
Activities of Daily Living in Healthy Adults and Children
Reliability of Registrations with Multiple Body Worn Sensors
Ryanne Lemmens
1,2
, Henk Seelen
1,2
, Yvonne Janssen-Potten
1,2
, Annick Timmermans
1,3
,
Marlous Schnackers
1
, Annet Eerden
2
, Richard Geers
2
and Rob Smeets
1,2
1
Department of Rehabilitation Medicine, Research School CAPHRI, Maastricht University, Maastricht, Netherlands
2
Adelante, Centre of Expertise in Rehabilitation and Audiology, Hoensbroek, Netherlands
3
BIOMED Biomedical Research Institute, Hasselt University, Hasselt, Belgium
1 OBJECTIVES
Patients with stroke or cerebral palsy often
encounter arm-hand problems during daily life.
Assessment is important to determine the progress of
arm-hand performance in patients during
rehabilitation, and to ascertain the effectiveness of
therapies. Many instruments are available to assess
capacity or perceived performance, but instruments
assessing actual performance are scarce (Lemmens
et al., 2012). Inertial sensors may be used to assess
actual performance. However, signal reliability
during execution of activities of daily living (ADL)
should be determined first.
Aim of this study was to examine the reliability
of the data of upper extremity skill performance in a
standardized setting, in both healthy adults and
healthy children, registered using a combination of
multiple body worn sensors.
2 METHODS
In this non-randomised cross-sectional study, both
healthy adults (aged > 50 years) and healthy children
were included. Because motor control processes may
mature with age, resulting in differences in skill
execution, the children were divided into two age
groups, i.e. 6-11 years and 12-18 years. Four 9-DOF
sensor devices, each containing a tri-axial
accelerometer, gyroscope and magnetometer were
attached to the dominant hand, wrist, upper arm and
chest of participants.
Data were registered during the execution of 5
repetitions of 2 tasks, i.e. ‘drinking from a cup’ and
‘eating with knife and fork’. Tasks were first
performed without extensive instructions (e.g. with
the instruction: “drink from the cup.”), and
subsequently with extensive instructions on how to
perform the task (e.g. “reach to the cup, grasp it,
bring it to your mouth, take a sip, put the cup back
on the table and go back to your starting position.”).
Signals were filtered with a 4
th
order zero-time
lag low-pass Butterworth filter (cut off frequency of
1.28 Hz). Repetitions of each specific task were
identified and intra-class correlation coefficients
(ICC) for each sensor and signal type were
determined as a measure of reliability, both within
and between subjects. For every person, a mean ICC
was measured. Since data was not normally
distributed, medians were calculated. The ICCs were
classified based on the kappa statistic classification
of Landis and Koch, i.e. ICC between 0.8-1.0=very
good; 0.6-0.8=good; 0.4-0.6=moderate; 0.2-0.4=fair;
<0.2=slight (Landis and Koch, 1977).
3 RESULTS
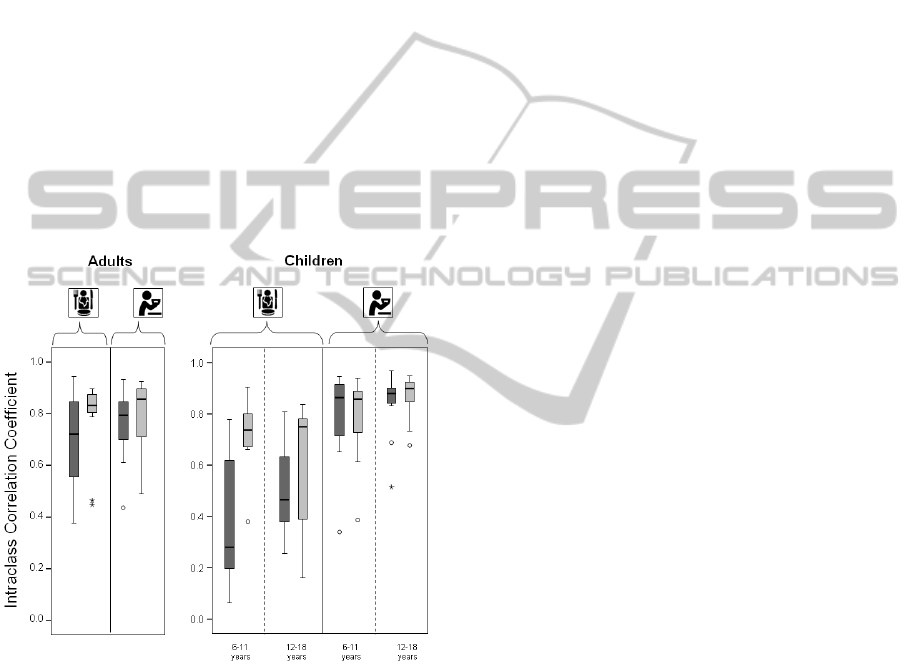
Figure 1: Within-subject reliability expressed as intra-class
correlation coefficients, for the skills eating and drinking.
Dark grey bars represent the performance of the task
without instruction, whereas light grey bars represent the
performance of the task with instruction.
Lemmens R., Seelen H., Janssen-Potten Y., Timmermans A., Schnackers M., Eerden A., Geers R. and Smeets R..
Activities of Daily Living in Healthy Adults and Children - Reliability of Registrations with Multiple Body Worn Sensors.
Copyright
c
2014 SCITEPRESS (Science and Technology Publications, Lda.)
Thirty adults were included (14 women, 16 men,
mean age 58.0 ± 5.1 years), 16 children aged
between 6-11 years (9 girls, 7 boys, mean age 8.5 ±
1.7 year) and 16 children aged between 12 and 18
years (8 girls, 8 boys, mean age 14.6 ± 1.5 years).
Figure 1 displays within-subject reliability of the
skills drinking and eating for both the adults and the
children. With regard to the within subject
reliability, the median ICC’s were good for the skill
eating and very good for the skill drinking.
Reliability was better for the skill performed with
instruction compared to the skill performed without
instruction, especially for the skill eating.
Furthermore it can be seen that the children aged
between 12-18 years showed a slightly higher
reliability compared to the children aged between 6-
12 years.
Figure 2 displays between-subject reliability of
the skills drinking and eating for both the adults and
the children.
Figure 2: Between-subject reliability expressed as intra-
class correlation coefficients, for the skills eating and
drinking. Dark grey bars represent the performance of the
task without instruction, whereas light grey bars represent
the performance of the task with instruction.
Between-subject reliability was good to very
good for both skills performed by adults. The skills
drinking performed by the children had a very good
reliability whereas the skill eating had a fair to
moderate reliability in the youngest children, and a
good reliability in the older children. Especially for
the skill eating, a big difference was seen regarding
the reliability of the performance without instruction
compared to the performance with instruction. For
the skill drinking, reliability was comparable
between younger children and the older children
whereas for the skill eating, performance of the older
children had a higher reliability.
4 DISCUSSION
Overall, the skill drinking as well as the skill eating
had a good to very good within-subject reliability in
both adults and children. Performance with
instruction had a higher reliability compared to
performance without instruction. By giving
instructions about how to perform the task, the
variability in execution of the task was reduced,
thereby increasing the reliability.
The performance of the skill drinking had a
higher reliability compared to the skill eating. This
can be explained by the complexity of the skills, i.e.
drinking is a rather simple skill, which cannot be
performed in many ways, whereas the skill eating
consists of more sub movements and can, in
addition, be performed in many different ways.
Between-subject reliability of the skill eating was
relatively low, especially for the performance
without instruction in the youngest children. This
can be explained by the fact that many children did
not use the knife to cut the food, whereas other
children had difficulties manipulating the knife. For
the performance with instruction, they were told
how to use the knife.
In conclusion, we have shown that a
combination of multiple body worn sensors is able
to reliably register activities of daily living in
healthy adults as well as in healthy children. Future
research will focus on the investigation of signal
reliability during activities of daily living performed
by patients and in a daily life setting.
REFERENCES
Landis, J. R. and Koch, G. G. (1977) The measurement of
observer agreement for categorical data. Biometrics,
33, 159-74.
Lemmens, R., Timmermans, A., Janssen-Potten, Y.,
Smeets, R. and Seelen, H. (2012) Valid and reliable
instruments for arm-hand assessment at ICF activity
level in persons with hemiplegia: a systematic review.
BMC Neurology, 12, 21.
