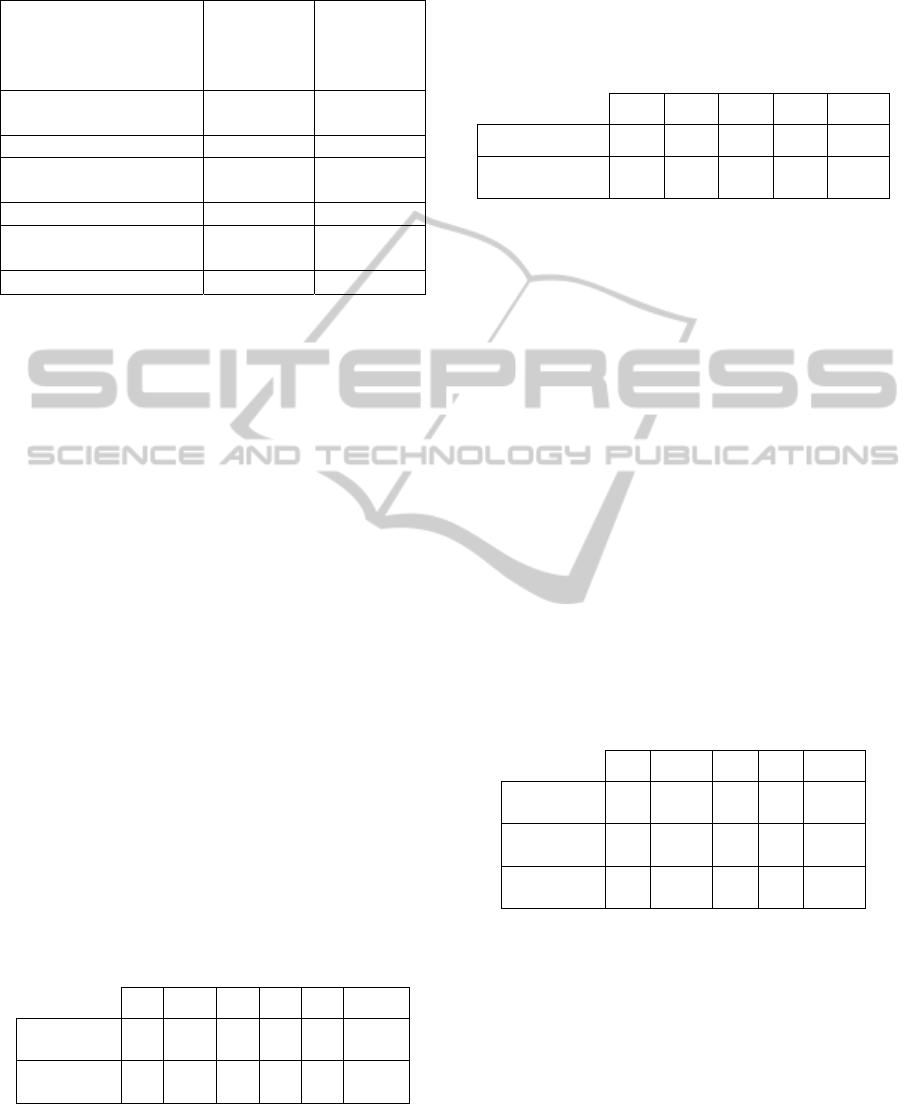
Table 2: Minimum and Maximum number of weekly
executions in each task during the second pilot.
Task
Minimum
number of
executions
per week
Maximum
number of
executions
per week
Daily Mood Check
Questionnaire
7 7
Speech Activity 3 5
Patient Health
Questionnaire (PHQ-9)
1 1
Sleep Questionnaire 0 7
Negative Thought
Questionnaire
3 7
Total 14 27
System engagement is measured based in the
length (Long, Medium, Short) of the daily session
selected by the patient. The choice of long sessions
suggests greater involvement and motivation. On the
other hand, the selection of short sessions suggested
little engagement and commitment.
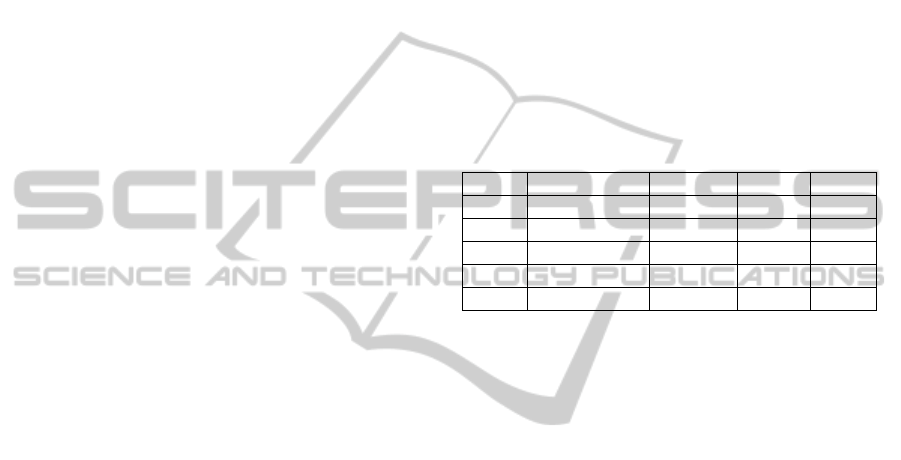
5.5 Initial Outcomes
The system was tested in two incremental pilots. The
first one was carried out in Edinburg during 7 days
with 5 patients in 2013. In this version, the system
only offered a Daily Mood Check questionnaire.
The results of this first pilot (see Table 3)
showed a 100% of system usage and treatment
adherence in 4 patients, and 71% in one patient. The
results related with the treatment adherence are the
same than the results of system usage due that only
one task was possible to be used. If the patient
accessed the system, he performed the activity. If
not, he could not do the task and he could not get it
back another day. In this first pilot it was not
possible to clearly measure the patient engagement
due to the same reason that only one task was
proposed every day, so the patient was not offered
with the selection of the session’s length.
Table 3: Assessment of the patient system usage (%) and
adherence to the treatment (%) in pilot 1.
P1 P2 P3 P4 P5 AVG
System
usage
1 0.71 1 1 1 0.942
Treatment
Adherence
1 0.71 1 1 1 0.942
The second pilot was carried out in Cluj-Napoca
during 15 days with 4 patients in 2013. This version
was more complete. The system could plan 5
different tasks and allow the user to select the length
of the sessions. The results for the second pilot are
showed in the following tables:
Table 4: Assessment of the patient system usage (%) and
adherence to the treatment (%) in pilot 2.
P1 P2 P3 P4 AVG
System usage 1 0.6 1 0.87 0.87
Treatment
Adherence
0.77 0.51 0.88 0.72 0.72
In the second pilot, the treatment adherence is
lower than in pilot 1. Patients were requested to
perform a minimum of 28 activities in 15 days and a
maximum of 54 (optimal result that we take as a
reference to calculate the treatment adherence).
Additionally, patients could select the length of the
session that allows us to analyse the patient
engagement to the system (see Table 5). Patient P2
had a low system usage (60%), so adherence was
also low (35%). The patients P1 and P3 got a 100%
use of the system. Regarding adherence, they
presented different results. This is due to the
selection of each patient in the length of the
conducted sessions. P1 selected mainly short
sessions, while P3 selected long sessions. Similarly,
P4 has less system usage than P1 but has almost the
same treatment adherence. That is because P4 has
made many more long sessions than P1, so P4 was
able to complete more tasks.
Table 5: Assessment of the patient engagement (%) in
pilot 2, based on type session selection (long, medium, or
short).
P1 P2 P3 P4 AVG
Long
selection
0.13 0.625 0.7 0.45 0.48
Medium
selection
0.2 0.125 0.2 0.0 0.13
Short
selection
0.66 0.25 0.1 0.54 0.39
The results obtained from these two pilots inform
us about the trends of the use of the system, the
treatment adherence, and patient engagement. The
low number of patients evaluated has been a
limitation of the study. In any case we started to
analyse the correlation between system usage,
treatment adherence and patient engagement. We
expect that the patient engagement can be improved
in order to obtain better results than the results
presented in Table 5 through the new contributions
described in this document. This improvement could
ICAART2014-DoctoralConsortium
52

affect in the treatment adherence even when the
system usage remains low.
Regarding the exit interview of the patient with
the clinician, the results obtained showed different
results. Some patients thought that the system plans
too long sessions, other described that sessions are
appropriate and others that there are too short
sessions.
Additionally, the patients of the pilot 2 were
asked about how much empathic was the virtual
agent. Two patients thought that the VA was
empathic and correct. In contrast, the third patient
answered that sometimes the VA was not really
empathic.
6 EXPECTED OUTCOME
The new contributions described in this document
(extension of the Session Planner and Cognitive-
Emotional module) will be implemented and
evaluated in the final pilot. We expect to obtain
more data that allow us to asset better conclusions
about the patient engagement and adherence
regarding our developed system.
In the long run, future pilots should include
patients control groups in order to compare the
obtained results between those patients that used the
system and those patients with the treatment that
does not include the use of the system. This would
help to conclude whether the use of our system
influenced and improved the adherence to the
treatment.
ACKNOWLEDGEMENTS
This paper reflects only the author’s views. The
European Community is not liable for any use that
may be made of the information contained herein.
This research is carried out within the EU FP7
Project “Help4Mood – A Computational
Distributed System to Support the Treatment of
Patients with Major Depression” [FP7-ICT-2009-
4; 248765].
REFERENCES
Andrist S., Leite I., Lehman J. 2013. Fun and fair:
influencing turn-taking in a multi-party game with a
virtual agent. In Proceedings of the 12th International
Conference on Interaction Design and Children
(IDC'13) pp., 352-355, New York.
Bernardini S., Porayska-Pomsta K., Sampath H. 2013.
Designing an Intelligent Virtual Agent for Social
Communication in Autism. Proceedings of the Ninth
AAAI Conference on Artificial Intelligence and
Interactive Digital Entertainment. pp. 9-15.
Bickmore T., Gruber A., Intille S., Mauer D. 2006. A
Handheld Animated Advisor for Physical Activity
Promotion. In American Medical Informatics
Association Annual Symposium, Washington, DC.
Bickmore T., Pfeifer L. 2008. Relational Agents for
Antipsychotic Medication Adherence. CHI'08
workshop on Technology in Mental Health Florence,
Italy.
Bresó, A. 2013. MSc Thesis: Generic Data Processing &
Analysis Architecture of a Personal Health System to
Manage Daily Interactive Sessions in Patients with
Major Depression. http://personales.upv.es/
adbregua/docs/A_Breso.pdf.
Brinkman W. P., van der Mast C. A. P. G., de Vliegher D.
2008. Virtual Reality Exposure Therapyfor Social
Phobia: A Pilot Study in Evoking Fear in a Virtual
World. In Proceedings of HCI2008 Workshop – HCI
for Technology Enhanced Learning. Liverpool, UK.
Castellano G., Paiva A., Kappas A., Aylett R., Hastie H.,
Barendregt W., Nabais F., Bull S. 2013. Towards
Empathic Virtual and Robotic Tutors. In Artificial
Intelligence in Education Lecture Notes in Computer
Science Volume 7926, pp 733-736.
Clark, A. J. 2007: Empathy in Counseling and
Psychotherapy. Perspectives and Practices. Lawrence
Erlbaum Associates.
Coombs, T., Deane, F. P., Lambert, G., & Griffiths, R.
2003. What influences patients’ medication
adherence? Mental health nurse perspectives and a
need for education and training. International journal
of mental health nursing, 12(2), 148-152.
Core M., Traum D., Lane H. C., Swartout W., Gratch J.,
van Lent M., Marsella S. 2006. Teaching Negotiation
Skills through Practice and Reflection with Virtual
Humans. Simulation Vol. 82(11), pp. 685–701.
Delamater A, 2006. Improving Patient Adherence.
Clinical Diabetes, vol. 24 no. 2 71-77.
Dias, J, Mascarenhas, S, & Paiva, A. 2011. Fatima
modular: Towards an agent architecture with a generic
appraisal framework. In Proceedings of the
International Workshop on Standards for Emotion
Modeling.
DiMatteo, M. R., Sherbourne, C. D., Hays, R. D., Ordway,
L., Kravitz, R. L., McGlynn, E. A., ... & Rogers, W.
H. 1993. Physicians' characteristics influence patients'
adherence to medical treatment: results from the
Medical Outcomes Study. Health psychology, 12(2),
93.
Dolder C. R., Lacro J. P., Leckband S., Jeste D. V., 2003.
Interventions to improve antipsychotic medication
adherence: review of recent literature. J Clin
Psychopharmacol; 23:389-99.
LeveragingAdaptiveSessionsBasedonTherapeuticEmpathyThroughaVirtualAgent
53

Donovan J. L., 1997. El paciente como decisor.
Utilización racional de medicamentos. International
Journal of Technology Assessment in Health Care (2ª
parte). Series divulgativas, documento nº 2, Sociedad
Española de Farmacéuticos de Atención Primaria
(SEFAP).
Gebhard P., Schröder M., Charfuelan M., Endres C., Kipp
M., Pammi S., Rumpler M., Türk O. 2008.
IDEAS4Games: Building Expressive Virtual
Characters for Computer Games. Proceedings of th 8th
International Conference on Intelligent Virutal
Agents, H. Prendinger, J. Lester and M. Ishizuka
(Eds.): LNAI 5208, pp. 426-440.
Gilden J, Staring A.B.P, Van der Gaag M, Mulder C.L,
2011. Does Treatment Adherence Therapy reduce
expense of healthcare use in patients with psychotic
disorders? Cost-minimization analysis in a randomized
controlled trial. Schizophrenia Research, vol. 133, no.
1–3, pp. 47–53.
Gross, J. J., & Thompson, R. A. 2007. Emotion regulation:
Conceptual foundations. Handbook of emotion
regulation, 3, 24.
Katon, W., Robinson, P., Von Korff, M., Lin, E., Bush, T.,
Ludman, E., & Walker, E. 1996. A multifaceted
intervention to improve treatment of depression in
primary care. Archives of General Psychiatry, 53(10),
924.
Kenny P., Parsons T., Gratch J., Leuski A., Rizzo A. 2007.
Virtual Patients for Clinical Therapist Skills Training.
7th International Conference on Intelligent Virtual
Agents, pp. 197-210, Paris France.
Krijn M., Emmelkamp P. M. G., Olafsson R. P., Biemond
R. 2004. Virtual reality exposure therapy of anxiety
disorders: A review. Clinical Psychology Review, Vol.
24(3) pp.259-281.
Lazarus, R. S. 1991. Emotion and adaptation (p. 557).
New York: Oxford University Press.
Lin, E. H., Von Korff, M., Ciechanowski, P., Peterson, D.,
Ludman, E. J., Rutter, C. M., & Katon, W. J. 2012.
Treatment adjustment and medication adherence for
complex patients with diabetes, heart disease, and
depression: a randomized controlled trial. The Annals
of Family Medicine, 10(1), 6-14.
Lincoln TM, Wilhelm K., Nestoriuc Y. 2007.
Effectiveness of psychoeducation for relapse,
symptoms, knowledge, adherencie and functioning in
psychotic disorders: a meta-analysis. Schizophr Res;
96:2232-45.
Márquez E, Casado JJ, Márquez JJ. 2001. Estrategias para
mejorar el cumplimiento terapéutico. FMC; 8:558-73.
Martínez-Miranda J., Jung B., Payr S., Petta P. 2008. The
Intermediary Agent’s Brain: Supporting Learning to
Collaborate at the Inter-Personal Level. In
Proceedings of the 7th. Conference on Autonomous
Agents and Multiagent Systems AAMAS'08, Volume 3,
pp. 1277 – 1280 IFAAMAS.
Mateas M., Stern A. 2003. Façade: An experiment in
building a fully-realized interactive drama. In Gama
Developers Conference, Game Design Track.
Neil, A. L., Batterham, P., Christensen, H., Bennett, K., &
Griffiths, K. M. 2009. Predictors of adherence by
adolescents to a cognitive behavior therapy website in
school and community-based settings. Journal of
Medical Internet Research, 11(1).
Orueta R. 2005. Estrategias para mejorar la adherencia
terapéutica en patologías crónicas. Inf Ter Sist Nac
Salud; 29(2):40-8.
Osterberg L, Blaschke T. Adherence to medication. N
Engl J Med 2005; 353(5):487-97.
Pampallona, S., Bollini, P., Tibaldi, G., Kupelnick, B., &
Munizza, C. 2002. Patient adherence in the treatment
of depression. The British Journal of Psychiatry,
180(2), 104-109.
Pontier M., Siddiqui G. A. 2008. Virtual Therapist That
Responds Empathically to Your Answers. Intelligent
Virtual Agents, pp. 417-425.
Raij A., Johnsen K., Dickerson R., Lok B., Cohen M.,
Duerson M., Pauly R., Stevens A., Wagner P., Lind D.
2007. Comparing Interpersonal Interactions with a
Virtual Human to Those with a Real Human.
Visualization and Computer Graphics, IEEE
Transactions 13(3), pp. 443-457.
Rigueira AI. 2001. Cumplimiento terapéutico: ¿qué
conocemos de España? Aten Primaria; 27(8):559-68.
Rizzo, Albert; Joseph, Brennan J. 2011. Psychology
Today. Virtual Reality, A New Therapy Part Two: The
SimCoach.
Sabatâe, E. 2003. Adherence to long-term therapies:
evidence for action. World Health Organization.
Safford, S. M., & Worthington, J. E. 1999. Computer
anxiety in individuals with serious mental illness.
Computers in human behavior, 15(6), 735-745.
Safren, S. A., O’Cleirigh, C. M., Bullis, J. R., Otto, M. W.,
Stein, M. D., & Pollack, M. H. 2012. Cognitive
Behavioral Therapy for Adherence and Depression
(CBT-AD) in HIV-Infected Injection Drug Users: A
Randomized Controlled Trial. Journal of Consulting
and Clinical Psychology, 80(3), 404-415.
K. R. Scherer, A. Schorr, and T. Johnstone (Eds.).
Appraisal Processes in Emotion: Theory, Methods,
Research. Oxford University Press, 2001.
Sotoca-Momblona J. M., Codina-Jané C. 2006. Cómo
mejorar la adherencia al tratamiento. JANO; 1605:39-
40.
Staring A. B. P., Mulder C. L., Van der Gaag M., Selten J.
P., Loonen A. J. M., Hengeveld M. W. 2006.
Understanding and improving treatment adherence in
patients with psychotic disorders; a review and a
proposed intervention. Curr Psychiatry Rev; 2: 487–
94.
Staring ABP, Van der Gaag M, Koopmans G. T, Selten J.
P, Van Beveren J. M, M. W. Hengeveld M. W,
Loonen A. J. M, Mulder C. L. 2010. Treatment
adherence therapy in people with psychotic disorders:
randomised controlled trial.BJP, 197:448-455.
Tartaro A., Cassell J. 2008. Playing with Virtual Peers:
Bootstrapping Contingent Discourse in Children with
Autism. Proceedings of International Conference of
the Learning Sciences (ICLS), Utrecht, Netherlands.
ICAART2014-DoctoralConsortium
54

Thwaites, R., Bennett-Levy, J.: Conceptualizing Empathy
in Cognitive Behaviour Therapy: Making the Implicit
Explicit. Behavioural and Cognitive Psychotherapy,
35, pp. 291-612 (2007).
Thompson, L., & McCabe, R. 2012. The effect of
clinician-patient alliance and communication on
treatment adherence in mental health care: a
systematic review. BMC psychiatry, 12(1), 87.
Titov, N., Dear, B. F., Johnston, L., Lorian, C., Zou, J.,
Wootton, B. & Rapee, R. M. 2013. Improving
adherence and clinical outcomes in self-guided
internet treatment for anxiety and depression:
randomised controlled trial. PloS one, 8(7), e62873.
Van Dulmen, S., Sluijs, E., van Dijk, L., de Ridder, D.,
Heerdink, R., & Bensing, J. 2007. Patient adherence to
medical treatment: a review of reviews. BMC health
services research, 7(1), 55.
Vergouwen, A. C., Bakker, A., Katon, W. J., Verheij, T.
J., & Koerselman, F. 2003. A systematic review of
interventions. Adequate follow-up can’t be optional,
64, 21.
Vittengl J. R., Clark L. A., Dunn T. W. Jarrett R. B. 2007.
Reducing relapse and recurrence in unipolar
depression: A comparative meta-analysis of cognitive
behavioral therapy's effect. J Consult Clin Psychol 75:
475-488.
WHO, 2012. Global burden of mental disorders and the
need for a comprehensive, coordinated response from
health and social sectors at the country level.
http://apps.who.int/gb/ebwha/pdf_files/EB130/B130_9
-en.pdf.
Yasavur U., Lisetti, C., Rishe N. 2013. Modeling Brief
Alcohol Intervention Dialogue with MDPs for
Delivery by ECAs. Intelligent Virtual Agents. Lecture
Notes in Computer Science Volume 8108, pp 92-105.
Yildiz, M., Veznedaroglu, B., Eryavuz, A., & Kayahan, B.
2004. Psychosocial skills training on social
functioning and quality of life in the treatment of
schizophrenia: A controlled study in Turkey.
International journal of psychiatry in clinical practice,
8(4), 219-225.
Zygmunt A., Olfson M., Boyer C. A., Mechanic D., 2002.
Interventions to improve medication adherence in
schizophrenia. Am J Psychiatry; 159:1653-64.
LeveragingAdaptiveSessionsBasedonTherapeuticEmpathyThroughaVirtualAgent
55
