
Provision of Personalized Data via Mobile Web Services in eHealth
Scenarios
Marc Jansen
1,2
, Abbas Siddiqui
1
and Oliver Koch
1
1
Computer Science Institute, University of Applied Sciences Ruhr West, Bottrop, Germany
2
Department of Media Technology, Linnaeus University, Växjö, Sweden
Keywords: Personalized Data, Context-awareness, Service Provision, Service Consumption, Middle-ware, eHealth,
mHealth.
Abstract: In societies where the demographic change leads to a more and more unbalanced state between the elderly
and all other different age groups, there, health management becomes one of the most significant problems,
e.g., in order to allow what is often called successful aging. Ubiquitous use of smart mobile devices enables
gathering of personalized data enriched with contextual information. This information can ideally be used in
modern eHealth scenarios, resulting in mobile health (mHealth) scenarios. This paper describes how highly
personalized and sensitive information, such as vital signs enriched with contextual information of a patient,
can be stored at mobile devices and provided via modern web technologies for later-on analysis and health
monitoring. Therefore, this paper presents a number of different scenarios in which such mobile technology
provides certain benefits, discusses benefits, drawbacks and challenges of such an approach and describes
an example implementation of an mHealth scenario.
1 INTRODUCTION
Nowadays, smartphones and other mobile devices
are used tremendously and this trend is still growing
rapidly. Here, the functions of smartphones in use
are much more than simple voice calling and text
messaging. The mobile users use mobile phones to
access their mail accounts, to share their calendars or
to even use their devices as a routing device (i.e., the
ones equipped with the GPS). Therefore, smart
mobile devices collect various information about
their users such as personalized information,
personal/business contacts, messages (emails, short
text messages like SMS, …), social interaction and
social contacts, calling history, work history and
footprints of internet usage (e.g., the browsing
history of a mobile web browser). Additionally, the
set of applications, a user has installed on his device,
provide a rough profile of usage of the device itself.
Two major advantages from the increased usage
of mobile devices are: On the one hand, the devices
are mobile and could therefore ideally be used to
follow their users round the clock and ubiquitously.
And on the other hand, a modern internet connection
is provided with most of the smart mobile devices,
this makes such kind of mobile devices a powerful
and valuable tool. The second reason for the success
of smart mobile devices is, that these devices are
usually equipped with a large set of different
sensors, allowing to contextualize the users’ current
tasks, e.g., by using the GPS sensor of a modern
mobile device, the current position of a user could
also be determined accurately, so that additional
information about the task could be gathered, either
to provide better support to users during the task or
to store additional contextualization data for later
analysis. In addition to GPS sensors, other sensors
like acceleration sensor, motion sensors, a digital
compass and alike, could be used on modern mobile
devices. In the context of eHealth scenarios,
additional sensors for monitoring current vital signs
of the user could be connected to a mobile device.
The idea presented in this paper is twofold, on
the one hand an architecture is presented that allows
to store the data on ones’ own device and not in
some central database. Here we argue that this is a
big advantage (in contrast to modern Cloud
Computing and Web 2.0 scenarios in which more
and more data is stored centrally), having in mind
that health data is always personalized data with a
big demand for security. The second idea is provided
in this paper is to combine vital data (gathered by
441
Jansen M., Siddiqui A. and Koch O..
Provision of Personalized Data via Mobile Web Services in eHealth Scenarios.
DOI: 10.5220/0004949704410446
In Proceedings of the 10th International Conference on Web Information Systems and Technologies (WEBIST-2014), pages 441-446
ISBN: 978-989-758-023-9
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

specialized eHealth sensors connected to a standard
mobile device) and contextualization data (gathered
by standard sensors of a mobile device) and to
provide it in an authentic and secure way, which
without the usage of mobile devices could hardly be
achieved. Additionally, two scenarios are presented
in detail to demonstrate the use of that kind of
technology. For one of the scenarios, an already
existing implementation is described. Here, both on
the implemented middleware and on the client side,
web based technologies have been used in order to
provide a user friendly implementation.
The rest of this paper is organized as follows:
first we provide an overview of related work in the
next section. After this we describe our approach in
section three, followed by a discussion of the
presented approach in section four. Section five
describes two scenarios in which the presented
approach provides benefits and section six describes
the web based implementation of one of these
scenarios. Finally, section seven provides a
conclusion and an outlook to future work.
2 RELATED WORK
Providing Web Services on mobile devices was
probably presented first by IBM (McFadden, et al.,
2003). In this work a solution is presented for a
specific scenario in which Web Services are hosted
on mobile devices. A more general approach for
providing Web Services on mobile devices is
presented in (Srirama, et al., 2006 and AlShawan, et
al., 2010). In (Li and Chou, 2011) the authors
suggest a different approach, focusing on the
optimization of the HTTP protocol for mobile Web
Services provisioning. Importantly, none of the
mentioned approaches manages to overcome certain
limitations of mobile devices, e.g., permanently
changing networks, IP addresses from networks with
network address translation (NAT) or the fact that
mobile devices are usually not designed to be always
online (might be switched off, might have not
network connection, …).
An additional approach that manages to
overcome these problems, is presented in (Jansen,
2013a). This approach utilizes a central proxy
infrastructure, that allows on the one hand to tackle
the mentioned challenges and on the other hand
provides a stable infrastructure for mobile device to
provide standardized Web Services. Furthermore,
the central proxy provides the major part of the
technical infrastructure that allows to use
standardized protocols for the deployed Web Service
at the mobile devices.
Additionally, the work presented in (Jansen,
2013b) argues for a new perspective to Web
Services especially if those services are deployed to
mobile devices. Here, the author argues that one of
the major benefits of mobile devices is the fact that
they are mobile. In connection especially to mHealth
scenarios, this fact allows to gather different kinds of
data from the sensors of a mobile devices that allows
to easily contextualize the user (in most mHealth
scenarios, the patient) in his/her current
task/situation.
3 APPROACH AND DISCUSSION
The approach we used for the implementation of the
example scenarios is based on a standardized Web
Services. As already explained, a number of
different approaches exist that allow the provision of
Web Services on mobile devices. Since from our
point of view, the approach described in (Jansen,
2013a), solves the most pressuring problems, we
decided to base our implementation on this
approach.
In addition to this, we implemented a
middleware layer allowing a loose coupling between
the provider of the mobile Web Services and the
consumer service in our case a web-based
application that visualizes the data measured by
different sensors and in different training sessions.
Another advantage of the approach described in
(Jansen, 2013a) is that it allows to store requests at
the central proxy, e.g., if the device that provides the
mobile Web Service is not connected to a network.
As soon as the device is connected again, the request
could be performed by the device and the result is
available for the client.
Additionally, this approach implements Web
Services for mobile devices based on standardized
protocols, so that developers who are familiar in
using Web Services do not need to learn a whole
new technology, but can rely on knowledge they
already have. Furthermore, also on the mobile Web
Service provider side, the approach utilizes
annotations pretty much in the same way as for the
implementation of Web Service on non-mobile
devices, providing again a very flat learning curve
for the new technology.
The chosen approach provides a number of
benefits, e.g., since the measured eHealth data only
remains on the mobile device of the patient, there is
no need for a central server infrastructure. This
results in lower management costs, easier to achieve
WEBIST2014-InternationalConferenceonWebInformationSystemsandTechnologies
442

security and no additional costs for central backups.
Additionally, there is no need for central personnel,
space, hardware and software provisioning and no
central costs for energy.
On the other hand, this de-centralized approach
also provides some drawbacks. Since the data is not
stored centrally, hence, no central backup strategy is
applicable, but the patient him-/herself is responsible
for his/her data. Also security management would be
easier to accomplish in an architecture with central
data storage. Additionally, new questions with
respect to the security of the data come into play
while the data remains on mobile devices: what
happens if the device gets lost or stolen? Therefore,
of course, the personal data should be stored
encrypted on the device of the patient. Still,
encryption would just solve the problem of privacy
(no one else but the owner of the mobile device
would be able to access the data), but not the
problem of availability of the data. Once the device
is no longer in reach of its owner, the data would no
longer be accessible for future analysis.
Besides the challenges that come from the
described drawbacks, an additional challenge comes
into play considering the target group for this kind of
mHealth applications. The usual target group for this
kind of applications consists of elderly. Since this
target group is usually not specifically well used to
handle mobile devices, a clear and precise
explanation of the necessary steps and the used
technology is more than ever necessary.
4 TWO EHEALTH SCENARIOS
Key strengths of mHealth system architectures based
on mobile Web Services encompass the following
aspects:
1. On-demand transmission of data to Health
professionals: the doctor receives only the
data that really interests him and especially at
the point in time he is interested in.
2. Data remains in the direct disposal area of the
patient: the need for informational self-
determination is thus optimally fulfilled.
The following two scenarios, describe the use of
Web Service based mHealth applications by
illustrating the two aforementioned strengths.
4.1 Scenario 1: Surgical Preparation
The central source of revenue for hospitals is the
surgical area. This is the actual place where the
decision is taken whether a hospital makes profit or
deficit. Therefore, usually all hospital processes are
aligned to the optimal utilization of the surgical area.
Any delay in the process or even surgeries that need
to be canceled or postponed at short notice, cause a
more or less considerable economic loss.
Prior to surgery, patients usually must follow
certain rules of conduct and take or discontinue
certain medicine for several days or weeks. Has
he/she not done so (e.g., medication for blood
clotting was not discontinued), the sugery has to be
canceled at a short notice. This may lead to an
underutilization of the surgical area and
consequently the associated economic losses.
A 78-year-old patient is to receive a new right
hip joint. She suffers from a lighter hypertension and
type II diabetes. At the same time she tends to water
retention, which manifests in an abrupt increase in
her weight. Normally hip replacement operations
rank among "standard" operations with less risk
involved. But, because of the patients’ secondary
diagnoses, however, there is a significant surgical
risk. Prior to the operation her risk factors must
therefore be closely monitored. To shorten the
period of rehabilitation after the surgery, the patient
should move as much as possible in advance to the
surgery and complete a specific exercise program to
strengthen certain muscle groups.
For several months already, the patient has a
smartphone. At her last doctor's appointment, four
weeks before the surgery, a mobile mHealth
application for collecting and managing various
sensor data (in this case, blood pressure meter, blood
glucose meter and scale connected via bluetooth), is
installed and configured on her mobile phone. The
data is provided via a mobile Web Service, which is
also installed on the device. At the same time the
female patient receives an introduction into a sensor
package that will be handed out to her. Part of the
mHealth application are also information films, in
which the preliminary physical exercises are
provided to her and she gets also informed about the
risks and the progress of the medical intervention.
In the following four weeks, the female patient
regularly measures her blood pressure, blood sugar
and weight. This data is automatically enriched with
location, time, and motion information from her
mobile phones sensors (GPS, accelerometer,
proximity sensor, etc.), allowing to contextualize the
data gathered by the medical sensors.
Thus, noticeable measured values (e.g. increased
heart rate and blood pressure due to sports activities)
can be interpreted, according to the context in which
they are occurred.
ProvisionofPersonalizedDataviaMobileWebServicesineHealthScenarios
443

The data is generated using the internal sensors of
smart phones and possibly even enriched by data
from external web services (e.g. historical weather
data). By using a feedback function, the patient may
give feedback, for example how she felt during the
exercise and the measurements. The logged
feedback and sensor data can be queried by the
hospital on-demand. When retrieving the data the
hospital doctors can decide if they want to get all
data or only aggregated data in terms of a status
report (surgery possible / not possible). In addition,
the mHealth application detects emergency
situations (e.g. very high blood sugar levels) and
alerts the hospital if necessary. The surgical
management can check at any time whether the
surgery will be possible, a change in behavior of the
patient is necessary or an adaptation of the surgical
plan is required.
Even at the stage of rehabilitation the Web
Service on the patient’s smartphone can provide on-
demand information about the patient compliance
(e.g., lack of physical exercise), allowing the timely
intervention of the treating physicians.
4.2 Scenario 2: Regular Data
Measurement by Patients
In the second scenario we imagine a 33 years old
male patient diagnosed of having a genetic disease
that disallows his body to effectively fight against
blood lipids. Therefore, he is likely to have an
increased risk of an attack. In order to lower this
risk, besides a special medication, the patient is
asked to have 24 hours blood pressure measurements
at least once a year. A couple of years ago, this was
more or less unhappy day every year, in which the
patient had to wear a heavy blood pressure monitor
over a whole day. Lately, his doctor told the patient
that with new upcoming technology in the mHealth
sector, the process for 24 hours blood pressure
monitoring could be eased a lot.
By connecting a small and light blood pressure
sensor to his smartphone, the patient is easily able to
collect the necessary data in a convenient way.
Furthermore, by collecting additional data from the
mobile device of the patient, e.g., the current
geolocation and/or the acceleration at which the
patient is currently moving, the gathered data could
be contextualized in order to ease the task for later
analysis.
Happy to know about these new possibilities, the
patient is willing to take his next 24 hours blood
pressure measurements with this new technology.
Two weeks after the measurement was done, the
patient has a new appointment with his doctor in
which the data from the measurement should be
discussed. During this discussion, the doctor
recognizes a tremendous increase in the blood
pressure at 17:03 at the day of the measurement.
First, neither the patient nor the doctor could explain
this increase, but by looking at the contextual data
gathered along the blood pressure values, the reason
for the increase of the blood pressure became clear.
By analyzing the geoposition of the patient and his
acceleration at the time of the increasing blood
pressure, it turned out that the patient was watching
his famous soccer team playing against another local
team. Knowing this, the patient remembers that at
this exact time, the opponents of his famous team
managed to shoot a goal. Being upset about this
event clearly explains the increase in the patients’
blood pressure values.
Again here in this scenario, beside the two major
advantages of on the one hand privacy of the data
(the data remains with the patient and is not stored
centrally) and the just in time provision of the
interesting data to the right person (in this case the
doctor) could easily be seen. Furthermore,
advantages of using modern mobile devices in
mHealth scenarios, like the rich source for the
contextualization of the patient are also obvious.
5 IMPLEMANTATION OF AN
EXAMPLE SCENARIO
The prototype consists of two parts namely Web
Services (i.e., running on a mobile device) and a
web based client (i.e., running in a browser).
The following paragraphs describe the detail
about these aforementioned components of the
prototype followed by the interaction among the
components.
5.1 Mobile Application
Android based mobiles are selected for the
implementation of the concept as according to the
International Data Corporation (IDC) Worldwide
Quarterly Mobile Phone Tracker’s 2013 report,
android based mobiles are the market leaders. An
Android based application is developed to collect the
various sensors data.
There are two categories of sensors, the ones
integrated in a mobile phone and others which are
externally linked via well-known communication
technologies (e.g., Bluetooth, Wi-Fi).
In this particular implementation, the location of
WEBIST2014-InternationalConferenceonWebInformationSystemsandTechnologies
444
a patient is determined by an integrated global
positioning system (GPS), and the speed of
movement is measured by a built-in accelerometer,
which measures the force of acceleration caused by
the gravity or weight to determine the speed. The
standard Android library is used to retrieve the
sensors data.
Besides the integrated sensors, to measure the
heart-rate and, to measure the instant speed of a
patient, a Zephyr sensor (Zephyr HxM BT – Heart
Rate Monitor) is used. The sensor is mounted to a
smart fabric based strap, which must be worn around
the chest. The data is periodically collected via
Bluetooth. The HxM sensor provides a Bluetooth
API to collect the data in a specific message format.
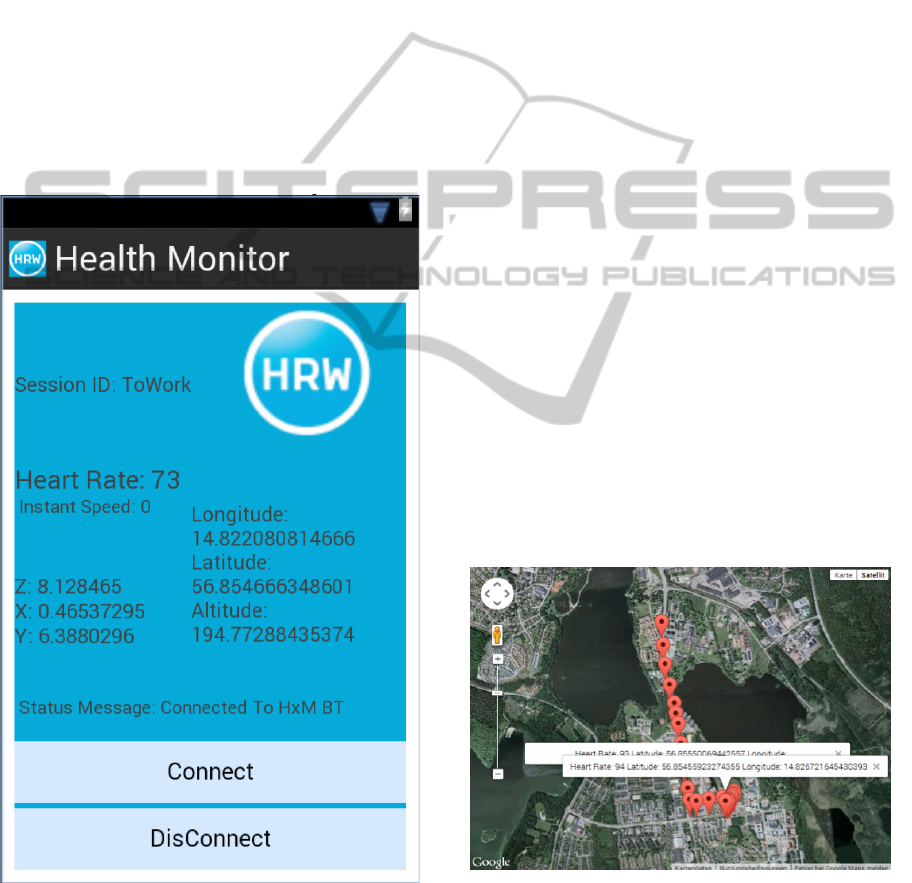
After the collection of the data from all those
aforementioned sensors, the data is saved by the
application shown in Figure 1 to a SQLite database.
Figure 1: A screenshot of the app collecting data from an
mHealth session.
A SQLite database runs without a server, which
makes it a suitable choice for the energy limited
mobile devices. Nevertheless, SQLite data is very
application related and dependent, once an
application is uninstalled then the data will no longer
be available. The database contains two tables
“sessions” and “sensorsData”.
Besides retrieval and storage of the sensors data,
another part of the application handles the incoming
request as a mobile Web Service. It fulfills the
authentic incoming request by sending the stored
data on the device to the client.
5.2 Web Client
The client runs in a browser and can be invoked
from everywhere. Most of the functionality is
implemented in JavaScript and HTML5.
Nevertheless, due to the same origin restriction,
some façade, according to the façade/proxy design
pattern (Gamma, et al., 1995) services needed to be
implemented on the server side. For this
implementation we have chosen PHP.
After a successful authentication (e.g., as a
doctor), the web application sends a Web Service
request to the mobile device of the patient in order to
receive a list of all available sessions. By choosing a
certain session, another Web Service request is send
to the mobile device that receives the data gathered
during this session. This data could then be
visualized in a tabular format or as a representation
in a Google Map, where, e.g., the data is located at
the correct geoposition and different parts of the data
could be visualized according to the geoposition at
which they appeared. An example of the visual
representation on the client side in a Google Map
could be seen in Figure 2.
Figure 2: Visual representation of gathered health data in a
Google Map.
5.3 How All Work Together
The functionality of the prototype is described from
ProvisionofPersonalizedDataviaMobileWebServicesineHealthScenarios
445

the two different perspectives namely a user (e.g., a
patient), and a user of the collected data such as a
general physician, a family member or patient
himself.
From the mobile-health-moniters’ user (e.g., a
patient) perspective, a user starts the application
which collects the sensors information on his/her
mobile device. Before starting a new session to
record the sensors data, a user must wear a HxM
chest strap with mounted heart-beat sensor to collect
the real heart-beat of a user, otherwise a default
value (i.e., which is “0” in this case) will be stored.
Once the session is started, every few seconds the
new values from the location sensor, 3-axis
accelerometer and HxM are retrieved and stored in
the “sensorsData table in the “mhealth” database.
Let’s assume, a user started a session during the
workout, once the workout is over, the user decides
to discontinue the session and clicks the disconnect
button, once the session is disconnected a new entry
in the “sessions” table will be stored with start-time
and end-time of the session.
When a concerned person (e.g., a personal
doctor, a family member, a care take, or the
user/patient him-/herself), let’s assume, a house-
doctor wants to know about the patient who is using
the mobile-health-monitoring app. The house-
doctor will enter the web-link in a browser to invoke
the mobile Web Service running on the mobile
device. Before accessing the patients’ data, the
house-doctor must identify him-/herself with
credentials through a username and a password.
After the house-doctor is identified, all the stored
sessions on the patients’ mobile device are retrieved
via the mobile Web Serivce. Now, the house-doctor
can select any session to analyse the measured data.
6 CONCLUSIONS AND FUTURE
WORK
Wrapping up, this paper provides a discussion about
the usage of standardized Web Services on mobile
devices like smartphones in the context of mHealth
scenarios. We provided some example scenarios, a
discussion about the current state of the art and also
about benefits and drawbacks of the presented
approach. Last but not least, a web-based
implementation of one of the example scenarios was
presented.
Nevertheless, beside the obvious benefits of such
an approach, there are also some topics that need to
be considered much more intensively in future
research.
One of the major things to have in mind, is the
security of the data on the phone of a patient. More
likely, data security (especially data privacy) could
be much easier realized for a central database (i.e.,
administrated by IT specialists). On the other hand,
data security is anyway a topic that users of smart
devices have to deal with and there are already quite
powerful technologies available that increase the
level of security for mobile data. Here, an important
task for future research efforts will be to integrate
such technologies in the described scenarios.
Another aspect comes into play if we consider
that the different kinds of data possibly gathered by
mobile devices need to be arranged and visualized in
a way that allows doctors to easily interpret this
data. Since doctors are usually not specialists in data
analysis, additional efforts need to be considered for
the presentation and analysis of the data.
Last but not least, the reliability of the medical
data gathered by not necessarily medical devices is
an issue that needs to be tackled.
REFERENCES
F. AlShahwan, K. Moessner, “Providing SOAP Web
Services and REST Web Services from Mobile
Hosts”, In: Fifth International Conference on Internet
and Web Applications and Services (ICIW 2010), pp.
174-179.
E. Gamma, R. Helm, R. Johnson, J. Vlissides, Design
Pattern – Elements of Reusable Object-Oriented
Software, Addison-Wesley. 1995.
M. Jansen. Analysis and Improvement of Energy
Consumption for Providing Mobile Web Services.
In.International Journal of Soft Computing and
Software Engineering, DOI: 10.7321/jscse. 2013a.
M. Jansen. About the Necessity to Change the Perspective
for Mobile Web Services. In: Proceedings of the 15th
IEEE International Symposium on Web Systems
Evolution, 2013b.
L. Li, W. Chou, “COFOCUS – Compact and Expanded
Restful Services for Mobile Environments”, In:
Proceedings of the 7
th
International Conference on
Web Information Systems and Technologies, pp. 51-
60, Noordwijkerhout, The Netherlands, 2011.
S. McFaddin, C. Narayanaswami, M. Raghunath, “Web
Services on Mobile Devices – Implementation and
Experience”, In Proceedings of the 5
th
IEEE Workshop
on Mobile Computing Systems & Applications
(WMCSA’03), pp. 100-109, Monterey, CA.
S. Srirama, M. Jarke, W. Prinz, “Mobile Web Service
Provisioning”, In: Proceedings of the Advanced
International Conference on Telecommunications and
International Conference on Internet and Web
Applications and Services (AICT/ICIW 2006), p. 120,
Guadeloupe, French Caribbean.
WEBIST2014-InternationalConferenceonWebInformationSystemsandTechnologies
446
