
Knowledge Management Problems in Healthcare
A Case Study based on the Grounded Theory
Erja Mustonen-Ollila
1
, Helvi Nyerwanire
1
and Antti Valpas
2
1
Department of Software Engineering and Information Management,
Lappeenranta University of Technology, Lappeenranta, Finland
2
Department of Obstetrics and Gynaecology, South Karelia Social and Health Care District, South Karelia, Finland
Keywords: Knowledge Management, Healthcare, Empirical Research, Case Study, Grounded Theory.
Abstract: Knowledge management describes how information communication technology systems are applied to
support knowledge creation, as well as in the capturing, organization, access, and use of an organization’s
intellectual capital. This paper investigates knowledge management problems in healthcare. The major
conclusions regarding the problems identified are: access to patient data in ICT systems or lack of data,
complex medical data, and problems in saving data to ICT systems; ICT system integration, architecture,
cost and regulations by political decisions and knowledge transfer problems; tacit knowledge missing in
ICT systems; communication and communication barriers between primary and special healthcare; ICT
security and trust problems; negative attitude or limited support from "peers" or superiors; patients’
resistance to recommendations; physicians’ stress and control-sharing problems, too short time in the
policlinic to search for patient information, limited personnel resources, and work pressure. A conceptual
framework of knowledge management is developed by the Grounded Theory approach. The data validates
past studies, and reveals relationships between categories. The relationships between the knowledge
management categories enhance confidence in the validity of the categories and relationships, and expand
the emerging theory.
1 INTRODUCTION
The concept of healthcare, as referred to in our
study, includes medicine, nursing, and rehabilitation
(Koskinen, 2010). In this study the healthcare
environment is referred to as a place in which
medical, clinical and nursing knowledge is ingrained
in practitioners (Räisänen et al., 2009). Knowledge
refers to the ways that information can be made
useful to support a specific task or make a decision
(Stair and Reynolds, 2006), personalized
information (Alavi and Leidner, 2001), awareness,
experience, skills, and learning (Suurla et al., 2002),
tacit knowledge (Polanyi, 1966; Nonaka, 1994),
explicit knowledge (Puusa and Eerikäinen, 2010;) as
well as the medical, clinical, and nursing knowledge
of physicians and nurses (Hill, 2010). Knowledge
management is defined as a process where
information communication technology (ICT)
systems are applied to support the activities in
organizing knowledge, expertise, skills and
communication (Suurla et al., 2002). Knowledge
management can be further defined as a
collaborative and integrated approach to the
creating, capturing, organizing, access and use of an
organization’s intellectual capital (Dalkir, 2005).
There exists collective knowledge in organizational
networks (Alavi and Leidner, 2001), and people
learn by working with each other in practice, and
transfer and receive knowledge on best practices
(Grover and Davenport, 2001). In spite of the above
definitions and past studies, there are several
problems that hamper knowledge management.
These problems include communication and
understanding problems between ICT professionals
and healthcare professionals (Martikainen et al.,
2012). One reason for this communication problem
can be the fact that the working communities do
different things and work differently, they have
different terms and vocabularies, and therefore they
do not understand each other (Dalkir, 2005).
Viitanen et al. (2011) argue that physicians have
problems with searching for the right data. The
patients’ resistance to recommendations, limited
15
Mustonen-Ollila E., Nyerwanire H. and Valpas A..
Knowledge Management Problems in Healthcare - A Case Study based on the Grounded Theory.
DOI: 10.5220/0005028200150026
In Proceedings of the International Conference on Knowledge Management and Information Sharing (KMIS-2014), pages 15-26
ISBN: 978-989-758-050-5
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

time and limited personnel resources, work pressure,
negative attitude or limited support from "peers" or
superiors can be causes for not following the
guidelines (Heilmann, 2010). Using the ICT system
can also take a lot of physicians’ work time, they
have problems with accessing patient data, and they
are highly critical towards ICT systems (Martikainen
et al., 2012; Nykänen et al., 2012). Finally, Kothari
et al. (2012) claim that physicians’ and nurses’ tacit
knowledge cannot be found in ICT systems.
As past studies have shown, a lot of knowledge
management problems exist in healthcare. We have
applied past studies and empirical evidence to carry
out a qualitative in-depth case study (Benbasat et al.,
1987; Yin, 2003) that identifies problems in
knowledge management in one healthcare
environment. We analyze the collected data with the
Grounded Theory (GT) approach, and develop a
conceptual framework with categories and
relationships between the categories (Glaser and
Strauss, 1967; Pawluch and Neiterman, 2010). Our
goal is to investigate knowledge management
problems in detail in a Social and Health Care
District and its central hospital, both located in
South Karelia, Finland. We explore strategies that
healthcare organizations deploy while learning about
their knowledge management problems, to what
extent these problems are shaped by the
organizational context, and how these potential
problems influence both ICT system development
work and patient care work in practice. We have
made 103 knowledge management observations
supported by empirical evidence.
We categorized the observations with GT
analysis (Glaser and Strauss, 1967), and the analysis
revealed 23 categories: Patient, Patient Data in ICT
Systems, Patient Data Transfer in ICT, Patient Data
Transfer on Paper, Lack of Patient Data Transfer
Control, Permission Denial of Patient Data Transfer,
Patient Care Process, Nurse, Nurse’s Lack of Time,
Physician, Physician’s Attitudes, Physician’s Stress,
Physician’s Lack of Time, Physician’s Tacit
Knowledge, Physician’s Medical and Clinical
Decisions, ICT Systems, ICT Systems Vendor, ICT
Systems Legislation, ICT Systems Technology, ICT
Systems Development Resources, ICT Systems
Communication Barriers, Primary and Special
Healthcare Services, and Social Issues.
The above categories were related to each other,
and we found six higher levels of abstraction of
statements based on our conceptual framework,
propositions to our categories, and relationships
between the categories.
The rest of the paper is structured as follows.
Section two describes related research, section three
presents the research method, and section four
outlines the data analysis. Finally, section five
contains conclusions and discussion.
2 RELATED RESEARCH
According to Fisher (2013), healthcare ICT systems
contain too much data, and the healthcare
professionals are not able to find the required
information and data of the patients. Viitanen et al.
(2011) and Martikainen et al. (2012) also claim that
it is difficult to find the previous patient records
because the search functions in the ICT systems and
their usability are poor. Physicians and other
healthcare professionals have difficulties in finding
the relevant data on time, they do not know what
kind of data to search for, and they are critical
towards ICT in general (Martikainen et al., 2012;
Nykänen et al., 2012; Viitanen et al., 2011). The
contextual aspects behind ICT system design are
difficult to understand, and therefore there is a
problem of how to involve healthcare professionals
in ICT system development activities. There are also
problems to visualize which different technologies
can be integrated together in ICT, and how to use
healthcare professionals’ knowledge in ICT
(Martikainen et al., 2012). When physicians are
requested to participate in healthcare ICT system
development, they find such activities quite pointless
(Martikainen et al., 2012). Viitanen et al. (2011)
claim that ICT systems lack suitable features to
support typical clinical decision-making, and ICT
systems are not able to provide the physicians with
the features and functionalities which are required to
perform clinical work on patients, for example to
analyze the state of the patient, make decisions about
the actions required, and perform the actions.
Young et al. (2000) state that junior physicians miss
proper ICT systems, which are robust, time neutral,
and need a short time to learn, because they need
ICT systems frequently in their work. Greig et al.
(2012) claim that it is difficult to share knowledge
and to know what knowledge exists in the working
organizations because the access is restricted.
Furthermore, verbal knowledge in mentoring and
formal or informal meetings is not stored in ICT
systems (Lin et al., 2008). It is not always known,
either, what other colleagues have not written down
in the ICT system (Nykänen et al., 2012). Kothari et
al. (2012) claim also that the tacit knowledge of
healthcare professionals is not found in ICT systems.
Accordingly, ICT systems, guidelines and divisions
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
16

of work, specializations, organizational structures,
cultural models and attitudes vary between public
primary, private primary and special healthcare
service environments (Viitanen et al., 2011).
Burgess et al. (2012) state that information transfer
and communication between primary and special
healthcare services fail. Primary healthcare takes
place in municipal health centres, private clinics,
working places, schools, and defence forces. These
organizations have their own type of patients and
only if the patient requires special healthcare, she or
he is guided to it, such as to a central hospital or
university hospital (Niskanen, 2002). One problem
is that proper coordination tools, such as medical
information about the patient in ICT systems
between private health centres and public healthcare
are lacking, and information is transferred on paper
or by fax, and some important data can be lost when
transferring it (Reddy et al., 2009). There is no
control in data transfer, and the staff must start the
programs manually (Häyrinen et al., 2008). The
healthcare ICT systems are expensive, regulated by
political decisions, not standardized, include
complex medical data, it is difficult to save data to
the systems and do statistics, and there exist security
and trust problems (Grimson et al., 2000). There are
also problems in integrating the separate ICT
systems in social care and healthcare because of the
laws concerning them (Niskanen, 2002; Laki
159/2007, 2007; STM, 2013). The systems are not
standardized, and healthcare organizations are
forced to take new versions of systems in use
regularly (Laki 159/2007, 2007; STM, 2013).
Central governments are shifting the social and
healthcare laws to local authorities in order to
arrange better social and healthcare for the citizens,
and healthcare service systems are divided into
primary, special healthcare, tertiary healthcare and
social services, which are supervised by the
municipal authorities of social and healthcare
districts. In Finland these services are supported by
the National government (Hämäläinen et al., 2013).
Finally, the integration of ICT systems is not
prepared for the future needs of patients (Linthicum,
2004). One problem is that patients will advise or
guide physicians towards other options for their
condition, and this will cause stress to the physicians
(Edwards et al., 2012). According to Blakeman et al.
(2006), physicians have problems in patient care
with patient involvement and sharing the control of
the patient’s health. Ammenwerth et al. (2006) state
that a physician has too short time in the policlinic to
search for patient information in the systems, and he
or she does not want to move back and forth
between systems, as for instance the X-ray pictures
have to be looked at in viewers. According to Gupta
(2009), integration is difficult due to a lack of
integration standards, and hospitals have currently a
lot of computer systems installed or built at various
periods of time by different vendors. Suomi and
Salmivalli (2002) argue that in paper-form
prescriptions one of the biggest problems is the
difficulty of reading the physician’s handwriting.
Kaye et al. (2010) claim that the barriers between
primary and special healthcare services are lack of
knowledge and skills, and poor communication. The
barriers are a result of non-recognition of health
professionals’ roles and responsibilities, and
inadequate communication between primary and
special healthcare services. One problem and
challenge in managing resources and service
improvement is due to complex healthcare
operations if an enterprise architectural solution is
missing, and the ICT systems’ architectural
descriptions within organizations lack the three
layers of business, application and technology
(Jonkers et al., 2003). Nilakanta et al. (2009) also
claim that business processes are more important
than clinical and diagnostics care, and knowledge
management capabilities and the organization’s
commitment and focus on knowledge support the
business processes. Thus, despite a growing interest
in knowledge management problems in healthcare,
their relationships have not been recognized in the
literature. Rather, past studies have focused on
knowledge management problems and ICT systems
in healthcare in general. Therefore, our study aims to
respond to this lack of studies and to provide useful
information of knowledge management in one
Social and Healthcare District and its central
hospital. Based on the past studies, we have
formulated the following research questions:
RQ1: What are the knowledge management
problems in healthcare?
RQ2: How are the knowledge management
problems in healthcare related to each other?
3 RESEARCH METHOD
This study utilizes both qualitative and quantitative
research processes and theory building approaches.
It takes an in-depth case study, theory building and
Grounded Theory (GT) perspective involving a
specific healthcare environment in which knowledge
management problems are studied (Glaser and
Strauss, 1967; Benbasat et al., 1987; Eisenhard,
1989; Yin, 2003; Cresswell, 2007; Pawluch and
KnowledgeManagementProblemsinHealthcare-ACaseStudybasedontheGroundedTheory
17

Neiterman, 2010). In this healthcare environment,
the case was selected so that it would either predict
similar outcomes (i.e. literal replication) or produce
contracting results but for predictable reasons (i.e.
theoretical replication) (Yin, 1994). Theory
triangulation was applied by interpreting a single
data set from multiple perspectives to understand the
research problems (Denzin, 1978). The concepts and
their relationships were validated with the grounded
theory approach (Glaser and Strauss, 1967;
Eisenhardt, 1989; Glaser, 1992). During the
research, theoretical background knowledge was
gained, which increased the credibility of the study
(Glaser, 1992; Miles and Huberman, 1994).
According to Eisenhardt (1989), the combination of
case study with the grounded theory approach has
three major strengths: it produces a novel theory, the
emergent theory is testable, and the resultant theory
is empirically valid. In the GT approach the theory
emerges from the data. According to Glaser (1992),
there is no need to review any literature of the
studied area before entering the field. This is in line
with our research, as we started collecting the data
before developing our conceptual framework.
Specifically, each interview transcript was analyzed,
and major emergent themes and concepts were
identified in order to form similar categories (Myers
and Avison, 2002). In our case study, a social and
healthcare district and its central hospital were the
units of analysis. The sample was limited to one
district and its central hospital, because the goal of
the study was to gain deep understanding of the
selected environment and to identify the knowledge
management problems at this specific site. The
target of the study was the Social and Healthcare
District of South Karelia in Finland and its central
hospital (Timonen, 2013; Eksote, 2013). The district
has about 133 000 inhabitants, and the total number
staff employees in the district is 3 843, of which
1 711 work in the health services. In the central
hospital, 17 special medical areas cover scheduled
clinical appointments in ward care, urgent care and
emergency. The number of scheduled clinical visits,
urgent care and emergency is approximately over 80
000 a year (Timonen, 2013; Raudasoja, 2013;
Eksote, 2013).
The knowledge management definitions and
objectives of the research formed the basis for
interviews and data collection. The interviewees
were also presented with the research problem, and
they were chosen because their role was to use,
create and transfer healthcare-related medical and
ICT information, and translate it to knowledge
relevant to the healthcare situation at hand. In order
to address the research questions, we conducted
seven audio-recorded unstructured and semi-
structured interviews that investigated experiences in
knowledge management issues in the chosen
healthcare environment. The interviews included
three individual interviews and four group
interviews, and they took place between June 2012
and November 2013. The interviewees were the
communications manager, ICT director, the central
hospital’s medical director (who was also the chief
physician in the internal medicine and
endocrinology department), the central hospital’s
chief physician in the obstetrics and gynaecology
department, the central hospital’s junior physician in
the emergency department of the district, and the
development manager of the National Archive of
Health Information (KanTa Services) project (STM,
2013) of the Ministry of Social Affairs and Health.
The interviewees had been involved in many
knowledge management issues and processes in
their own fields of expertise during their working
careers that extended over a period of 10 to 30 years
in different positions either in South Karelia Social
and Health Care District or other healthcare
environments in Finland. The development manager
of the Ministry of Social Affairs and Health was
interviewed about the past and future health
development in Finland, because the KanTa project
(STM, 2013) affects the healthcare development in
all social and healthcare districts in Finland.
Archival material was also studied, representing a
secondary source of data, and it included public
news and internal material of the development of the
Social and Health Care District, and public news of
the KanTa project of the Ministry of Social Affairs
and Health. Triangulation involved checking
different data sources simultaneously to improve the
reliability and validity of the data.
3.1 Data Collection and Categorization
The interviews included frequent elaboration and
clarification of the meanings and terms, they were
audio-recorded, and the recordings were transcribed,
yielding over 100 pages of transcripts. After
transcribing the interviews, we categorized the data
under the main categories, knowledge management
problems according to relevant terminology and
theories, which were the most often refereed work of
categorizing concepts in the studied research area.
The problem with the main categories was whether
there would be enough proof found in the data to
derive the knowledge management categories as
valid and reliable, and whether the categories
discovered in the data would be the correct ones.
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
18
Table 1: Categories and total number of different empirical observations.
Category Definition
Total
number of
observations
Patient A patient receives care and treatment by a physician. 42
Patient Data in ICT Systems
Patient’s personal data, medical history, treatments, tests, examinations,
diagnoses, and consultation requests in the ICT systems.
16
Patient Data Transfer on
Paper
Patient’s personal data, medical history etc. are transferred on paper. 7
Patient Data Transfer in ICT Patient’s personal data, medical history etc. are transferred in ICT systems. 6
Lack of Patient Data Transfer
Control
In many ICT systems’ areas the transfer of the patient’s personal data,
medical history etc. is not controlled and the staff must start the programs
manually.
3
Permission Denial of Patient
Data Transfer
A patient can deny her or his personal data, medical history etc. to be
transferred with ICT or on paper.
2
Patient Care Process
In the patient care process a physician makes a diagnostic decision and
determines the proper treatment for the patient.
8
Physician
A physician needs knowledge of anatomy, physiology, and medical science
and knowledge of how to apply this knowledge in practice.
17
Physician’s Tacit Knowledge
A physician’s tacit knowledge is related to how she or he is able to use his or
her biomedical knowledge, intuition and experience.
4
Physician’s Attitudes to ICT
and Patients
Physicians' attitudes towards ICT systems are negative because of lack of
time. Physicians have attitude problems towards patients who know about
their own diseases.
4
Physician’s Stress Patients cause stress to physicians. 2
Physician’s Medical and
Clinical Decisions
ICT systems do not support the clinical and medical work of the physician. 5
Physician’s Lack of Time Physician has lack of time in the policlinic to search for patient information. 2
ICT Systems
There are hundreds of ICT systems used in hospitals, which physicians and
other professionals use in their daily work with patients.
31
ICT Systems Vendor ICT systems’ vendor implements the ICT systems and ICT products. 7
ICT Systems Technology
ICT system technology connects the healthcare treatment process in which
different people and technologies work together.
19
ICT Systems Legislation
The laws prevent the integration of social and healthcare issues in ICT
systems. The social and healthcare laws have been transferred from the
Finnish national government to local authorities.
4
ICT Systems Development
Resources
System developers are not qualified enough to implement ICT systems to
healthcare due to their lack of training in biomedical informatics. ICT
development lacks money.
4
ICT Systems Communication
Barriers
The barriers between primary and special healthcare services and ICT
professionals are lack of knowledge and skills, and poor communication.
1
Nurse
Nurses work together with physicians, therapists, other healthcare staff,
families and patients.
6
Nurse’s Lack of Time
Nurses are busy, and do not have enough time to input data to the ICT
systems.
6
Primary and Special
Healthcare Services
Healthcare guarantees sufficient social and healthcare services for all
residents in the district.
4
Social Issues Patient’s social issues. 3
Total number of
observations
103
Table 2: An example of an observation concerning the category “Physician’s Tacit Knowledge”.
Knowledge
management problem
Definition Source Empirical evidence
Interviewed
person,
specialized
area/ expertise
Physicians have to
interpret the results
of special tests by
special devices by
themselves using
their tacit knowledge
The ICT systems are not able to
provide the physicians the features
and functionalities which are
required to perform clinical work
on patients, for example to analyze
the state of the patient.
Puusa and
Eerikäine
n, 2010;
Heilmann;
2010;
Hill, 2010
For example, in special treatment, the
information systems may control some
devices like the x-ray machine, e.g. by
collecting the data and analyzing it. Then
the doctor has to make the analysis of what
the data is, and then write it down to the
main system.
Junior
physician,
specializing in
gynecology
and women's
diseases
KnowledgeManagementProblemsinHealthcare-ACaseStudybasedontheGroundedTheory
19
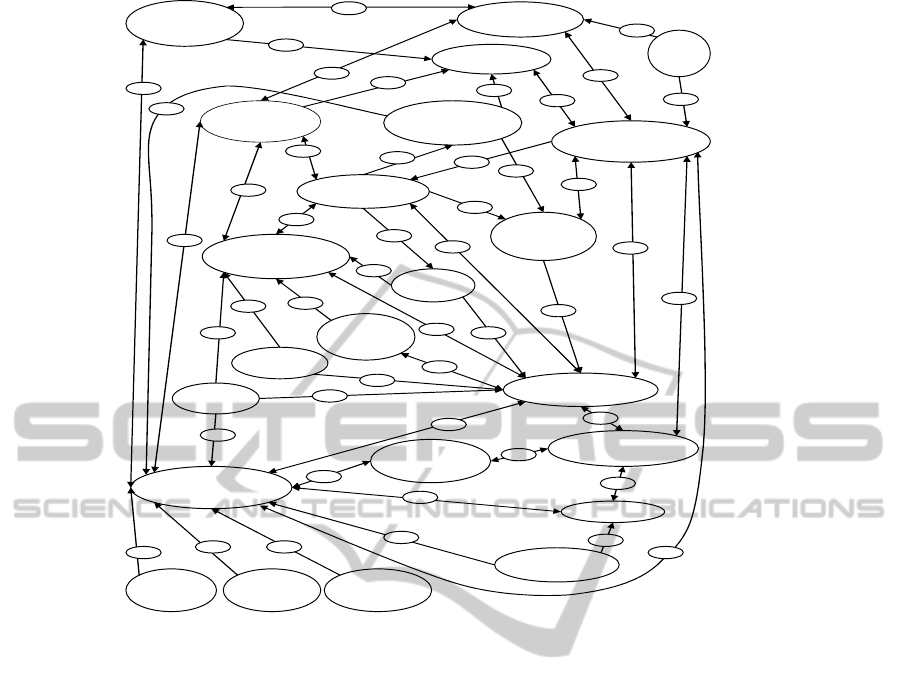
Figure 1: Conceptual framework of categories.
Based on our intuition and knowledge we made a
table 1. In table 1 the first column includes a specific
knowledge management problem discovered in the
empirical data; the second column includes the
definition of a knowledge management problem
based on the empirical data; the third column
includes evidence from the literature to the problem
in the first column; the fourth column includes the
name of the literature source of the third column;
and finally the fifth column includes the transcript
number and the interviewed person’s name and
occupation. By doing this we have created a chain of
evidence: from empirical data we have derived all
the knowledge management problems and validated
them with past studies. This table is available on
separate request from the authors.
4 ANALYSIS
After creating the chain of evidence in data
categorization, a total amount of 103 different
empirical observations under 23 categories (see
Table 1) were found by using Glaser and Strauss’s
(1967) and Pawluch and Neiterman’s (2010)
grounded theory analysis instructions, which support
the finding of categories grounded on data and based
on the researchers’ own intuition and knowledge. An
example of an observation concerning the category
“Physician’s Tacit Knowledge” is presented in Table
2.
Our conceptual framework of the discovered
categories (see Figure 1) is based on empirical
evidence and theories reflecting the findings in the
field (Glaser and Strauss, 1967; Pawluch and
Neiterman, 2010). Specifically, we have involved
fragmentation and reassembled our data into
thematic categories by trying to capture a broader
social system of ideas from the experience of the
social actors (Glaser and Strauss, 1967; Pawluch and
Neiterman, 2010), in this case the actors working in
the Social and Health Care District. After the
categories had been found, we determined the
properties of the categories and propositions
(hypotheses) for how the categories were related. In
Figure 1, the categories are shown as ellipses, and
the solid, numbered arrows describe the
relationships between the categories. These
relationships based on empirical data are presented
in detail in Table 3.
Nurse’s
Lackof
Time
PatientDatain
ICTSystems
PatientData
TransferinICT
LackofPatient
DataTransfer
Control
PermissionDenial
ofPatientData
Transfer
Physician’s
Tacit
Knowledge
Physician’s
Attitudes
Physician’s
Stress
Physician’s
LackofTime
Physician’sMedical
andClinical
Decisions
ICT
Systems
Ve
n
do
r
ICTSystems
Legislation
ICTSystems
Technology
ICTSystems
Development
R
esou
r
ces
SocialIssues
ICTSystems
Physician
Patient
PrimaryandSpecial
Healthcare Services
PatientCareProcess
Nurse
PatientData
Transferon
Paper
ICTSystems
Communication
Barriers
13
34
33
17
6
42
41
16
44
9
43
46
2
39
22
27
1
15
47
26
32
21
5
8
45
29
30
11
10
31
24
25
28
20
23
19
14
37
38
40
36
12
24
1835
7
3
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
20
Table 3: Properties of categories and propositions (hypotheses) on how the categories are related on the basis of the data.
Category/Categories
Properties of categories and propositions (hypotheses) on how
the categories are related (arrows in Figure 1)
Arrow
number
Patient Data in ICT Systems, Patient, Nurse,
Physician, ICT systems, Physician’s Medical
and Clinical Decisions
Physicians and nurses must document all care treatment in order
to follow up how the patient has been treated.
1, 2, 3,
4, 5
Patient Data Transfer in ICT, Patient, Patient
Care Process, Primary and Special Healthcare
Services
The patient moves back and forth between primary and special
healthcare services, because the patient data does not move
between services.
6, 7, 8
Patient Data Transfer on Paper, Patient, Patient
Care Process, Physician, Primary and Special
Healthcare Services, ICT System
Communication Barriers, ICT Systems
Primary and special healthcare services transfer patient data on
paper not by ICT systems even if they use the same ICT systems.
9, 7, 8,
10, 11,
43, 46
Patient Data Transfer in ICT, Lack of Patient
Data Transfer Control
It is possible that other complications will appear because the
data transfer is not controlled.
13, 14
Lack of Patient Data Transfer Control, ICT
Systems, Patient Data in ICT Systems, Patient
Data Transfer in ICT
In ICT systems’ areas data is distributed between heterogenic
and autonomous ICT systems, and there is no data transfer
control.
14, 41,
42
Permission Denial of Patient Data Transfer,
Patient, ICT Systems
The denial of patient information permission affects the ICT
system architecture, and data transfer is restricted.
15, 16,
17
Patient Care Process, Physician, Patient, Patient
Data in ICT Systems, Primary and Special
Healthcare Services
Physicians cannot track a patient’s location in the patient care
process in the ICT systems because of a large amount of data.
18, 7, 2,
1, 19, 45
Primary and Special Healthcare Services,
Patient Care Process, Patient, Physician
Right healthcare is not provided by the health centers and thus
the patients need hospital care.
19, 8, 7,
2
Physician’s Tacit Knowledge, Physician’s
Medical and Clinical Decisions, ICT Systems
A great deal of tacit knowledge is not transferred from healthcare
professionals via ICT systems to other healthcare professionals.
20, 21,
22, 23
Physician’s Tacit Knowledge, Physician, ICT
Systems
Healthcare professionals use “tricks” called as hidden knowledge
in ICT systems and computers.
20, 23
Physician’s Attitudes, Physician’s Medical and
Clinical Decisions, ICT Systems, Patient,
Physician
Junior physicians have attitude problems to patients who know
about their own diseases. The healthcare personnel’s attitudes
towards ICT systems are negative.
24, 25,
26, 27
Physician’s Stress, Patient, Physician’s Medical
and Clinical Decisions, Physician
Patients cause stress to the physicians by giving them advice
about their illnesses.
2, 28,
29, 30
Physician’s Lack of Time, Physician’s Medical
and Clinical Decisions, Patient Data in ICT
Systems, ICT Systems, Patient, Physician
Physicians have too short time in the policlinic to search for the
patient data in the ICT systems and other special systems and
devices.
31, 32,
22, 23
ICT Systems, Physician’s Medical and Clinical
Decisions, Patient, Physician
ICT systems do not guide medical decision-making. 23, 5, 27
Nurse’s Lack of Time, Nurse, Patient Care
Process, Patient
Physicians and nurses do not have enough time to input data to
ICT systems.
33, 34,
3, 47
ICT Systems Vendor, ICT Systems
The ICT vendor has problems in the change management of ICT
systems, and it takes years to implement the changes.
35
ICT Systems, ICT Systems Legislation, Social
Issues
Integration of social and healthcare issues in ICT systems is not
possible because of laws.
36, 37,
38
ICT Systems, ICT Systems Legislation, ICT
Systems’ Technology, Social Issues
Psychosocial support for the future needs of a patients is missing
from ICT systems and their integration.
36, 37,
38, 12
ICT Systems, ICT Systems Technology
The usability of ICT systems is poor because of many new ICT
versions, and too much unnecessary data must be saved in the
ICT systems.
12, 39
ICT Systems, ICT Systems Technology, ICT
Systems’ Vendor
It means huge work to implement a new interface to an old
fashioned application environment (ICT system environment).
12, 35
ICT Systems, ICT Systems Development
Resources
Qualified ICT personnel who know about biomedical knowledge
in the healthcare ICT systems area is lacking due to the growing
importance of ICT system integration.
40
ICT Systems, ICT Systems Communication
Barrier, Primary and Special Healthcare
Services
A knowledge and communication barrier exists between primary
and special healthcare services for patients. Communication and
understanding between ICT professionals and healthcare
professionals are poor.
11, 10,
ICT Communication Barrier, Primary and
Special Healthcare Services, Social Issues, ICT
Systems, ICT Systems’ Legislation
Laws regulate the communication of ICT systems between social
workers and healthcare patients with social problems.
36, 11,
10, 38
KnowledgeManagementProblemsinHealthcare-ACaseStudybasedontheGroundedTheory
21

Finally, in our in-depth case study, we took carefully
into consideration beforehand who to interview,
what to do next, what group to look for, and what
additional data we should collect in order to develop
a theory from the emerging data. The constant
comparison between the data and concepts in past
studies in order to accumulate evidence convergence
on simple and well-defined categories led us to a
higher level of abstraction of statements about the
relationships between the categories. This theorizing
was in line with Pawluch and Neiterman’s (2010)
suggestions of creating a grounded theory with
Glaser and Strauss’s (1967) approach. The higher
level of abstraction of the statements is presented in
the conclusions and discussion section.
5 CONCLUSIONS AND
DISCUSSION
This qualitative, empirical case study based on the
Grounded Theory approach (Glaser and Strauss,
1967) revealed that many knowledge management
problems can be found in knowledge and
information-intensive environments in the healthcare
domain. Based on seven in-depth interviews, the
study described knowledge management problems in
the South Karelia Social and Health Care District in
Finland and its central hospital. As the data
collection point of view we used the director level
of the central hospital, the ICT director, the
communications manager, and the junior and senior
physician level of the central hospital in the district,
as well as the development manager level of the
Ministry of Social Affairs and Health in Finland.
This multi-perspective point of view gave us rich
data for solving our research problems.
Our study is in line with the studies of
Martikainen et al. (2012), Viitanen et al. (2011),
Nykänen et al., (2012), and Fisher (2013)
concerning problems with patient data in ICT
systems. Studies of problems in ICT system
development, technologies, integration and ICT
systems’ lack of clinical decision-making
(Martikainen et al., 2012; Young et al., 2000) are
also in line with our study. The problems in
knowledge transfer and lack of data were also
verified (Greig et al., 2012, Lin et al., 2008). The
claims by Nykänen et al. (2012), and Kothari et al.
(2012) for tacit knowledge missing in ICT systems,
and the lack of data transfer control (Häyrinen et al.,
2008) were also confirmed. The claims by Polanyi
(1966), Nonaka (1994), Puusa and Eerikäinen
(2010), Heilmann (2010), and Hill (2010)
concerning the use of tacit knowledge in decision
making were also proved to be valid.
Attitude problems (Viitanen et al., 2011), failures
in information transfer, and communication and
communication barriers between primary and special
healthcare services (Burgess et al. 2012; Niskanen,
2002, Reddy et al., 2009; Kaye et al., 2010) were
also found. Difficulties in carrying out statistics
from the current data in ICT systems due to their
structure was confirmed (Grimson et al., 2000). We
also discovered that ICT systems are expensive,
regulated by political decisions, not standardized,
and include complex medical data, it is difficult to
save data to systems, and there exist security and
trust problems (Grimson et al., 2000). Integration
problems exist in healthcare and between social care
and healthcare because of laws (Niskanen, 2002;
Laki 159/2007, 2007; STM, 2013; Hämäläinen et al.,
2013; Linthicum, 2004; Gupta, 2009). Physicians’
stress and control-sharing problems (Edwards et al.,
2012; Blakeman et al., 2006) were also confirmed.
The statement of Ammenwerth et al. (2006) about
too short time in the policlinic to search for patient
information, and Suomi and Salmivalli’s (2002)
argument for paper problems were found to be valid
in our case as well. The claim for difficulties in
healthcare operations if an enterprise architectural
solution is missing (Jonkers et al., 2003) is in line
with our study. The claim of Nilakanta et al. (2009)
about business and knowledge management
processes being currently more important than
clinical and diagnostics care was corroborated. The
patients’ resistance to recommendations, limited
time and limited personnel resources, work pressure,
negative attitude or limited support from "peers" or
superiors were also confirmed (Heilmann, 2010).
In this study we discovered a higher level of
abstraction of statements based on our conceptual
framework, propositions to our categories, and
relationships between the categories as follows.
First, physicians’ tacit knowledge and experience,
technological skills to use ICT systems, and
knowledge of medical issues affect their medical and
clinical decisions, which are also affected by the
physicians' lack of time, stress and attitudes towards
patients and ICT. Second, medical and clinical
decisions are influenced by patient data in the ICT
systems, because a physician has no time to go
through every detail of the patient's past medical
history. Third, the patient data in the ICT systems is
affected by the patient her or himself, the physician,
permission denial of patient data by the patient, lack
of patient data, missing patient data, lack of patient
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
22

data transfer control, or too much data transfer
control by the laws. Fourth, the physician’s medical
and clinical decisions influence the patient care
process and patients who are affected by right or
wrong diagnoses, treatment and patient care. Fifth,
ICT systems’ communication barriers and
legislation, communication and knowledge barriers
and misunderstanding can prevent proper healthcare
of a patient, which is also affected by nurses' lack of
time and the available primary and special
healthcare services. Sixth, the ICT systems’ vendor,
technology, legislation, and lack of development
resources both at the ICT systems’ healthcare
organization and ICT system’s vendor side, together
with ICT systems’ communication barriers,
physician’s negative attitudes towards patients and
ICT systems, and reluctance to participate in ICT
systems’ development due to lack of time, combined
with lack of right medical and clinical decisions due
to lack of right data, as well as attitudes and
physician’s tacit knowledge and experience in the
decision making situation all affect patients' health
and can prevent the right patient care to be carried
out. All this also causes a lot of stress to both the
physician and the patient and forms a barrier to right
patient diagnoses and treatment. In the patient care
process, too many patients and data are directed at
the same time to one physician to be treated at a too
short notice and time. On the other hand, the ICT
systems in healthcare suffer from a lack of
resources, money and qualified personnel, and are
therefore affected by several issues at the same time.
The ICT systems also need integration and
modernization, and the ICT development personnel
needs a basic level of biomedical information
knowledge in order to understand the ICT systems in
healthcare and the healthcare professionals better,
but because of the lack of money both at the ICT
system vendors’ side and the healthcare
organization’s side, the resources must be focused
very carefully on time in order to meet the rising
costs of the patient care itself. The physicians and
nurses must also be given a basic level of ICT
education so that they are able to understand old and
new ICT systems, in addition to patients’ needs.
In our case study the purpose of the grounded
theory analysis (Glaser and Strauss, 1967) was to
find out categories and relationships between the
categories in one specific healthcare environment
with the inductive research approach. The concepts
were sharpened by building evidence from empirical
data describing the conceptual categories which
according to Glaser and Strauss (1967), and Pawluch
and Neiterman (2010) are the building blocks of the
grounded theory. Constant comparison between the
data and concepts was made so that the
accumulating evidence converged on simple and
well-defined categories. After the categories were
found, we defined the properties of the categories
and propositions (hypotheses) of how the categories
were related. In our in-depth case study, we took
carefully into consideration beforehand who to
interview, what to do next, what group to look for,
and what additional data we should collect in order
to develop a theory from the emerging data. Finally,
a conceptual framework of the categories was
developed, and the categories were grounded on
empirical evidence and theories reflecting the
findings in the field. The most fundamental
components in this conceptual framework were its
categories and the relationships between the
categories. This comparison with past studies led us
to six higher-level abstractions of statements about
the relationships between the categories. This
theorizing was in line with Pawluch’s and
Neiterman’s (2010) suggestions for creating a
grounded theory with Glaser and Strauss’s (1967)
approach. We also found empirical data which was
not supported by past studies, and we regard this
data as expansion to knowledge management in
healthcare. The expansion covers the following
issues. First, in the current ICT systems the same
patient data must be saved several times. Second, the
challenge is the attachment of private sector
admission notes (called internal referral notes or an
internal consultation request) such as X-ray pictures,
which must be sent on paper by post, or brought
along by the patient to the physician. Third, other
social and healthcare districts do not send feedback
forms about patients to the sending district of the
admission. Fourth, the guidelines about the process
are in written format, and can be viewed on web
pages (“Fair Treatment”, Käypähoito in Finnish),
but it is not known whether they are used. Fifth, the
ICT system vendors have difficulties in giving price
to the implementation and maintenance of e-services
of ICT systems. In this study, a special status in
theory building was given to the focal categories, the
social and healthcare district and its central hospital.
In our theory the ancillary category was the
knowledge management problem. We took care of
the boundary conditions in our theory creation,
because the phenomenon was so atypical that it held
only in this specific contextual healthcare
environment. Our results validated the conceptual
framework, which became the discovered theory for
the phenomenon. The data which confirmed the
emergent relationships enhanced confidence in the
KnowledgeManagementProblemsinHealthcare-ACaseStudybasedontheGroundedTheory
23

validity of the relationships. The data which
disconfirmed the relationships provided an
opportunity to expand and refine the emerging
theory. The results which did not get support from
past studies resulted in expansion to the theory. The
non-conflicting results strengthened the definitions
of our categories and the conceptual framework. The
past studies with similar findings were important
because they tied together the underlying similarities
in phenomena not associated with each other, and
stronger internal validity was achieved. There are,
however, several limitations in this study. First, we
had limited knowledge of the central hospital and
the social and healthcare district because access to
secondary sources was limited. Second, the results
may not be readily applicable to other districts and
central hospitals, as the phenomena were atypical.
Third, the use of only one social and healthcare
district and its central hospital affected our findings,
and thus generalization of the results can be difficult,
but not necessarily impossible. Fourth, we
performed a limited number of interviews, and the
nurses were not interviewed personally. Fifth, the
interviews were conducted in multiple languages,
which made the interviewing, transcribing, coding
and analyzing the material very demanding. The
translation made by the first author from one
language to another may have limited the analytical
strategies because the analysis was carried out only
of the interviews in the original material, and only
for conceptualization into the conceptual categories
and their meanings.
In the future, a large sample of data will be
collected in multiple case studies (Yin, 2003) with
several hospital departments and units of analysis
(Eisenhardt, 1989). Glaser and Strauss (1967) also
claim for both qualitative and quantitative data in
creating theory. Qualitative and quantitative data can
supplement each other and their comparison can
result in new theory.
REFERENCES
Alavi, M. and Leidner, D.E. (2001) ‘Review: Knowledge
Management and Knowledge Management Systems:
Conceptual Foundations and Research Issues’, MIS
Quarterly, vol. 25, no. 1, pp. 107-136.
Ammenwerth, E., Talmon, J., Ash, J. S., Bates, D. W.,
Beuscart-Zephir, M. C., Duhamel, A., Elkin, P. L.,
Gardner, R. M. and Geissbuhler, A. (2006) ‘Impact of
CPOE on mortality rates – contradictory findings,
important messages’, Methods of Information in
Medicine, vol. 45, no. 6, pp. 586-593.
Benbasat, I., Goldstein, D.K. and Mead, M. (1987) ‘The
Case Study Research Strategy in Studies of
Information Systems’, MIS Quarterly, vol. 11, no. 3,
pp. 369-386.
Blakeman, T., Macdonald, W., P., Gately, C. and Chew-
Graham, C. (2006) ‘A Qualitative Study of GPs’
Attitudes to Self-management of Chronic Disease’,
The British Journal of General Practice, vol. 56, no.
527, p. 407.
Burgess, C., Cowie, L. and Gulliford, M. (2012) ‘Patients'
perceptions of error in long-term illness care:
qualitative study’, Journal of Health Services
Research & Policy, vol. 17, no. 3, pp. 181-187.
Creswell, J.W. (2007) Qualitative Inquiry and Research
Design: Choosing Among Five Approaches,
California: Sage Publications.
Dalkir, K. (2005) Knowledge Management in Theory and
in Practice, London, UK: Butterworth-Heinemann
Publisher.
Denzin, N.K. (Ed.). (1978) The research act: A theoretical
introduction to sociological methods, New York:
McGraw-Hill.
Edwards, M., Wood, F., Davies, M. and Edwards, A.
(2012) ‘The Development of Health Literacy in
Patients with a Long-term Health Condition: the
Health Literacy Pathway Model’, BMC Public Health,
vol. 12, no. 1, p. 130.
Eisenhardt, K.M. (1989) ‘Building Theories from Case
Study Research’, Academy of Management Review,
vol. 14, no. 4, pp. 532-550.
Eksote. (2013)’Etelä-Karjalan Sosiaali- ja Terveyspiiri’,
Available:
http://www.eksote.fi/Fi/Eksote/Hallinto/raportit/Docu
ments/Terveydenhuollonjarjestamissuunnitelma.pdf
[10 November 2013].
Fisher, W.G (2013) ‘Doctors are drowning in too much
data, not enough appropriate information’, MedCity
News, Available: http://medcitynews.com/2012/03/
doctors-are-drowning-in-too-much-data-not-enough-
appropriate-information/ [23 May 2013].
Glaser, B. and Strauss, A.L. (1967) The Discovery of the
Grounded Theory: Strategies for Qualitative
Research, Chicago: Aldine.
Glaser, B.G. (1992) Emergence vs. Forcing: Basics of
Grounded Theory, Mill Valley, CA: Sociology Press.
Greig, G., Entwistle, V.A. and Beech, N. (2012)
‘Addressing complex healthcare problems in diverse
settings: Insights from activity theory’, Social Science
& Medicine, vol. 74, no. 3, pp. 305–312.
Grimson, J.,Grimson, W. and Hasselbring, W. (2000) ‘The
SI Challenge In Health Care’, Communications of the
ACM, vol. 43, no. 6.
Grover, V. and Davenport, T.H. (2001) ‘General
perspectives on knowledge management: Fostering a
research agenda’, Journal of Management Information
Systems, vol. 18, pp. 5-21.
Gupta, P. (2008) ‘IHE and CPOE: The Twine Shall Meet
for Healthcare’, SETLab Briefings, Infosys
Technologies Limited, Available: http://www.taurus
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
24

glocal.com/images/ihe-cpoe-infosys.pdf, [30 March
2014]
Heilmann, P. (2010) ‘To have and to hold: Personnel
shortage in a Finnish healthcare organization’,
Scandinavian Journal of Public Health, vol. 38, no. 5,
pp. 518-523.
Hill, K.S. (2010) ‘Improving quality and patient safety by
retaining nursing expertise’, The Online Journal of
Issues in Nursing, vol. 15, no. 3.
Hämäläinen, P., Reponen, J., Winblad, I., Kärki, J.,
Laaksonen, M., Hyppönen, H. and Kangas, M. (2013)
‘e-Health and e-Welfare of Finland: Check Point
2011’, National Institute for Health and Welfare.
Häyrinen, K., Saranto, K. and Nykänen, P. (2008)
’Definition, structure, content, use and impacts of
electronic health records: A review of the research
literature’, International Journal of Medical
Informatics, vol. 77, pp. 291-304.
Jonkers, H., Steen, M. and Bryant, B.R. (2003) ‘Towards a
Language for Coherent Enterprise Architecture
Description’, IEEE International Enterprise
Distributed Object Computing Conference (EDOC),
Brisbane, Australia.
Kaye, R., Kokia, E., Shalev, V., Idar, D. and Chinitz, D.
(2010) ‘Barriers and success factors in health
information technology: A practitioner's perspective’,
Journal of Management & Marketing in Healthcare,
vol. 3, no. 2, pp. 163-175.
Koskinen, J. (2010) ‘Phenomenological view of health and
patient empowerment with personal health record’,
Proceedings of the Well-being in the information
society (WIS) conference, Turku: University of Turku,
pp. 1-13.
Kothari, A., Rudman, D., Dobbins, M., Rouse, M.,
Sibbald, S. and Edwards, N. (2012) ‘The use of tacit
and explicit knowledge in public health: a qualitative
study’, Implementation Science, vol. 7, no. 1.
Laki 159/2007. (2007) ’Laki sosiaali- ja terveydenhuollon
asiakastietojen sähköisestä käsittelystä’, Available:
http://www.finlex.fi/fi/laki/alkup/2007/20070159 [10
October 2013].
Lin, C., Tan, B. and Chang, S. (2008) ‘An exploratory
model of knowledge flow barriers within healthcare
organizations’, Information & Management, vol. 45,
no. 5, pp. 331–339.
Linthicum, D.S. (2004) Next generation application
integration, Boston: Addison-Wesley.
Martikainen, S., Viitanen, J., Korpela, M. and Lääveri, T.
(2012) ’Physicians’ experiences of participation in
healthcare IT development in Finland: Willing but not
able’, International Journal of Medical Informatics,
vol. 81, no. 2, pp. 98–113.
Miles, M.B. and Huberman, A.M. (1994) Qualitative Data
analysis, Thousand Oaks, California: Sage
Publications.
Myers, M.D. and Avison, D.E. (ed.) (2002) Qualitative
Research in Information Systems: Review, London:
Sage Publications.
Nilakanta, S., Miller, L., Peer, A. and Boija, V.M. (2009)
‘Contribution of Knowledge and Knowledge
Management Capability on Business Processes among
Healthcare Organizations’, Proceedings of the 42
nd
Hawaii International Conference on System Sciences,
IEEE, pp. 1-9.
Niskanen, J.J. (2002) ‘Finnish care integrated?’,
International Journal of Integrated Care, vol. 2, no. 2.
Nonaka, I. (1994) ‘A dynamic theory of organizational
knowledge creation’, Organization Science, vol. 5, no.
1, pp. 14–37.
Nykänen, P., Kaipio, J. and Kuusisto, A. (2012)
’Evalution of the national nursing model and four
nursing documentation systems in Finland-Lessons
learned and directions for the Future’, International
Journal of Medical Informatics, vol. 81, no. 8, pp.
507–520.
Pawluch, D. and Neiterman, E. (2010) ‘What is Grounded
Theory and Where Does is Come from?’, in
Bourgeault A., Dingwall, R. and De Vries. R. (ed.)
The SAGE Handbook of Qualitative Methods in
Health Research, London: Sage Publications, pp. 174-
192.
Polanyi, M. (1966) The Tacit Dimension London:
Routledge.
Puusa, A. and Eerikäinen, M. (2010) ’Is Tacit Knowledge
Really Tacit?’, Electronic Journal of Knowledge
Management, vol. 8, no. 3, pp. 307-318.
Raudasoja, S. (2013) ‘Eksote’s Strenght is its strong
customer orientation’, External Publication of South
Karelia and Social and Health Care District,
Available: http://www.eksote.fi [20 January 2013].
Reddy, M.C., Paul, S.A., Abraham, J., McNeese, M.,
DeFlitch C., and Yen, J. (2009) ‘Challenges to
effective crisis management: Using information and
communication technologies to coordinate emergency
medical services and emergency department teams’,
International Journal of Medical Informatics, vol. 78,
no. 4, pp. 259–269.
Räisänen, T., Oinas-Kukkonen, H., Leiviskä, K.,
Seppänen, M. and Kallio, M. (2009) ’Managing
Mobile Healthcare Knowledge: Physicians'
Perceptions on Knowledge Creation and Reuse’, in
Olla, P. and Tan, J. (ed.) Mobile Health Solutions for
Biomedical Applications, New York, New Hersey: IGI
Global, pp. 111-127.
Stair, R. M. and Reynolds, G.W. (2006) Fundamentals of
Information Systems, Boston, Mass: Thomson Course
Technology.
STM. (2013) ’Sosiaali- ja terveysministeriö.
Tietojärjestelmähankkeet: sähköinen potilasarkisto ja
sosiaalialan tiedonhallinta’, Available: http://www.
stm.fi/vireilla/kehittamisohjelmat_ja_hankkeet/tietojar
jestelmahankkeet/kysymyksia_kanta_hankkeesta#vast
aus [5 October 2013].
Suomi, R. and Salmivalli, L. (2002) ‘Electronic
Prescriptions: Developments in Finland’, In
Proceedings of the IFIP Conference on Towards The
Knowledge Society: E-Commerce, E-Business,
Kluwer, BV, E-Government, pp. 481-495.
Suurla, R., Markkula, M. and Mustajärvi, O. (2002)
’Developing and implementing knowledge
KnowledgeManagementProblemsinHealthcare-ACaseStudybasedontheGroundedTheory
25

management in the parliament of Finland’, The
committee for the future: The Parliament of Finland,
Available: http://web.eduskunta.fi/dman/Document.
phxdocumentId=gk11307104202716&cmd=download
[4 September 2012].
Timonen, T. (2013) ‘Key figures: statistics from the
hospital’, Internal Publication of South Karelia Social
and Health Care District.
Viitanen, J., Hyppönen, H., Lääveri, T., Vänskä, J.,
Reponen, J. and Winblad, I. (2011) ’Nationality
questionnaire study on clinical ICT systems proofs:
Physicians suffer from poor usability’, International
Journal of Medical Informatics, vol. 80, no. 10, pp.
708–725.
Yin, R.Y. (1994) Applications of Case Study Research,
Applied Social Research Methods series 34, Newbury
Park, London: Sage Publications.
Yin, R.K. (2003). Case study research: design and
methods. California: Sage Publications.
Young, R.J., Horsley, S.D. and McKenna, M. (2000) ‘The
potential role of IT in supporting the work of junior
doctors’, Journal of the Royal College of Physicians of
London, vol. 34, no. 4.
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
26
