
Development and Testing of a Modular Upper Extremity Exoskeleton
for Infants
Tariq Rahman
1
, Cole Galloway
2
, Elena Kokkoni
2
and Michele Lobo
2
1
Department of Biomedical Research, Nemours/A.I. duPont Hospital for Children, Wilmington, Delaware 19899 U.S.A.
2
Department of Physical Therapy, University of Delaware, Nerwark, Delaware 19716 U.S.A.
Keywords: Orthosis, Upper Extremity, Exoskeleton, Motor Control, Infants.
Abstract: A passive upper extremity exoskeleton has been developed for people with neuromuscular weakness. The
WREX (Wilmington Robotic EXoskeleton) has been used successfully for a number of years by people
with disabilities such as muscular dystrophy and arthrogryposis. This paper describes the modification of
the WREX to be fitted with infants. The Pediatric WREX Plus (P-WREX+) can selectively assist or resist
antigravity arm movements based on the needs of each individual. It consists of a 3-D printed device that
can be mounted to a jacket or a chair and allows infants more access to their environment by augmenting
anti-gravity arm movement. The target population is infants born with brain injuries and at high risk for
significant neuro-motor impairments. The paper describes the development of the device and testing with an
infant with arthrogryposis over a 6-month period.
1 INTRODUCTION
Bioengineered devices for the arms have made
significant advances in the rehabilitation of adults
with nervous system injury. There is a surprising
lack of adaptation of these devices for use in
pediatric populations. This is especially troubling
given the importance of early intervention and
rehabilitation for optimal neurological and
behavioral development. This paper describes the
development of a novel upper extremity orthosis that
is based on the WREX, which is a passive upper
extremity orthosis.
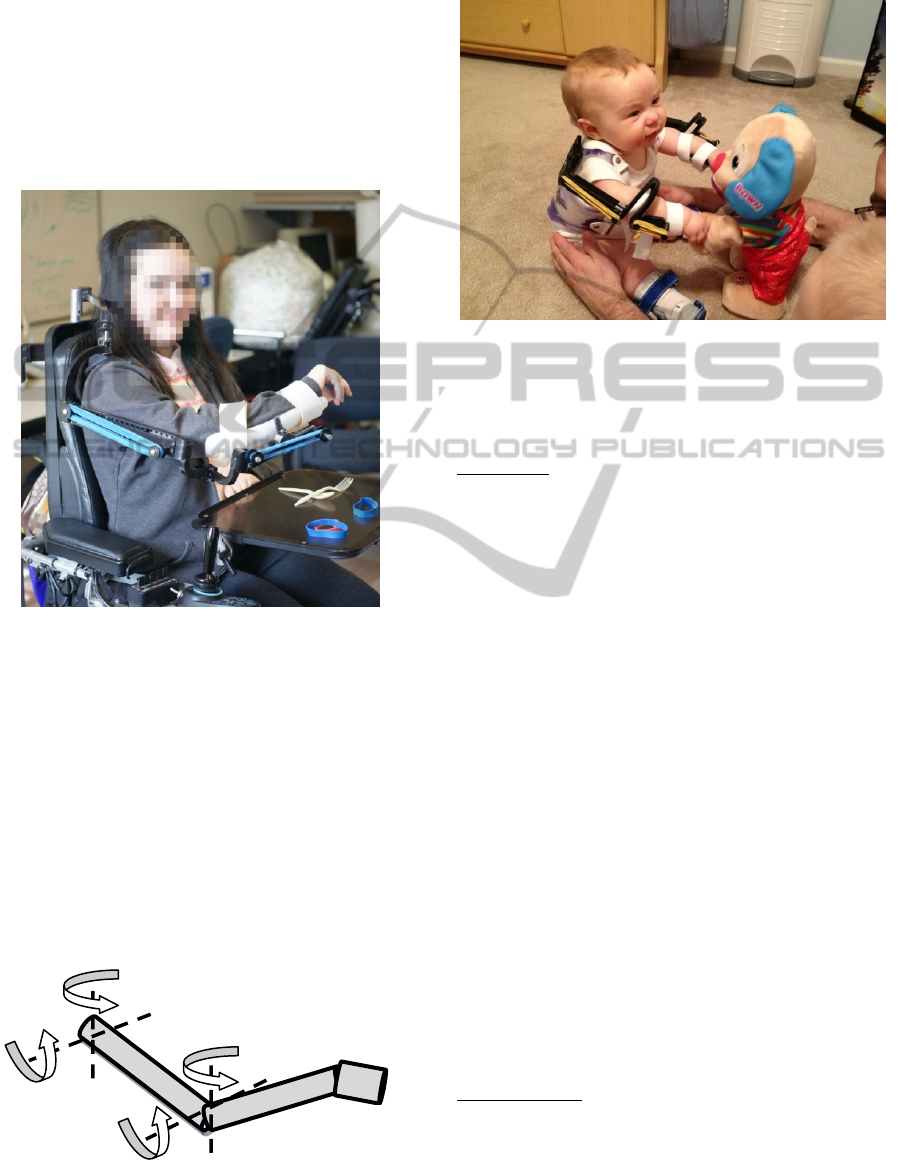
One version of the WREX, figure 1, is a
mechanical linkage that can be attached to a
wheelchair and is powered by elastic bands
(Haumont 2011, Rahman 2007). The device moves
alongside the arm and makes anti-gravity
movements effortless. This is particularly useful for
people with muscular dystrophy and spinal muscular
atrophy where weakness in larger proximal muscles
is evident while distal muscles are less affected. The
WREX allows them to navigate their hand in front
of them and perform activities of daily living. The
WREX comes in one size and can be adjusted to
accommodate different sized individuals and the
number of elastic bands can be changed depending
on the weight of the individual.
A second version of the WREX is made for
smaller children, figure 2. A 3-D printer is used to
fabricate the parts resulting in a lighter and custom
fitted device. Some of the children are able to
ambulate independently therefore require a body-
mounted WREX. We modified a
thoracolumabarosacral orthosis (TLSO) commonly
used for scoliosis treatment.
The WREX has been used successfully in
children older than 2 years of age but has not yet
been used in infants. This paper describes the
experience of using the P-WREX+ for wear and
intervention with an 8-month-old infant with
arthrogryposis multiplex congenita (AMC). Infants
with AMC are born with joint contractures and
muscle tissue fibrosis in more than one region of the
body. Typically the biceps and deltoid muscles are
weak preventing performance of key activities
against gravity.
We wanted to provide this technology in
coordination with intervention to advance the
exploratory and learning abilities of this infant with
special needs. Exoskeletons such as the WREX
advance movement and function in older children
and adults with neuro-motor impairments (Iwamuro
2008, Hesse 2003).
This study is the first to systematically test the
effects of a similar device on reaching ability in an
infant with significant arm movement impairments.
316
Rahman T., Galloway C., Kokkoni E. and Lobo M..
Development and Testing of a Modular Upper Extremity Exoskeleton for Infants.
DOI: 10.5220/0004938003160319
In Proceedings of the International Conference on Biomedical Electronics and Devices (TPDULL-2014), pages 316-319
ISBN: 978-989-758-013-0
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
2 P-WREX+ DEVELOPMENT
The WREX is 4 degrees of freedom, 2-link
mechanism, fig 2, that supports the weight of the
arm for all positions in 3-D space. It is passively
actuated by elastic bands placed on the forearm and
the upper arm links. A four bar mechanism on the
upper arm provides a vertical member at the elbow
during the entire vertical excursion. The stiffness of
elastic bands, and end points are chosen according to
Figure 1: WREX attached to wheelchair.
The P-WREX+ was scaled down in size to fit a 3-8
month old infant. The jacket was also made smaller
and lighter, Fig 3. All the parts of the P-WREX+
were made with ABS plastic. It is inexpensive,
lightweight, portable, adaptable, and easy to use. It
is fabricated by a small, in-house 3-D printer
(Dimension 1200, Stratasys, Eden Prairie, MN)
analysis described in (Rahman, 1995). The resulting
motion provides identical equilibrium for all
position of the arm. This allows an individual to
perform activities of daily living such as eating in a
gravity-free environment. The number of bands can
be varied according to the weight of the subject and
Figure 2: Joint layout of the wrex.
the link lengths can be adjusted for different sized
subjects.
Figure 3: p-wrex+.
3 EXPERIMENTAL PROTOCOL
Participant: We followed an 8-month-old infant
diagnosed with AMC for a 6-month period.
Although he was born with joint contractures, he had
functional passive range of motion at all joints of the
upper extremities at the time he entered the study.
This was the result of early intervention and daily
stretching. His muscle strength for raising his upper
extremities (shoulder flexion) against gravity while
sitting was poor minus. He could perform less than
10 degrees of shoulder flexion against gravity and
only partial range of motion with gravity eliminated.
The assessments were video recorded and later
coded by trained and reliable (>85% reliability)
coders. They recorded times the infant was
contacting the object and times he was looking at the
object
During the baseline period, the infant did not use
the P-WREX+ outside of the brief assessment
periods. During the intervention period, the infant
wore the P-WREX+ daily for an hour while
performing prescribed play activities aimed at
promoting reaching and object manipulation
abilities. During the post-intervention period, the
child kept the P-WREX+ and wore it daily as during
the intervention period but he was no longer
provided the prescribed play activities while wearing
the device
Data Analysis: Results were analyzed via visual
inspection of charted data.
Hand
Shoulder
DevelopmentandTestingofaModularUpperExtremityExoskeletonforInfants
317
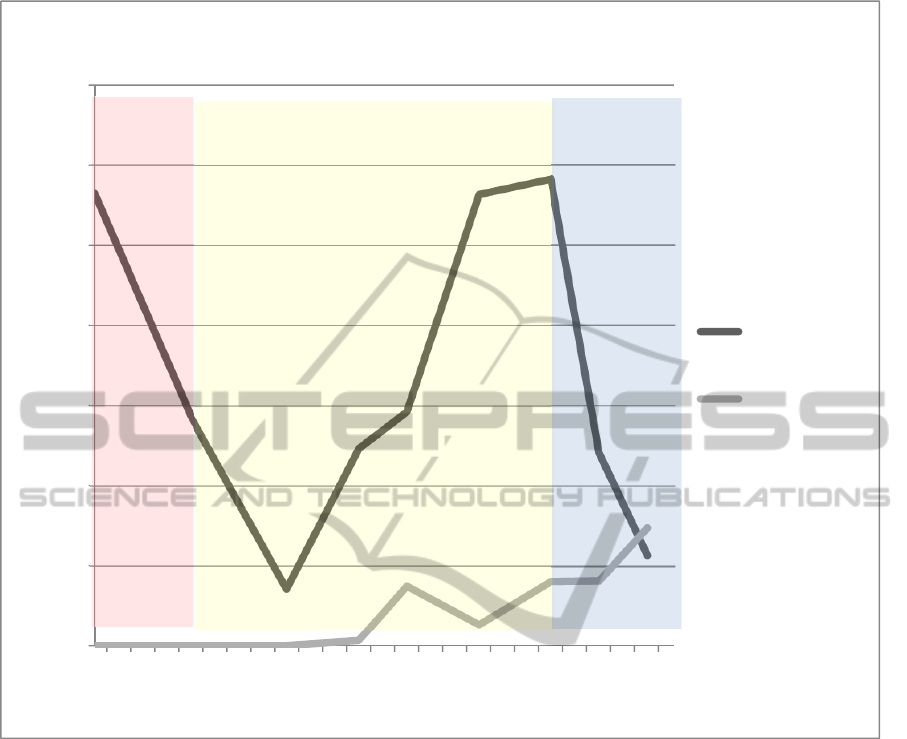
Figure 4: Graph showing the time the toy was contacted by the subject with the WREX.
4 RESULTS
There are several important findings from this
preliminary study. First, the infant was able to safely
and comfortably wear the P-WREX+ daily,
suggesting this and similar devices can successfully
be incorporated into the lives of families with infants
and young children.
Second, the infant was almost always better able
to interact with objects while wearing the P-
WREX+. Interaction with objects is important for
early language, perceptual-motor, social, and
cognitive development and is a precursor for future
essential life skills such as dressing and feeding.
Therefore, devices like the P-WREX+ may be useful
in advancing global development and upper
extremity function.
Third, intervention in combination with use of
the device was more effective at advancing behavior
than was use of the device alone.
This suggests devices like the P-WREX+ have
strong potential to advance development and
function when paired with play activities prescribed
by an early intervention expert.
Finally, the infant showed improved ability to
interact with objects, figs 4,5, throughout the study
even when he was not wearing the device. This
suggests devices like the P-WREX+ are not only
successful assistive devices that improve function
when worn, but that they may also be successful
rehabilitation tools that result in behavioral advances
even after they are doffed.
Future goals for this research program include:
1) determining the impact of the P-WREX+
for infants, children, and adults with a variety of
0
10
20
30
40
50
60
70
1 4 7 1013161922
PercentTime
WeekinStudy
TotalTimeContactingtheToy
P‐WREX+ON
P‐WREX+OFF
Intervention
Post‐
Interventio
n
Baseline
BIODEVICES2014-InternationalConferenceonBiomedicalElectronicsandDevices
318
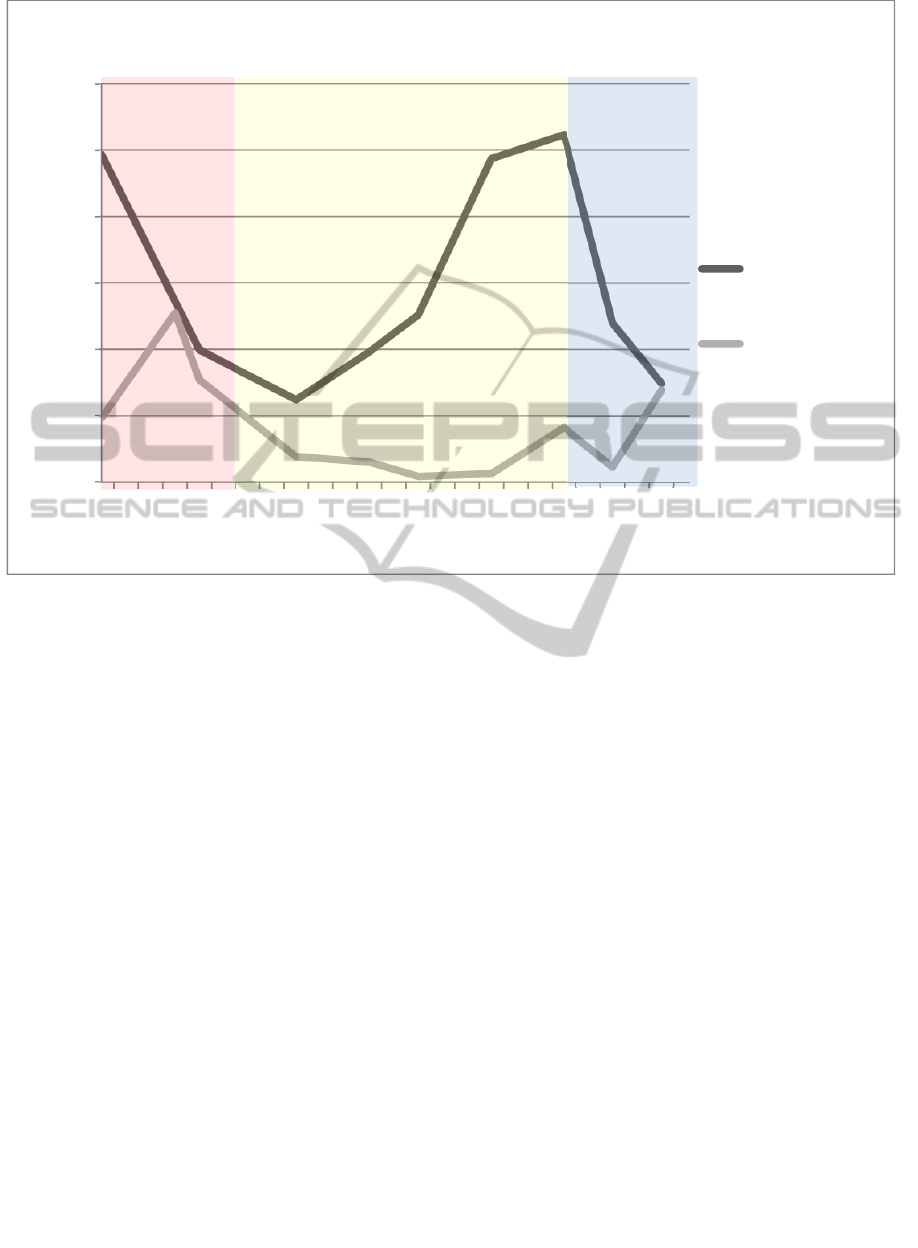
Figure 5: Graph showing the time the toy was contacted while looking at it by the subject with the WREX.
diagnoses impacting arm movement, such as brain
injury, brachial plexus palsy, and stroke, and, 2)
exploring both low-tech and high-tech future
adaptations of the device.
ACKNOWLEDGEMENTS
We would like to thank Mr Whitney Sample for
construction of the p-WREX+ and the Nemours
foundation for funding.
REFERENCES
Iwamuro, B.T., Cruz E.G., Connelly L.L., Fischer H.C.,
Kamper D.G., 2008. Effect of a Gravity-Compensating
Orthosis on Reaching After Stroke: Evaluation of the
Therapy Assistant WREX. Archives of Physical
Medicine and Rehabilitation. Nov;89(11):2121-2128.
Hesse S., Schmidt H., Werner C., Bardeleben A. 2003.
Upper and lower extremity robotic devices for
rehabilitation and for studying motor control. Current
Opinion in Neurology. Dec;16(6):705-710.
Haumont T., Rahman T., Sample W., King M., Church C.,
Henley J., Jayakumar S. 2011 “Wilmington robotic
exoskeleton: a novel device to maintain arm
improvement in muscular disease” J Pediatr Orthop.
31(5):e44-9. Jul- Aug.
Rahman T., Sample W., Seliktar R., Clark A.., Scavina
M., Moran K., Alexander M. 2007 “Design and
Testing of a Functional Arm Orthosis in Patients with
Neuromuscular Diseases”. Transactions of the IEEE
on Neural Systems and Rehabilitation Engineering.
Vol 15, No 2,
Rahman T., Ramanathan R., Seliktar R., Harwin W., 1995
"A Simple Technique to Passively Gravity-Balance
Articulated Mechanisms" Trans. of the ASME- J of
Mechanical Design, Vol. 117, No 4, pp. 655-658.
0
10
20
30
40
50
60
1 5 9 13 17 21
PercentTime
WeekinStudy
TotalTimeContactingToyWhileLookingAtIt
P‐WREX+ON
P‐WREX+OFF
Intervention Post‐
Interventio
n
Baseline
DevelopmentandTestingofaModularUpperExtremityExoskeletonforInfants
319
