
Knowledge Management Problems in Hospital Work
A Case Study on Experiences in the Obstetrics and Gynaecology Department
Helvi Nyerwanire
1
, Erja Mustonen-Ollila
1
, Antti Valpas
2
and Jukka Heikkonen
3
1
Department of Software Engineering and Information Management,
Lappeenranta University of Technology, Lappeenranta, Finland
2
Department of Obstetrics and Gynaecology, South Karelia Social and Health Care District, Lappeenranta, Finland
3
European Commission Joint Research Centre, Unit JRC.G1 Scientific Support to Financial Analysis, Ispra, Italy
Keywords: Knowledge Management, Healthcare, Empirical Research, Case Study, Grounded Theory.
Abstract: In this in-depth case study, nine interviews were carried out to investigate knowledge management problems
in one healthcare department in a hospital. Based on the Grounded Theory approach, we discovered six
thematic knowledge management problem categories: Patient, Patient Data, Physician, Midwife, ICT
Systems and Medical Equipment. Each thematic category was further decomposed into multiple items
(traits) ranging from 3 to 18 items.
1 INTRODUCTION
Knowledge management is defined as a
collaborative and integrated approach to create,
capture, organize, access and use of an
organization’s intellectual capital (Dalkir, 2005).
Räisänen et al. (2009) state that knowledge from
medical and nursing practices is stored to
information communication technologies (ICT),
which cover electronic health records, computerized
physician's order entry systems, mobile applications.
ICT covers also medical equipment for diagnosis or
treatment (IBM, 2014). Healthcare suffers from
confusing ICT terms and issues and missing the
right data about patients in them. (Viitanen et al.,
2011). Dalkir (2005) states that knowledge
ownership, non-promotion of the people when they
share knowledge, lack of trust between the
knowledge provider and receiver, and understanding
the difficulties between the knowledge provider and
receiver can cause problems in knowledge
management. In this study we carry out a qualitative,
in-depth case study (Yin, 2003) that identifies
problems in knowledge management in one
healthcare department in a hospital located in the
South Karelia Social and Health Care District,
Finland. The goal of this study is to categorize
knowledge management problems and create a
theory of knowledge management by using the
Grounded Theory (GT) approach (Glaser and
Strauss, 1967; Pawluch and Neiterman, 2010) and
the case study approach (Eisenhardt, 1989; Yin,
2003). We explore strategies that the department
deploys while learning about its knowledge
management problems, the extent to what these
problems are shaped by the organizational context,
and how these potential problems influence the
patient care work in practice. The rest of the paper is
structured as follows. Section two describes related
research, section three presents the research method,
and section four outlines the analysis. Section five
contains conclusions and discussion.
2 RELATED RESEARCH
Martikainen et al. (2012) claim that physicians and
nurses have difficulties in keeping a professional
distance to patients, lack of senior and experienced
physicians, as well as knowledge transfer and
capturing problems, and ICT professionals do not
listen to healthcare professionals' requests.
According to Viitanen et al. (2011), the new medical
equipment technologies are complex, there are
communication problems between the ICT systems,
lack of time to use ICT systems, new ICT systems,
as well as medical equipment and medical practices
requiring constant learning; and especially new
medical equipment forms a risk factor. Eppler
(2007) states that there are differences in medical
261
Nyerwanire H., Mustonen-Ollila E., Valpas A. and Heikkonen J..
Knowledge Management Problems in Hospital Work - A Case Study on Experiences in the Obstetrics and Gynaecology Department.
DOI: 10.5220/0005123802610267
In Proceedings of the International Conference on Knowledge Management and Information Sharing (KMIS-2014), pages 261-267
ISBN: 978-989-758-050-5
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)

procedures and practice, and according to Reddy et
al. (2009), there is lack of medical records and
patients' control of their own data. According to
Meade et al. (2009), healthcare professionals lack
the knowledge or competence to use IT tools, a
computer, or ICT systems. Gender differences and
junior and senior physicians’ differences in the ways
of working with ICT technology have been reported
(Westbrook et al., 2005). According to Nonaka
(1994) and Alavi and Leidner (2001), there are
problems in transferring tacit knowledge. Brixey et
al. (2010) claim for interruptions in the physicians’
workflow, and Mistiaen et al. (2007) claim for
failures in patient discharge coordination.
Westbrook et al. (2005) state for the senior
physicians' requests of junior physicians to help
them in computer problems, and Dias et al. (2003)
argue for nurses' and physicians' stress. Jatain (2013)
claims for problems caused by lack of ICT
knowledge, Courtney and McCutcheon ( 2010) state
for restrictions of expert nurses to attend patient care
conferences, and Priebe et al. (2011) argue for lack
of access to the medical and social history of
undocumented migrants. Gadon and Jacobs (2007)
report about communication barriers with limited
English -proficient patients, Chadi (2009) report
about physicians' lack of time in medical practice
due to large amount of tasks, and Gill et al. (2012)
claim that the wrong medication caused by
interruption of work can cause a critical condition to
the patient. Ijäs-Kallio (2010) discusses patients’
resistance to their diagnoses, Misra et al. (2013)
patients' limited memory concerning their past
medical illnesses and procedures, and Friesen et al.
(2009) nurses and physicians forgetting to save
patients' medical information in the system. Sands
(2004) writes about physicians worrying about
patient data security, and Stausberg et al. (2003)
mention extra work due to parallel checks from both
papers and ICT electronic records. Hebert et al.
(2011) argue that nurses and physicians have to
work in a hurry, which can cause a risk to the
patient, and Pellegrino (2003) states that physicians
and nurses have difficulties to find information in
the intranet, possibly because of lack of tuition on
how to use it. Not surprisingly, the enormous
number of past studies is confounding, and adequate
theoretical explanations have yet to emerge to
explain knowledge management in healthcare. In
particular, little is known of how knowledge
management problems are related to each other, and
which problems are actually the main ones.
Therefore, the aim of our study is to respond to this
lack of knowledge and to provide new information
about knowledge management problems in
healthcare. Though demanding in terms of data
collection and analysis, such investigations can
improve our understanding of knowledge
management problems in healthcare considerably in
practice and help us identify how the hospital
environment influences knowledge management at
the department level. Based on the past studies, we
have formulated the following research question,
RQ1: What are the knowledge management
problems in the obstetrics and gynaecology
department?
3 RESEARCH METHOD
The unit of analysis in this study is the Obstetrics
and Gynaecology department in the central hospital
of the South Karelia Social and Health Care District,
Finland. The department has 8 senior physicians, 3
specializing junior physicians, 42 midwives, and 10
nurses. On average 1155 births in a year have taken
place for the last ten years. In the department,
patients make clinical visits to the maternity ward,
and there is an open gynaecological clinic for
women (Raudasoja, 2013). This study takes the
qualitative, in-depth case study and Grounded
Theory (GT) approach to understand the complex
technological and social phenomena of knowledge
management problems in one specific healthcare
environment (Glaser and Strauss, 1967; Eisenhardt,
1989; Yin, 2003; Pawluch and Neiterman, 2010).
The definitions of knowledge management and
objectives of the research formed the basis for the
interviews and data collection. The interviewees
were chosen because their role was to use, create
and transfer healthcare-related medical and ICT
information, and translate it to knowledge relevant
to the healthcare situation at hand. In order to
address the research question, we carried out the
study with four midwives, three senior physicians
and two junior physicians in January-February 2013.
The physicians had 10 to 30 years of experience of
baby deliveries, and women’s diseases and
gynaecology. The midwives had 10 to 20 years of
experience in delivering babies and taking care of
women' illnesses. The interviewees chose options
from a list of 32 pre-structured questions and were
allowed to discuss the questions freely. The
interviews included frequent elaboration and
clarification of the meanings and terms, and they
were audio-recorded and transcribed to text, yielding
almost 250 pages of transcripts.
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
262
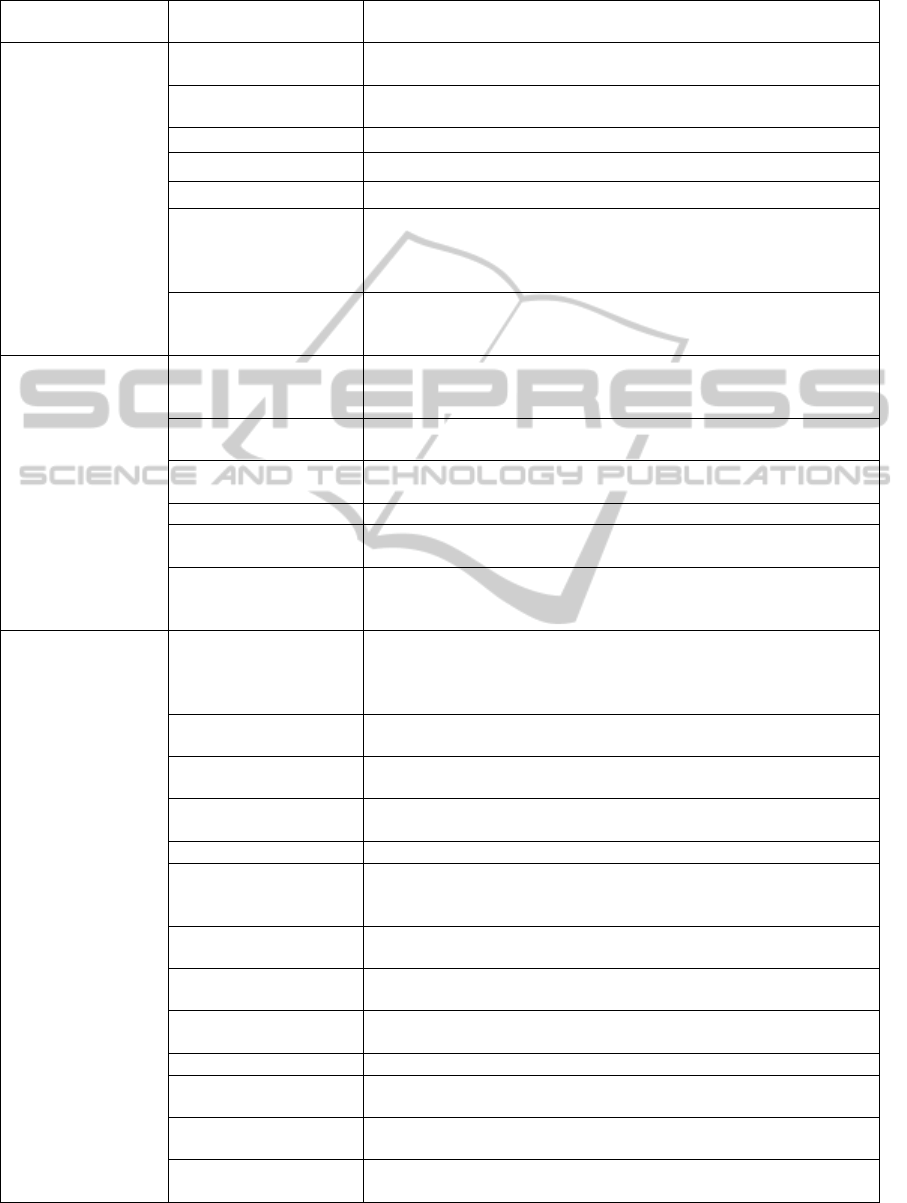
Table 1: Thematic category and definition, and item and definition.
Thematic category
and definition
Item Item definition
Patient:
A patient receives
care and treatment
from a physician or
a midwife
Characteristics
Each patient brings a set of unique characteristics to the care
situation.
Diagnosis attitude
Patient’s attitude towards diagnosis is positive or negative, and
beliefs and intentions can affect his/her behavior.
Medication Patient’s pharmaceutical drugs.
High health risk Patient’s high health risk increases the chance of disease or injury.
Demobilization Patient’s discharge from hospital to home.
Coordination problems
between local services
in primary and special
healthcare
Problems with patient healthcare coordination in local settings.
Lack of a contact tool
Lack of knowledge of which is the proper tool- a letter or phone
call- to make contact if the patient has housing, alcohol or drug
problems.
Patient data:
Patient’s personal
data, medical
history, treatments,
tests, examinations,
diagnoses, and
consultation
requests
Data in ICT systems
Patient’s personal data, medical history, treatments, tests,
examinations, diagnoses, and consultation requests in the ICT
systems.
Lack of data in ICT
systems
Patient’s personal data, medical history etc. are missing from the
ICT systems.
Lack of international
patients’ medical data
Lack of access to the medical history of undocumented migrants.
Transfer on paper Patient’s personal data, medical history etc. are transferred on paper.
Check from paper and
ICT
Both paper-based and electronic patient records must be checked in
parallel.
Access rights and
permission denial
Access through the portal is restricted to seeing patient data inside
or outside the hospital. The patient can deny access to his/her data
on paper or in ICT systems.
Physician:
A physician needs
knowledge of
anatomy,
physiology and
medical science in
practicing
medicine.
Thoughts about
midwives’ professional
distance towards
patients
Midwives want to keep a professional distance towards patients,
because they want to understand the patient from the patients’ point
of view by using midwives’ psychological knowledge.
Clinical work time
Physicians need time for clinical work, but midwives and nurses do
not.
Gender differences
Female physicians spend more time in consultation with the patient
than male physicians.
Dominant power
position
Senior physicians use their superior position over nurses, midwives,
and junior physicians.
Lack of resources Lack of physicians to carry out patient care in hospitals.
Non-routine work
Time is spent in face-to-face contact with patients by gathering
information and developing a relationship, doing administrative
work related to visits, and maintaining knowledge.
Medical and clinical
decisions
A physician makes a diagnostic decision and determines the proper
treatment for the patient.
Private files of patients
The physicians have private and secret files of a patient which they
do not share with others.
Tacit knowledge
A physician’s tacit knowledge is related to how she or he is able to
use his or her biomedical knowledge, intuition and experience.
Stress Patients cause stress to physicians.
Lack of time
Physicians do not have enough time in the policlinic to search for
patient information.
Tiredness
Physicians feel tired of reading system manuals or getting familiar
with new ICT systems constantly coming to use.
Professional distance to
patients
The knowledge of psychological aspects in a doctor-patient
relationship enables doctors to establish professional distance.
KnowledgeManagementProblemsinHospitalWork-ACaseStudyonExperiencesintheObstetricsandGynaecology
Department
263
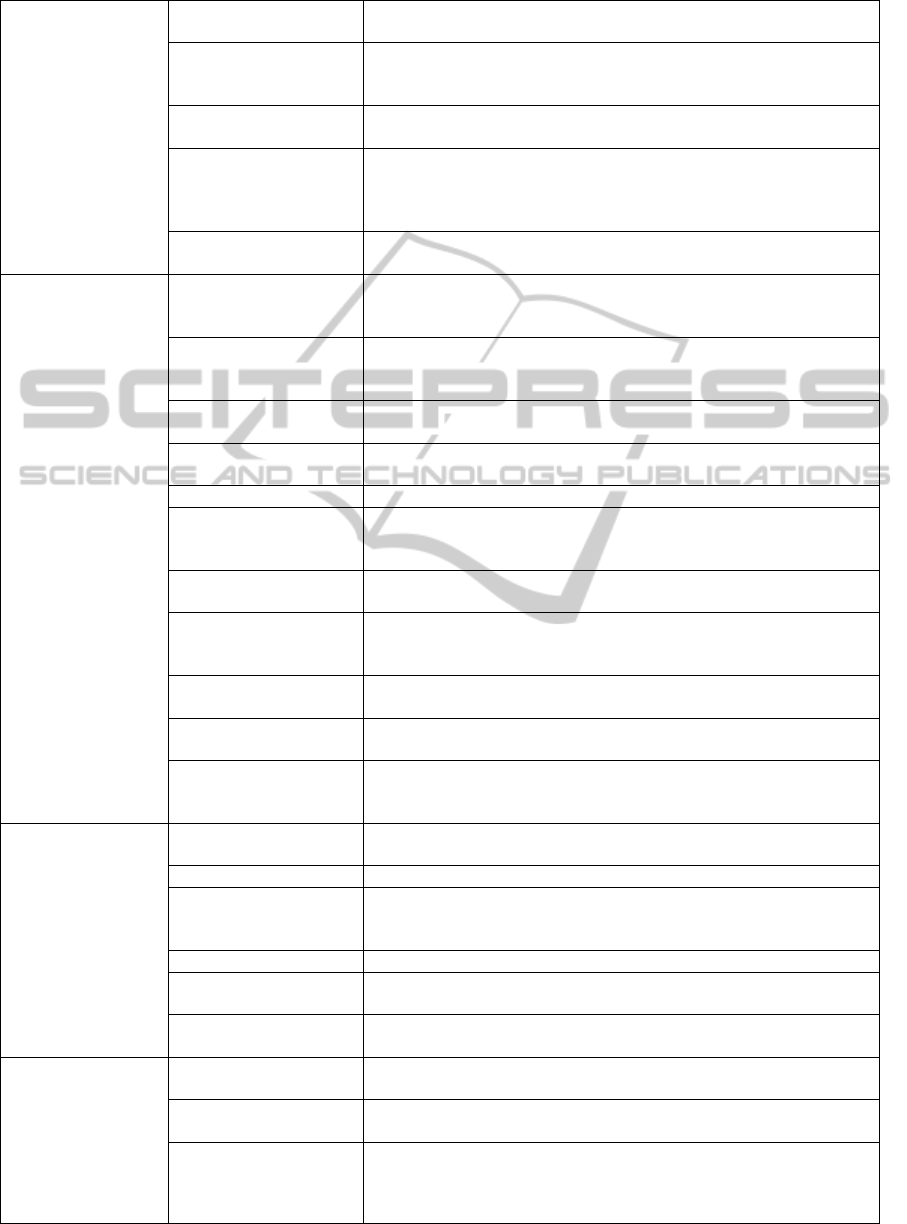
Table 1: Thematic category and definition, and item and definition (cont.).
Physician:
A physician needs
knowledge of
anatomy,
physiology and
medical science in
practicing
medicine.
Medical practice
differences
Physicians claim that there are medical procedures which are not
used in their internal unit.
Lack of ICT
competence and
knowledge
Physicians lack knowledge or competence to use IT tools,
computers, and ICT systems.
Work flow
interruptions
The work flow is interrupted by phone calls, computer systems,
specific equipment, and delays of patients or colleagues.
Lack of expertise
sharing between local
and university clinics’
physicians
In the hospital, the local clinic’s physicians cannot discuss or share
expertise in video consultations with university clinics.
Work competence
differences
Junior physicians have limited experience and they do not yet trust
their clinical judgment fully.
Midwife:
A midwife is a
trained nurse
specialized in
women's labor,
delivery, women’s
special illnesses,
and taking care of
the baby after the
birth.
Lack of knowledge of
the patient’s social
issues
During the patient interview the midwives do not know the patient's
social history without asking.
Lack of ICT and IT
competence and
knowledge
Midwives lack knowledge or competence of how to use IT tools,
computers, and ICT systems.
Acute work
The midwives are busy or have to work in a hurry in the baby
delivery room.
Work flow
interruptions
Constant work flow interruptions in baby delivery.
Stress The midwives feel stress also in miscarriage situations.
Diagnosis counseling
The physicians do not have time to explain the diagnosis to the
patient thoroughly, and thus the midwives have to explain the
diagnoses.
Lack of time
The midwives have to work in a hurry because of stressful and busy
work, challenging work, time pressures, or high job demands.
Lack of work
competence
development possibility
Expert midwives cannot participate in patient care conferences even
if they have in-depth knowledge of the patient care system.
Unclear responsibilities
Difficulty to distinguish the difference of work between midwives
and physicians.
New practices review
The new practices or information sent by the physicians are first
compared with the on-paper practices of the department or hospital.
Non-routine work
Time is spent in face-to-face contact with patients by gathering
information and developing a relationship, doing administrative
work related to visits, maintaining knowledge.
ICT Systems:
There are hundreds
of ICT systems
used in hospitals,
and the physicians
and other
professionals use
them in their daily
work with patients.
Communication
barriers
Hospitals using different ICT systems are not able to communicate,
and paper serves as a coordination tool.
User problems The hospital ICT systems are difficult to use.
Time spent in using
ICT systems
The healthcare ICT systems are difficult to use and not user
friendly, and it takes a lot of time to use the system. The systems
reduce the time spent with patients
Economic purposes ICT systems are rather made for economic purposes.
Information retrieval
difficulties
The users claim that it is difficult to find information from the
intranet, possibly because of lack of tuition in how to use it.
Physicians' attitudes
towards the ICT vendor
The ICT developers do not ask users about their opinions or
experiences of the ICT systems.
Medical equipment:
Medical equipment
is designed to aid in
the diagnosis,
monitoring or
treatment of
medical conditions.
Risks
When the system fails in the middle of a medical situation it poses a
risk to patient safety.
Responsibility for
failures
There are responsibility problems for technological failures between
physicians, selling firms and buyers of medical equipment.
Physician’s attitudes to
medical equipment
Physicians' attitudes towards medical equipment are negative
because of lack of time.
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
264

4 ANALYSIS WITH THE
GROUNDED THEORY
APPROACH
After transcribing the interviews we searched for
knowledge management problems from the
empirical data. Then we categorized the discovered
knowledge management problems under thematic
categories according to the relevant terminology and
past studies (see chapter 2) that were the most often
refereed work of categorizing concepts in the studied
research area. In this Grounded Theory analysis we
used our intuition and knowledge in fragmentating
and reassembling our data into thematic categories
(Glaser and Strauss, 1967; Pawluch and Neiterman,
2010). Finally, we decomposed each category into
multiple items (traits) by using content analysis to
derive the items from the data and validate them
with past studies. The special data table including
the categories, definitions, literature sources,
empirical evidence, transcript numbers etc. is
available by a separate request from the second
author. The thematic categories and definitions,
items and definitions are presented in Table 1 below.
As shown in Table 1, six thematic categories
were formed in the study: the Patient, Patient data,
Physician, Midwife, ICT systems, and Medical
equipment. The patient category had 14 observations
and 7 items; the Patient data category 20
observations and 6 items; the Physician category 33
observations and 18 items; the Midwife category 12
observations and 11 items; the ICT Systems
category 17 observations and 6 items; and the
Medical equipment category had 11 observations
and 3 items.
5 DISCUSSION AND
CONCLUSIONS
In the Grounded Theory approach the theory
emerges from the data. In our in-depth case study we
took carefully into consideration beforehand who to
interview, what to do next, what group to look for,
and what additional data we should collect in order
to develop a theory from the data. During the study
we learned that some questions in the interview
protocol tool were more specific to physicians than
to midwives and vice versa. Theoretical background
knowledge was gained during the research, which
increased the credibility of the study (Miles and
Huberman, 1994). According to Eisenhardt (1989),
the combination of case study with the Grounded
Theory approach has three major strengths: it
produces a novel theory, the emergent theory is
testable, and the resultant theory is empirically valid.
The first limitation of the study is the question of
whether there was enough data to derive the
knowledge management categories and items, and if
the discovered categories and items were the correct
ones. The second limitation is that the external
validity of the data is higher because we analyzed
real data, but our internal validity is lower because
we did not have complete data to all the stimuli.
Therefore some caution must be exercised when
interpreting the results. In the future, we will
continue the study, and our next task is to find out
propositions (hypotheses) on how the categories are
related on the basis of the data, and finally what is
the higher level of abstraction of the statements. Our
new theory, a conceptual framework which includes
thematic categories and items, and relationships
between the categories, will be based on empirical
evidence and theories reflecting the findings in the
field, which is in line with Pawluch and Neiterman’s
(2010) suggestions for creating a grounded theory
with the Glaser and Strauss (1967) approach based
on own intuition and knowledge. As our goal is to
create a theory, and to enhance the validity and
reliability of the categories and their relationships,
the data will be analyzed with novel intelligent
computing methods (Kohonen 1989) to find out
unique patterns and clusters of knowledge
management problems and items. The knowledge
management practices will be improved when the
physicians and nurses understand their own valuable
knowledge capital and practice, and understand
knowledge management problems when building up
healthcare information systems in the hospital.
Furthermore, four other departments have been
included in the research, and new interview rounds
have been and will be carried out in the following
order: in January - April 2014, a second round of
interviews was carried out in the Obstetrics and
Genecology department.; in March - May 2014 the
first interview round was carried out in the
Paediatric department.; in March - June 2014 the
first interview round is carried out in the Paediatric
Neurology department.; in May - September 2014
the first interview round will be carried out in the
Surgical department.; and finally in May -September
2014 the first interview round will be carried out in
the Anaesthesia and Surgery department.
REFERENCES
Alavi, M. and Leidner, D.E. (2001) ‘Review: Knowledge
KnowledgeManagementProblemsinHospitalWork-ACaseStudyonExperiencesintheObstetricsandGynaecology
Department
265

Management and Knowledge Management Systems:
Conceptual Foundations and Research Issues’, MIS
Quarterly, vol. 25, no. 1, pp. 107-136
Brixey, J.J., Robinson, D.J., Turley, J.P. and Zhang, J.
(2010) ‘ The roles of MDs and RNs as Initiators and
Recipients of Interruptions in Workflow‘,
International Journal of Medical Informatics, vol. 79,
no. 6, pp. 109-115.
Chadi, N. (2009) ‘Medical Leadership: Doctors at the
Helm of Change‘, McGill Journal of Medicine, vol.
12, no. 1.
Courtney, M. and McCutcheon, H. (2010) Using Evidence
to Guide Nursing Practice, Livingstone, Australia:
Elsiever Science.
Dalkir, K. (2005) Knowledge Management in Theory and
in Practice, London, UK: Butterworth-Heinemann
Publisher.
Dias, L., Chabner, B. A., Lynch, T. J. and Penson, R. T.
(2003) ‘Breaking bad news: a patient’s perspective‘,
The Oncologist, vol. 8, no. 6, pp. 587-596.
Eisenhardt, K.M. (1989) ‘Building Theories from Case
Study Research’, Academy of Management Review,
vol. 14, no. 4, pp. 532-550.
Eppler, M.J. (2007) ‘Knowledge communication problems
between experts and decision makers: an overview and
classification‘, The Electronic Journal of Knowledge
Management, vol. 5, no. 3, pp. 291-300.
Friesen, M. A., White, S. V. and Byers, J. F. (2009)
‘Handoffs: Implications for Nurses‘, in Hughes, R.G.
(ed.) Patient Safety and Quality: An Evidence-Based
Handbook for Nurses, US: Agency for Healthcare
Research and Quality.
Gadon, M. P. H. and Jacobs, E. A. (2007) ‘Caring for
patients with limited English proficiency: the
perspectives of small group practitioners‘, Journal of
General Internal Medicine, vol. 22, no. 2, pp. 341-
346.
Gill P.S., Kamath A. and Gill T.S. (2012) ‘Distraction: an
assessment of smartphone usage in healthcare work
settings‘, Risk Management and Healthcare Policy,
vol. 5, pp. 105-114.
Glaser, B. and Strauss, A.L. (1967) The Discovery of the
Grounded Theory: Strategies for Qualitative
Research, Chicago: Aldine.
Hebert, K., Moore, H. and Rooney, J. (2011) ‘The nurse
advocate in end-of-life care‘, The Ochsner Journal,
vol. 11, no. 4, pp. 325-329.
IBM, (2014) ‘Medical Technology Equipment Modality
Definitions/Glossary ‘, Available: http://www-03.ibm.
com/financing/pdf/us/igf4-a042.pdf [08 May 2014].
Ijäs-Kallio, T., Ruusuvuori, J. and Peräkylä, A. (2010)
‘Patient resistance towards diagnosis in primary care:
Implications for concordance‘, Health, vol. 14, no. 5,
pp. 505-522.
Jatain, R. (2013) ‘Different prospects of office automation
systems‘, International Journal of Computer Trends
and Technology, vol. 4, no. 3, pp. 210-212.
Kohonen, T. (1989)
Self-Organization and Associative
Memory, Berlin: Springer-Verlag.
Martikainen, S., Viitanen, J., Korpela, M. and Lääveri, T.
(2012) ‘Physicians’ experiences of participation in
healthcare IT development in Finland: Willing but not
able‘, International Journal of Medical Informatics,
vol. 81, no. 2, pp. 98–113.
Meade, B., Buckley, D. and Boland, M. (2009) ‘What
factors affect the use of electronic patient records by
Irish GPs?‘, International Journal of Medical
Informatics, vol. 78, no. 8, pp. 551–558.
Miles, M.B. and Huberman, A.M. (1994) Qualitative Data
analysis, Thousand Oaks, California: Sage
Publications.
Misra, S., Daly, B., Dunne, S., Millar, B., Packer, M. and
Asimakopoulou, K. (2013) ‘Dentist–patient
communication: what do patients and dentists
remember following a consultation? Implications for
patient compliance‘, Patient Preference and
Adherence, vol. 7, pp. 543-549.
Mistiaen, P., Francke, A.L. and Poot, E. (2007)
‘Interventions aimed at reducing problems in adult
patients discharged from hospital to home: a
systematic meta-review‘, BMC Health Services
Research, vol. 7, no. 1.
Nonaka, I. (1994) ‘A dynamic theory of organizational
knowledge creation’, Organization Science, vol. 5, no.
1, pp. 14–37.
Pawluch, D. and Neiterman, E. (2010) ‘What is Grounded
Theory and Where Does is Come from?’, in
Bourgeault A., Dingwall, R. and De Vries. R. (ed.)
The SAGE Handbook of Qualitative Methods in
Health Research, London: Sage Publications, pp. 174-
192.
Pellegrino, G. (2003) ‘Representations and uses of the
intranet: a comparative case study‘, Bulletin of
Science, Technology & Society, vol. 23, no. 4, pp. 281-
296.
Priebe, S., Sandhu, S., Dias, S., Gaddini, A., Greacen, T.,
Ioannidis, E. and Bogic, M. (2011) ‘Good practice in
health care for migrants: views and experiences of care
professionals in 16 European countries‘, BMC Public
Health, vol. 11, no. 1.
Raudasoja, S. (2013) ‘EKSOTE’s Strenght is its strong
customer orientation: South Karelia’s Social and
Healthcare District‘, External Publication of Eksote.
Reddy, M.C., Paul, S.A., Abraham, J., McNeese, M.,
DeFlitch, C. and Yen, J. (2009) ‘Challenges to
effective crisis management: Using information and
communication technologies to coordinate emergency
medical services and emergency department teams‘,
International Journal of Medical Informatics, vol. 78,
no. 4, pp. 259–269.
Räisänen, T., Oinas-Kukkonen, H., Leiviskä, K.,
Seppänen, M. and Kallio, M. (2010) Managing Mobile
Healthcare Knowledge: Physicians’ Perceptions on
Knowledge Creation and Reuse, in Rodrigues, J. (ed.)
Health Information Systems: Concepts,
Methodologies, Tools, and Applications (pp. 733-749).
Sands, D. Z. (2004) ‘Help for physicians contemplating
use of e-mail with patients‘, Journal of the American
Medical Informatics Association, vol. 11, no. 4, pp.
268-269.
KMIS2014-InternationalConferenceonKnowledgeManagementandInformationSharing
266

Stausberg, J., Koch, D., Ingenerf, J. and Betzler, M.
(2003) ‘Comparing paper-based with electronic patient
records: lessons learned during a study on diagnosis
and procedure codes‘, Journal of the American
Medical Informatics Association, vol. 10, no. 5, pp.
470-477.
Viitanen, J., Hyppönen, H., Lääveri, T., Vänskä, J.,
Reponen, J. and Winblad, I. (2011) ‘Nationality
questionnaire study on clinical ICT systems proofs:
Physicians suffer from poor usability‘, International
Journal of Medical Informatics, vol. 80, no 10, pp.
708–725.
Westbrook, J.I., Gosling, A.S. and Westbrook, M.T.
(2005) ‘Use of point-of-care online clinical evidence
by junior and senior doctors in New South Wales
public hospitals‘, Internal Medicine Journal, vol. 35,
no. 7, pp. 399–404.
Yin, R.K. (2003) Case study research: design and
methods, California: Sage Publications.
KnowledgeManagementProblemsinHospitalWork-ACaseStudyonExperiencesintheObstetricsandGynaecology
Department
267
