
The Educational Potential of Technologies for Older People
Reflections on the Well-being
Anelise Jantsch
1
, Simone C. O. Conceição
2
and José Valdeni de Lima
1
1
Universidade Federal do Rio Grande do Sul (UFRGS), Av. Paulo Gama,
110 - prédio 12105 - 3º andar sala 332, 90040-060, Porto Alegre (RS), Brazil
2
Faculty of Education, University Wisconsin-Milwaukee (UWM), Enderis Hall 623, 5320-0413, Milwaukee (WI), U.S.A.
Keywords: Health Education, Active Ageing, ICT, Elderly.
Abstract: Worldwide life expectancy has increased over the last century. In Brazil the population over 60 years was
approximately 10% in 2009, and it is expected to increase to 29% in 2050. This increase in life expectancy
leads us to consider strategies that can assist in maintaining the quality of life during the ageing process.
One strategy that must be considered is the health education to the elderly, so we construct a web
application – Active Ageing TV – that is based on the reports of World Health Organization, and on the use
of gerontology education to facilitate the learning process, and on the use of techniques to design according
to specific characteristics of older audience. To validate our application, a survey was conducted with
seniors who participated in a course of digital inclusion in Brazil, during 2009 to 2013. We used “Profile of
Individual Life Style" instrument to evaluate the lifestyle perceived by the participants. Our findings
indicate that seniors are looking for a preventive behavior, but information is necessary to assist them to
make right decisions for a healthy lifestyle.
1 INTRODUCTION
Worldwide life expectancy has increased over the
last century. In Brazil the population over 60 years
was approximately 10% in 2009, and it is expected
to increase to 29% in 2050 (IBGE, 2013). This
increase in life expectancy leads us to consider
strategies that can assist in maintaining the quality of
life during the ageing process (Veras, 2012).
Human ageing is a universal, progressive, and
gradual process. This process is different for each
individual. There are a variety of factors that affect
this process: genetics, biology, social factors,
environment, psychology, and culture (WHO, 2002).
Gerontology is “the scientific study of old age” and
consists of the integration of conceptual linkages
across the biological, psychological, and social
processes of aging (Alkema and Alley, 2006).
In Brazil, gerontology is still considered a new
science (Valadares et al., 2013), and is concerned
with the implementation of actions aimed at
improving the quality of life of those who are ageing
to ensure autonomy and independence. In turn,
educational gerontology refers to the use of a
teaching method to facilitate learning in older adults
through the exploration of the potential of this age
group (Ala-Mutka et al., 2008; Ianculescu and
Parvan, 2011; Kececi and Bulduk, 2012). In this
sense, continuing education requires a combination
of opportunities to encourage the promotion and the
maintenance of quality of life for the elderly.
According to the Ministry of Social Welfare and
Assistance in Brazil, "Ageing is a normal and
dynamic process, and it is not a disease. While
ageing is an inevitable and irreversible process,
chronic and disabling conditions that are often
observed with advancing age can be prevented or
delayed, not only by medical interventions, but also
interventions in social, economic, and environmental
aspects" (Brasil, 1996, p. 1).
The term "active ageing" was adopted by the
World Health Organization in 1990, and it is based
on the recognition of human rights of older people
and in the United Nations Principles of
independence, participation, dignity, care, and
personal fulfillment (WHO, 2002). The broad
concept of quality of life points to the need to
consider the aspects valued by the elderly related to
overall well-being such as health, life satisfaction,
and psychological well-being within the social and
539
Jantsch A., Conceição S. and de Lima J..
The Educational Potential of Technologies for Older People - Reflections on the Well-being.
DOI: 10.5220/0004959605390544
In Proceedings of the 6th International Conference on Computer Supported Education (CSEDU-2014), pages 539-544
ISBN: 978-989-758-020-8
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
physical environment in which they live. Therefore,
it is important to encourage a healthy lifestyle
through a balanced diet, regular exercise, social
interaction, enjoyable occupational activity, and
mechanisms to mitigate the stress and avoiding
smoking, alcoholism, and self-medication.
Self-care should be seen as the creation of new
opportunities to respond to life in a safe and healthy
way. For this reason, the issues addressed in
educational activities must involve more than
diseases and risk factors. Ageing, sexuality, leisure,
family relationship, and social rights of the elderly,
as well as numerous other factors that illustrate the
needs and interests of the older population, are
dimensions of life that must be considered to
promote self-care (Sousa and Assis, 2012). The
behavioral change to a healthy lifestyle is a key
ingredient to encourage active ageing.
This paper is organized as follows: section 2
shows the literature review on health education;
section 3 presents the Active Ageing TV application;
section 4 the methodology used to test the
comprehension about the content of Active Ageing
TV is explained; and in section 5 are presented the
concluding remarks.
2 HEALTH EDUCATION
Brazilians are living longer and this means that the
Brazilian society needs to promote programs for the
prevention and maintenance of health for the elderly.
Because the promotion of such programs has not
occurred, the ageing process of the Brazilian
population is now largely characterized by the
progressive accumulation of losses of functionality
in activities of daily living (Veras, 2012). The trend
is evident in the growing number of seniors who are
functionally disabled and have poor health. The
most common problems in elderly people are
Alzheimer's disease, depression, osteoporosis, and
falls. These problems show the need for an emphasis
on health promotion and prevention of frailties
(WHO, 2002).
According to Kececi and Bulduk: “the main
objective of health education is to provide
individuals and society with assistance so that they
can lead a healthy life through their own efforts and
actions. Therefore, health education supports and
develops all kinds of individual learning processes.
Similarly, it makes changes in the beliefs and value
systems of individuals, their attitudes and skill
levels; in other words, it changes their lifestyles”
(Kececi and Bulduk, 2012, p.160).
The World Health Organization suggests that
early education in life combined with opportunities
for lifelong learning can help people to develop
skills and confidence to adapt and maintain
independence as they grow older. Learning is
necessary to improve understanding (for instance,
learning related to health issues) and to enhance
capabilities for practical tasks (learning to use new
tools like online banking or how to use assistive
technologies to compensate for lack of
functionality), and learn new activities.
The motivation to learn for elderly people
depends strongly on the purpose of the learning
outcomes, and also in how much they consider
themselves able to achieve these results (self-
efficacy). The commitment to meaningful activities
for the elderly contributes to good health and
satisfaction with life and longevity (Ala-Mutka et.
al., 2008; Kececi and Bulduk, 2012; Ianculescu &
Parvan, 2011; Serbim et. al., 2012). The success of
health promotion can be evaluated by measuring to
what extent the intended objectives can be achieved
by target audience.
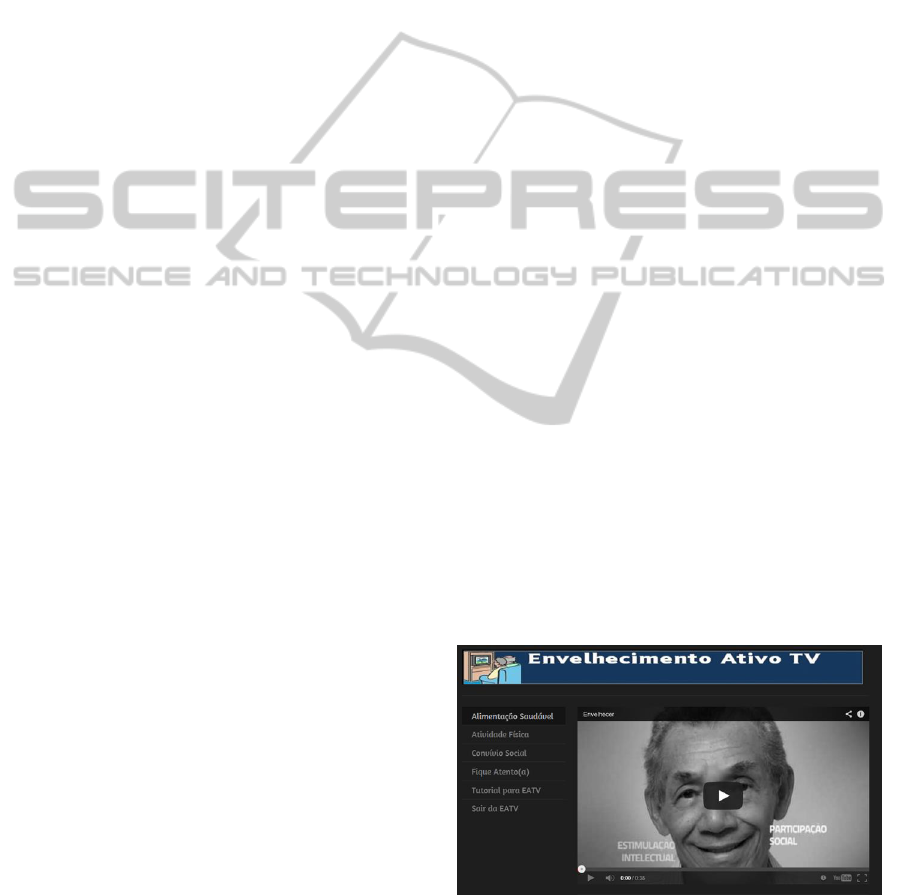
3 ACTIVE AGEING TV
We build a web application based on the WHO
Active Ageing reports (WHO, 2002), conventions
established by the field of educational gerontology
(Alkema and Alley, 2006), and the use of style
guides for interactive Digital TV for the elderly
(Rice and Alm, 2008). The platform selected for this
version of Active Ageing TV (Figure 1) is web
based. Today smartphones, tablets, connected
televisions and computers are all web receivers,
which allow a greater range of choice by seniors.
Figure 1: Active Ageing TV (Envelhecimento Ativo TV)
avaiable at http://envelhecimentoativotv.weebly.com.
Active Ageing TV focuses on information about
active ageing and activities recommended for the
CSEDU2014-6thInternationalConferenceonComputerSupportedEducation
540
elderly. Videos were used with content that includes
physical exercises and strategies that guide seniors
to make changes at home to meet their safety needs.
Information about social networks and senior
communities are also provided to give social
opportunities for the elderly.
Active Ageing TV aims to inform and to provide
resources in a variety of methods on how to maintain
independence and quality of life during the ageing
process, or, in other words to promote self-care to
the elderly. So, to achieve this purpose the videos
used were about the behavioral determinants defined
by WHO (WHO, 2002) like:
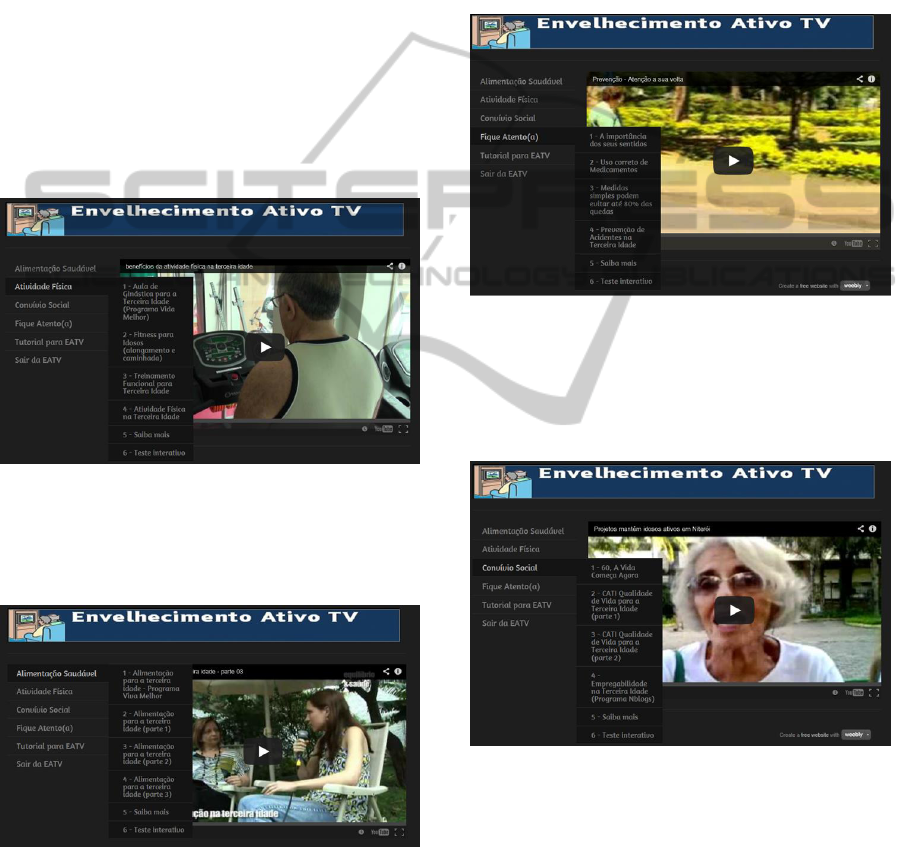
• Physical activity – regular practice of moderate
physical activity is essential for good health and to
preserve independence of the elderly, helping
reduce the risk of falls and related injuries (Figure
2).
Figure 2: Physical activity (Atividade física).
• Healthy diet – the maintenance of a balanced diet
rich in calcium can reduce the risk of injury in the
elderly (Figure 3).
Figure 3: Healthy diet (Alimentação saudável).
• Use of medications – the elderly tends to consume
greater number of medications than younger
people. As they age, people develop different
mechanisms for the absorption and the metabolism
of medications. If the elderly do not take their
medications as prescribed by physicians, their risk
of falls and side effects may be affected in
different ways (Figure 4).
• Risky behavior – the choices that people make and
the actions carried out can increase their chances
of falling, for example, to climb ladders, to wear
ill-fitting shoes, to bend over to perform everyday
tasks, to run without being aware of the
environment, or to avoid using artifacts to support
mobility such as canes or walkers (Figure 4).
Figure 4: Stay tuned (Fique atento (a)).
• Social interaction – incentive to stimulate social
interaction and conduct occupational activity as an
enjoyable way to relieve stress and prevent
depression and isolation (Figure 5).
Figure 5: Social interaction (Convívio social).
• Harmful habits – clarification about the
consequences of harmful habits like smoking,
alcoholism, and self-medication (Figures 2, 3, 4,
5).
In the Active Ageing TV application the user can
access four modules: healthy diet (Figure 3),
physical activity (Figure 2), social interaction
(Figure 5) and stay tuned (figure 4). Each module
has four videos extract by Youtube about the
TheEducationalPotentialofTechnologiesforOlderPeople-ReflectionsontheWell-being
541

proposed content, and a section “Know More” that
consists of a list of sites with more information
about the subject of study, and a section “Interactive
Test” that is a form to collect data about the user
behavior on that aspect.
The videos used were selected from the
reliability of its producers, such as universities,
government or broadcast TV programs with affairs
on health and wellness. One of the criteria was that
the protagonists of the videos would be the elderly,
and that the videos used were of short duration to
allow a discussion on the subject after its display.
This strategy makes a personal call to the elderly to
participate actively and think about their behavior in
health maintenance.
4 METHODOLOGY
We used qualitative and quantitative research
methods focusing on the behavioral determinants
adopted by elderly and its influence in their quality
of life. The 12 seniors surveyed were 60 years or
older and attended a course designed for digital
inclusion at the Federal University of Rio Grande do
Sul, Brazil between 2009 and 2012. We proposed a
Quality of Life course during four weeks in
November to December of 2013.
The seniors that have participated of our research
have an age average of 68 years. The group
encountered two times a week to study and discuss
about modules of Active Ageing TV. Each elderly
assisted the proposed videos individually and, after
that, all participants were invited to explain and
discuss with the whole group about what they
learned, what they already do to achieve a healthy
lifestyle and the strategies they used to do that. The
researcher assumed the role of mediator in this
educational practice, and it was created a
participative environment in which everyone felt
comfortable to show his/her ideas (Serbim et. al.,
2012; Sousa and Assis, 2012).
After watching all modules, each subject was
seen separately one per week, seniors were asked to
reflect on their lifestyle. For this we used two
instruments: (1) the "Profile of Individual Life
Style" instrument (Both et. al., 2008) and (2) an
individual semi-structured interview based on the
behavioral determinants of active ageing (WHO,
2002).
The Profile of Individual Life Style
Questionnaire (Both et. al., 2008) known as "The
Pentacle of Well-Being", with a conceptual basis for
evaluating the lifestyle of individuals or groups. This
instrument consists of 15 questions, divided into the
following factors: nutrition (factor 1), physical
activity (factor 3), preventive behavior (factor 4),
social relationships (factor 5) and stress management
(factor 2), without regard to socio-economic factors,
genetic heritage, political beliefs and other factors
that may influence the results.
Of course the ideal would be that all items were
completed at maximum level (corresponding to 3
points on the scale). Scores in levels zero (0) and
one (1) indicate that the individual must be guided
and helped to change his/her behavior in the items
assessed, since they pose risks to his/her health. The
general idea is to allow the person to identify
positive and negative aspects in his lifestyle, getting
information and opportunities to make decisions that
can lead to a life with more quality.
In our research we applied the instrument
individually and the senior received a copy of
his/her responses to check what points he/she is
doing well and the points he/she has to make efforts
to get better results. The meanings of the responses
are as follows: [0] never, [1] sometimes [2] often
and [3] always. The results indicate that diet and
physical activity should be improved. Like most of
group is living alone (8) or has a problem of
movement (4) or sedentary lifestyle. It demonstrates
the difficulty in maintaining a varied diet or frequent
physical activity.
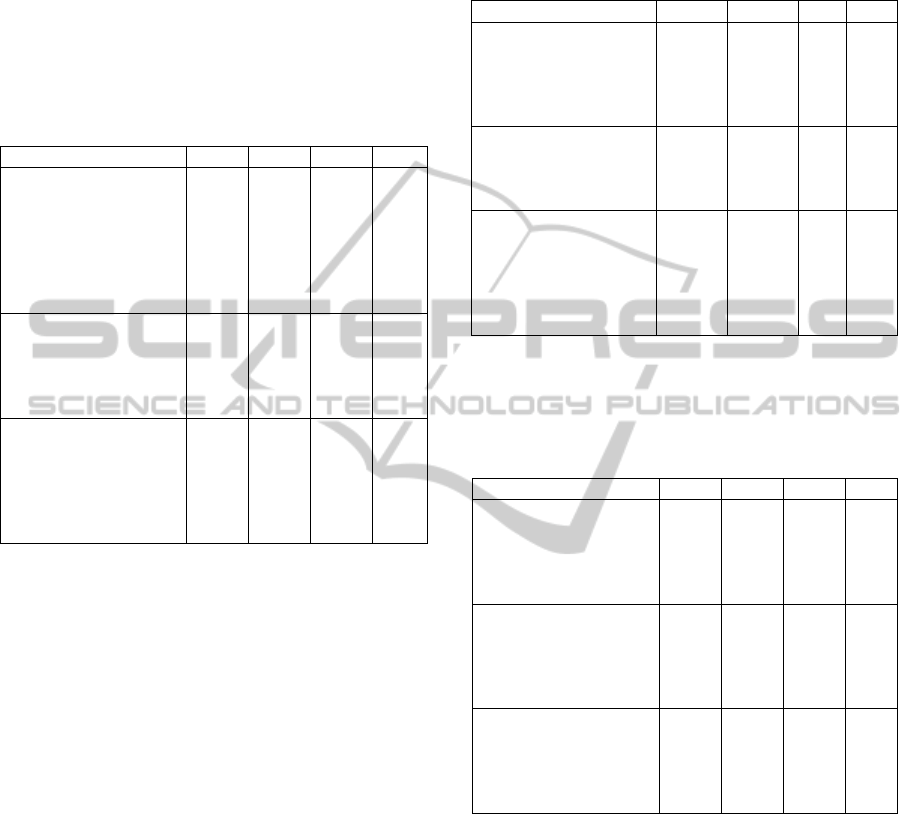
Table 1: Factor 1 (Nutrition).
[3] [2] [1] [0]
a. Your daily diet
includes at least 5
portions of fruit and
vegetables
31% 23% 31% 15%
b. You avoid eating
greasy foods (fatty
meats, fried foods)
and candies.
8% 46% 46% 0%
c. You do 4 to 5
different meals a day,
including full
breakfast.
31% 15% 39% 15%
Table 1 shows that 31% of group has 5 portions of
fruit and vegetables in their daily diet. On the other
hand, 46% sometimes avoid eating greasy foods and
candies, and 8% always avoid this kind of food.
Another factor that must be improved is the number
of meals a day, 39% sometimes do 4 to 5 meals, and
15% never do that. These outcomes were reinforced
with the speech of one senior: “with the video I will
try to insert more vegetables at meals; as I have
reflux, I'm adapting my diet and I have already
CSEDU2014-6thInternationalConferenceonComputerSupportedEducation
542
noticed better results; I started walking with a water
bottle in my purse... ”.
Senior’s speeches often lead to this: “You think
you know a lot, and maybe you know, but you do not
practice; things we already know but it's always
great to reinforce them; the elderly has resistance,
he/she is more stubborn, but if explain the change
and its benefits he/she can start to improve”.
Table 2: Factor 3 (Levels of Physical Activity).
[3] [2] [1] [0]
d. You realize at least
30 minutes of
moderate to intense
physical activity,
continuously or
cumulatively, 5 or
more days a week.
15% 31% 39% 15%
e. At least twice a
week you perform
exercises that involve
muscle strength and
stretching.
23% 46% 23% 8%
f. In your day by day,
you walk or you pedal
for transportation and
preferably use the
stairs instead of the
elevator.
15% 23% 54% 8%
In Table 2 we can see that although the elderly
group performs physical activities, they do not do it
in the frequency of five or more days per week. But,
23% perform exercises that involve muscle strength
and stretching twice a week. And, we can see that
sedentary lifestyle is represented in 54% of
individuals that sometimes use to walk or to pedal
for transportation, and prefer the elevator instead of
the stairs. After looking at the results a senior said:
"I'll promise to myself to start walking, because
when I doing exercises I felt good and I did not need
to take medicine for cholesterol that I need today".
Table 3 shows that the group has a preventive
behavior. They know their blood pressure, their
cholesterol levels and they are looking to control
them. But if the elderly look for to have a healthy
diet and better levels of physical practices, their
outcomes must be better. And Table 3 show too that
the group don’t smoke and drink alcohol with
moderation, and they use seatbelt and never drink
alcohol when they are driving.
Regarding to preventive behavior an elderly said:
“videos gave many tips on mobile, the height of the
bed, etc., there are things that I already do, but I
learned a lot, how to protect wires, take off rugs,
things that can cause accidents. As I live alone I
need to take care of myself".
Table 3: Factor 4 (Preventive Behavior).
[3] [2] [1] [0]
g. You know your
blood pressure, your
cholesterol levels and
you are looking to
control them.
46% 54% 0% 0%
h. You do not smoke
and you drink alcohol
in moderation (less
than 2 daily doses).
76,9% 7,7%
7,7
%
7,7
%
i. You always wear
your seatbelt and if
you drive, you respect
traffic regulations,
and you never ingest
alcohol when driving.
85% 15% 0% 0%
In Table 4 we can see that seniors have an active
participation in social life with family, friends and
community service.
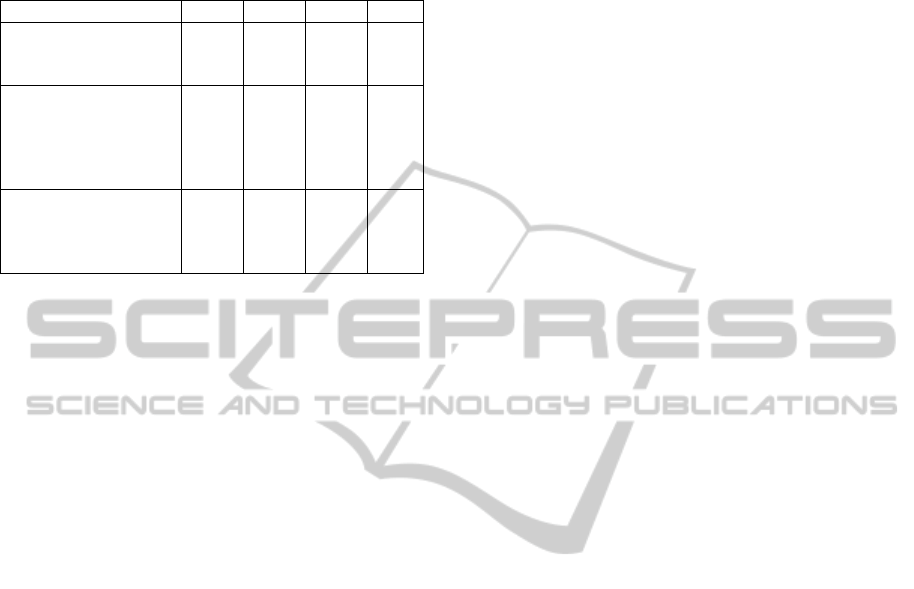
Table 4: Factor 5 (Quality of Relationships).
[3] [2] [1] [0]
j. You find yourself
surrounded by friends
and you are satisfied
with your
relationships.
77% 23% 0% 0%
k. Your leisure
includes meetings with
friends, group sports
activities, participation
in associations.
85% 15% 0% 0%
l. You try to be active
in your community
and you feel useful in
your social
environment.
67% 25% 0% 8%
Table 5 presents that they reserve at least five
minutes to relax by day (69%). And in the most
cases they can hold a discussion without change
their mood, even when they are contradicted (54%).
But, on the item of the balance between work and
leisure we can see that the group has some
difficulties to do that. Perhaps due to their creation
that has always prioritized the work and effort in
place of leisure.
Regarding the use of videos as course material, a
senior said: “Is interesting because you see the
video, you can assimilate the teachings more. I get
more attentive than if I have to read... I have history
of falls and the information of the videos was very
TheEducationalPotentialofTechnologiesforOlderPeople-ReflectionsontheWell-being
543
useful... I started to decrease the sugar and salt in
meals, and I started buying more fruit”.
Table 5: Factor 2 (Stress Management).
[3] [2] [1] [0]
m. You take time (at
least 5 minutes) every
day to relax.
69% 23% 8% 0%
n. You hold a
discussion without
changing your mood,
even you are
contradicted.
15% 54% 31% 0%
o. You balance the
time devoted to work
with the time devoted
to leisure.
15% 39% 46% 0%
The data considered here show a positive influence
that Active Ageing TV application performs in
quality of life and adoption of a healthy lifestyle by
seniors.
5 CONCLUSIONS
This paper presented a web application to help to
promote active ageing and adoption of behaviors by
the elderly that lead to a healthy lifestyle. Our
project was submitted to the Ethics Committee in
Research of the Federal University of Rio Grande do
Sul and was approved in accordance with the report
number 137.267 in 2012.
Active Ageing TV application differs from
others by using the educational approach as a
strategy to inform and to educate the elderly,
therefore encouraging them to become responsible
for maintaining their own health throughout life.
This is based on the concept of active ageing, as
defined by WHO reports. Our intention is to
disseminate the behavior determinants of active
aging policy to help seniors to maintain their
autonomy, independence, quality of life, and a
healthy life expectancy. Our contribution focuses on
the development of an application that seeks to
encourage the adoption of guidelines for active
ageing from the user perspective by promoting
greater awareness of the importance of certain
activities and lifestyle to improve the quality of life.
In fact, the lifestyle is one of the most important
factors for maintaining health as well as to promote
the extension of longevity of the population.
ACKNOWLEDGEMENTS
Jantsch A. is grateful to CAPES and CNPq for
scholarship and financial support, as well she is
grateful to seniors who participated in this research.
REFERENCES
Ala-Mutka, K., Malanowski, N., Punie, Y., Cabrera, M.,
2008. Active Ageing and the Potential of ICT for
Learning, © European Communities. ISBN 978-92-
79-09452-1.
Alkema,G. E., Alley, D. E., 2006. Gerontology’s Future:
An Integrative Model for Disciplinary Advancement. In
The Gerontologist, Vol. 46, No. 5, 2006, pp. 574-582.
Both, J.; Borgatto, A. F., Nascimento, J. V., Sonoo, C. N.,
Lemos, C. A. F., Nahas, M.V., 2008. Validation of the
“Individual Lifestyle Profile” Scale. In Revista
Brasileira de Atividade Física & Saúde, vol. 13, No. 1,
p. 5–14.
BRASIL, 1996. Ministério da Previdência e Assistência
Social. Plano de ação integrada para o
desenvolvimento da política nacional do idoso. Brasília.
Ianculescu, M., Parvan, M., 2011. Becoming a Digital
Citizen in an Aging World. In International Journal of
Education and Information Technologies, Issue 2,
Volume 5, 2011, pp. 182-189, ISSN 2074-1316.
IBGE – Instituto Brasileiro de Geografia e Estatística,
2013. Projeção da população do Brasil por sexo e
idade para o período 2000/2060.
Kececi, Ayla, Bulduk, Serap, 2012. Health Education for
the Elderly, Geriatrics, Prof. Craig Atwood (Ed.),
ISBN: 978-953-51-0080-5, InTech.
Rice, M., Alm, N., 2008. Designing new interfaces for
digital interactive television usable by older adults. In
Comput. Entertain. 6, 1, Article 6 (May 2008), 20
pages. doi=10.1145/1350843.1350849.
Serbim, A., Gerlack, L., Motta Marchi, D., Gaviolli, C.,
Cecconello, M., Moreira, L., Werlang, M., 2012.
Oficinas multiprofissionais: educação em saúde para
idosos de uma comunidade. In Gestão e Saúde.
Brasília, vol. 4, n. 1, nov. 2012.
Sousa, Letícia Marques de, Assis, Monica de, 2012.
Educação popular em saúde e grupos de idosos:
revisão sobre princípios teórico-metodológicos das
ações educativas em promoção da saúde. In Revista
APS (Atenção Primária à Saúde), v.15, n.4, p.443-453.
Valadares, M. de O., Vianna, L. G., Moraes, C. F., 2013.
The theme of human aging in research groups in
Brazil. In Revista Kairós Gerontologia, vol. 16, n. 2, p.
117-128. Online ISSN 2176-901X. Print ISSN 1516-2567.
São Paulo (SP), Brasil: FACHS/NEPE/PEPGG/PUC-SP.
Veras, Renato Peixoto, 2012. International Experiences
and Trends in Health Care Models for the Elderly. In
Ciência & Saúde Coletiva, vol. 17, n. 1, p. 231-238.
WHO/NMH/NPH, 2002. Active ageing: a policy
framework. Geneve: World Health Organization.
CSEDU2014-6thInternationalConferenceonComputerSupportedEducation
544
